
Drug-Related Problems Detected in Complex Chronic Patients by Community Pharmacists of Catalonia: Perception of the Person-Centred Approach Necessity

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Variables
2.3. Statistical Analysis
2.4. Ethics Approval and Informed Consent
3. Results
3.1. Patient Profile
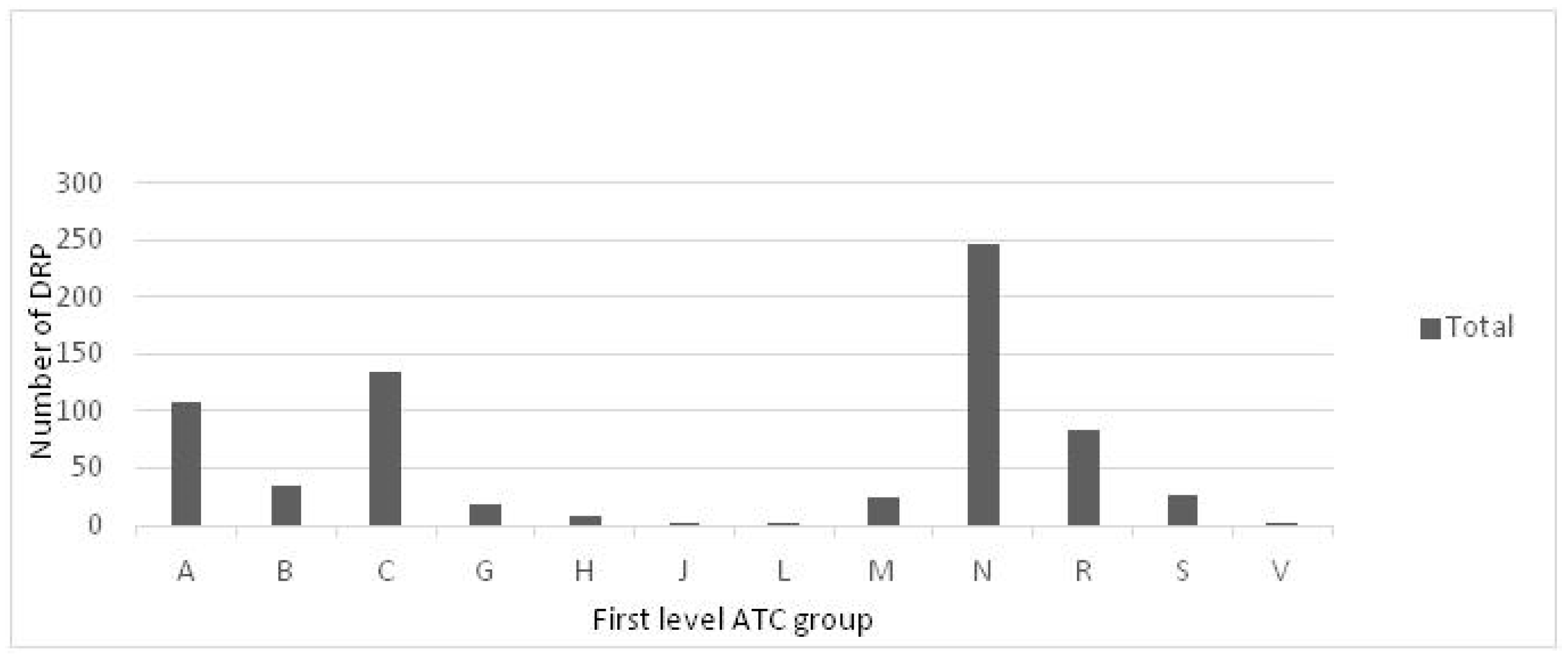
3.2. Prevalence and Type of Drug-Related Problem
3.3. Adherence
3.4. Pharmacists’ Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Medication Errors: Technical Series on Safer Primary Care; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241511643 (accessed on 25 September 2023).
- Kim, S.; Bennett, K.; Wallace, E.; Fahey, T.; Cahir, C. Measuring medication adherence in older community-dwelling patients with multimorbidity. Eur. J. Clin. Pharmacol. 2018, 74, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Von Buedingen, F.; Hammer, M.S.; Meid, A.D.; Müller, W.E.; Gerlach, F.M.; Muth, C. Changes in prescribed medicines in older patients with multimorbidity and polypharmacy in general practice. BMC Fam. Pract. 2018, 19, 131. [Google Scholar] [CrossRef]
- Kingston, A.; Robinson, L.; Booth, H.; Knapp, M.; Jagger, C.; MODEM project. Projections of multi-morbidity in the older population in England to 2035: Estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing 2018, 47, 374–380. [Google Scholar] [CrossRef]
- Puspitasari, H.P.; Aslani, P.; Krass, I. Challenges in the management of chronic noncommunicable diseases by Indonesian community pharmacists. Pharm. Pract. 2015, 13, 578. [Google Scholar] [CrossRef] [PubMed]
- Jódar-Sánchez, F.; Malet-Larrea, A.; Martín, J.J.; García-Mochón, L.; López del Amo, M.P.; Martínez-Martínez, F.; Gastelurrutia-Garralda, M.A.; Garcia-Cardenas, V.; Sabater-Hernández, D.; Sáez-Benito, L.; et al. Cost-utility analysis of a medication review with follow-up service for older adults with polypharmacy in community pharmacies in Spain: The conSIGUE program. Pharmacoeconomics 2015, 33, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Apikoglu-Rabus, S.; Yesilyaprak, G.; Izzettin, F.V. Drug-related problems and pharmacist interventions in a cohort of patients with asthma and chronic obstructive pulmonary disease. Respir. Med. 2016, 120, 109–115. [Google Scholar]
- Oni, T.; McGrath, N.; BeLue, R.; Roderick, P.; Colagiuri, S.; May, C.R.; Levitt, N.S. Chronic diseases and multi-morbidity—A conceptual modification to the WHO ICCC model for countries in health transition. BMC Public Health 2014, 14, 575. [Google Scholar] [CrossRef]
- Pehlivanli, A.; Eyupoglu, S.; Basgut, B.; Erturk, S.; Ozcelikay, A.T. Impact of a multidisciplinary approach involving clinical pharmacist on resolving drug related problems in chronic kidney patients: A prospective interventional study. BMC Nephrol. 2023, 24, 149. [Google Scholar]
- Alruqayb, W.S.; Price, M.J.; Paudyal, V.; Cox, A.R. Drug-related problems in hospitalised patients with chronic kidney disease: A systematic review. Drug Saf. 2021, 44, 1041–1045. [Google Scholar]
- World Health Organization (WHO). Rational Use of Medicines: Progress in Implementing the WHO Medicines Strategy. Bull World Health Organ. 2006. Available online: https://apps.who.int/gb/ebwha/pdf_files/EB118/B118_6-en.pdf (accessed on 25 September 2023).
- Catsalut. Servei Català de la Salut. Pharmaceutical Billing Reports. Available online: https://catsalut.gencat.cat/ca/proveidors-professionals/farmacia-medicaments/prestacio-farmaceutica/informes-facturacio/ (accessed on 25 September 2023). (In Catalan).
- Generalitat de Catalunya. IDESCAT. Statistics Institute of Catalonia. Population on January 1st. By Sex and Age Groups. 2023. Available online: https://www.idescat.cat/indicadors/?id=aec&n=15231 (accessed on 25 September 2023). (In Catalan).
- Allemann, S.S.; van Mil, J.W.; Botermann, L.; Berger, K.; Griese, N.; Hersberger, K.E. Pharmaceutical care: The PCNE definition 2013. Int. J. Clin. Pharm. 2014, 36, 544–555. [Google Scholar] [CrossRef]
- World Pharmacy Council. Sector Analysis Report 2023. Available online: https://d2s3n99uw51hng.cloudfront.net/static/2023%20WPC%20Sector%20Analysis%20Report%20-%20Public%20Version.pdf (accessed on 20 December 2023).
- General Council of Official Pharmaceutical Associations. Forum of Pharmaceutical Care in Community Pharmacy (Foro AF-FC), Practical Guide to Pharmaceutical Care Services in Community Pharmacy. 2010. Available online: https://www.farmaceuticos.com/wp-content/uploads/2020/02/ATFC_Guia-FORO-1.pdf (accessed on 25 September 2023).
- Nolte, E.; Merkur, S.; Anell, A.; European Observatory on Health Systems and Policies (Eds.) Achieving Person-Centred Health Systems: Evidence, Strategies and Challenges; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2020; ISBN 978-1-108-79006-2. [Google Scholar]
- World Health Organization. WHO, Global Strategy on Integrated People—Centred Health Services 2016–2026. Executive Summary: Placing People and Communities at the Centre of Health Services. 2015. Available online: https://africahealthforum.afro.who.int/firstedition/IMG/pdf/the_global_strategy_for_integrated_people_centred_health_services.pdf (accessed on 22 November 2023).
- Twigg, M.J.; Wright, D.; Kirkdale, C.L.; Desborough, J.A.; Thornley, T. The UK pharmacy care plan service: Description, recruitment and initial views on a new community pharmacy intervention. PLoS ONE 2017, 12, e0174500. [Google Scholar] [CrossRef] [PubMed]
- Royal Decree-Law 9/2011, of August 19, on Measures to Improve the Quality and Cohesion of the National Health System, Contribution to Fiscal Consolidation, and Raising the Maximum Amount of State Guarantees for 2011. Available online: https://www.boe.es/buscar/pdf/2011/BOE-A-2011-14021-consolidado.pdf (accessed on 21 December 2023).
- Catalan Council of Pharmacists’ Associations and Catalan Department of Health. Guidance for Pharmacists on the Pharmacotherapeutic Follow-Up Use of Monitored Dosage Systems (MDS); Catalan Council of Pharmacists’ Associations and Catalan Department of Health: Barcelona, Spain, 2012; 64p. (In Catalan) [Google Scholar]
- Torres-Novellas, B.; Guayta-Escolies, R.; Rius, P.; Castellà, A.; Lecha, M.P.; Modamio, P.; Mariño, E.L. A study protocol for an experimental study for a pharmaceutical care programme to improve chronic complex disease management: PCAF programme. Trends Med. 2021, 21, 1–5. [Google Scholar]
- Care Quality Commission. Multi-Compartment Compliance Aids (MCAs) in Adult Social Care. Available online: https://www.cqc.org.uk/guidance-providers/adult-social-care/multi-compartment-compliance-aids-mcas-adult-social-care (accessed on 25 September 2023).
- Walters, S.; Chakravorty, M.; McLachlan, S.; Odone, J.; Stevenson, J.M.; Minshull, J.; Schiff, R. Medication compliance aids unpackaged: A national survey. Br. J. Clin. Pharmacol. 2022, 88, 4595–4606. [Google Scholar] [PubMed]
- World Health Organization (WHO). Anatomical Therapeutic Chemical (ATC) Classification. Available online: https://www.who.int/tools/atc-ddd-toolkit/atc-classification (accessed on 25 September 2023).
- Morisky, D.E.; Green, L.W.L.D. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care. 1986, 24, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Generalitat de Catalunya. IDESCAT. Statistics Institute of Catalonia. Population on January 1st. 2023. Available online: https://www.idescat.cat/indicadors/?id=aec&n=15223 (accessed on 25 September 2023). (In Catalan).
- Sell, R.; Schaefer, M. Prevalence and risk factors of drug-related problems identified in pharmacy-based medication reviews. Int. J. Clin. Pharm. 2020, 42, 588–597, Erratum in Int. J. Clin. Pharm. 2021, 43, 1735. [Google Scholar] [CrossRef] [PubMed]
- Shahrami, B.; Forough, A.S.; Najmeddin, F.; Hadidi, E.; Toomaj, S.; Javadi, M.R.; Gholami, K.; Sadeghi, K. Identification of drug-related problems followed by clinical pharmacist interventions in an outpatient pharmacotherapy clinic. J. Clin. Pharm. Ther. 2022, 47, 964–972. [Google Scholar] [CrossRef]
- Goedken, A.; Huang, S.; McDonough, R.; Deninger, M.; Doucette, W. Medication-Related Problems Identified through Continuous Medication Monitoring. Pharmacy 2018, 6, 86. [Google Scholar] [CrossRef]
- Wong, C.W. Medication-related problems in older people: How to optimise medication management. Hong Kong Med. J. 2020, 26, 510–519. [Google Scholar] [CrossRef]
- Hoel, R.W.; Giddings Connolly, R.M.; Takahashi, P.Y. Polypharmacy management in older patients. Mayo Clin. Proc. 2021, 96, 242–256. [Google Scholar] [CrossRef]
- Troncoso-Mariño, A.; Roso-Llorach, A.; López-Jiménez, T.; Villen, N.; Amado-Guirado, E.; Fernández-Bertolin, S.; Carrasco-Ribelles, L.A.; Borras, J.M.; Violán, C. Medication-related problems in older people with multimorbidity in Catalonia: A real-world data study with 5 years’ follow-up. J. Clin. Med. 2021, 10, 709. [Google Scholar] [CrossRef]
- Ylä-Rautio, H.; Siissalo, S.; Leikola, S. Drug-related problems and pharmacy interventions in non-prescription medication, with a focus on high-risk over-the-counter medications. Int. J. Clin. Pharm. 2020, 42, 786–795. [Google Scholar] [PubMed]
- Bhattacharya, D.; Aldus, C.F.; Barton, G.; Bond, C.M.; Boonyaprapa, S.; Charles, I.S.; Fleetcroft, R.; Holland, R.; Jerosch-Heroald, C.; Salter, C.; et al. The feasibility of determining the effectiveness and cost-effectiveness of medication organisation devices compared with usual care for older people in a community setting: Systematic review, stakeholder focus groups and feasibility randomised controlled trial. Health Technol. Assess. 2016, 20, 1–250. [Google Scholar]
- Stewart, D.; McDonald, C.; MacLeod, J.; MacLure, K.; Gray, G.; McIntosh, T. The behaviors and experiences of the community pharmacy team on the provision of multi-compartment compliance aids. Res. Social. Adm. Pharm. 2018, 14, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, R.; Scott, S.; Bhattacharya, D. Quantifying and characterising multi-compartment compliance aid provision. Res. Social. Adm. Pharm. 2020, 16, 560–567. [Google Scholar] [PubMed]
- Martin, Y.; Cabral, G.; Salazar Zaffaroni, M.F.; Armando, P. Design, implementation and evaluation of a service for Medication compliance aids (MCAs) in an institutional pharmacy in the city of Córdoba. Rev. Fac. Cien Med. Univ. Nac. Cordoba 2022, 79, 310–317. (In Spanish) [Google Scholar]
- Abdulsalim, S.; Unnikrishnan, M.K.; Manu, M.K.; Alrasheedy, A.A.; Godman, B.; Morisky, D.E. Structured pharmacist-led intervention programme to improve medication adherence in COPD patients: A randomized controlled study. Res. Social. Adm. Pharm. 2018, 14, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Kini, V.; Ho, P.M. Interventions to improve medication adherence: A review. JAMA 2018, 320, 2461–2473. [Google Scholar] [PubMed]
- Tolley, A.; Hassan, R.; Sanghera, R.; Grewal, K.; Kong, R.; Sodhi, B.; Basu, S. Interventions to promote medication adherence for chronic diseases in India: A systematic review. Front. Public Health 2023, 11, 1194919. [Google Scholar]
- Kari, H.; Kortejärvi, H.; Airaksinen, M.; Laaksonen, R. Patient involvement is essential in identifying drug-related problems. Br. J. Clin. Pharmacol. 2018, 84, 2048–2058. [Google Scholar]
- Seidling, H.M.; Send, A.F.J.; Bittmann, J.; Renner, K.; Dewald, B.; Lange, D.; Bruckner, T.; Haefeli, W.E. Medication review in German community pharmacies—Post-hoc analysis of documented drug-related problems and subsequent interventions in the ATHINA-project. Res. Soc. Adm. Pharm. 2017, 13, 1127–1134. [Google Scholar] [CrossRef]
- Gyllensten, H.; Fuller, J.M.; Östbring, M.J. Commentary: How person-centred is pharmaceutical care? Int. J. Clin. Pharm. 2022, 44, 270–275. [Google Scholar] [PubMed]
- Spiegel, B.; Shane, R.; Palmer, K.; Donna Luong, D. Cost-effectiveness of pharmacist postdischarge follow-up to prevent medication-related admissions. Am. J. Accountable Care 2018, 6, 1–8. [Google Scholar]
- Simon-Tuval, T.; Neumann, P.J.; Greenberg, D. Cost-effectiveness of adherence-enhancing interventions: A systematic review. Expert. Rev. Pharmacoecon. Outcomes Res. 2016, 16, 67–84. [Google Scholar] [PubMed]


{kind=link}
| MDS (n = 95) | No MDS (n = 51) | p-Value | |
|---|---|---|---|
| Age, mean (±SD) | 80 (7.4) | 77 (6.6) | 0.0075 * |
| Age (stratified), n (%) | |||
| 51–64 | 3 (3.20) | 3 (5.90) | 0.0205 * |
| 65–74 | 18 (18.90) | 13 (25.50) | |
| 75–84 | 40 (42.10) | 29 (56.90) | |
| ≥85 | 34 (35.80) | 6 (11.80) | |
| Men, n (%) | 44 (46.30) | 28 (54.90) | 0.4147 |
| No. of medications, mean (±SD) | 11.6 (4.1) | 10.7 (4.7) | 0.1067 |
| No. of medications (stratified), n (%) | |||
| <5 medications | 5 (5.30) | 6 (11.80) | 0.5196 |
| 5–10 medications | 46 (48.40) | 25 (49.00) | |
| 11–14 medications | 25 (26.30) | 11 (21.60) | |
| >14 medications | 19 (20.00) | 9 (17.60) | |
| Patients with hypertension, n (%) | 77 (81.10) | 47 (92.20) | 0.1222 |
| Patients with metabolic disorders (Lipoproteins and lipidaemia), n (%) | 58 (61.10) | 34 (66.70) | 0.6241 |
| Patients with diabetes mellitus, n (%) | 51 (53.70) | 27 (52.90) | 1 |
| Patients with osteoarthritis, n (%) | 42 (44.20) | 21 (41.20) | 0.859 |
| Patients with heart failure, n (%) | 29 (30.50) | 11 (21.60) | 0.3359 |
| Patients with extremity or joint pain, n (%) | 22 (23.20) | 8 (15.70) | 0.3951 |
| Patients with severe depressive disorders, n (%) | 24 (25.30) | 8 (15.70) | 0.2611 |
| Patients with COPD, n (%) | 14 (14.70) | 12 (23.50) | 0.2726 |
| Patients with osteoporosis, n (%) | 17 (17.90) | 5 (9.80) | 0.289 |
| Patients with anaemia, n (%) | 19 (20.00) | 6 (11.80) | 0.3035 |
| Patients with rheumatic pathology, n (%) | 15 (15.80) | 6 (11.80) | 0.6793 |
| Type of DRP | MDS | No MDS | Total |
|---|---|---|---|
| 1: Inappropriate drug administration, n (%) | 59 (10.9) | 23 (15.4) | 82 (11.90) |
| 2: Personal characteristics, n (%) | 26 (4.8) | 5 (3.4) | 31 (4.50) |
| 3: Inappropriate drug conservation, n (%) | 52 (9.6) | 0 (0.0) | 52 (7.55) |
| 4: Contraindication, n (%) | 6 (1.1) | 0 (0.0) | 6 (0.87) |
| 5: Inadequate dose, schedule and/or duration, n (%) | 50 (9.3) | 14 (9.4) | 64 (9.29) |
| 6: Duplications, n (%) | 8 (1.5) | 7 (4.7) | 15 (2.18) |
| 7: Dispensing errors, n (%) | 3 (0.6) | 0 (0.0) | 3 (0.44) |
| 8: Errors in prescription, n (%) | 4 (0.7) | 0 (0.0) | 4 (0.58) |
| 9: Non-adherence, n (%) | 182 (33.7) | 33 (22.1) | 215 (31.20) |
| 10: Drug interactions, n (%) | 57 (10.6) | 25 (16.8) | 82 (11.90) |
| 11: Unnecessary drug therapy, n (%) | 19 (3.5) | 5 (3.4) | 24 (3.48) |
| 12: Other health problems affecting medication, n (%) | 8 (1.5) | 7 (4.7) | 15 (2.18) |
| 13: Probability of adverse drug reactions, n (%) | 40 (7.4) | 16 (10.7) | 56 (8.13) |
| 14: Undertreated health problem, n (%) | 6 (1.1) | 6 (4.0) | 12 (1.74) |
| 15: Others, n (%) | 20 (3.7) | 8 (5.4) | 28 (4.06) |
| MDS (n = 95) | No MDS (n = 51) | |||||
|---|---|---|---|---|---|---|
| Baseline Visit | Last Visit | p | Baseline Visit | Last Visit | p-Value | |
| Morisky Green test—medication adherent patient, n (%) | 49 (51.6) | 69 (72.6) | 0.0008 * | 31 (60.8) | 39 (76.5) | 0.0990 |
| Possession index—% medication adherence, (<60%), n (%) | 13 (13.7) | 10 (10.5) | 0.1242 | 5 (9.8) | 6 (11.8) | 0.4131 |
| Possession index—% medication adherence, (60%, 70%), n (%) | 4 (4.2) | 7 (7.4) | 8 (15.7) | 2 (3.9) | ||
| Possession index—% medication adherence, (70%, 80%), n (%) | 6 (6.3) | 17 (17.9) | 6 (11.8) | 9 (17.6) | ||
| Possession index—% medication adherence, (≥80%), n (%) | 72 (75.8) | 61 (64.2) | 32 (62.7) | 34 (66.7) | ||
| Possession index—% medication adherence (continuous) **, mean (±SD) | 84.7 (20.4) | 83.1 (18.5) | 0.4052 | 82.4 (19.4) | 83.7 (19.7) | 0.6754 |
| Type of Intervention | MDS (n = 572) | No MDS (n = 156) |
|---|---|---|
| Facilitate PDI, n (%) | 261 (45.6) | 78 (50.0) |
| Offer health education, n (%) | 215 (37.6) | 45 (28.8) |
| Propose lifestyle changes, n (%) | 57 (10.0) | 8 (5.1) |
| Report in pharmacovigilance, n (%) | 1 (0.2) | 0 (0.0) |
| Refer to the primary care physician and communicate DRPs, n (%) | 38 (6.6) | 25 (16.0) |
| Non-Adherent (n = 66) | Adherent (n = 80) | p-Value | |
|---|---|---|---|
| No. of DRPs, mean (±SD) | 7.83 (17.47) | 2.15 (6.04) | 0.014 * |
| No. of interventions, mean (±SD) | 8.08 (18.12) | 2.44 (6.05) | 0.018 * |
| No. of DRPs that caused referral, mean (±SD) | 0.56 (1.15) | 0.33 (0.671) | 0.145 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-Novellas, B.; Rius, P.; Figueiredo-Escribá, C.; Mariño, E.L.; Modamio, P. Drug-Related Problems Detected in Complex Chronic Patients by Community Pharmacists of Catalonia: Perception of the Person-Centred Approach Necessity. Healthcare 2024, 12, 240. https://doi.org/10.3390/healthcare12020240
Torres-Novellas B, Rius P, Figueiredo-Escribá C, Mariño EL, Modamio P. Drug-Related Problems Detected in Complex Chronic Patients by Community Pharmacists of Catalonia: Perception of the Person-Centred Approach Necessity. Healthcare. 2024; 12(2):240. https://doi.org/10.3390/healthcare12020240
Chicago/Turabian StyleTorres-Novellas, Berta, Pilar Rius, Carlos Figueiredo-Escribá, Eduardo L. Mariño, and Pilar Modamio. 2024. "Drug-Related Problems Detected in Complex Chronic Patients by Community Pharmacists of Catalonia: Perception of the Person-Centred Approach Necessity" Healthcare 12, no. 2: 240. https://doi.org/10.3390/healthcare12020240
APA StyleTorres-Novellas, B., Rius, P., Figueiredo-Escribá, C., Mariño, E. L., & Modamio, P. (2024). Drug-Related Problems Detected in Complex Chronic Patients by Community Pharmacists of Catalonia: Perception of the Person-Centred Approach Necessity. Healthcare, 12(2), 240. https://doi.org/10.3390/healthcare12020240