
The Effectiveness of Combined Exercise and Self-Determination Theory Programmes on Chronic Low Back Pain: A Systematic Review and Metanalysis

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality of the Included Studies
2.6. Risk of Bias of the Included Studies
2.7. Statistical Analysis
3. Results
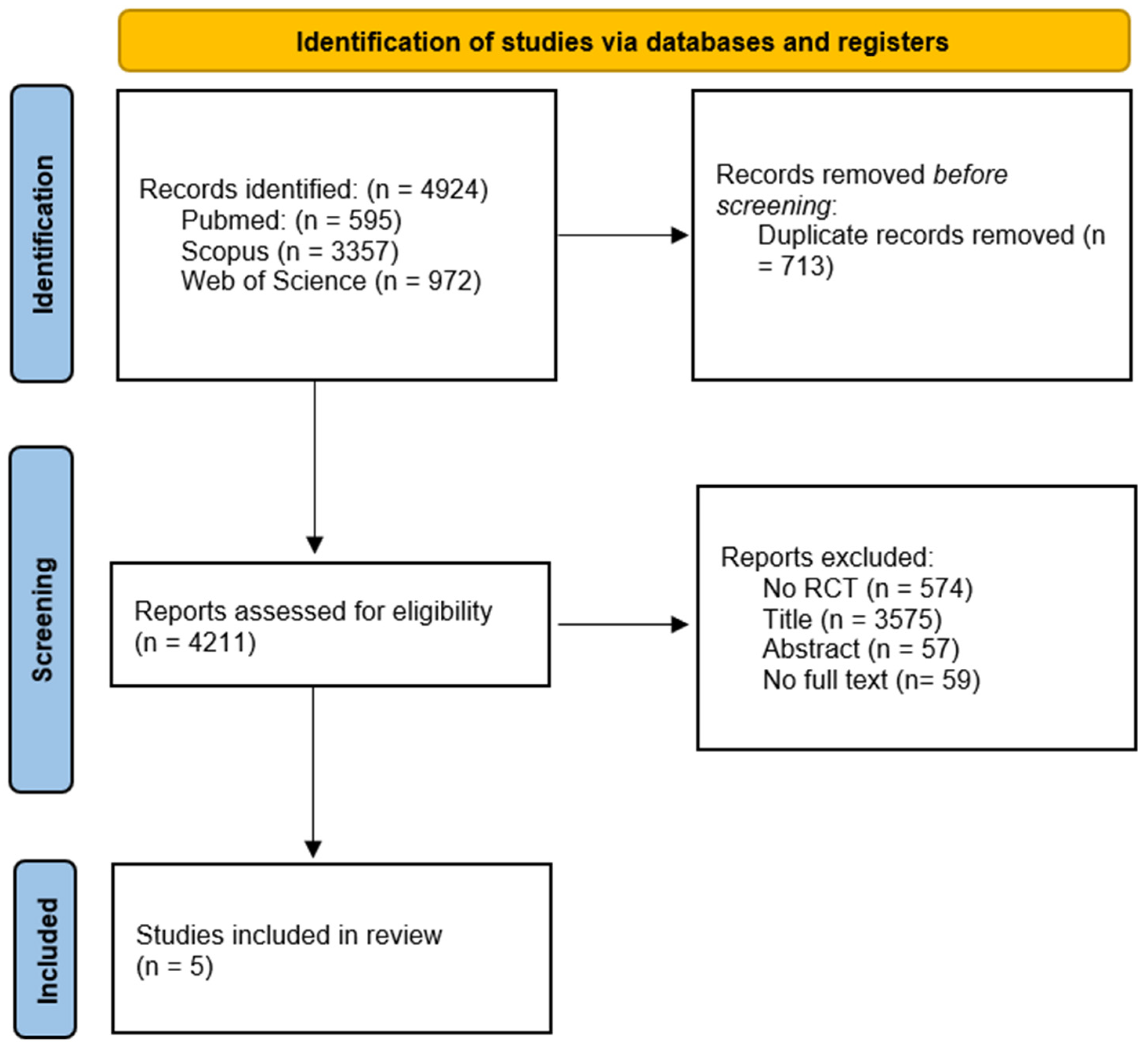
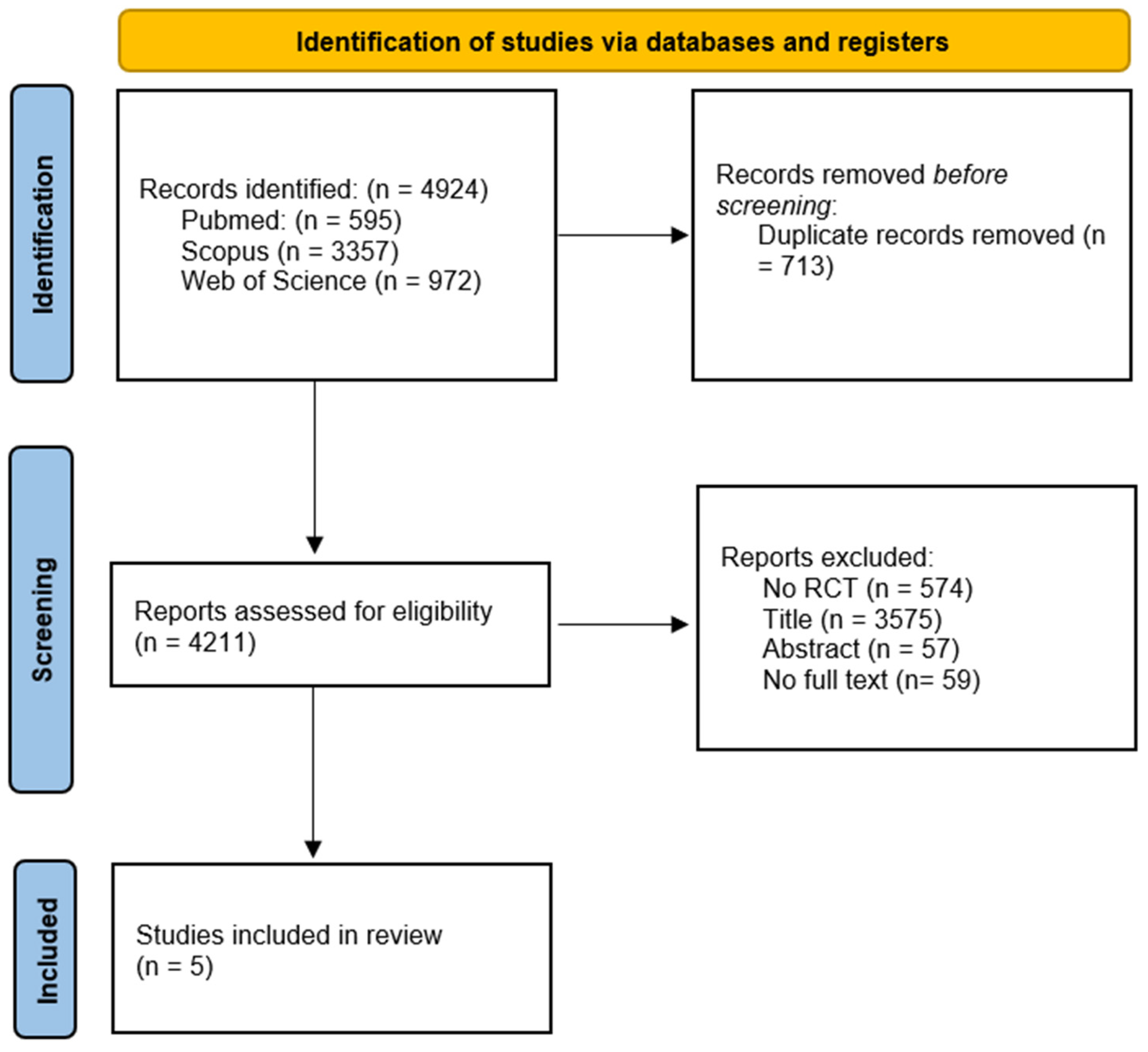
3.1. Search Selection
3.2. Characteristics of Studies
3.3. Methodological Quality of the Included Studies
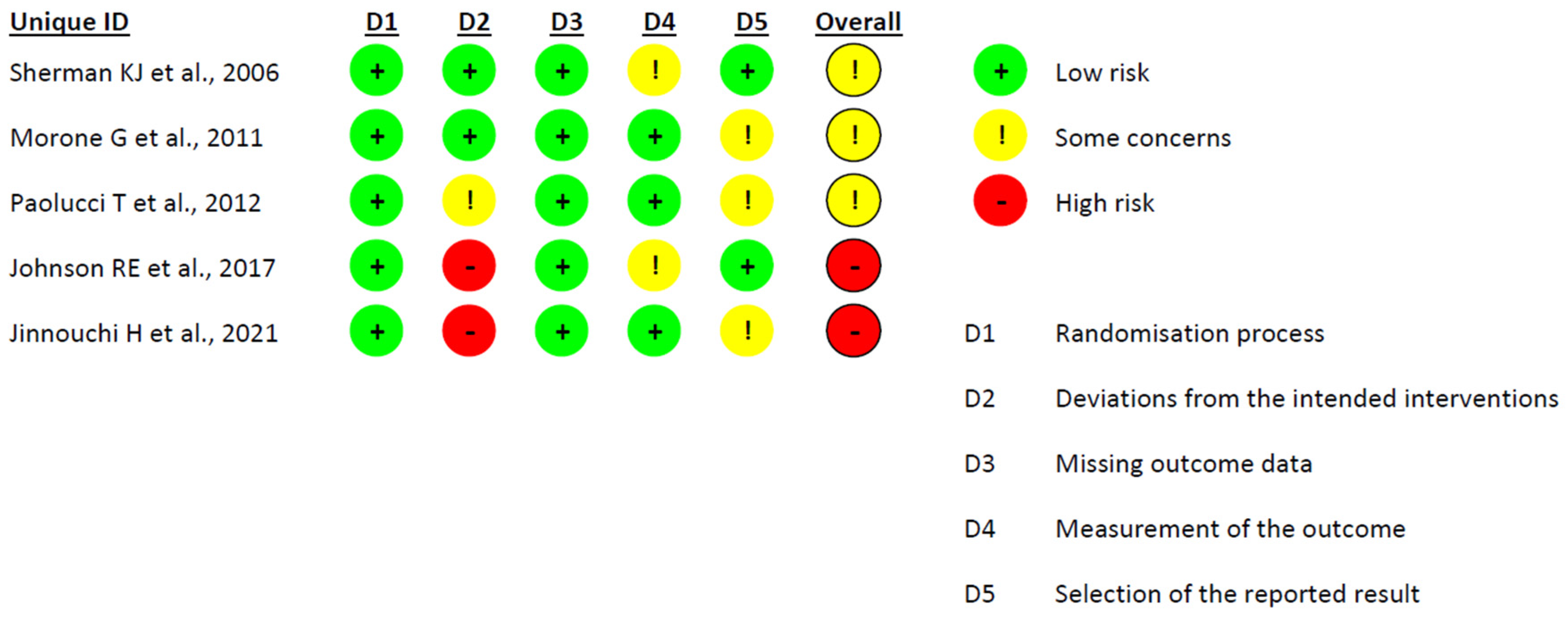
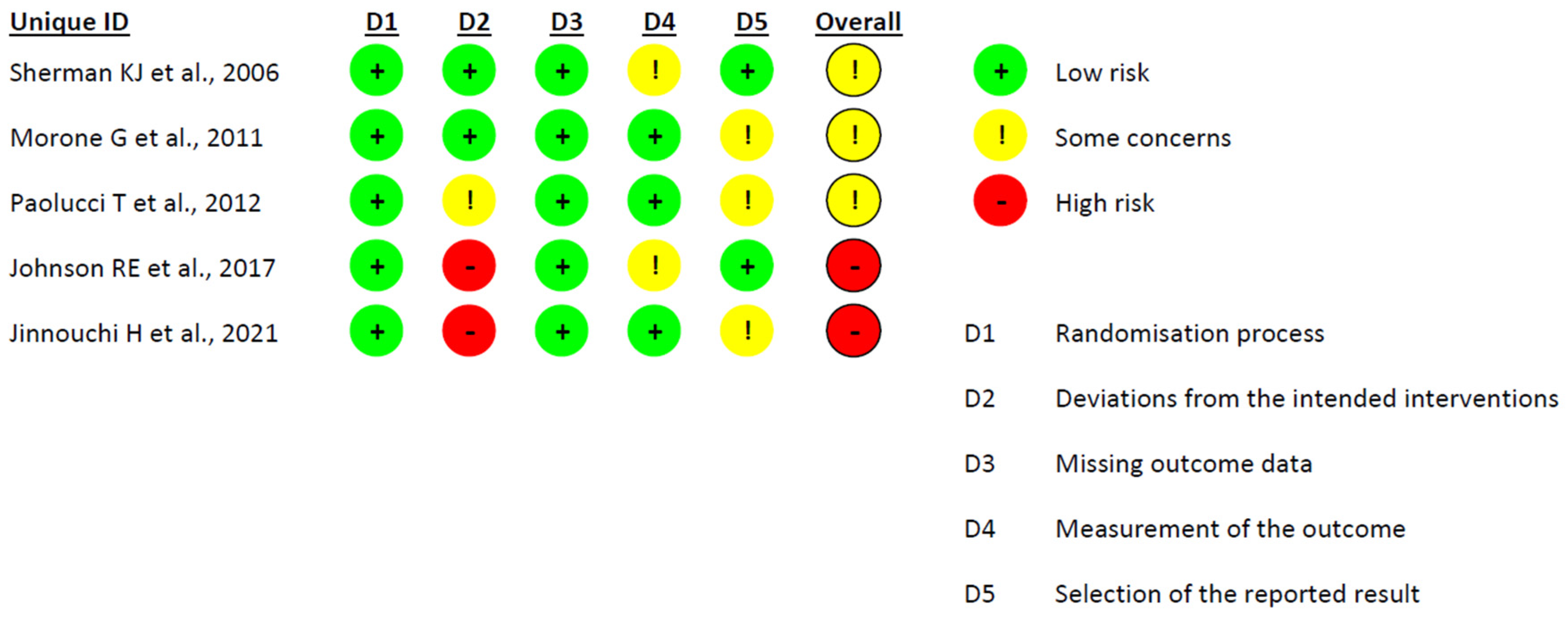
3.4. Risk of Bias of the Included Studies
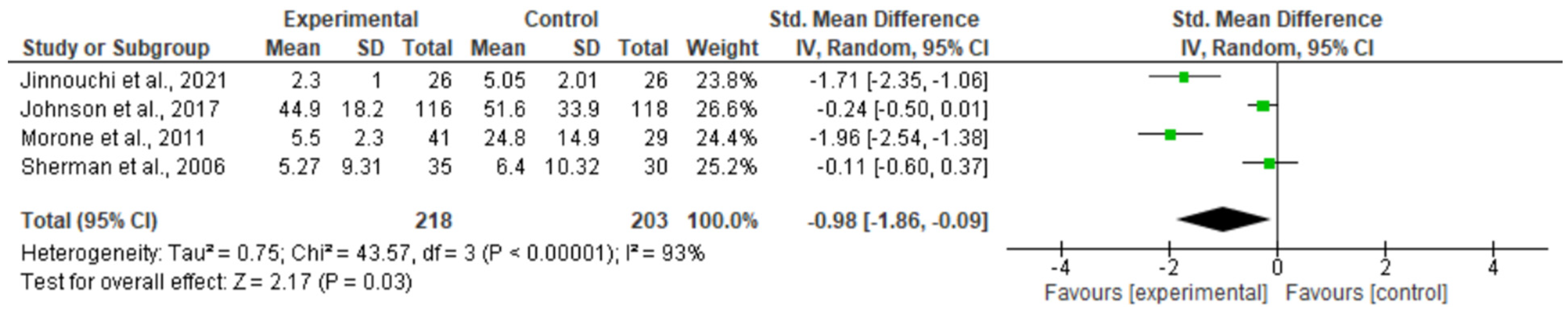
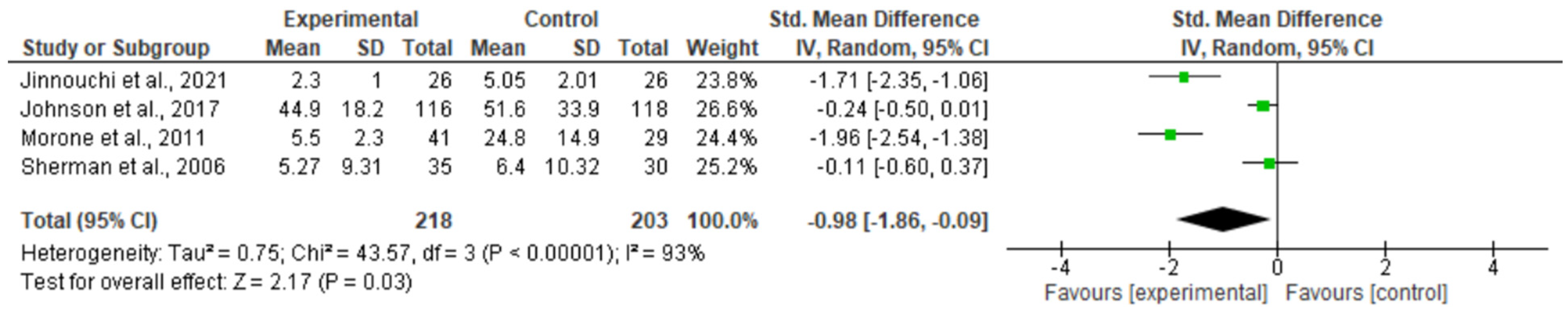
3.5. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Liddle, S.D.; Baxter, G.D.; Gracey, J.H. Chronic Low Back Pain: Patients’ Experiences, Opinions and Expectations for Clinical Management. Disabil. Rehabil. 2007, 29, 1899–1909. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What Low Back Pain Is and Why We Need to Pay Attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Shiri, R.; Falah-Hassani, K. Does Leisure Time Physical Activity Protect against Low Back Pain? Systematic Review and Meta-Analysis of 36 Prospective Cohort Studies. Br. J. Sports Med. 2017, 51, 1410–1418. [Google Scholar] [CrossRef]
- Lee, H.; Hübscher, M.; Moseley, G.L.; Kamper, S.J.; Traeger, A.C.; Mansell, G.; McAuley, J.H. How Does Pain Lead to Disability? A Systematic Review and Meta-Analysis of Mediation Studies in People with Back and Neck Pain. Pain 2015, 156, 988–997. [Google Scholar] [CrossRef]
- Bui, Q.; Doescher, M.; Takeuchi, D.; Taylor, V. Immigration, Acculturation and Chronic Back and Neck Problems among Latino-Americans. J. Immigr. Minor. Health 2011, 13, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Cilliers, F.; St-Onge, C.; van der Vleuten, C. Health Behaviour Theories: A Conceptual Lens to Explore Behaviour Change. In Researching Medical Education; Wiley: Hoboken, NJ, USA, 2022; pp. 251–265. [Google Scholar] [CrossRef]
- Brooks, J.M.; Iwanaga, K.; Chiu, C.Y.; Cotton, B.P.; Deiches, J.; Morrison, B.; Moser, E.; Chan, F. Relationships between Self-Determination Theory and Theory of Planned Behavior Applied to Physical Activity and Exercise Behavior in Chronic Pain. Psychol. Health Med. 2017, 22, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Geidl, W.; Semrau, J.; Pfeifer, K. Health Behaviour Change Theories: Contributions to an ICF-Based Behavioural Exercise Therapy for Individuals with Chronic Diseases. Disabil. Rehabil. 2014, 36, 2091–2100. [Google Scholar] [CrossRef] [PubMed]
- Henriques, M.A.; de Sousa Loura, D. Concepts and Theories in Behaviour Change to Support Chronic Disease Self-Management. In A Practical Guide on Behaviour Change Support for Self-Managing Chronic Disease; Springer: Berlin/Heidelberg, Germany, 2023; pp. 11–21. [Google Scholar] [CrossRef]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-Determination Theory Applied to Health Contexts: A Meta-Analysis. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.; Chatzisarantis, N.L.; Culverhouse, T.; Biddle, S.J. The Processes by Which Perceived Autonomy Support in Physical Education Promotes Leisure-Time Physical Activity Intentions and Behavior: A Trans-Contextual Model. J. Educ. Psychol. 2003, 95, 784. [Google Scholar] [CrossRef]
- Xu, H.R.; Zhang, Y.H.; Zheng, Y.L. The Effect and Mechanism of Motor Control Exercise on Low Back Pain: A Narrative Review. EFORT Open Rev. 2023, 8, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, N.; Gillison, F.; Rodham, K. How Do Peer Support Interventions for the Self-Management of Chronic Pain, Support Basic Psychological Needs? A Systematic Review and Framework Synthesis Using Self-Determination Theory. Patient Educ. Couns. 2022, 105, 3225–3234. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Patrick, H.; Deci, E.L.; Williams, G.C.; Ryan, R. Facilitating Health Behaviour Change and Its Maintenance: Interventions Based on Self-Determination Theory. Eur. Health Psychol. 2008, 10, 2–5. [Google Scholar]
- Sherman, K.J.; Cherkin, D.C.; Erro, J.; Miglioretti, D.L.; Deyo, R.A. Comparing Yoga, Exercise, and a Self-Care Book for Chronic Low Back Pain: A Randomized, Controlled Trial. Ann. Intern. Med. 2005, 143, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, T.; Alcuri, M.; Vulpiani, M.; Matano, A.; Bureca, I.; Paolucci, S.; Saraceni, V. Quality of Life Improved by Multidisciplinary Back School Program in Patıents with Chronic Non-Specific Low Back Pain: A Single Blind Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2011, 47, 533–541. [Google Scholar] [PubMed]
- Paolucci, T.; Morone, G.; Iosa, M.; Fusco, A.; Alcuri, R.; Matano, A.; Bureca, I.; Saraceni, V.M.; Paolucci, S. Psychological Features and Outcomes of the Back School Treatment in Patients with Chronic Non-Specific Low Back Pain. A Randomized Controlled Study. Eur. J. Phys. Rehabil. Med. 2012, 48, 245–253. [Google Scholar]
- Johnson, R.E.; Jones, G.T.; Wiles, N.J.; Chaddock, C.; Potter, R.G.; Roberts, C.; Symmons, D.P.M.; Watson, P.J.; Torgerson, D.J.; Macfarlane, G.J. Active Exercise, Education, and Cognitive Behavioral Therapy for Persistent Disabling Low Back Pain: A Randomized Controlled Trial. Spine 2007, 32, 1578–1585. [Google Scholar] [CrossRef]
- Jinnouchi, H.; Matsudaira, K.; Kitamura, A.; Kakihana, H.; Oka, H.; Hayama-Terada, M.; Yamagishi, K.; Kiyama, M.; Iso, H. Effects of Brief Self-Exercise Education on the Management of Chronic Low Back Pain: A Community-Based, Randomized, Parallel-Group Pragmatic Trial. Mod. Rheumatol. 2021, 31, 890–898. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0. 1. The Cochrane Collaboration. Available online: www.training.cochrane.org/handbook (accessed on 11 December 2023).
- Dubois, J.D.; Abboud, J.; St-Pierre, C.; Piché, M.; Descarreaux, M. Neuromuscular Adaptations Predict Functional Disability Independently of Clinical Pain and Psychological Factors in Patients with Chronic Non-Specific Low Back Pain. J. Electromyogr. Kinesiol. 2014, 24, 550–557. [Google Scholar] [CrossRef]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1140.e1–1140.e22. [Google Scholar] [CrossRef]
- Wood, L.; Hendrick, P.A. A Systematic Review and Meta-Analysis of Pain Neuroscience Education for Chronic Low Back Pain: Short-and Long-Term Outcomes of Pain and Disability. Eur. J. Pain 2019, 23, 234–249. [Google Scholar] [CrossRef]
- Pei, J.H.; Ma, T.; Nan, R.L.; Chen, H.X.; Zhang, Y.B.; Gou, L.; Dou, X.M. Mindfulness-Based Cognitive Therapy for Treating Chronic Pain A Systematic Review and Meta-Analysis. Psychol. Health Med. 2021, 26, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.L.; Ryan, C.G.; Martin, D.J. Pain Neurophysiology Education for the Management of Individuals with Chronic Low Back Pain: A Systematic Review and Meta-Analysis. Man. Ther. 2011, 16, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise Interventions for the Treatment of Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; Van Tulder, M.W.; Tomlinson, G. Systematic Review: Strategies for Using Exercise Therapy to Improve Outcomes in Chronic Low Back Pain. Ann. Intern. Med. 2005, 142, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Semrau, J.; Hentschke, C.; Peters, S.; Pfeifer, K. Effects of Behavioural Exercise Therapy on the Effectiveness of Multidisciplinary Rehabilitation for Chronic Non-Specific Low Back Pain: A Randomised Controlled Trial. BMC Musculoskelet. Disord. 2021, 22, 500. [Google Scholar] [CrossRef]
- Siyu, Y.; Hong, L.; Qun, Y.; Hua, Q.; Kang, W.; Yibiao, D.; Wenping, W.; Qian, S.; Bo, F.; Xiaonan, R. Effects of Exercise Training Combined with Psychological Intervention Compared to Exercise Training Alone in Prediabetes Subjects. J. Public Health 2020, 42, 388–394. [Google Scholar] [CrossRef]
- Wiles, L.; Cafarella, P.; Williams, M.T. Exercise Training Combined with Psychological Interventions for People with Chronic Obstructive Pulmonary Disease. Respirology 2015, 20, 46–55. [Google Scholar] [CrossRef]
- Van Laake-Geelen, C.C.M.; Smeets, R.J.E.M.; Quadflieg, S.P.A.B.; Kleijnen, J.; Verbunt, J.A. The Effect of Exercise Therapy Combined with Psychological Therapy on Physical Activity and Quality of Life in Patients with Painful Diabetic Neuropathy: A Systematic Review. Scand. J. Pain 2019, 19, 433–439. [Google Scholar] [CrossRef]
- Oakman, J.; Neupane, S.; Proper, K.I.; Kinsman, N.; Nygård, C.H. Workplace Interventions to Improve Work Ability: A Systematic Review and Meta-Analysis of Their Effectiveness. Scand. J. Work Environ. Health 2018, 44, 134–146. [Google Scholar] [CrossRef]
- Verbunt, J.A.; Smeets, R.J.; Wittink, H.M. Cause or Effect? Deconditioning and Chronic Low Back Pain. Pain 2010, 149, 428–430. [Google Scholar] [CrossRef]
- Verbunt, J.A.; Seelen, H.A.; Vlaeyen, J.W.S. Disuse and Physical Deconditioning in Chronic Low Back Pain. In Understanding and Treating Fear of Pain; Oxford Academy: Oxford, UK, 2004; pp. 139–162. [Google Scholar] [CrossRef]
- Turner, J.A.; LeResche, L.; Von Korff, M.; Ehrlich, K. Back Pain in Primary Care. Patient Characteristics, Content of Initial Visit, and Short-Term Outcomes. Spine 1998, 23, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Main, C.J.; Buchbinder, R.; Porcheret, M.; Foster, N. Addressing Patient Beliefs and Expectations in the Consultation. Best Pr. Res. Clin. Rheumatol. 2010, 24, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Keefe, F.J.; Main, C.J.; George, S.Z. Advancing Psychologically Informed Practice for Patients With Persistent Musculoskeletal Pain: Promise, Pitfalls, and Solutions. Phys. Ther. 2018, 98, 398–407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N Reports Excluded | Reason for Exclusion | Explanation |
|---|---|---|
| 574 | No RCT | The type of article was not a randomized controlled trial. They were case studies, non-randomized studies, protocols, etc. |
| 3575 | Title | After reading the title, it was verified that it was not related to the topic of the study and/or did not meet any of the PICOS criteria. |
| 57 | Abstract | After reviewing the title and being unsure of the possibility of inclusion, the abstract was read. After certifying that it did not meet any of the criteria of our PICO questions, the report was excluded. |
| 59 | No full text | For full texts not initially available in the databases consulted, the researchers contacted the authors of the studies to request the full text. When this was not possible and the authors did not respond, the article was excluded. |
| Authors, Year | Sample | Sample Age (Years ± SD) | Sex [Women (%)] | Pain Duration | Pain Intensity (VAS/NRS) [Mean (SD)] | Downs and Black | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Sherman KJ et al., 2006 [17] | 101 | At least 12 weeks | NR | 23 | Some concerns | ||
| EG: 35 | EG: 42 ± 15 | EG: 63% | |||||
| CG1: 36 | CG1: 44 ± 12 | CG1: 69% | |||||
| CG2: 30 | CG2: 45 ± 11 | CG2: 67% | |||||
| Morone G et al., 2011 [18] | 73 | At least 3 months | 21 | Some concerns | |||
| EG: 44 | EG: 61.2 (13.3) | EG: 24 (54.5%) | EG: 6.6 ± 2.2 | ||||
| CG: 29 | CG: 58.6 (12.2) | CG: 21 (72.41%) | CG: 7.1 ± 1.8 | ||||
| Paolucci T et al., 2012 [19] | 100 | weeks | 23 | Some concerns | |||
| EG: 29 | EG: NR | EG: 16 (55.1%) | EG: NR | ||||
| EG1:11 | EG1: 58.0 ± 13.1 | EG1: 5 (45.4%) | EG1: 6 ± 4 | ||||
| EG2:18 | EG2: 60 ± 15.7 | EG2:11 (61.1%) | EG2: 7 ± 2 | ||||
| CG: 21 | CG: NR | CG: 15 (71.4%) | CG: NR | ||||
| CG1(NES): 11 | CG1(NES): 56.1 ± 12.9 | CG1(NES):7 (63.6%) | CG1:7 ± 2 | ||||
| CG2(ES): 10 | CG2(ES): 58.4 ± 14.9 | CG2(ES):8 (80%) | CG2:8 ± 1 | ||||
| Johnson RE et al., 2017 [20] | 234 | 100 mm VAS: >20 mm or more RMDQ > 5 | EG: 44.9 ± 18.2 CG: 51.6 ± 22.9 VAS | 21 | High risk | ||
| EG:116 | EG: 47.3 ± 10.9 | EG:71 (61%) | |||||
| CG:118 | CG: 48.5 ± 11.4 | IG: 69 (58%) | |||||
| Jinnouchi H et al., 2021 [21] | 52 | At least 3 months | EG: 5.4, 4–7 CG: 5.1, 4–6 NRS | 22 | High risk | ||
| EG: 26 | EG: 65, 62–70 | EG: 65.4% | |||||
| IG: 26 | CG: 66, 64–71 | CG: 61.5% |
| Authors, Year | Experimental Intervention | Control Intervention | Programme Duration | Outcomes | Results | RMDQ Baseline | RMDQ End Treatment |
|---|---|---|---|---|---|---|---|
| Sherman KJ et al., 2006 [17] | Education (educational talk on proper body mechanics, the benefits of exercise, realistic goal setting, overcoming barriers, and feedback) + exercise (aerobic and strengthening exercises) | CG1: Yoga CG2: Educational book | 12 weeks, 12 sessions, 75 min each session | Disability (RMDQ) | Significant intragroup differences; Significant differences compared to CG1 (p = 0.034), and no significant differences compared to CG2 (p = 0.12) | EG: 9.0 ± 4.1 CG1: 8.1 ± 4.5 CG2: 8.0 ± 4.0 | EG: 5.27 ± 9.31 CG1: 3.12 ± 5.6 CG2:6.4 ± 10.32 |
| Morone G et al., 2011 [18] | Back school (theoretical lessons about the anatomical knowledge of the spine and its function and ergonomic positions, pain concepts, psychological aspects, stress management, workplace situations, sport activities, and re-education) + exercise (exercises based on the re-education of breathing, self-stretching trunk muscles, erector spine reinforcement, abdominal reinforcement, and postural exercises) | Usual care (analgesics, myorelaxants, and NSAIDs) | 4 weeks, 10 sessions | Disability (ODI), QoL (SF-36) | Significant EG improvements (p = 0.018) | EG: 6.6 ± 2.2 CG: 24.8 ± 14.6 | EG: 5.5 ± 2.3 CG: 24.8 ± 14.9 |
| Paolucci T et al., 2012 [19] | Back school (education about anatomical information related to the spine, its functioning and ergonomic positions, pain concepts, psychological aspects and stress management, workplace situation, and sport activities) + exercise (exercises based on the re-education of breathing, self-stretching trunk muscles, erector spine reinforcement, abdominal reinforcement, and postural exercises) | Usual care (NSAIDs and myorelaxants) | 4 weeks, 10 sessions | Disability (ODI), QoL (SF-36) | Significant EG1 and EG2 improvements (p < 0.001) | EG: NR EG1(NES): 24 ± 42 EG2(ES): 28 ± 18 CG: NR CG1(NES): 12 ± 13 CG2(ES): 34 ± 10 | EG: NR EG1(NES): 15.64 p = 0.001 EG2(ES): 18.28 p < 0.001 CG: NR CG1(NES): 2.28 p = 0.516 CG2(ES): 3.07 p = 0.381 |
| Johnson RE et al., 2017 [20] | Active exercise and education (problem solving, pacing, the regulation of activity, cognitive restoration, feedback, engaging in avoiding certain activities, pacing activities, and hobbies) + educational booklet and audiocassette | Educational booklet and audiocassette | 6 weeks, 8 sessions, 120 min each session | Disability (RMDQ), QoL (EQ-D5) | No statistically significant results in reducing disability (−0.6 score; 95% confidence interval, −1.6, 0.4). EG reduced disability by 0.6 points; | EG: 10.6 ± 3.9 CG: 10.9 ± 4.0 | EG:44.9 ± 18.2 CG:51.6 ± 22.9 |
| Jinnouchi H et al., 2021 [21] | Brief self-exercise education (100 min consultation, tailor-made self-exercise programme and individualized direct teaching) | Educational book | 24 weeks, 4 sessions, 30 min each session | Disability (RMDQ), QoL (EQ-D5) | Improvement on RMDQ −2.3 (−3.3 to 1.3, p < 0.001) | EG: 4.7, 1–7 (Average, points) CG: 5.1, 1–9 (Average, points) | EG: 2.3 ± 1 CG: 5.05 ± 2.019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navas-Otero, A.; Calvache-Mateo, A.; Martín-Núñez, J.; Valenza-Peña, G.; Hernández-Hernández, S.; Ortiz-Rubio, A.; Valenza, M.C. The Effectiveness of Combined Exercise and Self-Determination Theory Programmes on Chronic Low Back Pain: A Systematic Review and Metanalysis. Healthcare 2024, 12, 382. https://doi.org/10.3390/healthcare12030382
Navas-Otero A, Calvache-Mateo A, Martín-Núñez J, Valenza-Peña G, Hernández-Hernández S, Ortiz-Rubio A, Valenza MC. The Effectiveness of Combined Exercise and Self-Determination Theory Programmes on Chronic Low Back Pain: A Systematic Review and Metanalysis. Healthcare. 2024; 12(3):382. https://doi.org/10.3390/healthcare12030382
Chicago/Turabian StyleNavas-Otero, Alba, Andrés Calvache-Mateo, Javier Martín-Núñez, Geraldine Valenza-Peña, Sofía Hernández-Hernández, Araceli Ortiz-Rubio, and Marie Carmen Valenza. 2024. "The Effectiveness of Combined Exercise and Self-Determination Theory Programmes on Chronic Low Back Pain: A Systematic Review and Metanalysis" Healthcare 12, no. 3: 382. https://doi.org/10.3390/healthcare12030382
APA StyleNavas-Otero, A., Calvache-Mateo, A., Martín-Núñez, J., Valenza-Peña, G., Hernández-Hernández, S., Ortiz-Rubio, A., & Valenza, M. C. (2024). The Effectiveness of Combined Exercise and Self-Determination Theory Programmes on Chronic Low Back Pain: A Systematic Review and Metanalysis. Healthcare, 12(3), 382. https://doi.org/10.3390/healthcare12030382