
An Inclusive Framework for Collaboration between Midwives and Traditional Birth Attendants and Optimising Maternal and Child Healthcare in Restricted Rural Communities in South Africa: Policy Considerations

 , , and
, , and
Abstract
1. Introduction
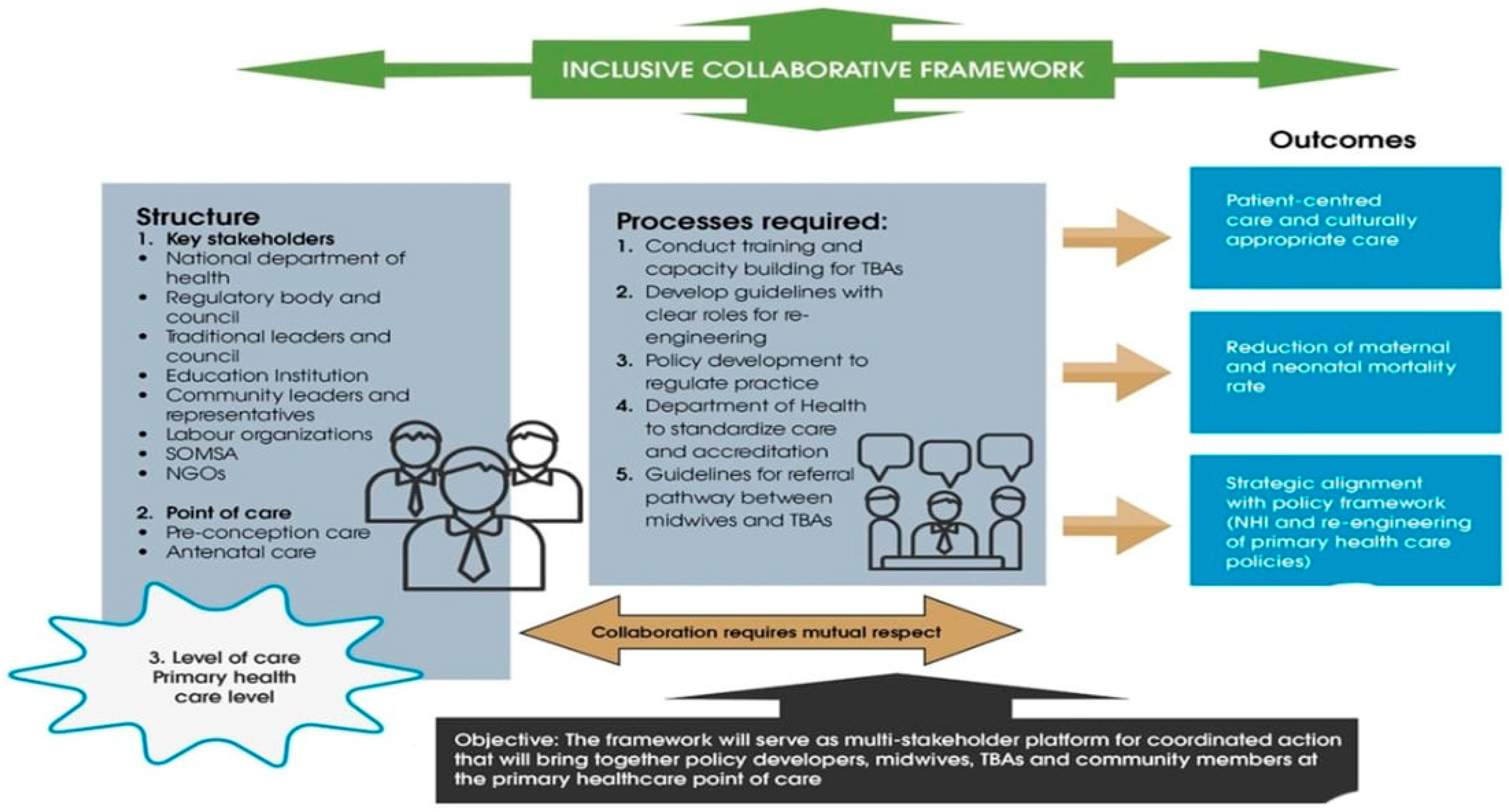
1.1. SPO Donabedian Framework
1.1.1. Structure
1.1.2. Processes
1.1.3. Outcome
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Sampling Strategy
2.4. Data Collection Procedure
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Characteristics of Study Participants
3.2. Nominal Group Ranking
3.2.1. Structure
“The framework will serve as a multi-stakeholder platform for coordinated action that will bring together policy developers, midwives, TBAs and community members at the primary healthcare point of care”.All stakeholders
“The National Department of Health as policymakers will be responsible for policy development and ensuring relevant guidelines are developed to facilitate the collaboration between traditional birth attendants and midwives”.
“The education institutions will be responsible for facilitating the training and developing the curriculum for the traditional birth attendants”.
“During antenatal care, the traditional birth attendants can be responsible for screening for pregnancy-related problems, assessing and referring high risk women to the antenatal clinics and providing information to the women to prepare for childbirth”.
…. Within the primary healthcare level, the TBAs can manage low-risk antenatal care women and refer them to the nearest clinic when dangers and problems are encountered during pregnancy”.
“We work almost the same as the community workers that visit the women at home; we also either make home visits or ask the mother to come to the indaba (sacred healing hut) after homebirths and being seen in the hospital. But mostly, we need to volunteer as traditional birth attendants to work as part of the ward-based teams”.TBA
3.2.2. Process
“The regulatory councils of the traditional birth attendants (Traditional Health Organisation) and the midwives (South African nursing council) are responsible for regulating and registering the practitioners once the policy to govern their practice has been implemented”.
3.2.3. Outcomes
“Pregnant women respect the care we provide to them during pregnancy as it is according to their culture and traditional beliefs”TBA
“If we work together, we can save more lives and help a lot of mothers that are dying during birth”TBA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, T.; Smith, H. Establishing partnership with traditional birth attendants for improved maternal and newborn health: A review of factors influencing implementation. BMC Pregnancy Childbirth 2017, 17, 365. [Google Scholar] [CrossRef]
- van Rooyen, R.M.D.; Pretorius, B.; Tembani, N.M.; ten Ham-Baloyi, W. Evidence-based recommendations to facilitate professional collaboration between allopathic and traditional health practitioners. Health SA Gesondheid 2017, 22, 291–299. [Google Scholar] [CrossRef]
- Turinawe, E.B.; Rwemisisi, J.T.; Musinguzi, L.K.; de Groot, M.; Muhangi, D.; de Vries, D.H.; Mafigiri, D.K.; Katamba, A.; Parker, N.; Pool, R. Traditional birth attendants (TBAs) as potential agents in promoting male involvement in maternity preparedness: Insights from a rural community in Uganda. Reprod. Health 2016, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Recommendations: Optimizing Health Worker Roles to Improve Access to Key Maternal and Newborn Health Interventions through Task Shifting; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Working with Individuals, Families and Communities to Improve Maternal and Newborn Health: A Toolkit for Implementation; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Graham, S.; Davis-Floyd, R. Indigenous midwives and the biomedical system among the Karamojong of Uganda: Introducing the Partnership Paradigm. Front. Sociol. 2021, 6, 670551. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Declaration of Alma-Ata (No. WHO/EURO: 1978-3938-43697-61471); World Health Organization, Regional Office for Europe: Geneva, Switzerland, 1978. [Google Scholar]
- Choguya, N.Z. Traditional and skilled birth attendants in Zimbabwe: A situational analysis and some policy considerations. J. Anthropol. 2015, 2015, 215909. [Google Scholar] [CrossRef]
- Musie, M.R.; Mulaudzi, M.F.; Anokwuru, R.; Bhana-Pema, V. Recognise and Acknowledge Us: Views of Traditional Birth Attendants on Collaboration with Midwives for Maternal Health Care Services. Int. J. Reprod. Med. 2022, 2022, 9216500. [Google Scholar] [CrossRef]
- Ntoimo, L.F.C.; Okonofua, F.E.; Ekwo, C.; Solanke, T.O.; Igboin, B.; Imongan, W.; Yaya, S. Why women utilize traditional rather than skilled birth attendants for maternity care in rural Nigeria: Implications for policies and programs. Midwifery 2022, 104, 103158. [Google Scholar] [CrossRef]
- Matlala, S.F. An assessment of traditional birth attendants as an untapped human resource to help sustain the health system in South Africa. Int. J. Dev. Sustain. 2023, 12, 39–51. [Google Scholar]
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- South African Department of Health. Traditional Health Practitioners Act 22 of 2007; Department of Health: Pretoria, South Africa, 2007.
- Peltzer, K. Traditional health practitioners in South Africa. Lancet 2009, 374, 956–957. [Google Scholar] [CrossRef]
- Michel, J.; Tediosi, F.; Egger, M.; Barnighausen, T.; McIntyre, D.; Tanner, M.; Evans, D. Universal health coverage financing in South Africa: Wishes vs reality. J. Glob. Health Rep. 2020, 4, e2020061. [Google Scholar] [CrossRef]
- Department of Health. National Health Insurance for South Africa. Towards Universal Health Coverage. 2017. Available online: https://www.gov.za/documents/national-health-act-national-health-insurance-policy-towards-universal-health-coverage-30 (accessed on 10 November 2023).
- Nemutandani, S.M.; Hendricks, S.J.; Mulaudzi, M.F. Perceptions and experiences of allopathic health practitioners on collaboration with traditional health practitioners in post-apartheid South Africa. Afr. J. Prim. Health Care Fam. Med. 2016, 8, 1007. [Google Scholar] [CrossRef]
- Nemutandani, M.S. A Model for Collaboration between Allopathic and Traditional Health Practitioners in the Management of HIV/AIDS and TB Patients in Vhembe District, Limpopo Province. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2016. [Google Scholar]
- Templeman, K.; Robinson, A. Integrative medicine models in contemporary primary health care. Complement. Ther. Med. 2011, 19, 84–92. [Google Scholar] [CrossRef]
- Chi, P.C.; Urdal, H. The evolving role of traditional birth attendants in maternal health in post-conflict Africa: A qualitative study of Burundi and northern Uganda. SAGE Open Med. 2018, 6, 2050312117753631. [Google Scholar] [CrossRef] [PubMed]
- Hermawan, R. Midwives and Traditional Birth Attendants (TBAs) Partnership Program in Indonesia: A Proposed for National Guidelines. Master’s Thesis, Georgia State University, Atlanta, GA, USA, 2016. [Google Scholar]
- Jiang, H.; Qian, X.; Chen, L.; Li, J.; Escobar, E.; Story, M.; Tang, S. Towards universal access to skilled birth attendance: The process of transforming the role of traditional birth attendants in Rural China. BMC Pregnancy Childbirth 2016, 16, 58. [Google Scholar] [CrossRef]
- SulaymanH, A. Integration of traditional birth attendants (TBAs) into the health sector for improving maternal health in Nigeria: A systematic review. Sub-Sahar. Afr. J. Med. 2019, 6, 55–62. [Google Scholar]
- Tossaint-Schoenmakers, R.; Versluis, A.; Chavannes, N.; Talboom-Kamp, E.; Kasteleyn, M. The challenge of integrating eHealth into health care: Systematic literature review of the Donabedian model of structure, process, and outcome. J. Med. Internet Res. 2021, 23, e27180. [Google Scholar] [CrossRef]
- Sarani, M.; Saravani, S. Assessment of prenatal care process based on donabedian model in Zabol city. J. Pharm. Sci. Res. 2017, 9, 2558–2563. [Google Scholar]
- Naz, S.; Saleem, S.; Islam, Z.S.; Bhamani, S.; Sheikh, L. Obstetric triage improvement process using the Donabedian model of quality care: A quality improvement initiative. BMJ Open Qual. 2022, 11, e001483. [Google Scholar] [CrossRef]
- Sepeng, N.V.; Makhado, T.G.; Makhado, L. Conceptual framework for rape survivors diagnosed with PTSD in the North-West Province of South Africa. Healthcare 2022, 11, 127. [Google Scholar] [CrossRef]
- Harvey, N.; Holmes, C.A. Nominal group technique: An effective method for obtaining group consensus. Int. J. Nurs. Pract. 2012, 18, 188–194. [Google Scholar] [CrossRef]
- Van De, A.; Delbecq, A.L. Nominal versus interacting group processes for committee decision-making effectiveness. Acad. Manag. J. 1971, 14, 203–212. [Google Scholar] [CrossRef]
- Hugé, J.; Mukherjee, N. The nominal group technique in ecology & conservation: Application and challenges. Methods Ecol. Evol. 2018, 9, 33–41. [Google Scholar]
- Polit, D.; Beck, C. Essentials of Nursing Research: Appraising Evidence for Nursing Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- National Maternity Guidelines Committee. Guidelines for Maternity Care in South Africa; South African National Department of Health: Pretoria, South Africa, 2015.
- Haruna, U.; Kansanga, M.M.; Bagah, D.A. Repositioning traditional birth attendants to provide improved maternal healthcare services in rural Ghana. Int. J. Health Plan. Manag. 2019, 34, e987–e994. [Google Scholar] [CrossRef]
- Ohaja, M.; Murphy-Lawless, J. Unilateral collaboration: The practices and understandings of traditional birth attendants in southeastern Nigeria. Women Birth 2017, 30, e165–e171. [Google Scholar] [CrossRef]
- Haruna, U.; Kansanga, M.M.; Galaa, S. Examining the unresolved conundrum of Traditional Birth Attendants’ involvement in maternal and child health care delivery in Ghana. Health Care Women Int. 2019, 40, 1336–1354. [Google Scholar] [CrossRef] [PubMed]
- Davis-Floyd, R. Mutual accommodation or biomedical hegemony? A brief anthropological overview of global issues in midwifery. In Ways of Knowing about Birth: Mothers, Midwives, Medicine, and Birth Activism by Davis-Floyd; Long, R., Ed.; Waveland Press: Grove, IL, USA, 2018; pp. 265–282. [Google Scholar]
- Hernandez, S.; Oliveira, J.B.; Shirazian, T. How a training program is transforming the role of traditional birth attendants from cultural practitioners to unique health-care providers: A community case study in rural Guatemala. Front. Public Health 2017, 5, 111. [Google Scholar] [CrossRef] [PubMed]
- Ohaja, M.; Murphy-Lawless, J.; Dunlea, M. Midwives’ views of traditional birth attendants within formal healthcare in Nigeria. Women Birth 2020, 33, e111–e116. [Google Scholar] [CrossRef] [PubMed]
- Sibley, L.M.; Tesfaye, S.; Fekadu Desta, B.; Hailemichael Frew, A.; Kebede, A.; Mohammed, H.; Ethier-Stover, K.; Dynes, M.; Barry, D.; Hepburn, K.; et al. Improving maternal and newborn health care delivery in rural amhara and oromiya regions of ethiopia through the maternal and newborn health in ethiopia partnership. J. Midwifery Women’s Health 2014, 59, S6–S20. [Google Scholar] [CrossRef]
- Garces, A.; McClure, E.M.; Espinoza, L.; Saleem, S.; Figueroa, L.; Bucher, S.; Goldenberg, R.L. Traditional birth attendants and birth outcomes in low-middle income countries: A review. Semin. Perinatol. 2019, 43, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Oyeneyin, L.; Osunmakinwa, O.; Olagbuji, Y. Incorporating traditional birth attendants into the mainstream maternal health system in Nigeria-An evaluation of the Ondo State Agbebiye program. Afr. J. Reprod. Health 2021, 25, 82–88. [Google Scholar] [PubMed]

{kind=link}
| Steps | Description of Steps | Time Frame |
|---|---|---|
| 1 | Introduction and explanation of the nominal technique process [28]. The researcher explained the 3 components of the SPO Donabedian framework to orientate the participants. | Lasted 15 min |
| 2 | Nominal or Silent Generation of ideas The PI posed the following question to start the workshop: What should a framework for collaboration between the midwives and TBAs for maternal health care services in South Africa entail? Participants were asked to note down the ideas that came to mind of the central question posed. Discussions were prohibited in this step, but the facilitator gave attention to those seeking clarity. | Lasted 30 min |
| 3 | Round-robin: Clarification of items and sharing of ideas. Each member of the group was given time to share their ideas with the group. These were grouped according to the structure, process, and outcome of the Donabedian framework as they emerged, and ideas were written down on the A3 flip charts. | Lasted 60 min |
| 4 | Discussion and presentation of ideas for consensus The facilitator encouraged questions and discussion during this period. This process was also used as an opportunity to probe the presenters for further explanations, as well as for the wider team to discuss and clarify presented ideas. | Lasted 120 min |
| 5 | Ranking of ideas Each stakeholder was to vote and rank the ideas presented. The ranking process followed the strategy [29] of ranking ideas by assigning a value to an idea according to priority. For those who attended Microsoft Teams, polls were used for ranking the ideas according to the order of priority between 1–5. | Lasted 15 min |
| Institution and Country | Occupation | Role |
|---|---|---|
| Tshwane Clinics, South Africa | Registered midwife | Pre-conception, pregnancy, labour, and postpartum care |
| Private clinic, South Africa | Registered midwife | Pre-conception, pregnancy, labour, and postpartum care |
| University, South Africa | Midwifery educators Student midwife | Conducting training and updating curriculum for midwifery care |
| University, Swaziland | Midwifery educators | Conducting midwifery training |
| Society of Midwives in South Africa | Registered midwife | Engagement activities for health professionals |
| Traditional Health Organisation (THO) | Coordinator | Regulatory body and council of traditional health practitioners, including TBAs |
| Soshanguve, South Africa | Traditional birth attendants | Pregnancy, labour, and postdelivery in rural communities |
| Nigeria | Researchers on traditional health practice | Studies on collaboration between midwives and TBAs |
| Ghana | Researchers on traditional health practice | Professor with expertise in implementation collaboration between midwives and TBAs |
| National Department of Health (DoH) | Director of Traditional Medicine, Director of Maternal and Child Healthcare | Policymakers |
| Rural Community | Civil society | Community representatives |
| United Nations International Children’s Emergency Fund (UNICEF) | Medical doctor | Health education strategies and advocacy for collaboration |
| DENOSA | Labour organisations | Justice and legal representations for health professionals |
| Processes (Items) | Voting and Ranking n (%) |
|---|---|
| Conduct training and capacity building for TBAs on low-risk antenatal, labour, and postpartum care | 20 (100%) |
| Develop standardised guidelines with clear TBA roles for maternity care | 15 (75%) |
| Regulation of practice through policy development | 13 (65%) |
| Quality control measures through the Department of Health, standardised care, and accreditation | 13 (65%) |
| Formulate guidelines for referral pathways for midwives and traditional birth attendants | 10 (50%) |
| Scope of practice of traditional birth attendants | 8 (40%) |
| Establish a database system to record all the registered traditional birth attendants in South Africa | 8 (40%) |
| Conduct community workshops on baby care, high-risk maternal conditions such as pre-eclampsia, HIV, and postpartum haemorrhage, and the road to health booklets | 8 (40%) |
| Meetings, i.e., (engagement platforms with stakeholders and MNM meetings (maternal and neonatal mortality meetings) | 3 (15%) |
| Identify appropriate ways to remunerate traditional birth attendants in line with national health insurance (NHI) policies | 3 (15%) |
| Develop a herbal medicine clarification system recording all herbal medicine used during pregnancy | 3 (15%) |
| Record background information on the origin of traditional practice | 0 |
| Criteria to identify pregnant patients at risk, such as pre-eclampsia, and refer patients | 0 |
| Outcomes (Items) | Voting and Ranking n (%) |
|---|---|
| Patient-centred care and culturally appropriate care | 20 (100%) |
| Reduction in maternal and neonatal mortality rates | 16 (80%) |
| Strategic alignment with policy framework (NHI and re-engineering of primary healthcare policies | 16 (80%) |
| Improve the acceptance and recognition of traditional health as a legitimate system of healthcare | 12 (60%) |
| Improve access to maternal healthcare services at the community level | 11 (55%) |
| Strengthen knowledge-sharing through joint capacity-building programmes | 11 (55%) |
| Extend the collaboration to SBAs, community representatives, and traditional health practitioners (THPs) | 7 (35%) |
| Foster continuous professional development | 5 (25%) |
| A culture shift in the delivery of healthcare | 2 (10%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musie, M.R.; Mulaudzi, F.M.; Anokwuru, R.; Sepeng, N.V. An Inclusive Framework for Collaboration between Midwives and Traditional Birth Attendants and Optimising Maternal and Child Healthcare in Restricted Rural Communities in South Africa: Policy Considerations. Healthcare 2024, 12, 363. https://doi.org/10.3390/healthcare12030363
Musie MR, Mulaudzi FM, Anokwuru R, Sepeng NV. An Inclusive Framework for Collaboration between Midwives and Traditional Birth Attendants and Optimising Maternal and Child Healthcare in Restricted Rural Communities in South Africa: Policy Considerations. Healthcare. 2024; 12(3):363. https://doi.org/10.3390/healthcare12030363
Chicago/Turabian StyleMusie, Maurine Rofhiwa, Fhumulani Mavis Mulaudzi, Rafiat Anokwuru, and Nombulelo Veronica Sepeng. 2024. "An Inclusive Framework for Collaboration between Midwives and Traditional Birth Attendants and Optimising Maternal and Child Healthcare in Restricted Rural Communities in South Africa: Policy Considerations" Healthcare 12, no. 3: 363. https://doi.org/10.3390/healthcare12030363
APA StyleMusie, M. R., Mulaudzi, F. M., Anokwuru, R., & Sepeng, N. V. (2024). An Inclusive Framework for Collaboration between Midwives and Traditional Birth Attendants and Optimising Maternal and Child Healthcare in Restricted Rural Communities in South Africa: Policy Considerations. Healthcare, 12(3), 363. https://doi.org/10.3390/healthcare12030363