_MD__MPH_PhD.png)
Family in Crisis: Do Halfway Houses Perform Better Than Families with Expressed Emotion toward Patients with Schizophrenia? A Direct Adjusted Comparison

 , ,
, ,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Measurements
- -
- Brief Psychiatric Rating Scale (BPRS): BPRS originally included 16 interviewer-rated items assessing the intensity of symptoms of schizophrenia [29]. The most commonly used 18-item version with the addition of excitement and disorientation in 1966 has a five-factor structure, including Thinking disorder, Withdrawal, Anxiety/Depression, Hostility/Suspicion, and Activity factors [30].
- -
- Perceived Criticism (PC): The PC instrument was introduced to measure perceived criticism in a sample of depressed patients and their spouses [31] but it has since been used with several other populations, including patients with schizophrenia [32,33]. It consists of only one self-rated question rated on a 10-point Likert scale: “How critical do you feel hostel nurses/your parents have been of you overall in the last month?”.
- -
- Five Minutes Speech Sample (FMSS): The FMSS [34] is a tool for measuring EE. In comparison to the CFI, the standard assessment tool of EE, the FMSS is easier to use, needs far less time to administer, and requires shorter training of the interviewer. It can also be used even when the researcher does not know the patient very well. Each rater (i.e., care provider or family member) is asked to talk continuously for 5 min about each patient (in his/her absence) and the interview is audiotaped. All recorded 5 min interviews are then scored according to specific rules based on the assessment of the following: (a) the initial statement in terms of content and voice tone, (b) the quality of the patient–rater relationship, (c) the number of negative or positive comments, and (d) the display or report of specific behaviors during the interview (see Supplementary Methods for details on scoring). Every 5 min speech sample is eventually characterized as high, borderline, or low on Criticism and EOI; combined classifications may also arise (e.g., ‘high critical’, ‘high EOI’, ‘high critical + EOI’). FMSS interviews were scored by a trained author (S.D.) and an acceptable inter-rater agreement with another trained author (P.F.) was recorded in 20 interviews (criticism, EOI kappa = 0.89; critical comments ICC = 0.91; positive attitude statements ICC = 0.90).
2.3. Statistical Analysis
3. Results
3.1. Sample Descriptives, Univariate Comparisons, and Correlations
3.1.1. Patients (Inpatients–Outpatients) and Raters (Nurses–Parents)
3.1.2. EE Ratings
3.2. Univariate Patient-Related Predictors of EE Outcomes in the Total Sample
3.3. Adjusting for Patient-Related Confounders Only
3.3.1. Effect of Patient Group on EE Outcomes after Adjusting for Patient-Related Confounders Only
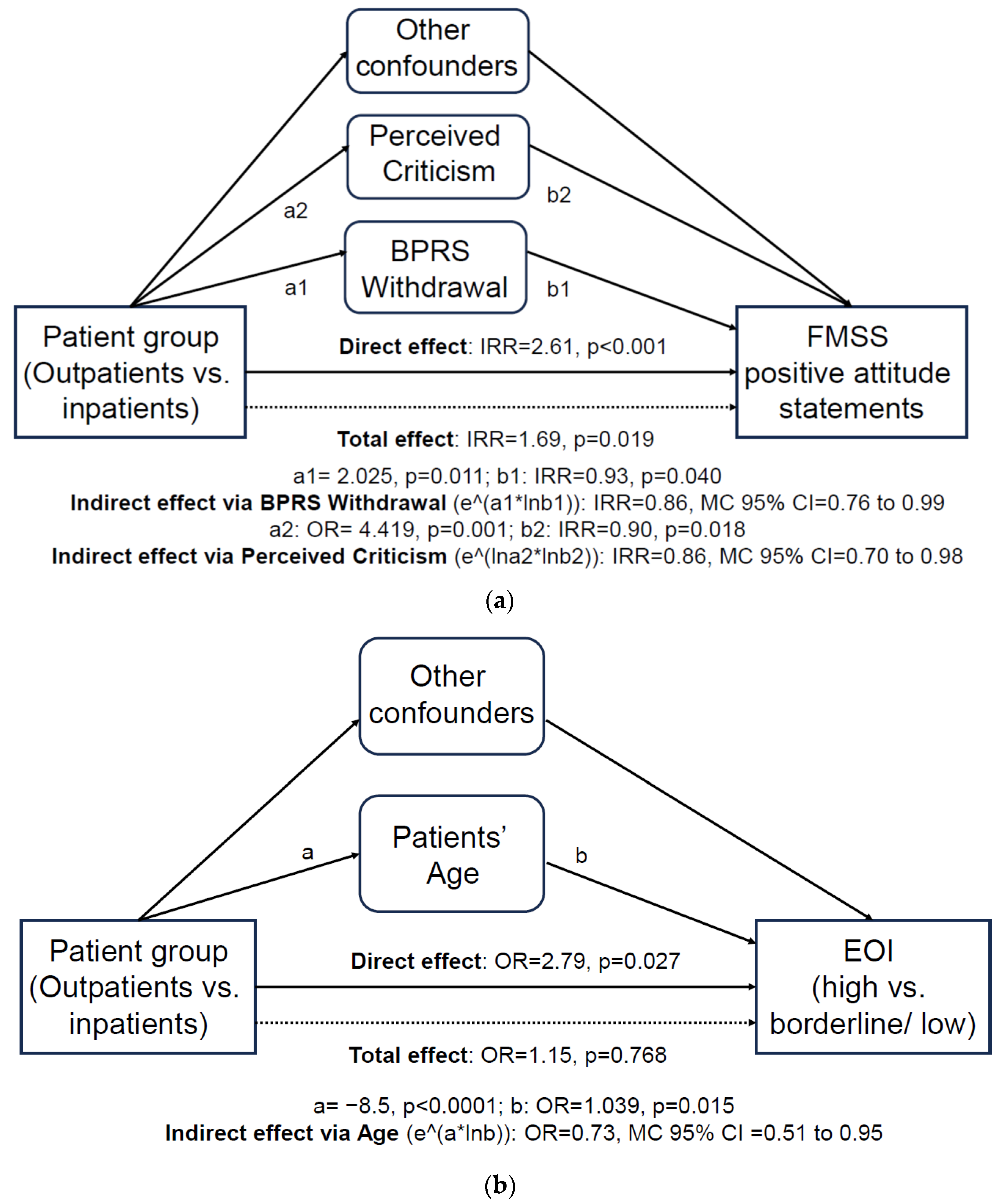
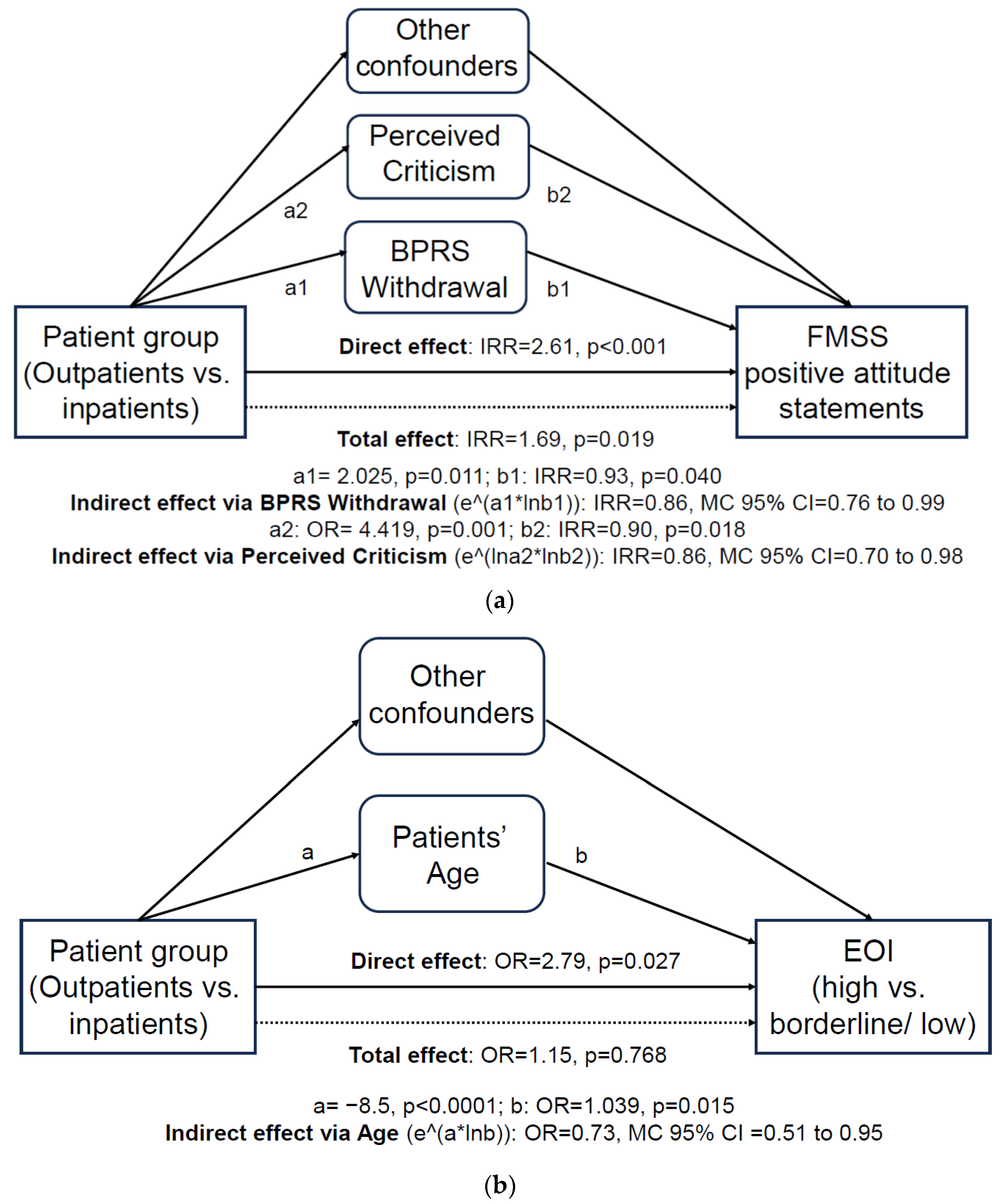
3.3.2. Patient-Related Mediators of the Effect of Patient Group on EE Outcomes
3.4. Adjusting for Both Patient- and Rater-Related Confounders
3.4.1. Effect of Patient Group on EE Outcomes after Adjusting for Patient- and Rater-Related Confounders
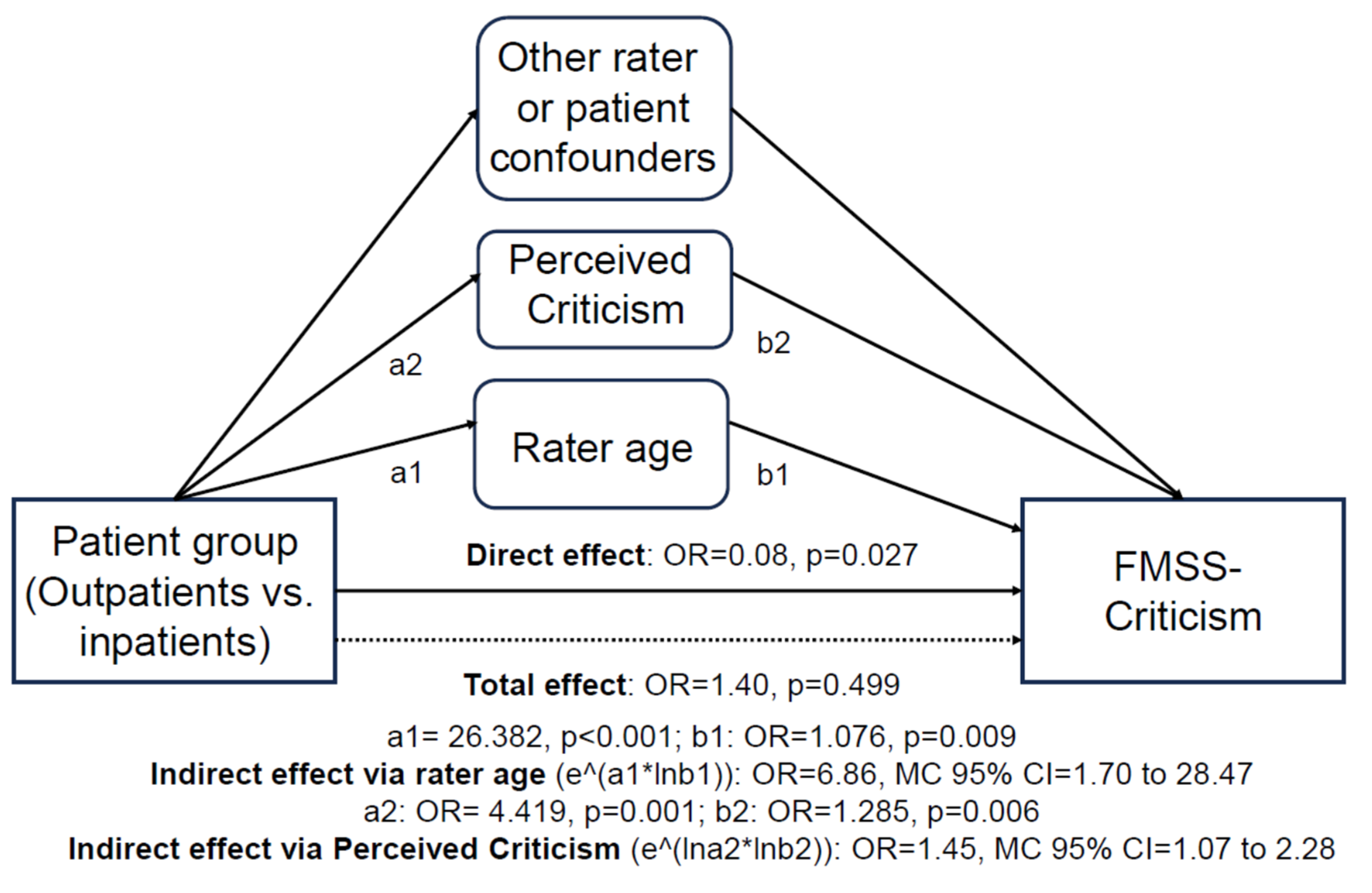
3.4.2. Patient- and Rater-Related Mediators of the Effect of Patient Group on EE outcomes
3.5. Post Hoc Empirical Power Calculations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, G.W.; Birley, J.L.; Wing, J.K. Influence of family life on the course of schizophrenic disorders: A replication. Br. J. Psychiatry 1972, 121, 241–258. [Google Scholar] [CrossRef]
- Alvarez-Jimenez, M.; Priede, A.; Hetrick, S.E.; Bendall, S.; Killackey, E.; Parker, A.G.; McGorry, P.D.; Gleeson, J.F. Risk factors for relapse following treatment for first episode psychosis: A systematic review and meta-analysis of longitudinal studies. Schizophr. Res. 2012, 139, 116–128. [Google Scholar] [CrossRef]
- Porcelli, S.; Bianchini, O.; De Girolamo, G.; Aguglia, E.; Crea, L.; Serretti, A. Clinical factors related to schizophrenia relapse. Int. J. Psychiatry Clin. Pract. 2016, 20, 54–69. [Google Scholar] [CrossRef]
- Vaughn, C.; Leff, J. The Measurement of Expressed Emotion in the Families of Psychiatric Patients. Br. J. Soc. Clin. Psychol. 1976, 15, 157–165. [Google Scholar] [CrossRef]
- Wearden, A.J.; Tarrier, N.; Barrowclough, C.; Zastowny, T.R.; Rahill, A.A. A review of expressed emotion research in health care. Clin. Psychol. Rev. 2000, 20, 633–666. [Google Scholar] [CrossRef]
- Hooley, J.M.; Parker, H.A. Measuring expressed emotion: An evaluation of the shortcuts. J. Fam. Psychol. 2006, 20, 386–396. [Google Scholar] [CrossRef]
- Butzlaff, R.L.; Hooley, J.M. Expressed emotion and psychiatric relapse: A meta-analysis. Arch. Gen. Psychiatry 1998, 55, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.F.; Chan, S.K.W.; Chung, Y.L.; Ng, S.M.; Hui, C.L.M.; Suen, Y.N.; Chen, E.Y.H. The predictive power of expressed emotion and its components in relapse of schizophrenia: A meta-analysis and meta-regression. Psychol. Med. 2021, 51, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.; Berry, K.; Varese, F.; Bucci, S. Are family warmth and positive remarks related to outcomes in psychosis? A systematic review. Psychol. Med. 2019, 49, 1250–1265. [Google Scholar] [CrossRef] [PubMed]
- Van Humbeeck, G.; Van Audenhove, C.; Pieters, G.; De Hert, M.; Storms, G.; Vertommen, H.; Peuskens, J.; Heyrman, J. Expressed emotion in the client-professional caregiver dyad: Are symptoms, coping strategies and personality related? Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 364–371. [Google Scholar] [CrossRef]
- Hooley, J.M.; Hiller, J.B. Personality and expressed emotion. J. Abnorm. Psychol. 2000, 109, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Barrowclough, C.; Haddock, G.; Lowens, I.; Connor, A.; Pidliswyj, J.; Tracey, N. Staff expressed emotion and causal attributions for client problems on a low security unit: An exploratory study. Schizophr. Bull. 2001, 27, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Barrowclough, C.; Johnston, M.; Tarrier, N. Attributions, expressed emotion, and patient relapse: An attributional model of relatives’ response to schizophrenic illness. Behav. Ther. 1994, 25, 67–88. [Google Scholar] [CrossRef]
- Hooley, J.M. Expressed emotion and locus of control. J. Nerv. Ment. Dis. 1998, 186, 374–378. [Google Scholar] [CrossRef]
- Amaresha, A.C.; Venkatasubramanian, G. Expressed emotion in schizophrenia: An overview. Indian J. Psychol. Med. 2012, 34, 12–20. [Google Scholar] [CrossRef]
- Kohler, C.G.; Walker, J.B.; Martin, E.A.; Healey, K.M.; Moberg, P.J. Facial emotion perception in schizophrenia: A meta-analytic review. Schizophr. Bull. 2010, 36, 1009–1019. [Google Scholar] [CrossRef]
- Weinreb, S.; Li, F.; Kurtz, M.M. A meta-analysis of social cognitive deficits in schizophrenia: Does world region matter? Schizophr. Res. 2022, 243, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, M.-A.; Plana, I.; Bédard Lacroix, J.; Godmaire-Duhaime, F.; Jackson, P.L.; Achim, A.M. Social cognition in first-degree relatives of people with schizophrenia: A meta-analysis. Psychiatry Res. 2013, 209, 129–135. [Google Scholar] [CrossRef]
- Muliyala, K.P.; Thirthalli, J. Expressed emotions and relapse of psychosis: New vistas for an old concept. Schizophr. Res. 2019, 209, 48–49. [Google Scholar] [CrossRef]
- Thonse, U.; Behere, R.V.; Praharaj, S.K.; Sharma, P. Facial emotion recognition, socio-occupational functioning and expressed emotions in schizophrenia versus bipolar disorder. Psychiatry Res. 2018, 264, 354–360. [Google Scholar] [CrossRef]
- McPherson, P.; Krotofil, J.; Killaspy, H. What Works? Toward a New Classification System for Mental Health Supported Accommodation Services: The Simple Taxonomy for Supported Accommodation (STAX-SA). Int. J. Environ. Res. Public Health 2018, 15, 190. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.; Barrowclough, C.; Haddock, G. The role of expressed emotion in relationships between psychiatric staff and people with a diagnosis of psychosis: A review of the literature. Schizophr. Bull. 2011, 37, 958–972. [Google Scholar] [CrossRef] [PubMed]
- Snyder, K.S.; Wallace, C.J.; Moe, K.; Liberman, R.P. Expressed Emotion by Residential Care Operators and Residents’ Symptoms and Quality of Life. Psychiatr. Serv. 1994, 45, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Tattan, T.; Tarrier, N. The expressed emotion of case managers of the seriously mentally ill: The influence of expressed emotion on clinical outcomes. Psychol. Med. 2000, 30, 195–204. [Google Scholar] [CrossRef]
- Ball, R.A.; Moore, E.; Kuipers, L. Expressed emotion in community care staff: A comparison of patient outcome in a 9-month follow-up of two hostels. Soc. Psychiatry Psychiatr. Epidemiol. 1992, 27, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Ketola, J.; Jahangiri, E.; Hakko, H.; Riipinen, P.; Räsänen, S. Assisted living for mentally ill—A systematic literature review and its recommendations. Nord. J. Psychiatry 2022, 76, 403–422. [Google Scholar] [CrossRef] [PubMed]
- McPherson, P.; Krotofil, J.; Killaspy, H. Mental health supported accommodation services: A systematic review of mental health and psychosocial outcomes. BMC Psychiatry 2018, 18, 128. [Google Scholar] [CrossRef]
- First, M.; Williams, J.; Karg, R.; Spitzer, R. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2016. [Google Scholar]
- Overall, J.E.; Gorham, D.R. The Brief Psychiatric Rating Scale. Psychol. Rep. 1962, 10, 799–812. [Google Scholar] [CrossRef]
- Burger, G.K.; Calsyn, R.J.; Morse, G.A.; Klinkenberg, W.D.; Trusty, M.L. Factor structure of the expanded Brief Psychiatric Rating Scale. J. Clin. Psychol. 1997, 53, 451–454. [Google Scholar] [CrossRef]
- Hooley, J.M.; Teasdale, J.D. Predictors of relapse in unipolar depressives: Expressed emotion, marital distress, and perceived criticism. J. Abnorm. Psychol. 1989, 98, 229–235. [Google Scholar] [CrossRef]
- Medina-Pradas, C.; Navarro, J.B.; Pousa, E.; Montero, M.I.; Obiols, J.E. Expressed and perceived criticism, family warmth, and symptoms in schizophrenia. Span. J. Psychol. 2013, 16, E45. [Google Scholar] [CrossRef] [PubMed]
- Onwumere, J.; Kuipers, E.; Bebbington, P.; Dunn, G.; Freeman, D.; Fowler, D.; Garety, P. Patient perceptions of caregiver criticism in psychosis: Links with patient and caregiver functioning. J. Nerv. Ment. Dis. 2009, 197, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Magaña, A.B.; Goldstein, J.M.; Karno, M.; Miklowitz, D.J.; Jenkins, J.; Falloon, I.R. A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Res. 1986, 17, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: Boston, MA, USA, 2013. [Google Scholar]
- Lash, T.L.; VanderWeele, T.J.; Haneuse, S.; Rothman, K.J. Modern Epidemiology, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Preacher, K.J.; Zyphur, M.J.; Zhang, Z. A general multilevel SEM framework for assessing multilevel mediation. Psychol. Methods 2010, 15, 209–233. [Google Scholar] [CrossRef] [PubMed]
- Westfall, J.; Kenny, D.A.; Judd, C.M. Statistical power and optimal design in experiments in which samples of participants respond to samples of stimuli. J. Exp. Psychol. Gen. 2014, 143, 2020–2045. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage Publications: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Olivier, J.; May, W.L.; Bell, M.L. Relative effect sizes for measures of risk. Commun. Stat. Theory Methods 2017, 46, 6774–6781. [Google Scholar] [CrossRef]
- Kumle, L.; Võ, M.L.; Draschkow, D. Estimating power in (generalized) linear mixed models: An open introduction and tutorial in R. Behav. Res. Methods 2021, 53, 2528–2543. [Google Scholar] [CrossRef]
- Leucht, S.; Kane, J.M.; Kissling, W.; Hamann, J.; Etschel, E.; Engel, R. Clinical implications of Brief Psychiatric Rating Scale scores. Br. J. Psychiatry 2005, 187, 366–371. [Google Scholar] [CrossRef]
- Moore, E.; Ball, R.A.; Kuipers, L. Expressed emotion in staff working with the long-term adult mentally ill. Br. J. Psychiatry 1992, 161, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Oliver, N.; Kuipers, E. Stress and its relationship to expressed emotion in community mental health workers. Int. J. Soc. Psychiatry 1996, 42, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, D.J. Recent developments in expressed emotion and schizophrenia. Br. J. Psychiatry 1992, 160, 601–620. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Kuipers, L. Behavioural correlates of expressed emotion in staff-patient interactions. Soc. Psychiatry Psychiatr. Epidemiol. 1992, 27, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Yates, M.; Mallindine, C.; Ryan, S.; Jackson, S.; Chinnon, N.; Kuipers, E.; Hammond, S. Expressed Emotion in relationships between staff and patients in forensic services: Changes in relationship status at 12 month follow-up. Leg. Criminol. Psychol. 2002, 7, 203–218. [Google Scholar] [CrossRef]
- Francis, A.; Papageorgiou, P. Expressed emotion in Greek versus Anglo-Saxon families of individuals with schizophrenia. Aust. Psychol. 2004, 39, 172–177. [Google Scholar] [CrossRef]
- Singh, S.P.; Harley, K.; Suhail, K. Cultural Specificity of Emotional Overinvolvement: A Systematic Review. Schizophr. Bull. 2013, 39, 449–463. [Google Scholar] [CrossRef]
- Alvarez-Jiménez, M.; Gleeson, J.F.; Cotton, S.M.; Wade, D.; Crisp, K.; Yap, M.B.; McGorry, P.D. Differential predictors of critical comments and emotional over-involvement in first-episode psychosis. Psychol. Med. 2010, 40, 63–72. [Google Scholar] [CrossRef]
- Hinojosa-Marqués, L.; Domínguez-Martínez, T.; Kwapil, T.R.; Barrantes-Vidal, N. Predictors of criticism and emotional over-involvement in relatives of early psychosis patients. PLoS ONE 2020, 15, e0234325. [Google Scholar] [CrossRef]
- Van Humbeeck, G.; Van Audenhove, C.; Pieters, G.; De Hert, M.; Storms, G.; Vertommen, H.; Peuskens, J.; Heyrman, J. Expressed emotion in staff-patient relationships: The professionals’ and residents’ perspectives. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Tompson, M.C.; Goldstein, M.J.; Lebell, M.B.; Mintz, L.I.; Marder, S.R.; Mintz, J. Schizophrenic patients’ perceptions of their relatives’ attitudes. Psychiatry Res. 1995, 57, 155–167. [Google Scholar] [CrossRef]
- Wei, Y.; Peng, Y.; Li, Y.; Song, L.; Ju, K.; Xi, J. Caregivers’ burden and schizophrenia patients’ quality of life: Sequential mediating effects of expressed emotion and perceived expressed emotion. Front. Psychiatry 2022, 13, 961691. [Google Scholar] [CrossRef]
- Levy, E.; Shefler, G.; Loewenthal, U.; Umansky, R.; Bar, G.; Heresco-Levy, U. Characteristics of schizophrenia residents and staff rejection in community mental health hostels. Isr. J. Psychiatry Relat. Sci. 2005, 42, 23–32. [Google Scholar]
- Bentsen, H.; Notland, T.H.; Boye, B.; Munkvold, O.G.; Bjørge, H.; Lersbryggen, A.B.; Uren, G.; Oskarsson, K.H.; Berg-Larsen, R.; Lingjaerde, O.; et al. Criticism and hostility in relatives of patients with schizophrenia or related psychoses: Demographic and clinical predictors. Acta Psychiatr. Scand. 1998, 97, 76–85. [Google Scholar] [CrossRef]
- da Silva, A.H.S.; de Souza Tressoldi, L.; de Azevedo-Marques, J.M.; Shuhama, R.; Del-Ben, C.M.; Galera, S.A.F.; da Silva Gherardi-Donato, E.C.; Vedana, K.G.G.; Zanetti, A.C.G. Predictors of Expressed Emotion in First Episode Psychosis. Issues Ment. Health Nurs. 2020, 41, 908–915. [Google Scholar] [CrossRef]
- Zanetti, A.C.G.; Vedana, K.G.G.; Pereira, C.C.M.; de Azevedo Marques, J.M.; da Silva, A.H.S.; Martin, I.d.S.; Dantas, R.A.S.; de Souza, J.; Galera, S.A.F.; Gherardi-Donato, E.C.d.S. Expressed emotion and socio-demographic and clinical factors in families of Brazilian patients with schizophrenia. Int. J. Soc. Psychiatry 2019, 65, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Bentsen, H.; Boye, B.; Munkvold, O.G.; Notland, T.H.; Lersbryggen, A.B.; Oskarsson, K.H.; Ulstein, I.; Uren, G.; Bjørge, H.; Berg-Larsen, R.; et al. Emotional overinvolvement in parents of patients with schizophrenia or related psychosis: Demographic and clinical predictors. Br. J. Psychiatry 1996, 169, 622–630. [Google Scholar] [CrossRef]
- Koutra, K.; Triliva, S.; Roumeliotaki, T.; Lionis, C.; Vgontzas, A.N. Identifying the socio-demographic and clinical determinants of family functioning in Greek patients with psychosis. Int. J. Soc. Psychiatry 2015, 61, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.J.; Docherty, N.M. Parent coping styles and schizophrenic patient behavior as predictors of expressed emotion. Fam. Process 2000, 39, 435–444. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Avraam, G.; Samakouri, M.; Tzikos, A.; Arvaniti, A. High Expressed Emotion and Warmth among Families of Patients with Schizophrenia in Greece. Healthcare 2022, 10, 1957. [Google Scholar] [CrossRef]
- Lee, E.E.; Martin, A.S.; Kaufmann, C.N.; Liu, J.; Kangas, J.; Daly, R.E.; Tu, X.M.; Depp, C.A.; Jeste, D.V. Comparison of schizophrenia outpatients in residential care facilities with those living with someone: Study of mental and physical health, cognitive functioning, and biomarkers of aging. Psychiatry Res. 2019, 275, 162–168. [Google Scholar] [CrossRef]
- Willetts, L.E.; Leff, J. Expressed emotion and schizophrenia: The efficacy of a staff training programme. J. Adv. Nurs. 1997, 26, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Falloon, I.R. Family interventions for mental disorders: Efficacy and effectiveness. World Psychiatry 2003, 2, 20–28. [Google Scholar] [PubMed]
- Rodolico, A.; Bighelli, I.; Avanzato, C.; Concerto, C.; Cutrufelli, P.; Mineo, L.; Schneider-Thoma, J.; Siafis, S.; Signorelli, M.S.; Wu, H.; et al. Family interventions for relapse prevention in schizophrenia: A systematic review and network meta-analysis. Lancet Psychiatry 2022, 9, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Koomen, L.E.M.; van der Horst, M.Z.; Deenik, J.; Cahn, W. Lifestyle interventions for people with a severe mental illness living in supported housing: A systematic review and meta-analysis. Front. Psychiatry 2022, 13, 966029. [Google Scholar] [CrossRef]
- McPherson, P.; Lloyd-Evans, B.; Dalton-Locke, C.; Killaspy, H. A Systematic Review of the Characteristics and Efficacy of Recovery Training for Mental Health Staff: Implications for Supported Accommodation Services. Front. Psychiatry 2021, 12, 624081. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Inpatients N = 40 | Outpatients N = 40 | p-Value | |
|---|---|---|---|
| Sex (Male) | 27 (67.5%) | 22 (55.0%) | 0.251 a |
| Age (years) | 48.6 ± 9.3 | 40.1 ± 7.8 | <0.001 c |
| Family status | 1.000 b | ||
| Single | 34 (85.0%) | 33 (82.5%) | |
| Married | 1 (2.5%) | 2 (5.0%) | |
| Divorced/Widowed | 5 (12.5%) | 5 (12.5%) | |
| Education | 0.002 a | ||
| Primary/High School | 33 (82.5%) | 20 (50.0%) | |
| University or higher | 7 (17.5%) | 20 (50.0%) | |
| Employment | 0.762 b | ||
| Employed | 7 (17.5%) | 10 (25.0%) | |
| Unemployed | 30 (75.0%) | 27 (67.5%) | |
| Retired | 3 (7.5%) | 3 (7.5%) | |
| Smoking | 28 (70.0%) | 24 (60.0%) | 0.348 a |
| History of violent behavior | 14 (35.0%) | 10 (25.0%) | 0.329 a |
| History of suicide attempts | 3 (7.5%) | 3 (7.5%) | 1.000 b |
| Duration of disease (years) | 18.2 ± 10.9 | 13.4 ± 7.2 | 0.025 c |
| No. of hospitalizations | 2 (2–4) | 2 (1–3) | 0.012 d |
| BPRS Thinking disorder | 5 (4–7.5) | 6.5 (5–9.5) | 0.190 d |
| BPRS Withdrawal | 6 (4–8) | 8.5 (6–11.5) | 0.015 d |
| BPRS Anxiety/Depression | 7.5 (6–9.5) | 9 (6.5–12) | 0.162 d |
| BPRS Hostility/Suspicion | 4 (3–5.5) | 4 (3–6.5) | 0.964 d |
| BPRS Activity | 3 (3–4) | 3 (3–4.5) | 0.345 d |
| BPRS Total | 28 (22.5–37) | 33.5 (28.5–40.5) | 0.027 d |
| Perceived Criticism | 3.7 ± 2.4 | 5.80 ± 2.66 | <0.001 c |
| Nurses (N = 22) | Parents (N = 56) | ||
| Sex (Male) | 6 (27.3%) | 24 (42.9%) | 0.203 a |
| Age (years) | 40.0 ± 7.2 | 68.0 ± 8.6 | <0.001 c |
| Education | 0.007 a | ||
| Primary/High School | 8 (36.4%) | 39 (69.6%) | |
| University or higher | 14 (63.6%) | 17 (30.4%) |
| Five Minutes Speech Sample (FMSS) Outcomes | Nurses | Parents | p-Value |
|---|---|---|---|
| Criticism | 0.310 a† | ||
| High | 84 (54.2%) | 33 (58.9%) | |
| Borderline | 65 (41.9%) | 23 (41.1%) | |
| Low | 6 (3.9%) | 0 (0.0%) | |
| Emotional Overinvolvement (EOI) | 0.940 b†† | ||
| High | 72 (46.5%) | 27 (48.2%) | |
| Borderline | 65 (41.9%) | 22 (39.3%) | |
| Low | 18 (11.6%) | 7 (12.5%) | |
| EE Categories (n = 7) | 0.049 a§ | ||
| High critical | 54 (34.8%) | 17 (30.4%) | |
| High EOI | 42 (27.1%) | 11 (19.6%) | |
| High critical + EOI | 30 (19.4%) | 16 (28.6%) | |
| Borderline critical | 1 (0.6%) | 4 (7.1%) | |
| Borderline EOI | 0 (0.0%) | 0 (0.0%) | |
| Borderline critical + EOI | 28 (18.1%) | 8 (14.3%) | |
| Low critical + EOI | 0 (0.0%) | 0 (0.0%) | |
| EE Categories (n = 2) | 0.659 b | ||
| High EE | 126 (81.3%) | 44 (78.6%) | |
| Low EE | 29 (18.7%) | 12 (21.4%) |
| Inpatients (N = 155 Ratings) | Outpatients (N = 56 Ratings) | p-Value | ||
|---|---|---|---|---|
| FMSS-Criticism | ||||
| Critical comments | 1.55 ± 2.40 | 1.12 ± 1.94 | 0.446 a | |
| Critical comments ≥ 1 | 59 (38.1%) | 20 (35.7%) | 0.755 b | |
| Dissatisfaction comments | 3.54 ± 2.47 | 3.00 ± 2.00 | 0.241 a | |
| Dissatisfaction comments ≥1 | 138 (89.0%) | 48 (85.7%) | 0.510 b | |
| Initial statement | Negative | 38 (24.5%) | 15 (26.8%) | 0.217 b |
| Neutral | 64 (41.3%) | 16 (28.6%) | ||
| Positive | 53 (34.2%) | 25 (44.6%) | ||
| Quality of relationship | Negative | 59 (38.1%) | 21 (37.5%) | 0.717 b |
| Neutral | 16 (10.3%) | 8 (14.3%) | ||
| Positive | 80 (51.6%) | 27 (48.2%) | ||
| FMSS-EOI | ||||
| Positive attitude statements | 0.55 ± 0.82 | 0.89 ± 0.87 | 0.003 a | |
| Positive attitude statements ≥ 1 | 59 (38.1%) | 35 (62.5%) | 0.002 b | |
| Positive comments | 7.10 ± 3.53 | 4.61 ± 3.33 | <0.001 a | |
| Positive comments ≥ 5 | 115 (74.2%) | 26 (46.4%) | <0.001 b | |
| Self-sacrificing or overprotective behavior | 0 (0%) | 4 (7.1%) | 0.005 c | |
| Intense emotional display during interview | 1 (0.6%) | 7 (12.5%) | <0.001 c | |
| Excessive detail about the past | 53 (34.2%) | 9 (16.1%) | 0.011 b |
| FMSS—Criticism (OR, p) | FMSS Critical Comments (IRR, p) | FMSS—EOI (OR, p) | FMSS Positive Attitude Statements (IRR, p) | |
|---|---|---|---|---|
| Patient Predictors | Logit, Patients | NB, Patients | Logit, Patients | Poisson, Patients |
| Group (outpatients vs. inpatients) | 1.40, 0.499 | 0.72, 0.319 | 1.15, 0.768 | 1.69, 0.019 |
| Sex (female vs. male) | 1.73, 0.014 | |||
| Age (years) | 1.06, 0.011 | |||
| Family status (ever married vs. single) | ||||
| Education (university or higher vs. lower) | 2.38, 0.092 | |||
| Employment (Ref. employed) | Unemployed: 0.40, 0.006 Pensioner: - | Unemployed: 4.46, 0.006 Pensioner: 7.25, 0.025 | ||
| Smoking | ||||
| Disease duration (years) | ||||
| No. of previous hospitalizations | ||||
| History of violent behavior | ||||
| History of suicide attempts | ||||
| BPRS Thinking disorder | 0.87, 0.025 | |||
| BPRS Withdrawal | 1.09, 0.032 | 0.84, 0.004 | ||
| BPRS Anxiety/Depression | ||||
| BPRS Hostility/Suspicion | 0.77, 0.026 | |||
| BPRS Activity | 0.73, 0.027 | |||
| BPRS Total | 0.93, 0.00048 * | 0.98, 0.090 | ||
| Perceived Criticism | 1.26, 0.013 | 0.86, 0.090 |
| FMSS—Criticism (OR, p) | FMSS Critical Comments (IRR, p) | FMSS—EOI (OR, p) | FMSS Positive Attitude Statements (IRR, p) | |
|---|---|---|---|---|
| Patient predictors | Logit, Patients | NB, Patients | Logit, Patients | Poisson, Patients |
| Group (outpatients vs. inpatients) | 0.71, 0.577 0.08, 0.027 | 0.52, 0.105 0.16, 0.035 | 2.79, 0.027 1.49, 0.644 | 2.61, 0.00031 * 1.40, 0.486 |
| Sex (female vs. male) | 1.48, 0.050 1.48, 0.049 | |||
| Age (years) | 0.99, 0.775 0.95, 0.199 | 1.01, 0.503 0.99, 0.680 | 1.07, 0.006 1.05, 0.052 | 1.00, 0.920 0.99, 0.489 |
| Family status (ever married vs. single) | ||||
| Education (university or higher vs. lower) | 1.07, 0.895 1.26, 0.681 | 0.88, 0.741 0.93, 0.837 | 1.35, 0.453 1.52, 0.317 | 0.87, 0.519 0.91, 0.649 |
| Employment (Ref. employed) | Unemployed: 0.55, 0.087 0.49, 0.046 Pensioner: 1.74, 0.329 1.68, 0.345 | Unemployed: 4.09, 0.005 4.37, 0.005 Pensioner: 3.37, 0.109 3.57, 0.108 | ||
| Smoking | ||||
| Disease duration (years) | 1.00, 0.980 1.01, 0.659 | 0.98, 0.385 0.99, 0.710 | 0.96, 0.053 0.96, 0.131 | 1.01, 0.420 1.01, 0.293 |
| No. of previous hospitalizations | 1.04, 0.698 1.01, 0.881 | 1.06, 0.254 1.05, 0.381 | 1.15, 0.044 1.14, 0.076 | 1.02, 0.525 1.02, 0.637 |
| History of violent behavior | ||||
| History of suicide attempts | ||||
| BPRS Thinking disorder | 0.94, 0.303 0.93, 0.268 | |||
| BPRS Withdrawal | 1.06, 0.373 1.09, 0.199 | 1.07, 0.108 1.10, 0.023 | 0.87, 0.020 0.87, 0.027 | 0.93, 0.032 0.94, 0.058 |
| BPRS Anxiety/Depression | ||||
| BPRS Hostility/Suspicion | 0.86, 0.131 0.86, 0.152 | |||
| BPRS Activity | 0.99, 0.914 1.04, 0.781 | |||
| Perceived Criticism | 1.06, 0.023 1.27, 0.023 | 1.15, 0.024 1.18, 0.010 | 1.01, 0.939 1.02, 0.766 | 0.91, 0.022 0.90, 0.018 |
| Rater predictors | ||||
| Age (years) | - 1.08, 0.021 | - 1.04, 0.108 | - 1.03, 0.268 | - 1.02, 0.156 |
| Sex (female vs. male) | - 2.14, 0.076 | - 2.45, 0.008 | - 3.23, 0.003 | - 1.37, 0.156 |
| Education (university or higher vs. lower) | - 0.99, 0.973 | - 1.22, 0.502 | - 1.17, 0.644 | - 0.91, 0.592 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferentinos, P.; Douki, S.; Yotsidi, V.; Kourkouni, E.; Dragoumi, D.; Smyrnis, N.; Douzenis, A. Family in Crisis: Do Halfway Houses Perform Better Than Families with Expressed Emotion toward Patients with Schizophrenia? A Direct Adjusted Comparison. Healthcare 2024, 12, 375. https://doi.org/10.3390/healthcare12030375
Ferentinos P, Douki S, Yotsidi V, Kourkouni E, Dragoumi D, Smyrnis N, Douzenis A. Family in Crisis: Do Halfway Houses Perform Better Than Families with Expressed Emotion toward Patients with Schizophrenia? A Direct Adjusted Comparison. Healthcare. 2024; 12(3):375. https://doi.org/10.3390/healthcare12030375
Chicago/Turabian StyleFerentinos, Panagiotis, Stamatina Douki, Vasiliki Yotsidi, Eleni Kourkouni, Dimitra Dragoumi, Nikolaos Smyrnis, and Athanasios Douzenis. 2024. "Family in Crisis: Do Halfway Houses Perform Better Than Families with Expressed Emotion toward Patients with Schizophrenia? A Direct Adjusted Comparison" Healthcare 12, no. 3: 375. https://doi.org/10.3390/healthcare12030375
APA StyleFerentinos, P., Douki, S., Yotsidi, V., Kourkouni, E., Dragoumi, D., Smyrnis, N., & Douzenis, A. (2024). Family in Crisis: Do Halfway Houses Perform Better Than Families with Expressed Emotion toward Patients with Schizophrenia? A Direct Adjusted Comparison. Healthcare, 12(3), 375. https://doi.org/10.3390/healthcare12030375