
A Single-Center Analysis of Patient Characteristics and Overall Survival in Patients with Resectable Gallbladder Cancer


Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Demographic, Clinical, Pathological, and Survival Data Collection
2.3. Statistical Analysis
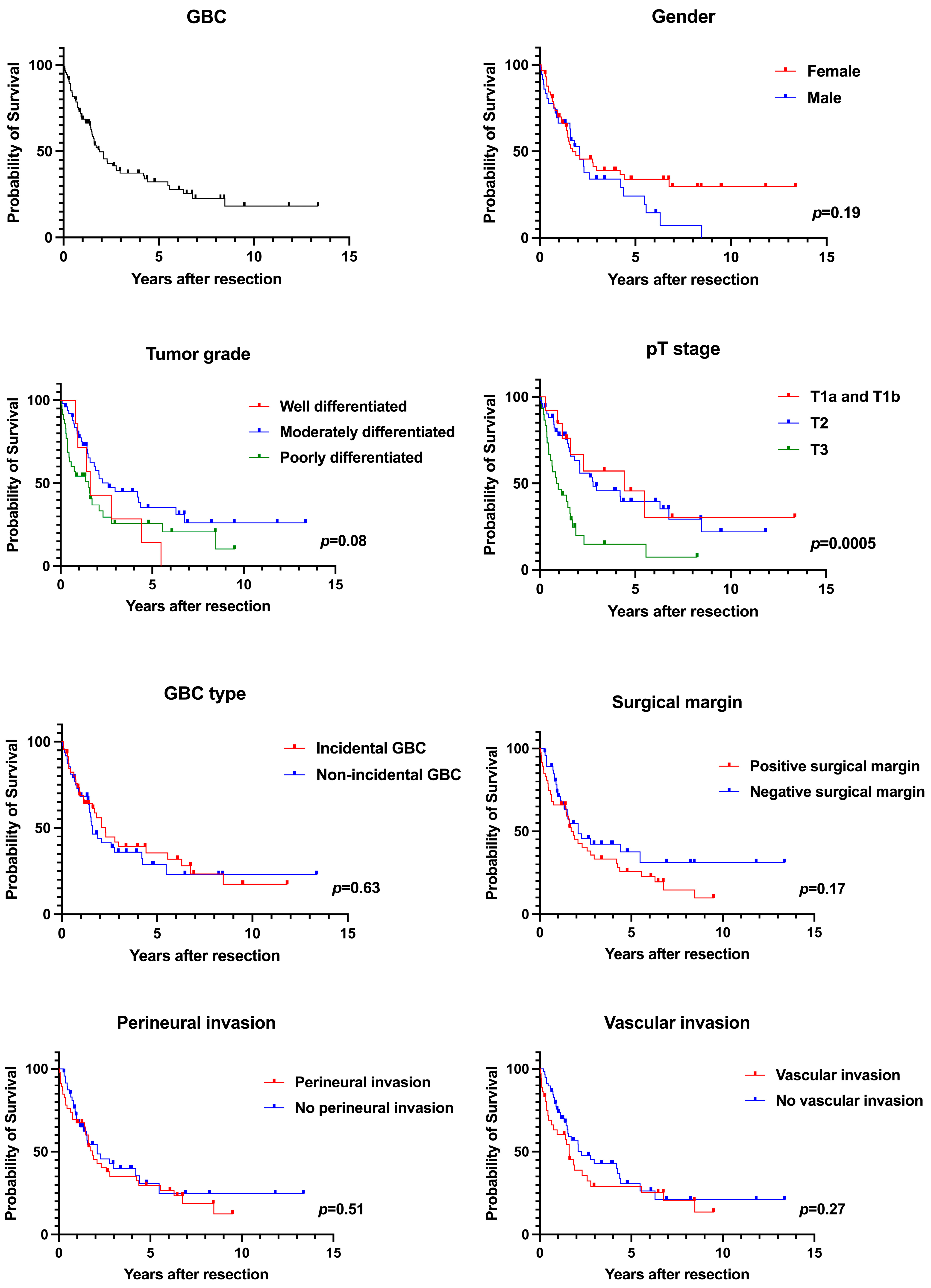
3. Results
3.1. Sex Disparities in GBC
3.2. Adjuvant Chemotherapy and Radiotherapy
3.3. Incidental vs. Non-Incidental GBC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Thandra, K.C.; Barsouk, A. Epidemiology of gallbladder cancer. Clin. Exp. Hepatol. 2019, 5, 93–102. [Google Scholar] [CrossRef] [PubMed]
- de Bitter, T.J.J.; de Reuver, P.R.; Lohman, E.A.J.d.S.; Kroeze, L.I.; Vink-Börger, M.E.; van Vliet, S.; Simmer, F.; von Rhein, D.; Jansen, E.A.M.; Verheij, J.; et al. Comprehensive clinicopathological and genomic profiling of gallbladder cancer reveals actionable targets in half of patients. npj Precis. Oncol. 2022, 6, 83. [Google Scholar] [CrossRef] [PubMed]
- Vega, E.A.; Mellado, S.; Salehi, O.; Freeman, R.; Conrad, C. Treatment of Resectable Gallbladder Cancer. Cancers 2022, 14, 1413. [Google Scholar] [CrossRef] [PubMed]
- Stinton, L.M.; Shaffer, E.A. Epidemiology of gallbladder disease: Cholelithiasis and cancer. Gut Liver 2012, 6, 172–187. [Google Scholar] [CrossRef]
- Huang, J.; Patel, H.K.; Boakye, D.; Chandrasekar, V.T.; Koulaouzidis, A.; Iii, D.E.L.-P.; Ngai, C.H.; Pun, C.N.; Bai, Y.; Lok, V.; et al. Worldwide distribution, associated factors, and trends of gallbladder cancer: A global country-level analysis. Cancer Lett. 2021, 521, 238–251. [Google Scholar] [CrossRef]
- Ouyang, G.; Liu, Q.; Wu, Y.; Liu, Z.; Lu, W.; Li, S.; Pan, G.; Chen, X. The global, regional, and national burden of gallbladder and biliary tract cancer and its attributable risk factors in 195 countries and territories, 1990 to 2017: A systematic analysis for the Global Burden of Disease Study 2017. Cancer 2021, 127, 2238–2250. [Google Scholar] [CrossRef]
- Kashyap, L.; Singh, A.; Tomar, S.; Gupta, A.; Sansar, B.; Chaudhary, A.K.; Mishra, B.K.; Sambasivaiah, K.; Kapoor, A. Pattern of Care and Outcomes of Gallbladder Cancer Patients: Retrospective Study from a High Incidence Region in India. South Asian J. Cancer 2023, 12, 245–249. [Google Scholar] [CrossRef]
- Kumar, A.; Sarangi, Y.; Gupta, A.; Sharma, A. Gallbladder cancer: Progress in the Indian subcontinent. World J. Clin. Oncol. 2024, 15, 695–716. [Google Scholar] [CrossRef]
- Henley, S.J.; Weir, H.K.; Jim, M.A.; Watson, M.; Richardson, L.C. Gallbladder Cancer Incidence and Mortality, United States 1999–2011. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1319–1326. [Google Scholar] [CrossRef]
- SEER*Explorer: An Interactive Website for SEER Cancer Statistics. Surveillance Research Program, National Cancer Institute. 17 April 2024. Available online: https://seer.cancer.gov/statistics-network/explorer/ (accessed on 20 April 2024).
- Choi, K.S.; Choi, S.B.; Park, P.; Kim, W.B.; Choi, S.Y. Clinical characteristics of incidental or unsuspected gallbladder cancers diagnosed during or after cholecystectomy: A systematic review and meta-analysis. World J. Gastroenterol. 2015, 21, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, B.; Zheng, C.; Liu, W.; Hong, T.; He, X. Incidental gallbladder cancer after laparoscopic cholecystectomy: Incidence, management, and prognosis. Asia Pac. J. Clin. Oncol. 2020, 16, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.-N.; Song, M.; Lee, J.H.; Song, K.B.; Hwang, D.W.; Ahn, C.-S.; Hwang, S.; Hong, S.-M. Validation of the 8th Edition of the American Joint Committee on Cancer Staging System for Gallbladder Cancer and Implications for the Follow-up of Patients without Node Dissection. Cancer Res. Treat. 2020, 52, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Yang, J.D.; Peeraphatdit, T.; Roberts, L.R. The incidence rates and survival of gallbladder cancer in the USA. Eur. J. Cancer Prev. 2019, 28, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Hong, T.S.; Hezel, A.F.; Kooby, D.A. Current Management of Gallbladder Carcinoma. Oncologist 2010, 15, 168–181. [Google Scholar] [CrossRef]
- Sturm, N.; Schuhbaur, J.S.; Hüttner, F.; Perkhofer, L.; Ettrich, T.J. Gallbladder Cancer: Current Multimodality Treatment Concepts and Future Directions. Cancers 2022, 14, 5580. [Google Scholar] [CrossRef]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef]
- Ozer, M.; Goksu, S.Y.; Sanford, N.N.; Porembka, M.; Khurshid, H.; Ahn, C.; Maxwell, M.C.; Beg, M.S.; Kazmi, S.M. A Propensity Score Analysis of Chemotherapy Use in Patients with Resectable Gallbladder Cancer. JAMA Netw. Open 2022, 5, e2146912. [Google Scholar] [CrossRef]
- Hakeem, A.R.; Papoulas, M.; Menon, K.V. The role of neoadjuvant chemotherapy or chemoradiotherapy for advanced gallbladder cancer—A systematic review. Eur. J. Surg. Oncol. 2019, 45, 83–91. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Barmpounakis, P.; Demiris, N.; Jah, A.; Spiers, H.V.; Talukder, S.; Martin, J.L.; Gibbs, P.; Harper, S.J.; Huguet, E.L.; et al. Surgical outcomes of gallbladder cancer: The OMEGA retrospective, multicentre, international cohort study. eClinicalMedicine 2023, 59, 101951. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kim, S.H.; Park, S.; Han, S.; Kim, Y.; Lee, K.; Lee, W.J.; Woo, S.M.; Kim, T. Adjuvant chemoradiation therapy in gallbladder cancer. J. Surg. Oncol. 2010, 102, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, D.A.; Wong, P.; Chen, Y.-J.; Singh, G.P.; Fong, Y.; Li, D.; Ituarte, P.H.G.; Melstrom, L.G. Adjuvant Chemoradiation in Resected Biliary Adenocarcinoma: Evaluation of SWOG S0809 with a Large National Database. Ann. Surg. Oncol. 2024, 31, 4896–4904. [Google Scholar] [CrossRef]
- Alarabiyat, M.; Raza, S.S.; Isaac, J.; Mirza, D.; Marudanayagam, R.; Roberts, K.; Abradelo, M.; Bartlett, D.C.; Dasari, B.V.; Sutcliffe, R.P.; et al. Incidental gallbladder cancer diagnosis confers survival advantage irrespective of tumour stage and characteristics. World J. Gastroenterol. 2022, 28, 1996–2007. [Google Scholar] [CrossRef] [PubMed]
- Mazer, L.M.; Losada, H.F.; Chaudhry, R.M.; Velazquez-Ramirez, G.A.; Donohue, J.H.; Kooby, D.A.; Nagorney, D.M.; Adsay, N.V.; Sarmiento, J.M. Tumor Characteristics and Survival Analysis of Incidental Versus Suspected Gallbladder Carcinoma. J. Gastrointest. Surg. 2012, 16, 1311–1317. [Google Scholar] [CrossRef]
- Pyo, J.-S.; Son, B.K.; Lee, H.Y.; Oh, I.W.; Chung, K.H. Incidental Carcinoma after Cholecystectomy for Benign Disease of the Gallbladder: A Meta-Analysis. J. Clin. Med. 2020, 9, 1484. [Google Scholar] [CrossRef]

{kind=link}
| All Patients (n = 94) | n (%) or Median (IQR) |
|---|---|
| Female sex | 58 (61.7%) |
| Age (years) | 71 (61.8–77.0) |
| Race | |
| White | 71 (75.5%) |
| Black | 23 (24.5%) |
| Tumor characteristics | |
| Tumor size (cm) | 3.3 (1.9–5.0) |
| Tumor histology | |
| Adenocarcinoma | 91 (96.8%) |
| Squamous cell carcinoma | 2 (2.1%) |
| Adenosquamous cell carcinoma | 1 (1.1%) |
| Incidental GBC | 46 (48.9%) |
| Perineural invasion | 46 (48.9%) |
| Vascular invasion | 36 (38.3%) |
| Positive surgical margin | 47 (50%) |
| Tumor grade of differentiation (n = 92) | |
| Grade I (well differentiated) | 7 (7.6%) |
| Grade II (moderately differentiated) | 49 (53.3%) |
| Grade III (poorly differentiated) | 36 (39.1%) |
| T-stage a | |
| pT1a | 2 (2.1%) |
| pT1b | 11 (11.7%) |
| pT2 | 51 (54.3%) |
| pT3 | 30 (31.9%) |
| Treatment | |
| Adjuvant chemotherapy | 57 (60.6%) |
| Adjuvant radiotherapy | 16 (17.0%) |
| Neoadjuvant chemotherapy | 3 (3.2%) |
| Clinical characteristics | |
| Cholelithiasis | 74 (78.7%) |
| Gallbladder polyp | 12 (12.8%) |
| Inflammatory bowel disease | 3 (3.2%) |
| Hypertension | 67 (71.3%) |
| Diabetes mellitus | 25 (26.6%) |
| Tobacco use | 43 (45.7%) |
| Alcohol use | 20 (21.3%) |
| BMI (kg/m2) | 28.8 (25.1–36.6) |
| Laboratory variables | |
| AST (IU/L) | 35.5 (23.0–75.3) |
| ALT (IU/L) | 33.0 (18.8–68.0) |
| ALP (IU/L) | 102 (78.8–153) |
| Albumin (g/dL) | 3.6 (3.1–4.1) |
| Total bilirubin (mg/dL) | 0.7 (0.5–1.0) |
| Direct bilirubin | 0.3 (0.2–0.65) |
| Creatinine (mg/dL) | 0.8 (0.7–1.0) |
| GFR (mL/min/1.73 m2) | 83.0 (63.0–93.0) |
| Hemoglobin (g/dL) | 12.6 (10.9–13.5) |
| Platelet (×109/L) | 244 (193–317) |
| Duration from surgery to death, days (n = 62) | 463 (166–783) |
| Variables (%) | Median Survival (Years) | p Value (Log-Rank) |
|---|---|---|
| Sex | 0.19 | |
| Female (61.7%) | 1.7 | |
| Male (38.3%) | 2.1 | |
| Race | 0.37 | |
| White (75.5%) | 1.8 | |
| Black (24.5%) | 3.0 | |
| Tumor characteristics | ||
| Tumor grade of differentiation | 0.08 | |
| Grade I (well differentiated) (7.6%) | 1.6 | |
| Grade II (moderately differentiated) (53.3%) | 2.6 | |
| Grade III (poorly differentiated) (39.1%) | 1.5 | |
| T-stage a | 0.0005 | |
| T1a (2.1%) and T1b (11.7%) | 4.4 | |
| T2 (54.3%) | 2.8 | |
| T3 (31.9%) | 0.9 | |
| Vascular invasion | 0.27 | |
| Present (38.3%) | 1.6 | |
| Absent (61.7%) | 2.3 | |
| Perineural invasion | 0.51 | |
| Present (48.9%) | 1.8 | |
| Absent (51.1%) | 2.1 | |
| Surgical margin | 0.17 | |
| Positive (50%) | 1.7 | |
| Negative (50%) | 2.1 | |
| Metastasis | 0.08 | |
| Yes (54.3%) | 1.6 | |
| No (45.7%) | 2.9 | |
| Clinical characteristics | ||
| Cholelithiasis | 0.76 | |
| Yes (78.7%) | 1.9 | |
| No (21.3%) | 2.1 | |
| Gallbladder polyp | 0.15 | |
| Yes (12.8%) | 5.5 | |
| No (87.2%) | 1.7 | |
| Hypertension | 0.94 | |
| Yes (71.3%) | 1.7 | |
| No (28.7%) | 2.3 | |
| Diabetes mellitus | 0.34 | |
| Yes (26.6%) | 2.1 | |
| No (73.4%) | 1.9 | |
| Alcohol use | 0.28 | |
| Yes (21.3%) | 2.8 | |
| No (78.7%) | 1.7 | |
| BMI (kg/m2) | 0.13 | |
| 18.5–24.9 (20.2%) | 1.4 | |
| 25.0–29.9 (34.0%) | 1.8 | |
| ≥30 (45.7%) | 2.8 | |
| Treatment | ||
| Adjuvant Chemotherapy | 0.20 | |
| Yes (60.6%) | 2.1 | |
| No (39.4%) | 1.1 | |
| Adjuvant Radiotherapy | 0.36 | |
| Yes (17%) | 2.1 | |
| No (83%) | 1.9 |
| Variables | Incidental GBC (n = 46, 48.9%) | Non-Incidental GBC (n = 48, 51.1%) | p Value |
|---|---|---|---|
| Female sex | 28 (60.9%) | 30 (62.5%) | 0.97 |
| Age (years) | 71 (64–77) | 71 (61–77) | 0.96 |
| Clinical characteristics | |||
| Cholelithiasis | 42 (91.3%) | 32 (66.7%) | 0.002 |
| Gallbladder polyp | 4 (8.7%) | 8 (16.7%) | 0.25 |
| Inflammatory bowel disease | 0 (0%) | 3 (6.3%) | 0.08 |
| Hypertension | 30 (65.2%) | 37 (77.1%) | 0.21 |
| Diabetes mellitus | 12 (26.1%) | 13 (27.1%) | 0.91 |
| Tobacco use | 27 (58.7%) | 21 (43.8%) | 0.15 |
| Alcohol use | 11 (23.9%) | 9 (18.8%) | 0.55 |
| Laboratory variables | |||
| Hemoglobin (g/dL) | 13 (11–14) | 12 (11–14) | 0.37 |
| Platelet (×109/L) | 238 (202–276) | 262 (185–345) | 0.16 |
| AST (IU/L) | 48 (23–78) | 29 (23–69) | 0.50 |
| ALT (IU/L) | 34 (18–75) | 32 (21–64) | 0.86 |
| ALP (IU/L) | 101 (68–150) | 102 (81–176) | 0.72 |
| Albumin (g/dL) | 3.6 (3.2–4.1) | 3.6 (3.1–4.0) | 0.98 |
| Total bilirubin (mg/dL) | 0.75 (0.5–1) | 0.7 (0.4–1) | 0.93 |
| Creatinine (mg/dL) | 0.8 (0.7–1) | 0.8 (0.6–1.1) | 0.63 |
| GFR (mL/min/1.73 m2) | 83 (64–92) | 84 (62–96) | 0.97 |
| Tumor characteristics | |||
| Tumor size (cm) | 2.7 (1.7–4.8) | 4 (2–5.4) | 0.47 |
| Vascular invasion | 19 (41.3%) | 17 (35.4%) | 1.00 |
| Perineural invasion | 26 (56.5%) | 20 (41.7%) | 0.69 |
| Positive surgical margin | 27 (58.7%) | 20 (41.7%) | 0.17 |
| Adjuvant chemotherapy | 28 (60.9%) | 29 (60.4%) | 0.94 |
| Adjuvant radiotherapy | 7 (15.2%) | 9 (18.8%) | 0.69 |
| Death | 31 (67.4%) | 31 (64.6%) | 0.78 |
| Duration between surgery and death (days) | 428 (164–1018) | 498 (166–588) | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Öztürk, N.B.; Dadamyan, A.; Jamil, L.H. A Single-Center Analysis of Patient Characteristics and Overall Survival in Patients with Resectable Gallbladder Cancer. Healthcare 2024, 12, 2091. https://doi.org/10.3390/healthcare12202091
Öztürk NB, Dadamyan A, Jamil LH. A Single-Center Analysis of Patient Characteristics and Overall Survival in Patients with Resectable Gallbladder Cancer. Healthcare. 2024; 12(20):2091. https://doi.org/10.3390/healthcare12202091
Chicago/Turabian StyleÖztürk, N. Begüm, Artem Dadamyan, and Laith H. Jamil. 2024. "A Single-Center Analysis of Patient Characteristics and Overall Survival in Patients with Resectable Gallbladder Cancer" Healthcare 12, no. 20: 2091. https://doi.org/10.3390/healthcare12202091
APA StyleÖztürk, N. B., Dadamyan, A., & Jamil, L. H. (2024). A Single-Center Analysis of Patient Characteristics and Overall Survival in Patients with Resectable Gallbladder Cancer. Healthcare, 12(20), 2091. https://doi.org/10.3390/healthcare12202091