_Rachiotis.png)
Applicability and Validity of Second Victim Assessment Instruments among General Practitioners and Healthcare Assistants (SEVID-IX Study)

 ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
1.1. Background and Rationale
1.2. Objectives
2. Methods
2.1. Study Design, Setting, and Participants
2.2. Variables
- eight demographic items (gender, objective age, subjective age, occupational group, workplace, nation),
- an item about prior knowledge of the term “second victim” (yes/no),
- an item regarding previously completed specialization in palliative care (yes/no),
- The modified SeViD-questionnaire covered:
- i.
- symptoms after a potentially traumatic situation with multiple-answer options (yes/no) for various possible symptoms such as anxiety about being excluded from work by colleagues, anxiety about getting fired, listlessness, depressive symptoms, lack of concentration, flashbacks during work, flashbacks outside of work, aggressiveness, defensive behavior, psychosomatic symptoms such as headache and back pain, sleeplessness, drug or alcohol abuse, feelings of shame, feelings of guilt, loss of self-esteem, social isolation, anger towards others, anger towards oneself, desire for support, and desire to better understand the incident,
- ii.
- duration of symptoms for more than 12 months (yes/no), and
- iii.
- complete recovery from symptoms (yes/no).
- iv.
- Symptom count was measured by summing the reported symptoms mentioned earlier.
- Four free-text entries gathered information on the situation, symptoms, support received, interaction with the pandemic, and coping strategies in regards to SVP.
- Experience, symptoms, and support strategies of SVP were measured using the G-SVESTR comprising nine dimensions with three to five items each. We computed an overall G-SVESTR score as the sum of the nine partially recorded mean values of the subscales, deviating from previous studies by including this overall score. Notably, the support subscales of the G-SVESTR instruments were not included in the overall score [31].
- Symptoms and support options of MI were measured using the German version of the eight-item MISS-HP scale. We included six questions on religiosity and spirituality to determine whether to use the 8-item or 10-item G-MISS-HP, as two items of the latter depend on religiosity.
- The questionnaire ended with an open commentary field.
2.3. Data Collection
2.3.1. Study Size
2.3.2. Statistics
3. Results
3.1. Participants
3.2. Descriptive Data
3.3. Main Results
4. Discussion
4.1. Key Results
4.1.1. Collegial Support–Optional
4.1.2. Secular Version of G-MISS-HP
4.1.3. “Subjective” and “Objective” SVP
4.1.4. G-SVESTR Sum Score
4.1.5. The Role of Personality Traits
4.1.6. The Role of Trauma, Depression, and PTSD
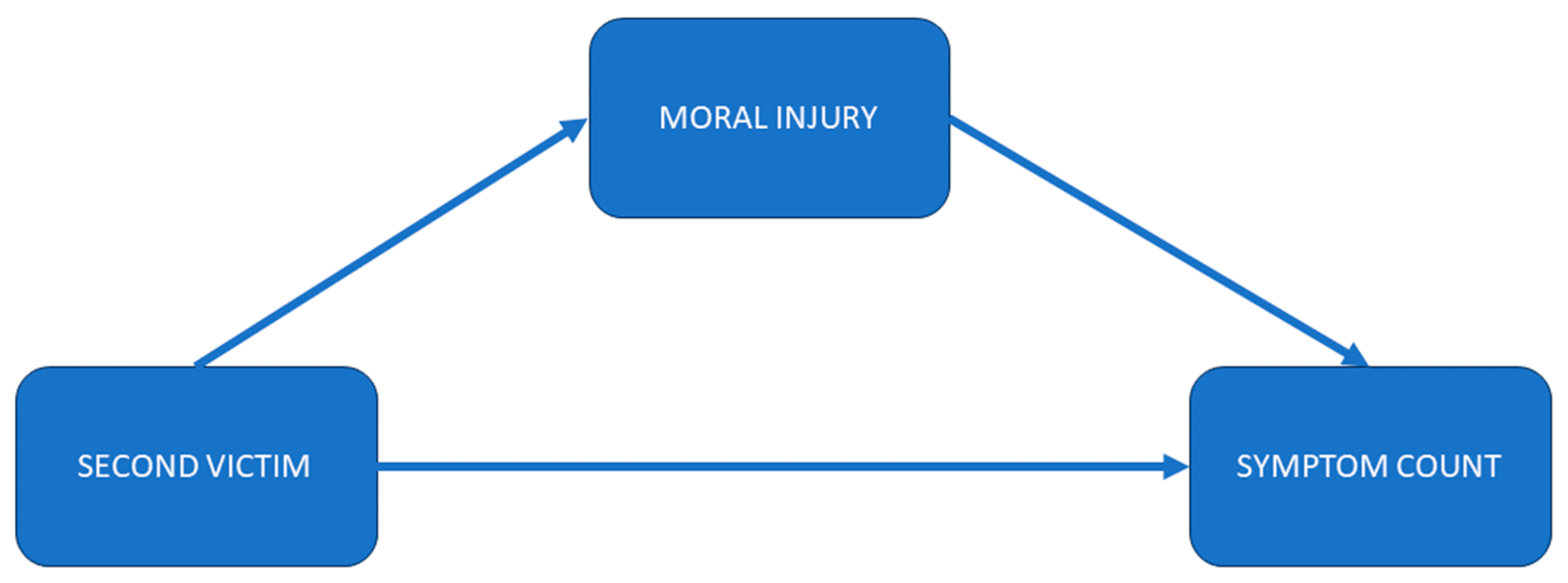
4.1.7. Influence of MI and SV on Symptom Count
4.1.8. The Role of Collegial Support in Coping with SVP
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, A.W. Medical error: The second victim. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Seys, D.; Wu, A.W.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Scott, S.D.; Conway, J.; Sermeus, W.; Vanhaecht, K. Health care professionals as second victims after adverse events: A systematic review. Eval. Health Prof. 2013, 36, 135–162. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; Seys, D.; Russotto, S.; Strametz, R.; Mira, J.; Sigurgeirsdóttir, S.; Wu, A.W.; Põlluste, K.; Popovici, D.G.; Sfetcu, R.; et al. An evidence and consensus-based definition of second victim: A strategic topic in healthcare quality, patient safety, person-centeredness and human resource management. Int. J. Environ. Res. Public Health 2022, 19, 16869. [Google Scholar] [CrossRef] [PubMed]
- Seys, D.; Panella, M.; Russotto, S.; Strametz, R.; Joaquín Mira, J.; Van Wilder, A.; Godderis, L.; Vanhaecht, K. In search of an international multidimensional action plan for second victim support: A narrative review. BMC Health Serv. Res. 2023, 23, 816. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, B.; Powell, D.; Higgins, M.F. The Second Victim: A Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Ozeke, O.; Ozeke, V.; Coskun, O.; Budakoglu, I.I. Second victims in health care: Current perspectives. Adv. Med. Educ. Pract. 2019, 10, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.D.; Hirschinger, L.E.; Cox, K.R.; McCoig, M.; Brandt, J.; Hall, L.W. The natural history of recovery for the healthcare provider “second victim” after adverse patient events. Qual. Saf. Health Care 2009, 18, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Berlin, L. Medical errors, malpractice, and defensive medicine: An ill-fated triad. Diagnosis 2017, 4, 133–139. [Google Scholar] [CrossRef]
- Panella, M.; Rinaldi, C.; Leigheb, F.; Knesse, S.; Donnarumma, C.; Kul, S.; Vanhaecht, K.; Di Stanislao, F. Prevalence and costs of defensive medicine: A national survey of Italian physicians. J. Health Serv. Res. Policy 2017, 22, 211–217. [Google Scholar] [CrossRef]
- Müller, B.S.; Donner-Banzhoff, N.; Beyer, M.; Haasenritter, J.; Müller, A.; Seifart, C. Regret among primary care physicians: A survey of diagnostic decisions. BMC Fam. Pract. 2020, 21, 53. [Google Scholar] [CrossRef]
- Donner-Banzhoff, N.; Müller, B.; Beyer, M.; Haasenritter, J.; Seifart, C. Thresholds, rules and defensive strategies: How physicians learn from their prior diagnosis-related experiences. Diagnosis 2020, 7, 115–121. [Google Scholar] [CrossRef]
- Quillivan, R.R.; Burlison, J.D.; Browne, E.K.; Scott, S.D.; Hoffman, J.M. Patient safety culture and the second victim phenomenon: Connecting culture to staff distress in nurses. Jt. Comm. J. Qual. Patient Saf. 2016, 42, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Strametz, R.; Koch, P.; Vogelgesang, A.; Burbridge, A.; Rösner, H.; Abloescher, M.; Huf, W.; Ettl, B.; Raspe, M. Prevalence of second victims, risk factors and support strategies among young German physicians in internal medicine (SeViD-I survey). J. Occup. Med. Toxicol. 2021, 16, 11. [Google Scholar] [CrossRef] [PubMed]
- Strametz, R.; Fendel, J.C.; Koch, P.; Roesner, H.; Zilezinski, M.; Bushuven, S.; Raspe, M. Prevalence of Second Victims, Risk Factors, and Support Strategies among German Nurses (SeViD-II Survey). Int. J. Environ. Res. Public Health 2021, 18, 10594. [Google Scholar] [CrossRef] [PubMed]
- Marung, H.; Strametz, R.; Roesner, H.; Reifferscheid, F.; Petzina, R.; Klemm, V.; Trifunovic-Koenig, M.; Bushuven, S. Second Victims among German Emergency Medical Services Physicians (SeViD-III-Study). Int. J. Environ. Res. Public Health 2023, 20, 4267. [Google Scholar] [CrossRef] [PubMed]
- Potura, E.; Klemm, V.; Roesner, H.; Sitter, B.; Huscsava, H.; Trifunovic-Koenig, M.; Voitl, P.; Strametz, R. Second Victims among Austrian Pediatricians (SeViD-A1 Study). Healthcare 2023, 11, 2501. [Google Scholar] [CrossRef] [PubMed]
- Krommer, E.; Ablöscher, M.; Klemm, V.; Gatterer, C.; Rösner, H.; Strametz, R.; Huf, W.; Ettl, B. Second Victim Phenomenon in an Austrian Hospital before the Implementation of the Systematic Collegial Help Program KoHi: A Descriptive Study. Int. J. Environ. Res. Public Health 2023, 20, 1913. [Google Scholar] [CrossRef] [PubMed]
- Shay, J. Achilles in Vietnam: Combat Trauma and the Undoing of Character; Simon and Schuster: New York, NY, USA, 2010. [Google Scholar]
- Mantri, S.; Lawson, J.M.; Wang, Z.; Koenig, H.G. Identifying Moral Injury in Healthcare Professionals: The Moral Injury Symptom Scale-HP. J. Relig. Health 2020, 59, 2323–2340. [Google Scholar] [CrossRef]
- Mantri, S.; Lawson, J.M.; Wang, Z.; Koenig, H.G. Prevalence and Predictors of Moral Injury Symptoms in Health Care Professionals. J. Nerv. Ment. Dis. 2021, 209, 174–180. [Google Scholar] [CrossRef]
- Ducharlet, K.; Trivedi, M.; Gelfand, S.L.; Liew, H.; McMahon, L.P.; Ashuntantang, G.; Brennan, F.; Brown, M.; Martin, D.E. Moral Distress and Moral Injury in Nephrology During the COVID-19 Pandemic. Semin. Nephrol. 2021, 41, 253–261. [Google Scholar] [CrossRef]
- Čartolovni, A.; Stolt, M.; Scott, P.A.; Suhonen, R. Moral injury in healthcare professionals: A scoping review and discussion. Nurs. Ethics 2021, 28, 590–602. [Google Scholar] [CrossRef] [PubMed]
- Fourie, C. Who is experiencing what kind of moral distress? Distinctions for moving from a narrow to a broad definition of moral distress. AMA J. Ethics 2017, 19, 578–584. [Google Scholar] [PubMed]
- Nørøxe, K.B.; Pedersen, A.F.; Bro, F.; Vedsted, P. Mental well-being and job satisfaction among general practitioners: A nationwide cross-sectional survey in Denmark. BMC Fam. Pract. 2018, 19, 130. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.; Mohos, A.; Kalabay, L.; Torzsa, P. Potential correlates of burnout among general practitioners and residents in Hungary: The significant role of gender, age, dependant care and experience. BMC Fam. Pract. 2018, 19, 193. [Google Scholar] [CrossRef] [PubMed]
- Castelli, L.; Di Tella, M.; Benfante, A.; Taraschi, A.; Bonagura, G.; Pizzini, A.; Romeo, A. The psychological impact of COVID-19 on general practitioners in Piedmont, Italy. J. Affect. Disord. 2021, 281, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Dell’Oste, V.; Barberi, F.M.; Bertelloni, C.A.; Pedrinelli, V.; Dell’Osso, L. Mental Health Symptoms among General Practitioners Facing the Acute Phase of the COVID-19 Pandemic: Detecting Different Reaction Groups. Int. J. Environ. Res. Public Health 2022, 19, 4007. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, N.C.; Blomme, R.J. Burnout among general practitioners, a systematic quantitative review of the literature on determinants of burnout and their ecological value. Front. Psychol. 2022, 13, 1064889. [Google Scholar] [CrossRef] [PubMed]
- Werdecker, L.; Esch, T. Burnout, satisfaction and happiness among German general practitioners (GPs): A cross-sectional survey on health resources and stressors. PLoS ONE 2021, 16, e0253447. [Google Scholar] [CrossRef]
- Strametz, R. Entwicklung und Validation eines Fragebogens zur Beurteilung der Inzidenz und Reaktionen von Second Victims im Deutschsprachigen Raum (SeViD). Zbl Arbeitsmed 2020, 71, 19–23. [Google Scholar] [CrossRef]
- Strametz, R.; Siebold, B.; Heistermann, P.; Haller, S.; Bushuven, S. Validation of the German Version of the Second Victim Experience and Support Tool-Revised. J. Patient Saf. 2022, 18, 182–192. [Google Scholar] [CrossRef]
- Trifunovic-Koenig, M.; Strametz, R.; Gerber, B.; Mantri, S.; Bushuven, S. Validation of the German Version of the Moral Injury Symptom and Support Scale for Health Professionals (G-MISS-HP) and Its Correlation to the Second Victim Phenomenon. Int. J. Environ. Res. Public Health 2022, 19, 4857. [Google Scholar] [CrossRef]
- Koenig, H.G.; Ames, D.; Youssef, N.A.; Oliver, J.P.; Volk, F.; Teng, E.J.; Haynes, K.; Erickson, Z.D.; Arnold, I.; O’Garo, K.; et al. The Moral Injury Symptom Scale-Military Version. J. Relig. Health 2018, 57, 249–265. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G.; Youssef, N.A.; Pearce, M. Assessment of Moral Injury in Veterans and Active Duty Military Personnel with PTSD: A Review. Front. Psychiatry 2019, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- Burlison, J.D.; Scott, S.D.; Browne, E.K.; Thompson, S.G.; Hoffman, J.M. The Second Victim Experience and Support Tool: Validation of an Organizational Resource for Assessing Second Victim Effects and the Quality of Support Resources. J. Patient Saf. 2017, 13, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Winning, A.M.; Merandi, J.; Rausch, J.R.; Liao, N.; Hoffman, J.M.; Burlison, J.D.; Gerhardt, C.A. Validation of the second victim experience and support tool-revised in the neonatal intensive care unit. J. Patient Saf. 2021, 17, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Rammstedt, B.; Kemper, C.J.; Klein, M.C.; Beierlein, C.; Kovaleva, A. A short scale for assessing the big five dimensions of personality: 10 item big five inventory (BFI-10). Methods Data Anal. 2013, 7, 17. [Google Scholar]
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Ball, H.L. Conducting Online Surveys. J. Hum. Lact. 2019, 35, 413–417. [Google Scholar] [CrossRef]
- Freund, R.J.; Littell, R.C.; Creighton, L. Regression Using JMP; SAS Institute: Cary, NC, USA, 2003. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage: Newcastle upon Tyne, UK, 2013. [Google Scholar]
- Flachaire, E. Bootstrapping heteroskedastic regression models: Wild bootstrap vs. pairs bootstrap. Comput. Stat. Data Anal. 2005, 49, 361–376. [Google Scholar] [CrossRef]
- Salibian-Barrera, M.; Zamar, R.H. Bootstrapping robust estimates of regression. Ann. Stat. 2002, 30, 556–582. [Google Scholar] [CrossRef]
- Fox, J.; Weisberg, S. Bootstrapping Regression Models in R. An Appendix to An R Companion to Applied Regression, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018; Available online: https://socialsciences.mcmaster.ca/jfox/Books/Companion/appendices/Appendix-Bootstrapping.pdf (accessed on 23 November 2023).
- Hayes, A.F.; Scharkow, M. The Relative Trustworthiness of Inferential Tests of the Indirect Effect in Statistical Mediation Analysis:Does Method Really Matter? Psychol. Sci. 2013, 24, 1918–1927. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Leahey, M.; Wright, L.M. Application of the Calgary Family Assessment and Intervention Models: Reflections on the Reciprocity Between the Personal and the Professional. J. Fam. Nurs. 2016, 22, 450–459. [Google Scholar] [CrossRef]
- Kørup, A.K.; Søndergaard, J.; Lucchetti, G.; Ramakrishnan, P.; Baumann, K.; Lee, E.; Frick, E.; Büssing, A.; Alyousefi, N.A.; Karimah, A. Religious values of physicians affect their clinical practice: A meta-analysis of individual participant data from 7 countries. Medicine 2019, 98, e17265. [Google Scholar] [CrossRef]
- Bushuven, S.; Trifunovic-Koenig, M.; Bentele, M.; Bentele, S.; Strametz, R.; Klemm, V.; Raspe, M. Self-Assessment and Learning Motivation in the Second Victim Phenomenon. Int. J. Environ. Res. Public Health 2022, 19, 16016. [Google Scholar] [CrossRef] [PubMed]
- Haagsma, J.A.; Polinder, S.; Toet, H.; Panneman, M.; Havelaar, A.H.; Bonsel, G.J.; van Beeck, E.F. Beyond the neglect of psychological consequences: Post-traumatic stress disorder increases the non-fatal burden of injury by more than 50%. Inj. Prev. 2011, 17, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Furnham, A.; Crump, J. Personality traits, types, and disorders: An examination of the relationship between three self-report measures. Eur. J. Personal. 2005, 19, 167–184. [Google Scholar] [CrossRef]
- Marcus, B.; Schütz, A. Who are the people reluctant to participate in research? Personality correlates of four different types of nonresponse as inferred from self-and observer ratings. J. Personal. 2005, 73, 959–984. [Google Scholar] [CrossRef]
- Brandt, N.D.; Drewelies, J.; Willis, S.L.; Schaie, K.W.; Ram, N.; Gerstorf, D.; Wagner, J. Acting Like a Baby Boomer? Birth-Cohort Differences in Adults’ Personality Trajectories During the Last Half a Century. Psychol. Sci. 2022, 33, 382–396. [Google Scholar] [CrossRef]
- AHA. Emergency Cardiovascular Care Program Administration Manual Guidelines for Program Administration and Training. International Version. Available online: https://www.heart.org/-/media/BDD5142CCDEE4490A577770FC7EBE670.ashx (accessed on 1 February 2023).
- Fliege, H.; Rose, M.; Arck, P.; Levenstein, S.; Klapp, B.F. Validierung des “perceived stress questionnaire”(PSQ) an einer deutschen Stichprobe. [Validation of the “Perceived Stress Questionnaire”(PSQ) in a German sample.]. Diagnostica 2001, 47, 142–152. [Google Scholar] [CrossRef]
- Whooley, M.A.; Avins, A.L.; Miranda, J.; Browner, W.S. Case-finding instruments for depression: Two questions are as good as many. J. Gen. Intern. Med. 1997, 12, 439–445. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scores | Mean (M) | SD | Median | Min | Max |
|---|---|---|---|---|---|
| MISS-HP-8 item (sum) | 24.1 | 12.2 | 21 | 6 | 57 |
| G-SVESTR (sum) | 22.1 | 5.7 | 21.3 | 11.4 | 32.2 |
| G-SVESTR (Psychological Distress) | 3.47 | 1.06 | 3.50 | 1 | 5 |
| G-SVESTR (Physical Distress) | 2.61 | 1.04 | 2.60 | 1 | 5 |
| G-SVESTR (Colleagial Support) | 1.94 | 0.65 | 2.00 | 1 | 4 |
| G-SVESTR (Supervisor Support) | 2.50 | 1.10 | 2.5 | 1 | 5 |
| G-SVESTR (Institutional Support) | 3.14 | 1.10 | 3.33 | 1 | 5 |
| G-SVESTR (Professional Self-Efficacy) | 2.66 | 1.15 | 2.75 | 1 | 5 |
| G-SVESTR (Turnover Intentions) | 1.88 | 1.03 | 1.5 | 1 | 4.25 |
| G-SVESTR (Absenteeism) | 1.82 | 0.96 | 1.33 | 1 | 4 |
| G-SVESTR (Resilience) | 2.10 | 0.92 | 2.00 | 1 | 4.75 |
| Bootstrapping (Bias-Corrected and Accelerated Method Based on 1000 Samples) | ||||||
|---|---|---|---|---|---|---|
| B | Bias | Std. Error | Sig. (2-Tailed) | BCa 95% Confidence Interval | ||
| Lower | Upper | |||||
| (Constant) | 9.80 | 0.04 | 1.65 | <0.001 | 7.03 | 12.71 |
| Age | −0.08 | −0.001 | 0.03 | 0.01 | −0.14 | −0.003 |
| Bootstrapping (Bias-Corrected and Accelerated Method Based on 1000 Samples) | ||||||
|---|---|---|---|---|---|---|
| B | Bias | Std. Error | Sig. (2-Tailed) | BCa 95% Confidence Interval | ||
| Lower | Upper | |||||
| (Constant) | 0.86 | −0.04 | 3.77 | 0.82 | −5.69 | 8.35 |
| Age | −0.04 | 0.00 | 0.03 | 0.20 | −0.11 | 0.02 |
| Extraversion | −0.01 | −0.01 | 0.44 | 0.98 | −0.88 | 0.82 |
| Neuroticism | 1.64 | 0.02 | 0.43 | <0.001 | 0.68 | 2.53 |
| Openness | 0.12 | 0.00 | 0.42 | 0.77 | −0.72 | 0.92 |
| Conscientiousness | −0.15 | 0.03 | 0.60 | 0.80 | −1.27 | 1.18 |
| Agreeableness | 0.82 | −0.02 | 0.54 | 0.13 | −0.23 | 1.84 |
| Bootstrapping (Bias-Corrected and Accelerated Method Based on 1000 Samples) | ||||||
|---|---|---|---|---|---|---|
| B | Bias | Std. Error | Sig. (2-Tailed) | BCa 95% Confidence Interval | ||
| Lower | Upper | |||||
| (Constant) | −12.12 | −0.01 | 3.91 | <0.001 | −19.66 | −4.34 |
| Age | 0.00 | 0.00 | 0.03 | 0.97 | −0.07 | 0.06 |
| Extraversion | 0.41 | −0.04 | 0.45 | 0.37 | −0.45 | 1.19 |
| Neuroticism | 1.23 | −0.02 | 0.49 | 0.01 | 0.29 | 2.15 |
| Openness | 0.20 | 0.00 | 0.39 | 0.61 | −0.61 | 0.93 |
| Conscientiousness | 0.58 | 0.05 | 0.54 | 0.28 | −0.46 | 1.90 |
| Agreeableness | 0.95 | −0.03 | 0.49 | 0.06 | 0.05 | 1.78 |
| G-SVESTR | 0.32 | 0.00 | 0.08 | <0.001 | 0.17 | 0.50 |
| Bootstrapping (Bias-Corrected and Accelerated Method Based on 1000 Samples) | ||||||
|---|---|---|---|---|---|---|
| B | Bias | Std. Error | Sig. (2-Tailed) | BCa 95% Confidence Interval | ||
| Lower | Upper | |||||
| (Constant) | −14.85 | 0.02 | 4.21 | <0.001 | −23.89 | −6.31 |
| Age | 0.00 | 0.00 | 0.03 | 0.93 | −0.07 | 0.07 |
| Extraversion | 0.39 | −0.03 | 0.45 | 0.38 | −0.44 | 1.14 |
| Neuroticism | 1.65 | −0.01 | 0.45 | <0.001 | 0.78 | 2.52 |
| Openness | 0.28 | −0.01 | 0.38 | 0.44 | −0.46 | 0.94 |
| Conscientiousness | 0.34 | 0.07 | 0.58 | 0.55 | −0.78 | 1.77 |
| Agreeableness | 1.62 | −0.04 | 0.50 | <0.001 | 0.69 | 2.44 |
| G-SVESTR | 0.23 | 0.00 | 0.10 | 0.03 | 0.03 | 0.43 |
| G-MISS-HP | 0.08 | 0.00 | 0.04 | 0.03 | 0.01 | 0.16 |
| Unstandardized Effect | BootLLCI | BootULCI | |
|---|---|---|---|
| Total | −0.04 | −0.08 | −0.009 |
| Openness | −0.0001 | −0.008 | 0.009 |
| Conscientiousness | −0.0003 | −0.008 | 0.009 |
| Extraversion | −0.0001 | −0.009 | 0.01 |
| Agreeableness | −0.009 | −0.03 | 0.002 |
| Neuroticism | −0.03 | −0.06 | −0.005 |
| Bootstrapping (Bias-Corrected (BC) Method Based on 5000 Samples) | |||||
|---|---|---|---|---|---|
| B | Std. Error | Sig. (2-Tailed) | BC 95% Confidence Interval | ||
| Lower | Upper | ||||
| (Constant) | 27.55 | 7.36 | <0.01 | 12.88 | 42.22 |
| Physical distress | 4.82 | 4.31 | <0.001 | 2.91 | 6.73 |
| Collegial support | 5.21 | 1.53 | 0.01 | 2.10 | −8.34 |
| Interaction | −1.55 | 0.46 | 0.01 | −2.46 | −0.64 |
| Age | −0.03 | 0.03 | 0.33 | −0.09 | 0.03 |
| Openness | 0.05 | 0.36 | 0.89 | −0.67 | 0.76 |
| Conscientiousness | 0.26 | 0.37 | 0.58 | −0.66 | 1.17 |
| Extraversion | 0.21 | 0.37 | 0.57 | −0.53 | 0.94 |
| Agreeableness | 0.43 | 0.47 | 0.36 | −0.50 | 1.36 |
| Neuroticism | 0.87 | 0.40 | 0.03 | 0.07 | 1.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bushuven, S.; Trifunovic-Koenig, M.; Bunz, M.; Weinmann-Linne, P.; Klemm, V.; Strametz, R.; Müller, B.S. Applicability and Validity of Second Victim Assessment Instruments among General Practitioners and Healthcare Assistants (SEVID-IX Study). Healthcare 2024, 12, 351. https://doi.org/10.3390/healthcare12030351
Bushuven S, Trifunovic-Koenig M, Bunz M, Weinmann-Linne P, Klemm V, Strametz R, Müller BS. Applicability and Validity of Second Victim Assessment Instruments among General Practitioners and Healthcare Assistants (SEVID-IX Study). Healthcare. 2024; 12(3):351. https://doi.org/10.3390/healthcare12030351
Chicago/Turabian StyleBushuven, Stefan, Milena Trifunovic-Koenig, Maxie Bunz, Patrick Weinmann-Linne, Victoria Klemm, Reinhard Strametz, and Beate Sigrid Müller. 2024. "Applicability and Validity of Second Victim Assessment Instruments among General Practitioners and Healthcare Assistants (SEVID-IX Study)" Healthcare 12, no. 3: 351. https://doi.org/10.3390/healthcare12030351
APA StyleBushuven, S., Trifunovic-Koenig, M., Bunz, M., Weinmann-Linne, P., Klemm, V., Strametz, R., & Müller, B. S. (2024). Applicability and Validity of Second Victim Assessment Instruments among General Practitioners and Healthcare Assistants (SEVID-IX Study). Healthcare, 12(3), 351. https://doi.org/10.3390/healthcare12030351