
Comparative Analysis of the Impact of Training through Simulation Using the Crisis Resource Management Tool for Primary Care Professionals

 , , , , ,
, , , , ,  ,
, 
Abstract
1. Introduction
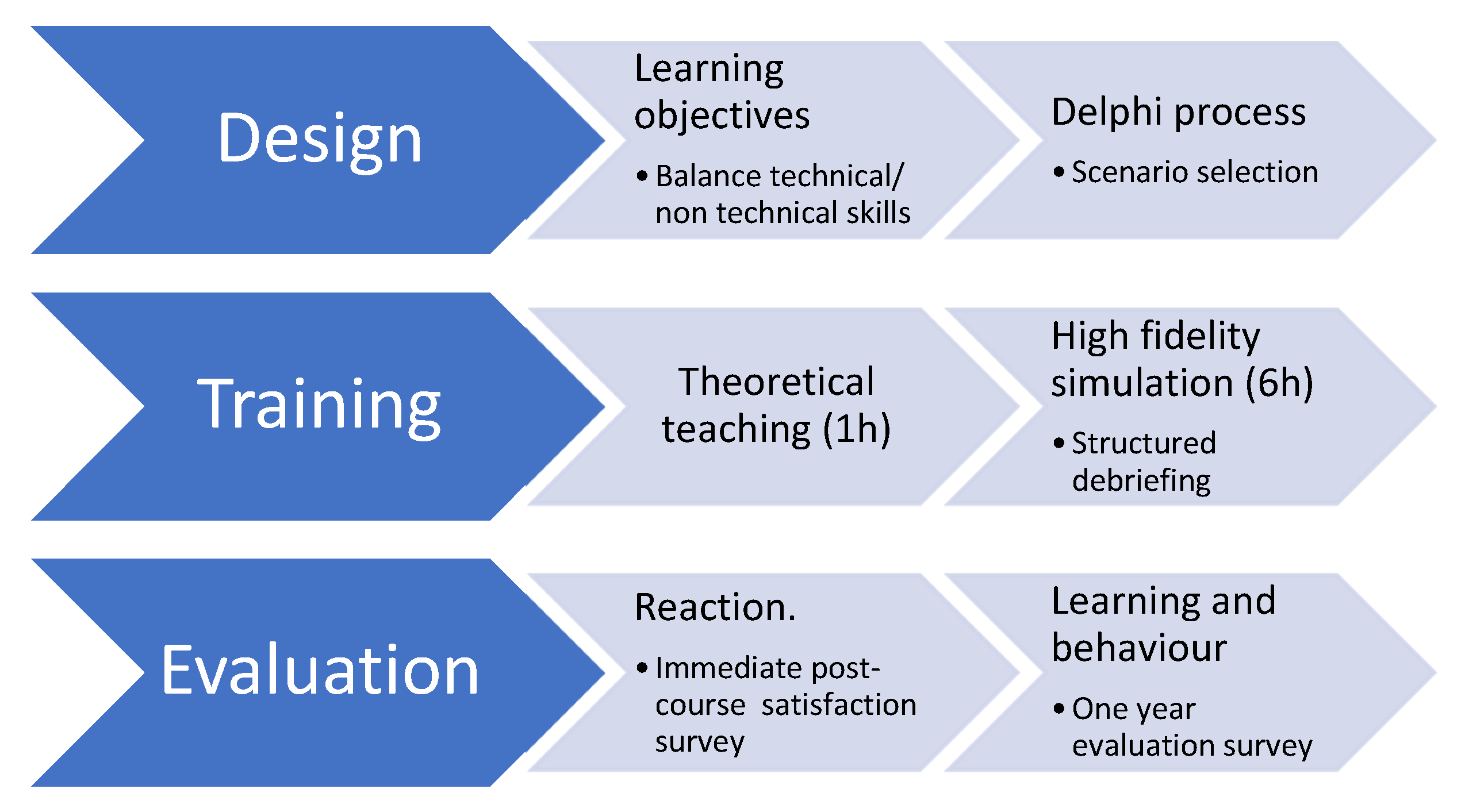
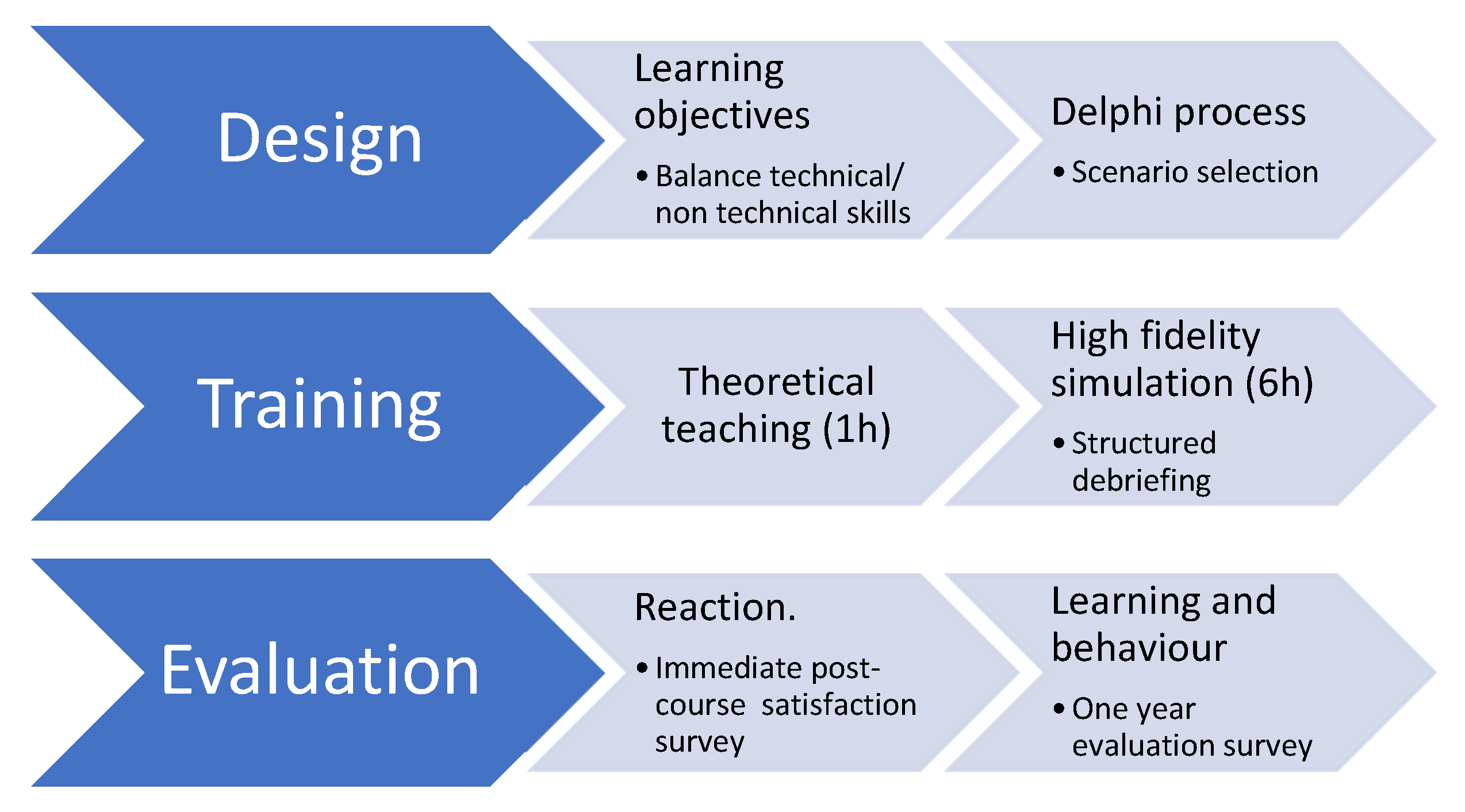
2. Materials and Methods
- Leadership—common mental model and distribution of workload;
- Effective communication—assertiveness training (difficult conversations);
- Help tools in patient transfer processes (handoff);
- Setting priorities dynamically;
- Periodic reassessment;
- Use of cognitive aids;
- Anticipation and planning—establishing a pause for reflection;
- Use of all available information and resources.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministerio de Sanidad y Consumo. Estudio APEAS. In Estudio Sobre La Seguridad De Los Pacientes En Atención Primaria De Salud; Ministerio de Sanidad y Consumo: Madrid, Spain, 2008. [Google Scholar]
- Buljac-Samardžić, M.; Doorn, C.M.D.-V.; Maynard, M.T. What Do We Really Know About Crew Resource Management in Healthcare? An Umbrella Review on Crew Resource Management and Its Effectiveness. J. Patient Saf. 2021, 17, e929–e958. [Google Scholar] [CrossRef]
- Phillips, J. Return on investment—Beyond the four levels. In Proceedings of the Academy of Human Resource Development Conference, St. Louis, MO, USA, 2–5 March 1995. [Google Scholar]
- Gaba, D.M.; Howard, S.K.; Fish, K.J.; Smith, B.E.; Sowb, Y.A. Simulation-Based Training in Anesthesia Crisis Resource Management (ACRM): A Decade of Experience. Simul. Gaming 2001, 32, 175–193. [Google Scholar] [CrossRef]
- Bracco, F.; De Tonetti, G.; Masini, M.; Passarelli, M.; Geretto, F.; Celleno, D. Crisis Resource Management in the Delivery Room: Development of Behavioral Markers for Team Performance in Emergency Simulation. Int. J. Environ. Res. Public Health 2018, 15, 439. [Google Scholar] [CrossRef]
- Bank, I.; Snell, L.; Bhanji, F. Pediatric Crisis Resource Management Training Improves Emergency Medicine Trainees’ Perceived Ability to Manage Emergencies and Ability to Identify Teamwork Errors. Pediatr. Emerg. Care 2014, 30, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Reznek, M.; Smith-Coggins, R.; Howard, S.; Kiran, K.; Harter, P.; Sowb, Y.; Gaba, D.; Krummel, T. Emergency Medicine Crisis Resource Management (EMCRM): Pilot Study of a Simulation-based Crisis Management Course for Emergency Medicine. Acad. Emerg. Med. 2003, 10, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Angulo, C.C.; María Quintillá Martínez, J.; Espinosa Ramírez, S. Los Orígenes: Crew Resource Management Emergency Crisis Resource Management SEMES (E-CRM SEMES) Clinical Simulations and Safety in Emergencies: Emergency Crisis Resource Management. Emergencias 2020, 32, 135–137. [Google Scholar]
- Gilic, F.; Schultz, K.; Sempowski, I.; Blagojevic, A. “Nightmares–Family Medicine” Course Is an Effective Acute Care Teaching Tool for Family Medicine Residents. Simul. Healthc. 2019, 14, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Beddows, J.; Abdalla, M.; Blanchard, D.; Hammond, E.; Hay, F.; Webb, M.; Protheroe, J. ‘I’m just ringing to get a repeat prescription for my contraceptive pill, doctor’: Developing authentic simulated telephone consultations for medical students. Educ. Prim. Care 2021, 32, 303–307. [Google Scholar] [CrossRef]
- Morreel, S.; Philips, H.; Colliers, A.; Verhoeven, V. Performance of a new guideline for telephone triage in out-of-hours services in Belgium: A pilot study using simulated patients. Health Serv. Manag. Res. 2020, 33, 166–171. [Google Scholar] [CrossRef]
- Pan, X.; Slater, M.; Beacco, A.; Navarro, X.; Rivas, A.I.B.; Swapp, D.; Hale, J.; Forbes, P.A.G.; Denvir, C.; Hamilton, A.F.d.C.; et al. The Responses of Medical General Practitioners to Unreasonable Patient Demand for Antibiotics—A Study of Medical Ethics Using Immersive Virtual Reality. PLoS ONE 2016, 11, e0146837. [Google Scholar] [CrossRef]
- Castelao, E.F.; Boos, M.; Ringer, C.; Eich, C.; Russo, S.G. Effect of CRM team leader training on team performance and leadership behavior in simulated cardiac arrest scenarios: A prospective, randomized, controlled study. BMC Med. Educ. 2015, 15, 116. [Google Scholar] [CrossRef]
- Johnson, G.G.; Beaumont, J.; Paton-Gay, J.D.; Widder, S.; Gillman, L.M. Multidisciplinary, multisite trauma team training during COVID-19: Lessons from the first virtual E-S.T.A.R.T.T. course. Can. J. Surg. 2021, 64, E609–E612. [Google Scholar] [CrossRef]
- Curran, C.; Lydon, S.; E Kelly, M.; Murphy, A.W.; O’connor, P. An analysis of general practitioners’ perspectives on patient safety incidents using critical incident technique interviews. Fam. Pract. 2019, 36, 736–742. [Google Scholar] [CrossRef] [PubMed]
- de Wet, C.; Bowie, P.; O’donnell, C. ‘The big buzz’: A qualitative study of how safe care is perceived, understood and improved in general practice. BMC Fam. Pract. 2018, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Harbitz, M.B.; Stensland, P.S.; Gaski, M. Rural general practice staff experiences of patient safety incidents and low quality of care in Norway: An interview study. Fam. Pract. 2022, 39, 130–136. [Google Scholar] [PubMed]
- Madden, C.; Lydon, S.; Murphy, A.W.; O’Connor, P. The patient’s “story”: An examination of patient-reported safety incidents in general practice. Fam. Pract. 2022, 39, 1095–1102. [Google Scholar] [CrossRef]
- Rodríguez-Cogollo, R.; Paredes-Alvarado, I.R.; Galicia-Flores, T.; Barrasa-Villar, J.I.; Castán-Ruiz, S. Cultura de seguridad del paciente en residentes de medicina familiar y comunitaria de Aragón. Rev. Calid. Asist. 2014, 29, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Rall, M.; Gaba, M. Human Performance and Patient Safety. In Miller’s Anesthesia, 6th ed.; Miller, R.D., Ed.; Elsevier: Philadelphia, PA, USA, 2005. [Google Scholar]
- Rall, M.; van Gessel, E.; Staender, S. Education, teaching & training in patient safety. Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 251–262. [Google Scholar]
- Reason, J. Understanding adverse events: Human factors. Heart 1995, 4, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Gaba, D.M. Crisis resource management and teamwork training in anaesthesia. Br. J. Anaesth. 2010, 105, 3–6. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Simon, R.; Rivard, P.; Dufresne, R.L.; Raemer, D.B. Debriefing with Good Judgment: Combining Rigor-ous Feedback with Genuine Inquiry. Anesthesiol. Clin. 2007, 25, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Kolb, D.A. Experiential Learning: Experience as the Source of Learning and Development; Prentice Hall: Englewood Cliffs, NJ, USA, 1984. [Google Scholar]
- Kirkpatrick, D.L. The Four Levels of Evaluation. In Evaluating Corporate Training: Models and Issues; Springer: Dordrecht, The Netherlands, 1998; pp. 95–112. [Google Scholar]
- Bartolomé, A.; Gómez-Arnau, J.I.; del Valle, S.G.; González-Arévalo, A.; Santa-Úrsula, J.A.; Hidalgo, I. Seguridad del paciente y sistemas de comunicación de incidentes. Rev. Calid. Asist. 2005, 20, 228–234. [Google Scholar] [CrossRef]
- Spencer, R.; Campbell, S.M. Tools for primary care patient safety: A narrative review. BMC Fam. Pract. 2014, 15, 166. [Google Scholar] [CrossRef] [PubMed]
- Portela Romero, M.; Bugarín González, R.; Rodríguez Calvo, M.S. La cultura de seguridad del paciente en los médicos internos residentes de Medicina Familiar y Comunitaria de Galicia. Atención Primaria 2017, 49, 343–350. [Google Scholar] [CrossRef]
- Campbell, S.M.; Bell, B.G.; Marsden, K.; Spencer, R.B.B.; Kadam, U.; Perryman, K.; Rodgers, S.; Litchfield, I.; Reeves, D.; Chuter, A.B.; et al. A Patient Safety Toolkit for Family Practices. J. Patient Saf. 2018, 16, e182–e186. [Google Scholar] [CrossRef]
- Bray, L.; Krogh, T.B.; Østergaard, D. Simulation-based training for continuing professional development within a primary care context: A systematic review. Educ. Prim. Care 2023, 34, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, D.; Dieckmann, P.; Lippert, A. Simulation and CRM. Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Crofts, J.; Ellis, D.; Draycott, T.; Winter, C.; Hunt, L.; Akande, V. Change in knowledge of midwives and obstetricians following obstetric emergency training: A randomised controlled trial of local hospital, simulation centre and teamwork training. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Blum, R.H.; Raemer, D.B.; Carroll, J.S.; Sunder, N.; Felstein, D.M.; Cooper, J.B. Crisis resource management training for an anaesthesia faculty: A new approach to continuing education. Med. Educ. 2004, 38, 45–55. [Google Scholar] [CrossRef]
- Gardner, R.; Walzer, T.B.; Simon, R.; Raemer, D.B. Obstetric Simulation as a Risk Control Strategy: Course design and evaluation. Simul. Healthc. 2008, 3, 119–127. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Garg, R.; Atiq, H.; Baig, N.; Bernardino, M.; Bigham, B.; Dickson, S.; Geduld, H.; Al-Hilali, Z.; Karki, S.; et al. Cardiopulmonary resuscitation in low-resource settings: A statement by the International Liaison Committee on Resuscitation, supported by the AFEM, EUSEM, IFEM, and IFRC. Lancet Glob. Health 2023, 11, e1444–e1453. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Workshop-Related Variables | Total (n = 283) | ME (n = 138) | RE (n = 145) | Delta | p |
|---|---|---|---|---|---|
| Organization | 87.63 | 89.86 | 85.52 | 4.34 | 0.27 |
| Facilities used | 78.45 | 77.54 | 79.31 | −1.77 | 0.7 |
| Available resources | 81.27 | 81.16 | 81.38 | −0.22 | 0.9 |
| Comfort of the classroom | 57.95 | 55.80 | 60.00 | −4.20 | 0.5 |
| Duration of each scenario | 68.90 | 68.12 | 69.66 | −1.54 | 0.8 |
| Number of students in each scenario | 77.39 | 78.99 | 75.86 | 3.12 | 0.5 |
| Content level | 82.33 | 83.33 | 81.38 | 1.95 | 0.3 |
| Post-stage debriefing | 86.22 | 84.78 | 87.59 | −2.80 | 0.5 |
| Usefulness of the content learned | 84.10 | 83.33 | 84.83 | −1.49 | 0.1 |
| General impression of the scenarios | 83.39 | 81.88 | 84.83 | −2.94 | 0.5 |
| Survey Responses (One Year after Courses, 2018) (n = 156) | |||||
|---|---|---|---|---|---|
| Strongly Agree (5) | 4 | 3 | 2 | Strongly Disagree (1) | |
| 94 (60.3%) | 61 (39.1%) | 0 | 0 | 1 (0.6%) |
| 96 (61.5%) | 56 (35.9%) | 3 (1.9%) | 0 | 1 (0.6%) |
| 89 (57.05%) | 65 (41.7%) | 1 (0.6%) | 0 | 1 (0.6%) |
| 120 (76.9%) | 33 (21.1%) | 1 (0.6%) | 1 (0.6%) | 1 (0.64%) |
| 43 (27.6%) | 77 (49.4%) | 24 (15.4%) | 11 | 1 (0.6%) |
| yes | no | ||||
| 144 (92.3%) | 12 (7.7%) | |||
| 136 (87.2%) | 20 (12.8%) | |||
| Total | ME | RE | p | |
|---|---|---|---|---|
| 99.4 | 98.7 | 100 | 0.32 |
| 97.7 | 98.7 | 96.2 | 0.31 |
| 98.7 | 98.7 | 98.7 | 1 |
| 98.1 | 98.7 | 97.4 | 0.56 |
| 76.9 | 74.4 | 79.5 | 0.45 |
| 92.3 | 91 | 93.6 | 0.55 |
| 87.2 | 80.8 | 93.6 | 0.02 |
| Total | UM | UR | p | |
|---|---|---|---|---|
| 62 (39.7%) | 38 (48.7%) | 24 (30.8) | 0.02 |
| 60 (38.5%) | 34 (43.6%) | 26 (38.5%) | 0.2 |
| 67 (42.9%) | 39 (50%) | 28 (35.9%) | 0.07 |
| 36 (23.1%) | 18 (23.1%) | 18 (23.1%) | 1 |
| 113 (72.4%) | 52 (66.7%) | 61 (78.2%) | 0.1 |
| 12 (7.7%) | 7 (9%) | 5 (6.4%) | 0.5 |
| 20 (12.8%) | 15 (19.2%) | 5 (6.4%) | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardino-Santos, M.; Arnal-Velasco, D.; Reboto-Cortés, P.; Garmendia-Fernandez, C.; Renilla-Sánchez, E.; Navalón-Liceras, R.J.; Botillo-Pérez, E.; Ortega, M.A.; Gómez-Arnau Díaz-Cañabate, J.I.; De León-Luis, J.A. Comparative Analysis of the Impact of Training through Simulation Using the Crisis Resource Management Tool for Primary Care Professionals. Healthcare 2024, 12, 230. https://doi.org/10.3390/healthcare12020230
Bernardino-Santos M, Arnal-Velasco D, Reboto-Cortés P, Garmendia-Fernandez C, Renilla-Sánchez E, Navalón-Liceras RJ, Botillo-Pérez E, Ortega MA, Gómez-Arnau Díaz-Cañabate JI, De León-Luis JA. Comparative Analysis of the Impact of Training through Simulation Using the Crisis Resource Management Tool for Primary Care Professionals. Healthcare. 2024; 12(2):230. https://doi.org/10.3390/healthcare12020230
Chicago/Turabian StyleBernardino-Santos, Marta, Daniel Arnal-Velasco, Pilar Reboto-Cortés, Cristina Garmendia-Fernandez, Esther Renilla-Sánchez, Ricardo Jose Navalón-Liceras, Elena Botillo-Pérez, Miguel A. Ortega, Juan Ignacio Gómez-Arnau Díaz-Cañabate, and Juan A. De León-Luis. 2024. "Comparative Analysis of the Impact of Training through Simulation Using the Crisis Resource Management Tool for Primary Care Professionals" Healthcare 12, no. 2: 230. https://doi.org/10.3390/healthcare12020230
APA StyleBernardino-Santos, M., Arnal-Velasco, D., Reboto-Cortés, P., Garmendia-Fernandez, C., Renilla-Sánchez, E., Navalón-Liceras, R. J., Botillo-Pérez, E., Ortega, M. A., Gómez-Arnau Díaz-Cañabate, J. I., & De León-Luis, J. A. (2024). Comparative Analysis of the Impact of Training through Simulation Using the Crisis Resource Management Tool for Primary Care Professionals. Healthcare, 12(2), 230. https://doi.org/10.3390/healthcare12020230