

Spatial Survival Model for COVID-19 in México
 , , , , and
, , , , and
Abstract
1. Introduction
2. Study Area
2.1. Database
2.2. Spatial Autocorrelation
2.3. Statistical Model
2.3.1. Prior Distributions
2.3.2. Posterior Distributions
3. Results
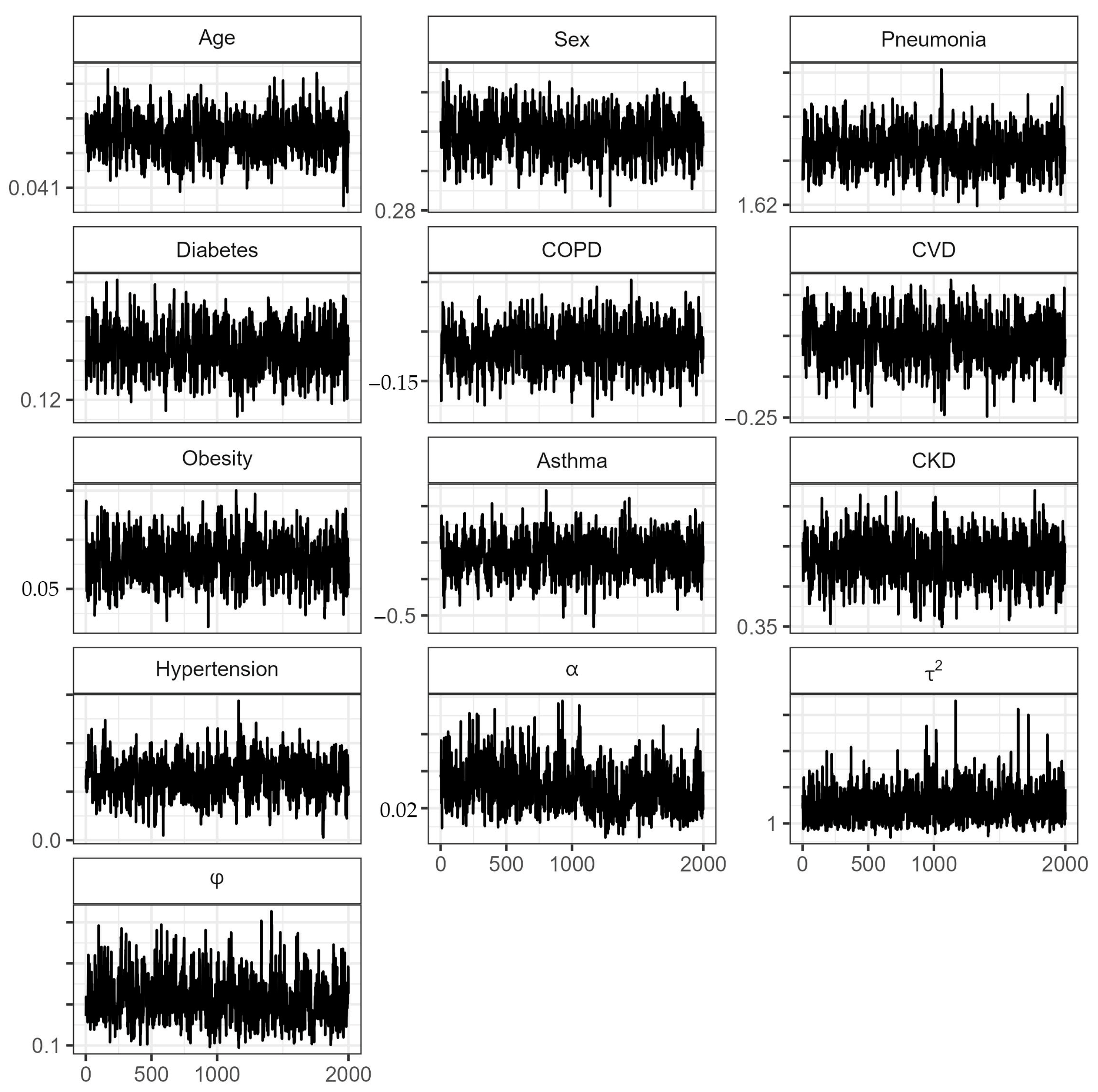
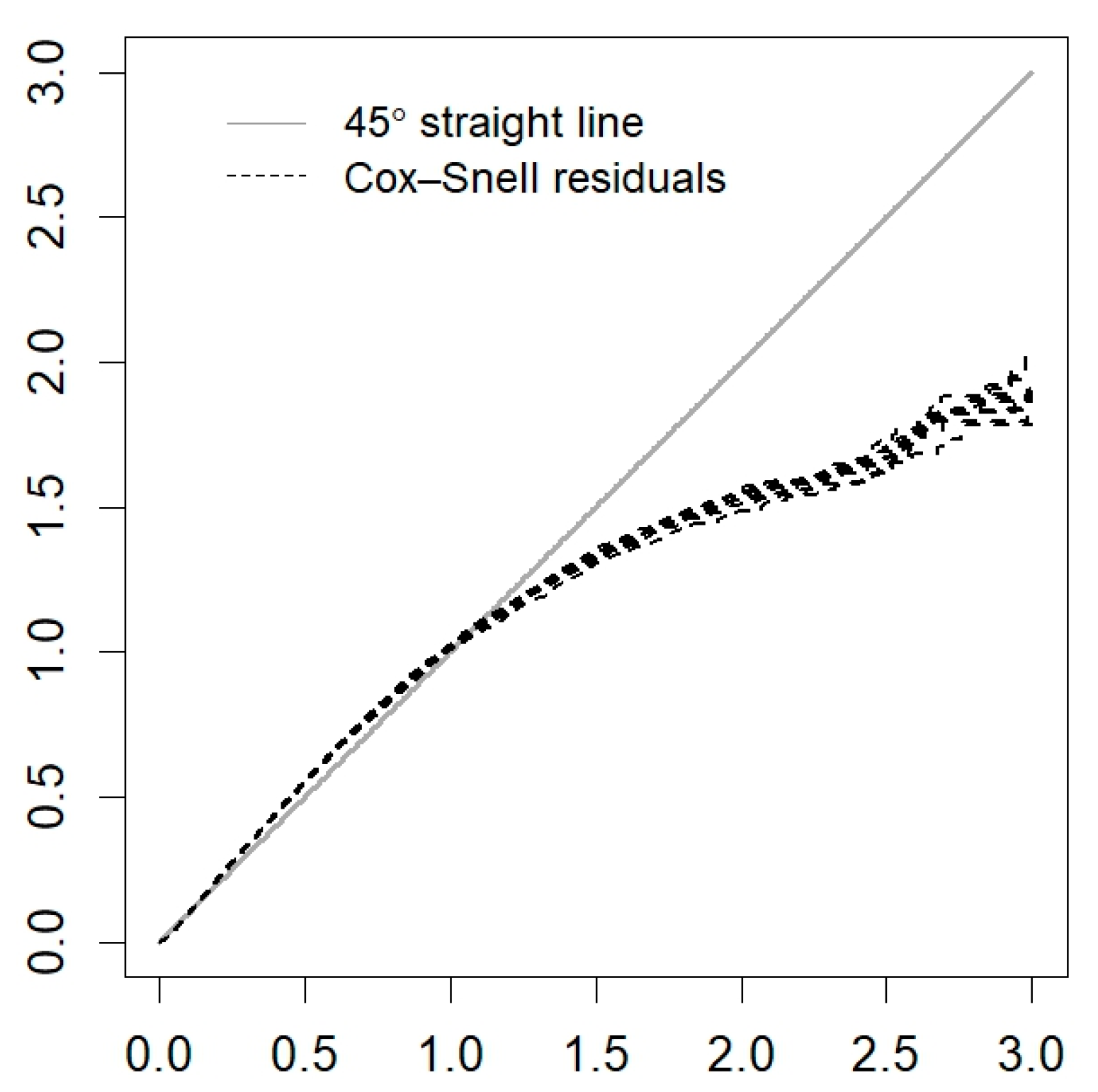
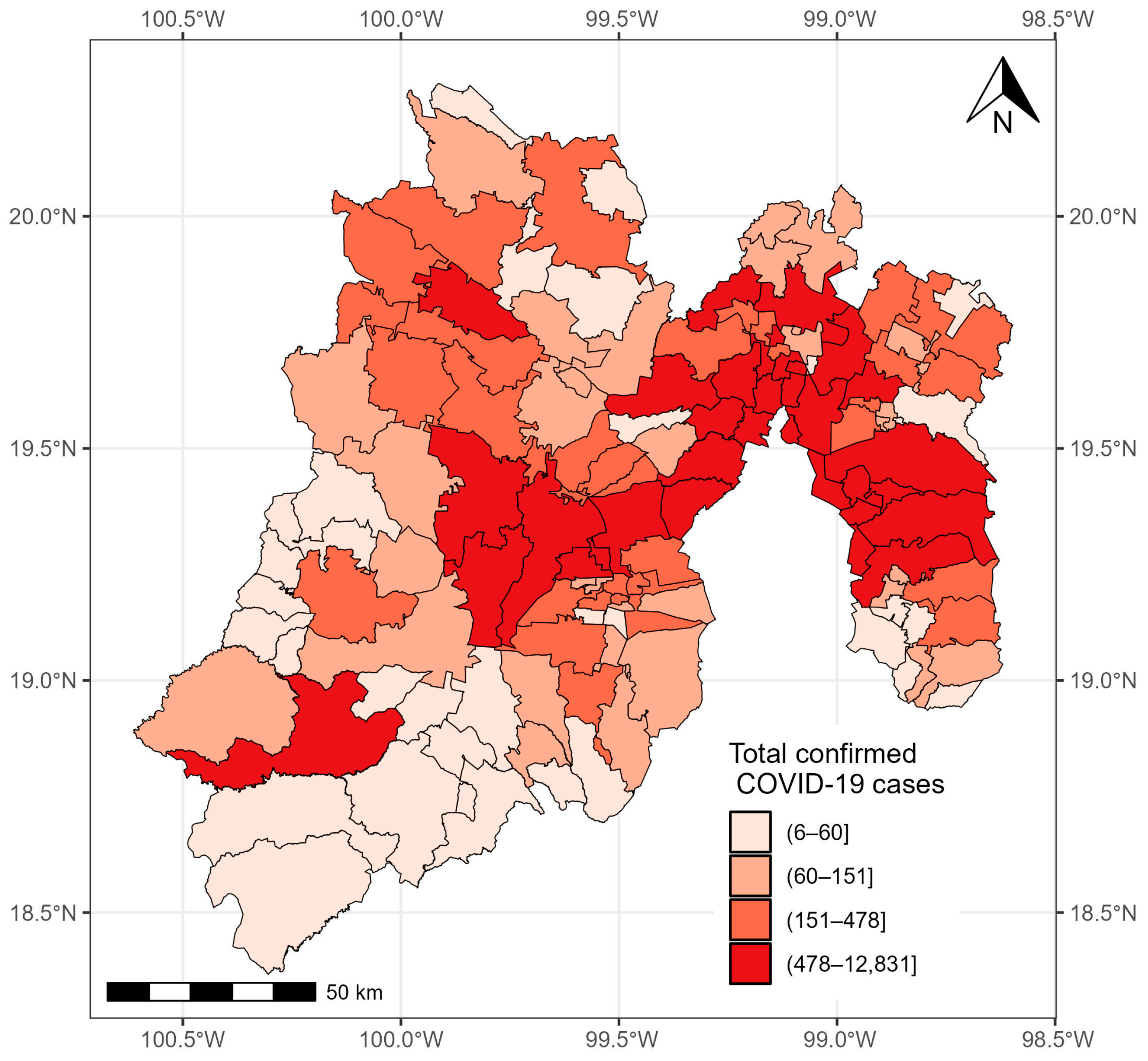
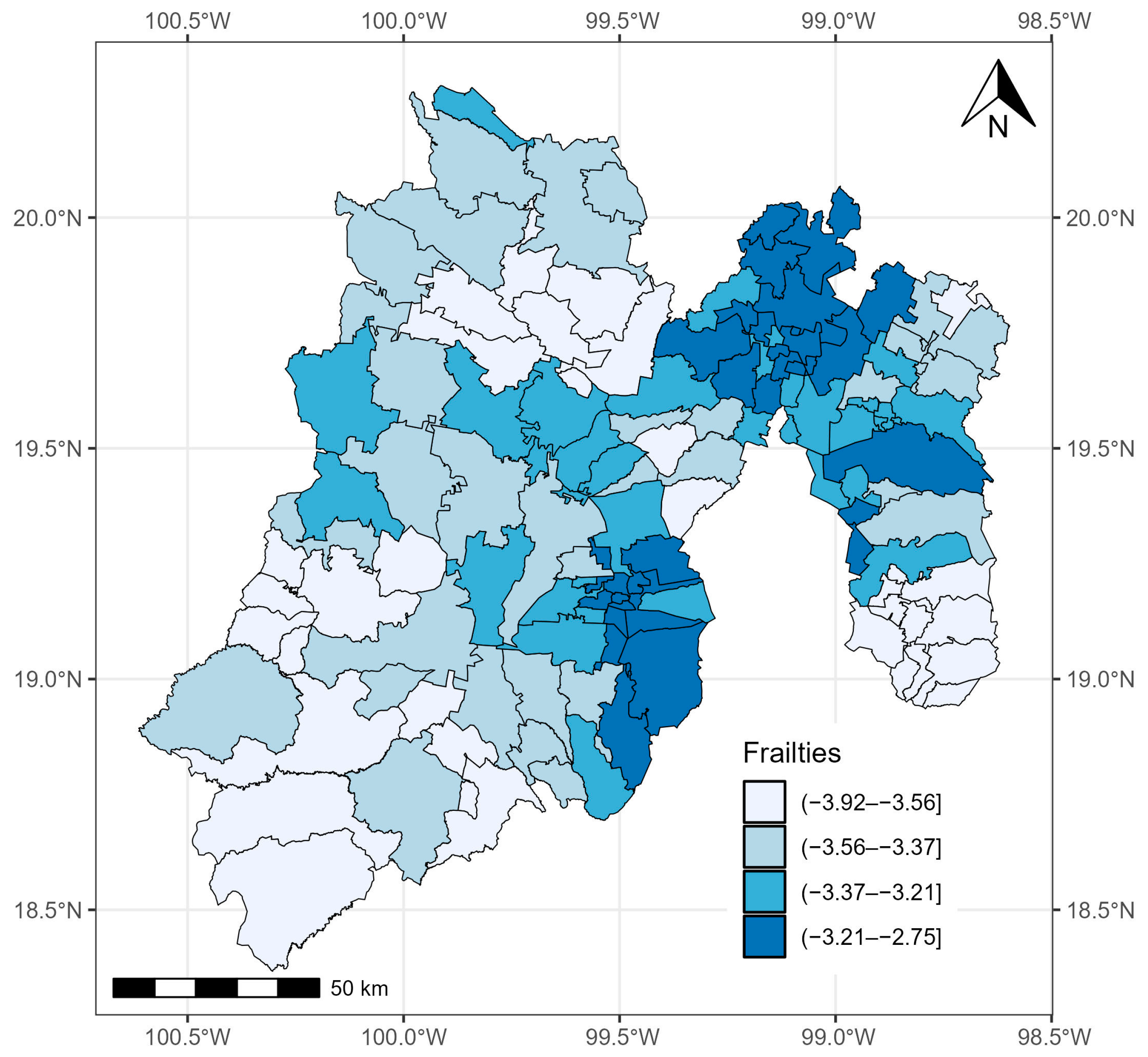
3.1. State of México
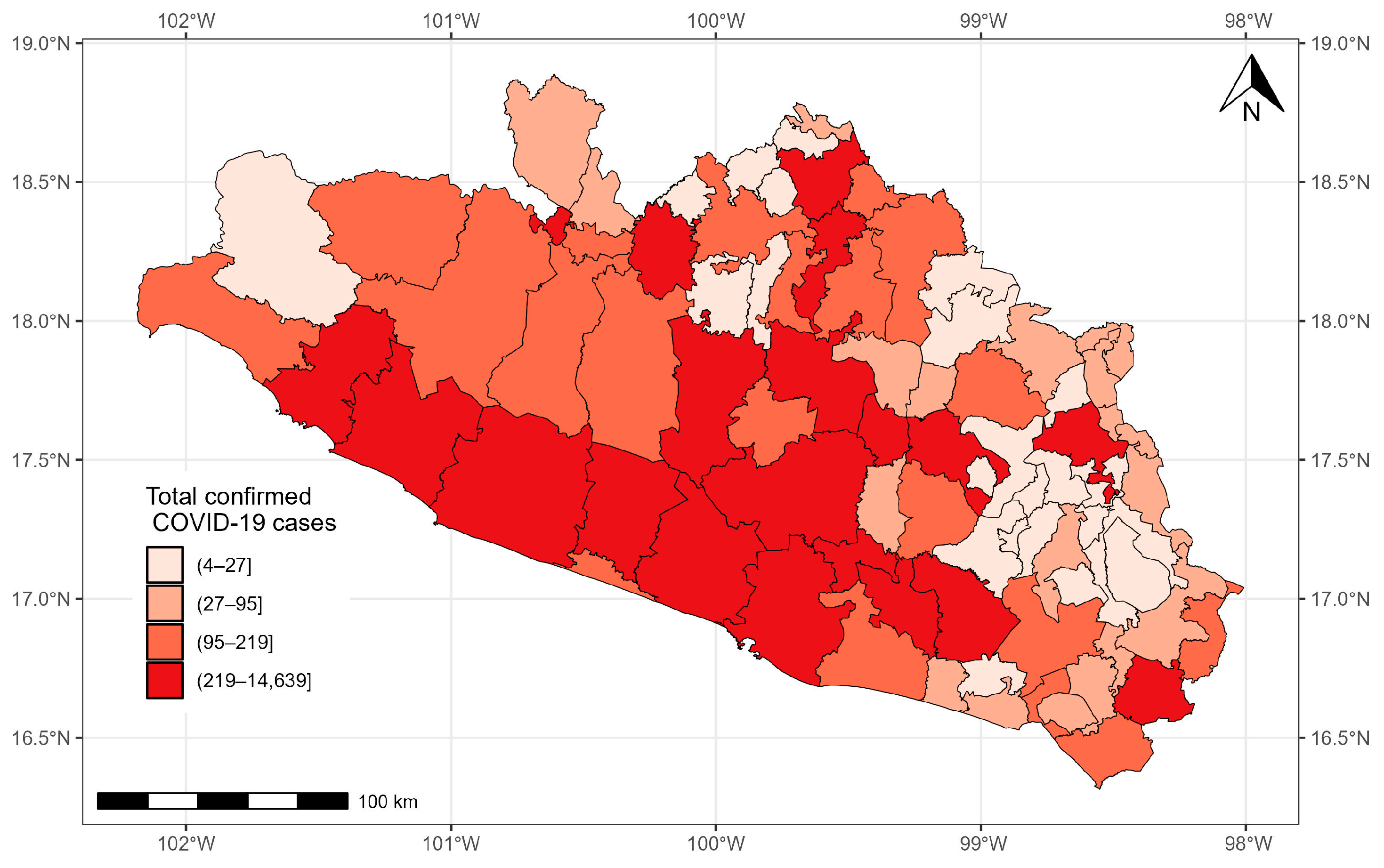
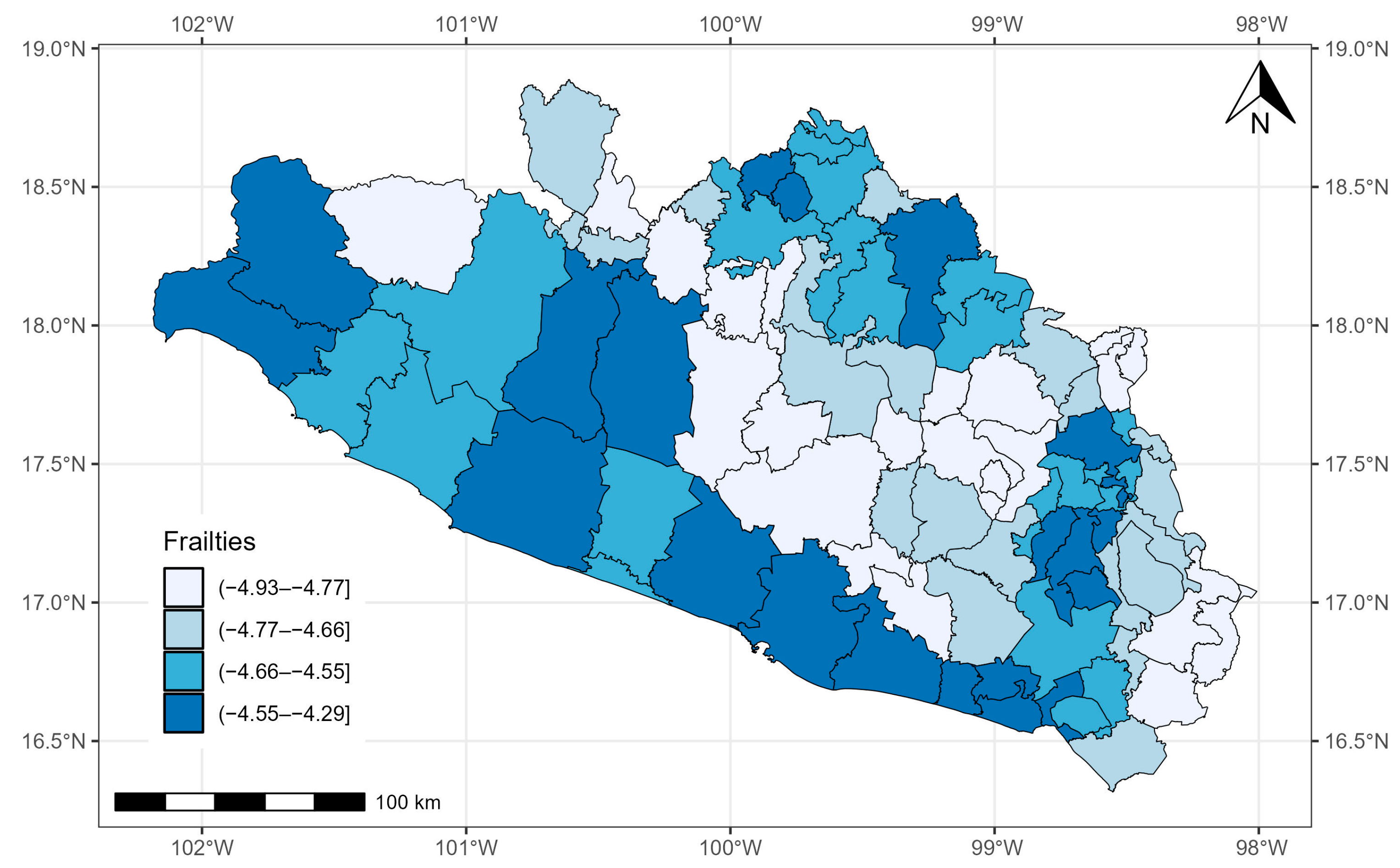
3.2. State of Guerrero
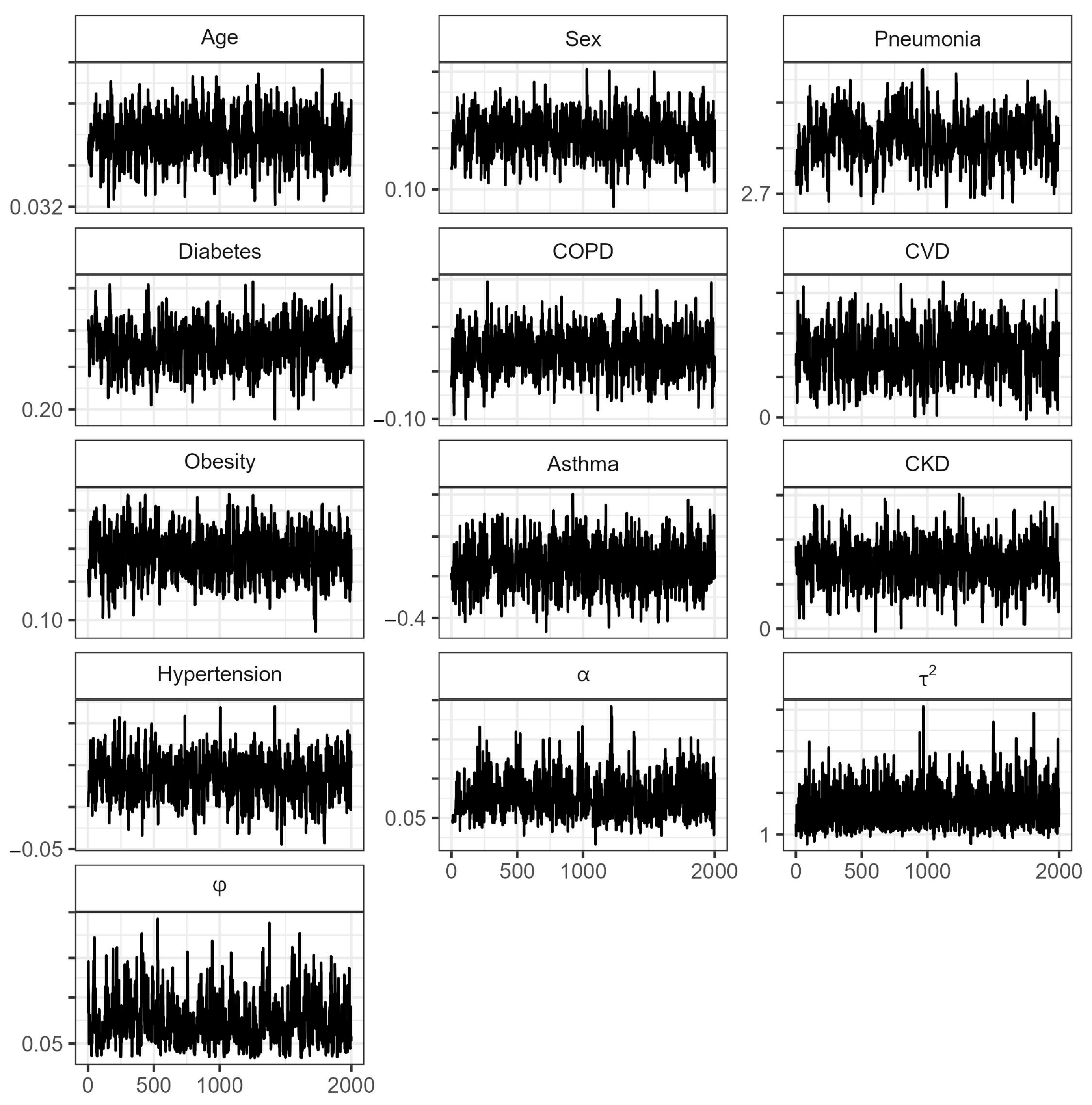
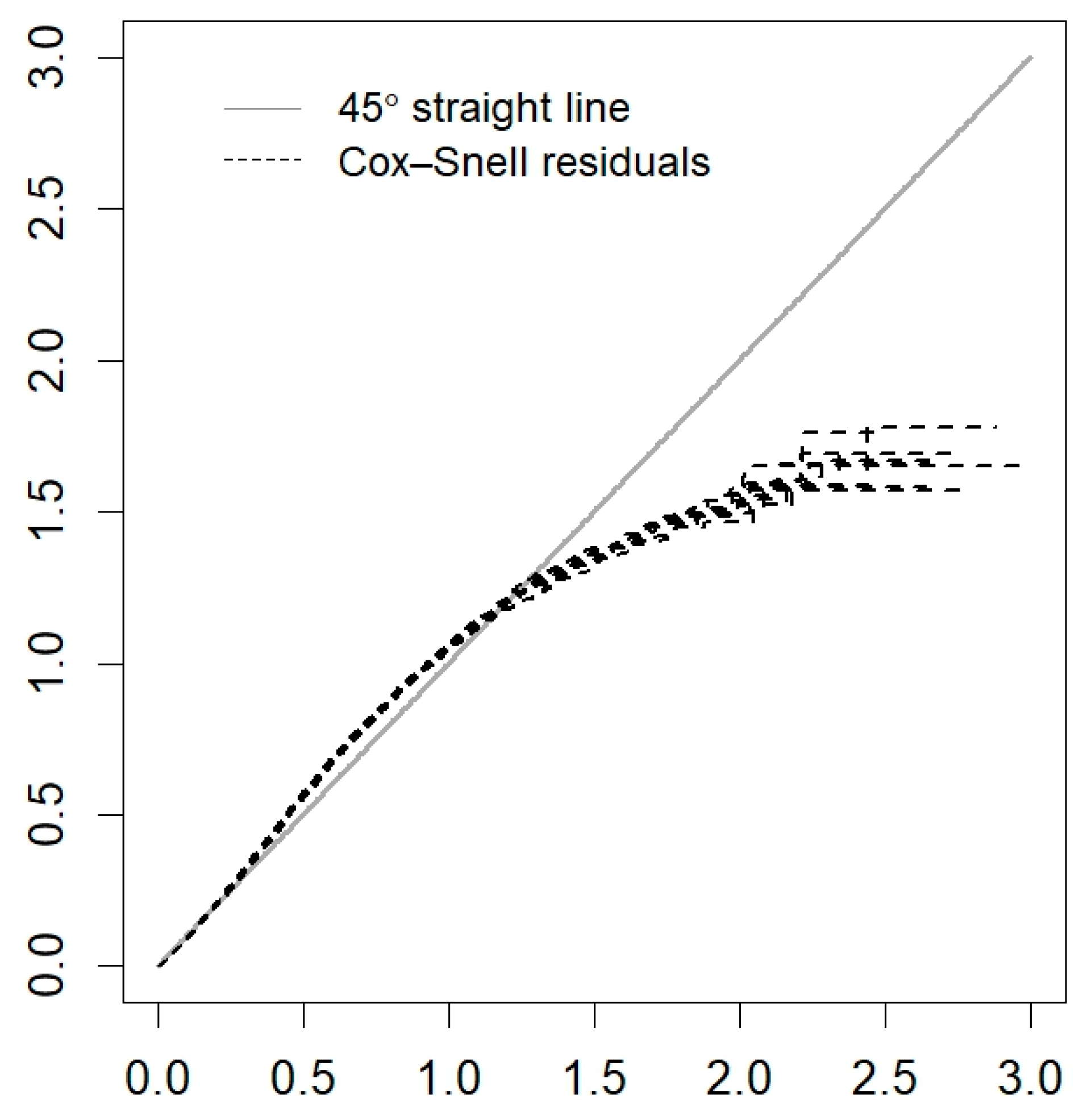
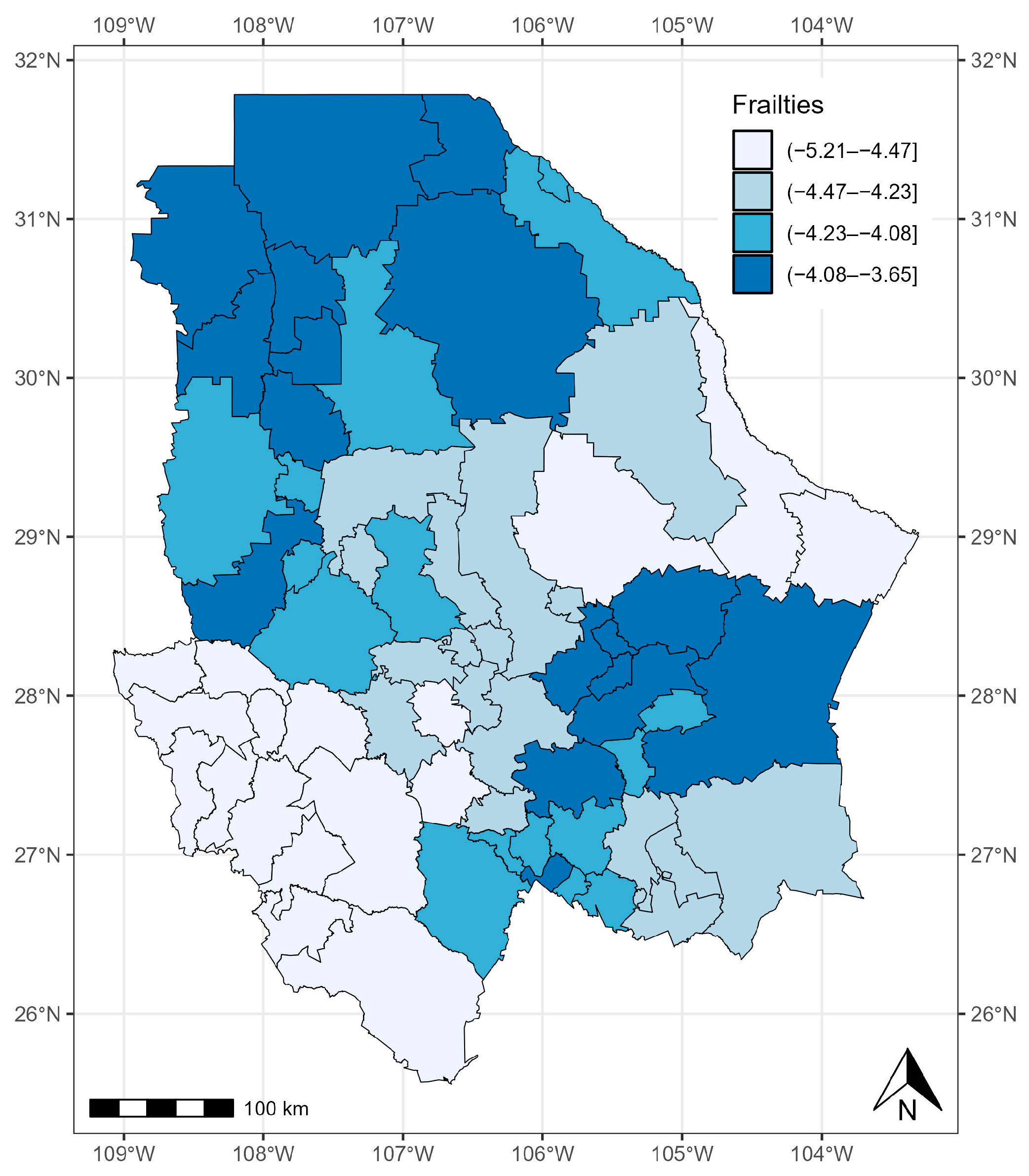
3.3. State of Chihuahua
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Maza-De La Torre, G.; Montelongo-Mercado, E.A.; Noyola-Villalobos, H.F.; García-Ruíz, A.; Hernández-Díaz, S.; Santiago-Torres, M.; Moreno-Delgado, L.F.; Carrera-Altamirano, R.; Muñoz-Monroy, E.; Martínez-Cuazitl, A.; et al. Epidemiología de los pacientes hospitalizados con COVID-19 en un hospital de tercer nivel. Gac. Médica México 2021, 157, 246–254. [Google Scholar] [CrossRef]
- Escobedo-de la Peña, J.; Rascón-Pacheco, R.A.; de Jesús Ascencio-Montiel, I.; González-Figueroa, E.; Fernández-Gárate, J.E.; Medina-Gómez, O.S.; Borja-Bustamante, P.; Santillán-Oropeza, J.A.; Borja-Aburto, V.H. Hypertension, diabetes and obesity, major risk factors for death in patients with COVID-19 in Mexico. Arch. Med. Res. 2021, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. COVID-19 in Latin America. Lancet Infect. Dis. 2020, 20, 547–548. [Google Scholar] [CrossRef]
- Piovani, D.; Nikolopoulos, G.K.; Bonovas, S. Pitfalls and perils of survival analysis under incorrect assumptions: The case of COVID-19 data. Biomedica 2021, 41, 21–28. [Google Scholar] [CrossRef]
- Salinas-Aguirre, J.E.; Sánchez-García, C.; Rodríguez-Sanchez, R.; Rodríguez-Muñoz, L.; Díaz-Castaño, A.; Bernal-Gómez, R. Clinical characteristics and comorbidities associated with mortality in patients with COVID-19 in Coahuila (Mexico). Rev. Clin. Esp. 2022, 222, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Escudero, G.; Carrillo-Vega, M.F.; Granados-García, V.; Martínez-Valverde, S.; Toledano-Toledano, F.; Garduño-Espinosa, J. A survival analysis of COVID-19 in the Mexican population. BMC Public. Health 2020, 20, 1616. [Google Scholar]
- Márquez-González, H.; Méndez-Galván, J.F.; Reyes-López, A.; Klünder-Klünder, M.; Jiménez-Juárez, R.; Garduño-Espinosa, J.; Solórzano-Santos, F. Coronavirus disease-2019 survival in Mexico: A cohort study on the interaction of the associated factors. Front. Public. Health 2021, 9, 1018. [Google Scholar] [CrossRef]
- Millán-Guerrero, R.O.; Caballero-Hoyos, R.; Monárrez-Espino, J. Poverty and survival from COVID-19 in Mexico. J. Public Health 2021, 43, 437–444. [Google Scholar] [CrossRef]
- Ahmed, F.E.; Vos, P.W.; Holbert, D. Modeling survival in colon cancer: A methodological review. Mol. Cancer 2007, 6, 15. [Google Scholar] [CrossRef]
- Kwon, J.; Sung, K.R.; Jo, J.; Yang, S.H. Glaucoma progression and its relationship with corrected and uncorrected intraocular pressure in eyes with history of refractive corneal surgery. Curr. Eye Res. 2018, 43, 1136–1144. [Google Scholar] [CrossRef]
- Guzmán Martínez, M.; Pérez-Castro, E.; Reyes-Carreto, R.; Acosta-Pech, R. Spatial Modeling in Epidemiology. In Recent Advances in Medical Statistics; IntechOpen: London, UK, 2022. [Google Scholar]
- Allotey, P.A.; Harel, O. Modeling geostatistical incomplete spatially correlated survival data with applications to COVID-19 mortality in Ghana. Spat. Stat. 2023, 54, 100730. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.M.; Rowlingson, B.S. Spatsurv: An R package for bayesian inference with spatial survival models. J. Stat. Softw. 2017, 77, 1–32. [Google Scholar] [CrossRef]
- Louzada, F.; Do Nascimento, D.C.; Egbon, O.A. Spatial statistical models: An overview under the bayesian approach. Axioms 2021, 10, 307. [Google Scholar] [CrossRef]
- Kirby, R.S.; Delmelle, E.; Eberth, J.M. Advances in spatial epidemiology and geographic information systems. Ann. Epidemiol. 2017, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Diggle, P.J.; Ribeiro, P.J. Model-Based Geostatistics; Springer: New York, NY, USA, 2007; p. 228. [Google Scholar]
- Xu, H. Comparing spatial and multilevel regression models for binary outcomes in neighborhood studies. Sociol. Methodol. 2014, 44, 229–272. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Wartenberg, D. Spatial epidemiology: Current approaches and future challenges. Environ. Health Perspect. 2004, 112, 998–1006. [Google Scholar] [CrossRef]
- Lin, C.H.; Wen, T.H. How Spatial Epidemiology Helps Understand Infectious Human Disease Transmission. Trop. Med. Infect. Dis. 2022, 7, 164. [Google Scholar] [CrossRef]
- Thamrin, S.A.; Jaya, A.K.; Mengersen, K. Bayesian spatial survival modelling for dengue fever in Makassar, Indonesia. Gac. Sanit. 2021, 35, S59–S63. [Google Scholar] [CrossRef]
- Lawson, A.B.; Banerjee, S.; Haining, R.; Ugarte, L. Handbook of Spatial Epidemiology; CRC Press: New York, NY, USA, 2016. [Google Scholar]
- Nunes, C.; Taylor, B.M. Modelling the time to detection of urban tuberculosis in two big cities in Portugal: A spatial survival analysis. Int. J. Tuberc. Lung Dis. 2016, 20, 1219–1225. [Google Scholar] [CrossRef]
- Henderson, R.; Shimakura, S.; Gorst, D. Modeling spatial variation in leukemia survival data. J. Am. Stat. Assoc. 2002, 97, 965–972. [Google Scholar] [CrossRef]
- Li, Y.; Lin, X. Semiparametric Normal Transformation Models for Spatially Correlated Survival Data. J. Am. Stat. Assoc. 2006, 101, 591–603. [Google Scholar] [CrossRef]
- Aswi, A.; Cramb, S.; Duncan, E.; Hu, W.; White, G.; Mengersen, K. Bayesian spatial survival models for hospitalisation of Dengue: A case study of Wahidin hospital in Makassar, Indonesia. Int. J. Environ. Res. Public Health 2020, 17, 878. [Google Scholar] [CrossRef]
- Mahanta, K.K.; Hazarika, J.; Barman, M.P.; Rahman, T. An application of spatial frailty models to recovery times of COVID-19 patients in India under Bayesian approach. J. Sci. Res. 2021, 65, 150–155. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, D.; He, C.Z. A hierarchical conditional autoregressive model for colorectal cancer survival data. Wiley Interdiscip. Rev. Comput. Stat. 2014, 6, 37–44. [Google Scholar] [CrossRef]
- Lu, W.; Ying, Z. On semiparametric transformation cure models. Biometrika 2004, 91, 331–343. [Google Scholar] [CrossRef]
- Daniel, K.; Onyango, N.O.; Sarguta, R.J. A spatial survival model for risk factors of Under-Five Child Mortality in Kenya. Int. J. Environ. Res. Public Health 2021, 19, 399. [Google Scholar] [CrossRef]
- Martins, R.; Silva, G.L.; Andreozzi, V. Bayesian joint modeling of longitudinal and spatial survival AIDS data. Stat. Med. 2016, 35, 3368–3384. [Google Scholar] [CrossRef]
- Schnell, P.; Bandyopadhyay, D.; Reich, B.J.; Nunn, M. A marginal cure rate proportional hazards model for spatial survival data. J. R. Stat. Soc. Ser. C Appl. Stat. 2015, 64, 673–691. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística e Informática. Censo de Población y Vivienda 2020; INEGI: Lima, Peru, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 15 December 2021).
- Ministry of Health. Datos Abiertos Bases Históricas. Dirección General de Epidemiología. 2020. (Secretaría de Salud). Available online: https://www.gob.mx/salud/documentos/datosabiertos-bases-historicas-direccion-general-de-epidemiologia (accessed on 25 November 2021).
- Zhou, H.; Hanson, T. A Unified Framework for fitting Bayesian semiparametric models to arbitrarily censored survival data, including spatially referenced data. J. Am. Stat. Assoc. 2018, 113, 571–581. [Google Scholar] [CrossRef]
- Zhou, H.; Hanson, T.; Zhang, J. SpBayesSurv: Fitting bayesian spatial survival models using R. J. Stat. Softw. 2020, 92. [Google Scholar] [CrossRef]
- Brooks, S.P.; Gelman, A. General methods for monitoring convergence of iterative simulations. J. Comput. Graph. Stat. 1998, 7, 434–455. [Google Scholar]
- Gelman, A.; Rubin, D.B. Inference from iterative simulation using multiple sequences. Stat. Sci. 1992, 7, 457–511. [Google Scholar] [CrossRef]
- Plummer, M.; Best, N.; Cowles, K.; Vines, K. Coda: Convergence diagnosis and output analysis for MCMC. R News 2006, 6, 7–11. [Google Scholar]
- Lee, E.T.; Wang, J. Statistical Methods for Survival Data Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2003; Volume 476. [Google Scholar]
- Klein, J.P.; Moeschberger, M.L. Survival Analysis: Techniques for Censored and Truncated Data; Springer: New York, NY, USA, 1997. [Google Scholar]
- Perera, M.; Tsokos, C. A statistical model with non-linear effects and non-proportional hazards for breast cancer survival analysis. Adv. Breast Cancer Res. 2018, 7, 65–89. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van Der Linde, A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B Stat. Methodol. 2002, 64, 583–639. [Google Scholar] [CrossRef]
- Watanabe, S. Asymptotic equivalence of Bayes cross validation and widely applicable information criterion in singular learning theory. J. Mach. Learn Res. 2010, 11, 3571–3594. [Google Scholar]
- Geisser, S.; Eddy, W.F. A predictive approach to model selection. J. Am. Stat. Assoc. 1979, 74, 153–160. [Google Scholar] [CrossRef]
- Pérez-Sastré, M.A.; Valdés, J.; Ortiz-Hernández, L. Clinical characteristics and severity of COVID-19 among Mexican adults. Gac. Med. Mex. 2020, 156, 373–381. [Google Scholar] [CrossRef]
- Plasencia Urizarri, T.M.; Aguilera Rodríguez, R.; Almaguer Mederos, L.E. Comorbilidades y gravedad clínica de la COVID-19: Revisión sistemática y meta-análisis. Rev. Habanera Cienc. Médicas 2020, 19, 1–17. [Google Scholar]
- Instituto Nacional de Salud Pública. Encuesta Nacional de Salud y Nutrición (ENSANUT); Instituto Nacional de Salud Pública: Mexico City, Mexico, 2018. [Google Scholar]
- Kammar-Garcia, A.; Vidal-Mayo, J.D.J.; Vera-Zertuche, J.M.; Lazcano-Hernandez, M.; Vera-Lopez, O.; Segura-Badilla, O.; Aguilar-Alonso, P.; Navarro-Cruz, A.R. Impact of comorbidities in Mexican SARS-CoV-2-positive patients: A retrospective analysis in a national cohort. Rev. Investig. Clin. 2020, 72, 151–158. [Google Scholar] [CrossRef]
- Muñoz, X.; Pilia, F.; Ojanguren, I.; Romero-Mesones, C.; Cruz, M.-J. Is asthma a risk factor for COVID-19? Are phenotypes important? ERJ Open Res. 2021, 7, 00216–02020. [Google Scholar] [CrossRef] [PubMed]
- Farne, H.; Singanayagam, A. Why asthma might surprisingly protect against poor outcomes in COVID-19. Eur. Respir. J. 2020, 56, 2003045. [Google Scholar] [CrossRef] [PubMed]
- Liuzzo Scorpo, M.; Ferrante, G.; La Grutta, S. An Overview of Asthma and COVID-19: Protective factors against SARS-CoV-2 in pediatric patients. Front. Pediatr. 2021, 9, 661206. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Hernández, L.; Pérez-Sastré, M.A. Inequidades sociales en la progresión de la COVID-19 en población mexicana. Rev. Panam. Salud Publica 2020, 44, 1. [Google Scholar] [CrossRef]
- Tan, T.Q.; Kullar, R.; Swartz, T.H.; Mathew, T.A.; Piggott, D.A.; Berthaud, V. Location matters: Geographic disparities and impact of Coronavirus disease 2019. J. Infect. Dis. 2020, 222, 1951–1954. [Google Scholar] [CrossRef]
- Deb Nath, N.; Khan, M.M.; Schmidt, M.; Njau, G.; Odoi, A. Geographic disparities and temporal changes of COVID-19 incidence risks in North Dakota, United States. BMC Public Health 2023, 23, 720. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Code | Description |
|---|---|---|
| Age | Number of years | Patient’s age |
| Gender | 1: Male; 2: Female | Identifies the gender of the patient |
| Pneumonia | 1: Yes; 2: No | Indicates if the patient has pneumonia |
| Diabetes | 1: Yes; 2: No | Indicates if the patient has diabetes |
| Chronic obstructive pulmonary disease | 1: Yes; 2: No | Indicates if the patient has COPD |
| Cardiovascular disease | 1: Yes; 2: No | Indicates if the patient has CVD |
| Obesity | 1: Yes; 2: No | Indicates if the patient has obesity |
| Asthma | 1: Yes; 2: No | Indicates if the patient has asthma |
| Chronic renal disease | 1: Yes; 2: No | Indicates if the patient has CKD |
| Hypertension | 1: Yes; 2: No | Indicates if the patient has hypertension |
| Variable | Mean | Median | 95% CrI | CrI-Upper | |
|---|---|---|---|---|---|
| Age | 0.042 | 0.042 | (0.041, 0.043) ** | 1.01 | 1.02 |
| Sex (male) | 0.341 | 0.341 | (0.308, 0.373) ** | 1.00 | 1.01 |
| Pneumonia | 1.680 | 1.679 | (1.645, 1.719) ** | 1.00 | 1.02 |
| Diabetes | 0.164 | 0.164 | (0.130, 0.197) ** | 1.01 | 1.03 |
| COPD | 0.017 | 0.017 | (−0.066, 0.096) | 1.00 | 1.00 |
| CVD | −0.096 | −0.094 | (−0.186, −0.011) ** | 1.01 | 1.04 |
| Obesity | 0.129 | 0.129 | (0.085, 0.170) ** | 1.01 | 1.07 |
| Asthma | −0.228 | −0.226 | (−0.389, −0.081) ** | 1.02 | 1.08 |
| CKD | 0.463 | 0.463 | (0.394, 0.535) ** | 1.01 | 1.05 |
| Hypertension | 0.063 | 0.064 | (0.026, 0.098) ** | 1.00 | 1.00 |
| 0.068 | 0.066 | (0.036, 0.110) ** | 1.66 | 2.97 | |
| 1.551 | 1.464 | (0.901, 2.692) ** | 1.01 | 1.05 | |
| 0.273 | 0.263 | (0.133, 0.470) ** | 1.01 | 1.03 | |
| −4.167 | −4.173 | (−4.182, −4.131) ** | - | - | |
| −0.059 | -0.061 | (−0.071, −0.045) ** | - | - |
| Variable | Mean | Median | 95% CrI | CrI-Upper | |
|---|---|---|---|---|---|
| Age | 0.035 | 0.035 | (0.033, 0.037) ** | 1.00 | 1.00 |
| Sex (Male) | 0.191 | 0.192 | (0.127, 0.252) ** | 1.00 | 1.00 |
| Pneumonia | 2.819 | 2.818 | (2.718, 2.913) ** | 1.00 | 1.01 |
| Diabetes | 0.304 | 0.305 | (0.239, 0.368) ** | 1.00 | 1.00 |
| COPD | 0.140 | 0.140 | (0.001, 0.277) ** | 1.00 | 1.00 |
| CVD | 0.206 | 0.206 | (0.063, 0.354) ** | 1.00 | 1.00 |
| Obesity | 0.219 | 0.218 | (0.146, 0.296) ** | 1.00 | 1.00 |
| Asthma | −0.120 | −0.119 | (−0.343, 0.103) | 1.00 | 1.02 |
| CKD | 0.196 | 0.197 | (0.073, 0.325) ** | 1.01 | 1.03 |
| Hypertension | 0.070 | 0.071 | (0.004, 0.132) ** | 1.00 | 1.00 |
| 0.076 | 0.072 | (0.041, 0.126) ** | 1.03 | 1.11 | |
| 1.838 | 1.731 | (1.072, 3.166) ** | 1.00 | 1.00 | |
| 0.083 | 0.077 | (0.032, 0.163) ** | 1.00 | 1.00 | |
| −4.315 | −4.280 | (−4.520, −4.198) ** | - | - | |
| 0.174 | 0.174 | (0.152, 0.208) ** | - | - |
| Variable | Mean | Median | 95% CrI | CrI-Upper | |
|---|---|---|---|---|---|
| Age | 0.048 | 0.048 | (0.046, 0.050) ** | 1.01 | 1.03 |
| Sex (male) | 0.310 | 0.310 | (0.257, 0.365) ** | 1.00 | 1.00 |
| Pneumonia | 1.689 | 1.688 | (1.630, 1.750) ** | 1.00 | 1.02 |
| Diabetes | 0.341 | 0.341 | (0.283, 0.401) ** | 1.00 | 1.00 |
| COPD | 0.068 | 0.070 | (−0.072, 0.209) | 1.00 | 1.00 |
| CVD | −0.021 | −0.022 | (−0.130, 0.087) | 1.00 | 1.00 |
| Obesity | 0.277 | 0.277 | (0.211, 0.342) ** | 1.00 | 1.00 |
| Asthma | −0.141 | −0.144 | (−0.313, 0.029) | 1.00 | 1.00 |
| CKD | 0.531 | 0.533 | (0.420, 0.633) ** | 1.00 | 1.01 |
| Hypertension | 0.245 | 0.245 | (0.183, 0.301) ** | 1.00 | 1.00 |
| 0.099 | 0.096 | (0.051, 0.160) ** | 1.00 | 1.01 | |
| 2.158 | 2.035 | (1.261, 3.724) ** | 1.00 | 1.01 | |
| 0.099 | 0.093 | (0.043, 0.185) ** | 1.00 | 1.01 | |
| −4.384 | −4.362 | (−4.593, −4.286) ** | |||
| 0.155 | 0.159 | (0.133, 0.178) ** |
| State | PH Model | DIC | WAIC | LPML |
|---|---|---|---|---|
| State of México | Spatial | 186,805.2 | 186,809.3 | −93,404.61 |
| Cox | 193,904.9 | 194,385.3 | −97,192.46 | |
| Guerrero | Spatial | 46,866.87 | 46,871.20 | −23,435.59 |
| Cox | 48,396.29 | 48,395.89 | −24,197.94 | |
| Chihuahua | Spatial | 63,225.16 | 63,232.3 | −31,616.2 |
| Cox | 65,013.54 | 65,014.24 | −32,507.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Castro, E.; Guzmán-Martínez, M.; Godínez-Jaimes, F.; Reyes-Carreto, R.; Vargas-de-León, C.; Aguirre-Salado, A.I. Spatial Survival Model for COVID-19 in México. Healthcare 2024, 12, 306. https://doi.org/10.3390/healthcare12030306
Pérez-Castro E, Guzmán-Martínez M, Godínez-Jaimes F, Reyes-Carreto R, Vargas-de-León C, Aguirre-Salado AI. Spatial Survival Model for COVID-19 in México. Healthcare. 2024; 12(3):306. https://doi.org/10.3390/healthcare12030306
Chicago/Turabian StylePérez-Castro, Eduardo, María Guzmán-Martínez, Flaviano Godínez-Jaimes, Ramón Reyes-Carreto, Cruz Vargas-de-León, and Alejandro Iván Aguirre-Salado. 2024. "Spatial Survival Model for COVID-19 in México" Healthcare 12, no. 3: 306. https://doi.org/10.3390/healthcare12030306
APA StylePérez-Castro, E., Guzmán-Martínez, M., Godínez-Jaimes, F., Reyes-Carreto, R., Vargas-de-León, C., & Aguirre-Salado, A. I. (2024). Spatial Survival Model for COVID-19 in México. Healthcare, 12(3), 306. https://doi.org/10.3390/healthcare12030306