
Opioid Treatment in Primary Care: Knowledge and Practical Use of Opioid Therapy



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
- Criteria for deciding which painkillers to use;
- Knowledge related to morphine substitutes and their proper doses;
- Knowledge related to the management of specific patients;
- Opioids with the highest prescription rate.
2.2. Data Assembly (Study Period and How It Was Performed) and Collection
2.3. Statistical Approach
3. Results
3.1. General Characteristics of Participants
3.2. The Choice of Pain Medication and Opioid Prescription
3.3. Primary Care Physician Knowledge on the Topic of Opioid Usage
3.4. Comparison of the Right Clinical Decision with the Percentage of Doctors Declaring Opioid Use
4. Discussion
4.1. Main Findings
4.2. What This Study Provides
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Zimmermann, A.; Mędrzycka-Dąbrowska, W.; Zagłoba, M. Patient’s right to pain treatment. Palliat. Med. Pract. 2018, 12, 11–19. [Google Scholar]
- O’Brien, T.; Christrup, L.; Drewes, A.; Fallon, M.; Kress, H.; McQuay, H.; Mikus, G.; Morlion, B.; Perez-Cajaraville, J.; Pogatzki-Zahn, E.; et al. European Pain Federation position paper on appropriate opioid use in chronic pain management. Eur. J. Pain 2017, 21, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Pieters, J.; Dolmans, D.H.J.M.; Verstegen, D.M.L.; Warmenhoven, F.C.; Courtens, A.M.; van den Beuken-van Everdingen, M.H.J. Palliative care education in the undergraduate medical curricula: Students’ views on the importance of, their confidence in, and knowledge of palliative care. BMC Palliat. Care 2019, 18, 72. [Google Scholar] [CrossRef]
- The European Pain Federation (EFIC) 2013. APPEAL (Advancing Provision of Pain Education and Learning) Study. Available online: http://hepmp.med.bg.ac.rs/wp-content/uploads/2018/01/Pain_APPEAL-Study_Backgrounder-dok.pdf (accessed on 27 July 2023).
- Hooten, W.M.; Dvorkin, J.; Warner, N.S.; Pearson, A.C.; Murad, M.H.; Warner, D.O. Characteristics of physicians who prescribe opioids for chronic pain: A meta-narrative systematic review. J. Pain Res. 2019, 12, 2261–2289. [Google Scholar] [CrossRef] [PubMed]
- Alford, D.P. Opioid Prescribing for Chronic Pain—Achieving the Right Balance through Education. N. Engl. J. Med. 2016, 374, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Polacek, C.; Christopher, R.; Mann, M.; Udall, M.; Craig, T.; Deminski, M.; Sathe, N.A. Healthcare professionals’ perceptions of challenges to chronic pain management. Am. J. Manag. Care 2020, 26, e135–e139. [Google Scholar] [CrossRef]
- Polish Society of Family Medicine. Online Calculator to Convert Opioid Doses. Available online: https://kalkulatoropioidow.pl/ (accessed on 25 July 2023).
- Häuser, W.; Morlion, B.; Vowles, K.E.; Bannister, K.; Buchser, E.; Casale, R.; Chenot, J.; Chumbley, G.; Drewes, A.M.; Dom, G.; et al. European* clinical practice recommendations on opioids for chronic noncancer pain—Part 1: Role of opioids in the management of chronic noncancer pain. Eur. J. Pain 2021, 25, 949–968. [Google Scholar] [CrossRef]
- Yang, J.; A Bauer, B.; Wahner-Roedler, D.L.; Chon, T.Y.; Xiao, L. The Modified WHO Analgesic Ladder: Is It Appropriate for Chronic Non-Cancer Pain? J. Pain Res. 2020, 13, 411–417. [Google Scholar] [CrossRef]
- EAPC Atlas of Palliative Care in Europe 2019. Available online: https://mariabouri.eu/sitecake-content/1d2d3ae4-7d60-11e9-9993-000000000000-1.pdf (accessed on 25 July 2023).
- Caraceni, A.; Hanks, G.; Kaasa, S.; Bennett, M.I.; Brunelli, C.; Cherny, N.; Dale, O.; De Conno, F.; Fallon, M.; Hanna, M.; et al. Use of opioid analgesics in the treatment of cancer pain: Evidence-based recommendations from the EAPC. Lancet Oncol. 2012, 13, e58–e68. [Google Scholar] [CrossRef]
- Ciałkowska-Rysz, A.; Dzierżanowski, T. Podstawowe zasady farmakoterapii bólu u chorych na nowotwory i inne przewlekłe, postępujące, zagrażające życiu choroby [Basic principles of pharmacotherapy of pain in patients with cancer and other chronic, progressive, life-threatening diseases]. Med. Paliatywna/Palliat. Med. 2014, 6, 1–6. [Google Scholar]
- Wordliczek, J.; Kotlińska-Lemieszek, A.; Leppert, W.; Woroń, J.; Dobrogowski, J.; Krajnik, M.; Przeklasa-Muszyńska, A.; Jassem, J.; Drobnik, J. Pharmacotherapy of pain in cancer patients—Recommendations of the Polish Association for the Study of Pain, Polish Society of Palliative Medicine, Polish Society of Oncology, Polish Society of Family Medicine, Polish Society of Anaesthesiology and Intensive Therapy and Association of Polish Surgeons. Ann. Surg. 2018, 90, 51–80. [Google Scholar] [CrossRef]
- Mills, S.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Punwasi, R.; de Kleijn, L.; Rijkels-Otters, J.B.M.; Veen, M.; Chiarotto, A.; Koes, B. General practitioners’ attitudes towards opioids for non-cancer pain: A qualitative systematic review. BMJ Open 2022, 12, e054945. [Google Scholar] [CrossRef]
- Green, C.R.; Wheeler, J.R.; Marchant, B.; LaPorte, F.; Guerrero, E. Analysis of the physician variable in pain management. Pain Med. 2001, 2, 317–327. [Google Scholar] [CrossRef]
- Desveaux, L.; Saragosa, M.; Kithulegoda, N.; Ivers, N.M. Understanding the behavioural determinants of opioid prescribing among family physicians: A qualitative study. BMC Fam. Pract. 2019, 20, 59. [Google Scholar] [CrossRef]
- Tyson, D.M.; Chavez, M.N.; Lake, P.; Gutierrez, A.; Sherry, P.; Rigg, K.K.; Marshall, V.K.; Henderson, H.; di Ciccone, B.L.; Rajasekhara, S.; et al. Perceptions of prescription opioid medication within the context of cancer survivorship and the opioid epidemic. J. Cancer Surviv. 2021, 15, 585–596. [Google Scholar] [CrossRef]
- Paul, A.K.; Smith, C.M.; Rahmatullah, M.; Nissapatorn, V.; Wilairatana, P.; Spetea, M.; Gueven, N.; Dietis, N. Opioid Analgesia and Opioid-Induced Adverse Effects: A Review. Pharmaceuticals 2021, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.-C.; Pallotti, P.; Dickinson, R.; Harley, C. ‘If you can’t see a dilemma in this situation you should probably regard it as a warning’: A metasynthesis and theoretical modelling of general practitioners’ opioid prescription experiences in primary care. Br. J. Pain 2019, 13, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Makhlouf, S.M.; Pini, S.; Ahmed, S.; Bennett, M.I. Managing Pain in People with Cancer—A Systematic Review of the Attitudes and Knowledge of Professionals, Patients, Caregivers and Public. J. Cancer Educ. 2020, 35, 214–240. [Google Scholar] [CrossRef] [PubMed]
- Dzierżanowski, T.; Ciałkowska-Rysz, A. Accessibility of opioid analgesics and barriers to optimal chronic pain treatment in Poland in 2000–2015. Support. Care Cancer 2017, 25, 775–781. [Google Scholar] [CrossRef]
- Krebs, E.E.; Bergman, A.A.; Coffing, J.M.; Campbell, S.R.; Frankel, R.M.; Matthias, M.S. Barriers to guideline-concordant opioid management in primary care—A qualitative study. J. Pain 2014, 15, 1148–1155. [Google Scholar] [CrossRef]
- Grata-Borkowska, U.; Drobnik, J.; Bujnowska-Fedak, M.M.; Pokorna-Kałwak, D.; Odonicz-Czarnecki, G. Leczenie bólu w praktyce lekarza rodzinnego—Doniesienie wstępne [Pain management in family physician practice—Preliminary report]. Forum Med. Rodz. 2015, 9, 456–459. [Google Scholar]
- Hannes, K.; Leys, M.; Vermeire, E.; Aertgeerts, B.; Buntinx, F.; Depoorter, A.-M. Implementing evidence-based medicine in general practice: A focus group based study. BMC Fam. Pract. 2005, 6, 37. [Google Scholar] [CrossRef]
- Dzierżanowski, T.; Kozłowski, M. Opioid prescribing attitudes of palliative care physicians versus other specialists: A questionnaire-based survey. Postgrad. Med. J. 2022, 98, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N.; Sheehan, B.K.A.; Scanlan, N.E.; Matthews, M.; Ross, E.L. Beliefs and attitudes about opioid prescribing and chronic pain management: Survey of primary care providers. J. Opioid Manag. 2014, 10, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Richards, G.C.; Mahtani, K.R.; Muthee, T.B.; DeVito, N.J.; Koshiaris, C.; Aronson, J.K.; Goldacre, B.; Heneghan, C.J. Factors associated with the prescribing of high-dose opioids in primary care: A systematic review and meta-analysis. BMC Med. 2020, 18, 68. [Google Scholar] [CrossRef]
- Klepstad, P.; Kaasa, S.; Borchgrevink, P.C. Starting Step III opioids for moderate to severe pain in cancer patients: Dose titration: A systematic review. Palliat. Med. 2011, 25, 424–430. [Google Scholar] [CrossRef]
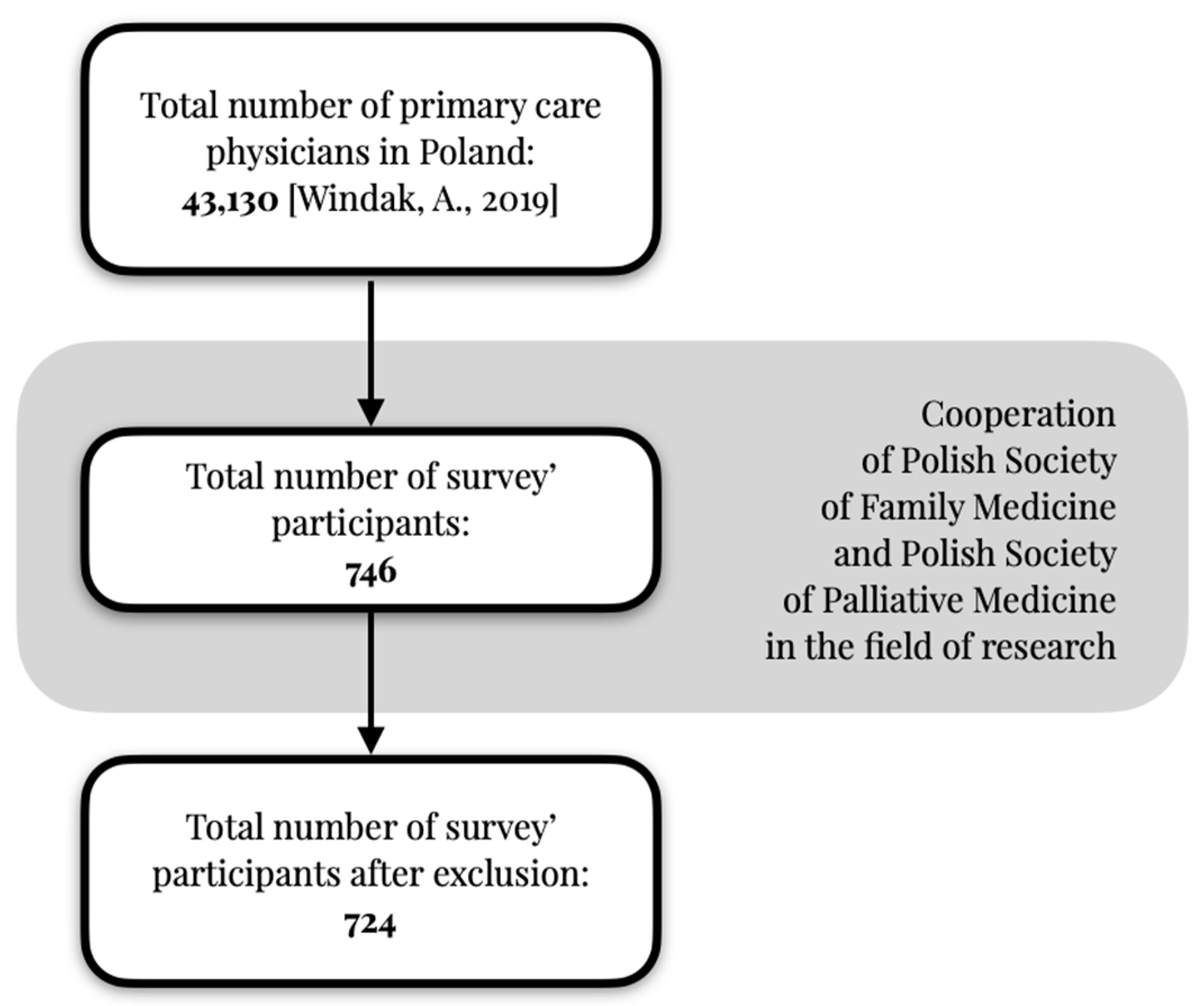
- Windak, A. Primary Health Care in Poland—Diagnosis and Draft Changes; Report, Instytut Medycyny Wsi im; Witold Chodźka in Lublin: Lublin, Poland, 2019. [Google Scholar]
- Eysenbach, G. Improving the quality of web surveys: The checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.N.D.; Payne, V.L.; Meeks, D.W.; Rao, R.; Singh, H. Physicians’ Diagnostic Accuracy, Confidence, and Resource Requests: A Vignette Study. JAMA Intern. Med. 2013, 173, 1952–1958. [Google Scholar] [CrossRef]
- Kuhn, J.; van den Berg, P.; Mamede, S.; Zwaan, L.; Bindels, P.; van Gog, T. Improving medical residents’ self-assessment of their diagnostic accuracy: Does feedback help? Adv. Health Sci. Educ. 2022, 27, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Glowacki, D. Effective pain management and improvements in patients’ outcomes and satisfaction. Crit. Care Nurse 2015, 35, 33–41. [Google Scholar] [CrossRef]
- Carey, M.L.; Zucca, A.C.; Freund, M.A.; Bryant, J.; Herrmann, A.; Roberts, B.J. Systematic review of barriers and enablers to the delivery of palliative care by primary care practitioners. Palliat. Med. 2019, 33, 1131–1145. [Google Scholar] [CrossRef]
- Green, E.; Knight, S.; Gott, M.; Barclay, S.; White, P. Patients’ and carers’ perspectives of palliative care in general practice: A systematic review with narrative synthesis. Palliat. Med. 2018, 32, 838–850. [Google Scholar] [CrossRef]
- Thelen, M.; Brearley, S.G.; Walshe, C. A grounded theory of interdependence between specialist and generalist palliative care teams across healthcare settings. Palliat. Med. 2023, 37, 1474–1483. [Google Scholar] [CrossRef]
- Fan, W.; Yan, Z. Factors affecting response rates of the web survey: A systematic review. Comput. Hum. Behav. 2010, 26, 132–139. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participant Characteristics | N (%) |
|---|---|
| Professional length of service as a primary care physician (n = 744) | |
| Less than 1 year | 92 (12.4) |
| From 1 year to 5 years | 244 (32.8) |
| From 6 years to 15 years | 182 (24.5) |
| More than 16 years | 206 (27.7) |
| I do not work now in primary health care/not a doctor | 20 (2.7) |
| Primary health care is the main place of work (n = 724) | |
| Yes | 634 (87.6) |
| YES, and I simultaneously work in palliative care | 24 (3.3) |
| No | 54 (7.5) |
| NO, and I simultaneously work in palliative care | 12 (1.7) |
| Average number of hours spent in primary care per week (n = 724) | |
| Less than 10 h per week | 32 (4.4) |
| 10–20 h per week | 42 (5.8) |
| 20–40 h per week | 464 (64.1) |
| More than 40 h per week | 186 (25.7) |
| Respondents’ medical specialties (n = 724) | |
| Family medicine specialist | 334 (46.1) |
| Undergoing specialization in family medicine | 226 (31.2) |
| Internal medicine specialist | 124 (17.1) |
| Palliative medicine specialist | 12 (1.7) |
| Pediatric specialist | 20 (2.8) |
| Other | 18 (2.5) |
| None | 88 (12.2) |
| Question | Answers | Total Group, N (%) | Only Family Medicine Specialists, N (%) | Only Participants with Work Experience of 1 Year or Longer, N (%) |
|---|---|---|---|---|
| 724 (100) | 334 (100) | 636 (100) | ||
| Criterion for determining the choice of pain medication, according to respondents. | Pain intensity measured by pain rating scale | 387 (53.5) | 172 (51.5) | 332 (52.2) |
| Nature of pain | 201 (27.8) | 96 (28.7) | 174 (27.4) | |
| Dynamics of pain evolution; speed of escalation | 88 (12.2) | 40 (12.0) | 78 (12.3) | |
| Own experience with a particular drug | 44 (6.1) | 18 (5.4) | 44 (6.9) | |
| Location of pain | 4 (0.1) | 2 (0.6) | 3 (0.5) | |
| Do you write prescriptions for opioid drugs? | I initiate pain management with weak or strong opioids as needed | 388 (53.6) | 182 (54.4) | 354 (55.6) |
| I use tramadol and buprenorphine preparations (in patches) | 234 (32.3) | 112 (33.5) | 200 (31.4) | |
| I write opioid drugs, but only as a continuation of therapy | 92 (12.7) | 26 (7.8) | 64 (10.6) | |
| I use only tramadol | 29 (4.0) | 12 (3.6) | 16 (2.5) |
| Question | Answers | Total Group, N (%) | Only Family Medicine Specialists, N (%) | Only Participants with Work Experience of 1 Year or Longer, N (%) |
|---|---|---|---|---|
| 724 (100) | 334 (100) | 636 (100) | ||
| What dose of morphine is equivalent to 400 mg of tramadol (approximate, in accordance with Polish guidelines)? | I don’t know | 307 (42.4) | 136 (40.7) | 258 (40.6) |
| 40 mg | 152 (21.0) | 66 (19.8) | 128 (20.1) | |
| 80 mg | 133 (18.4) | 70 (21.0) | 114 (18.0) | |
| 20 mg | 100 (13.9) | 38 (11.4) | 88 (13.9) | |
| 60 mg | 51 (7.0) | 22 (6.6) | 45 (7.1) | |
| What dose of oral morphine is equivalent to 35 mg of buprenorphine (tts, approximate, in accordance with Polish guidelines)? | I don’t know | 350 (48.3) | 142 (42.6) | 280 (44.0) |
| 80 mg | 135 (18.6) | 72 (21.6) | 124 (19.5) | |
| 20 mg | 133 (18.4) | 64 (19.2) | 118 (18.6) | |
| 40 mg | 68 (9.4) | 26 (7.8) | 62 (9.8) | |
| 60 mg | 57 (7.9) | 28 (8.4) | 50 (7.9) | |
| The patient takes 400 mg (tramadol retard per day in two divided doses. In addition, he takes paracetamol 500 mg every 8 h. Current pain severity is 6/10 on the NRS scale. What treatment will you suggest (in accordance with Polish guidelines)? | Initiate treatment with buprenorphine patch, starting with a dose of 35 μg/h (tts) and gradually increase the dose every 6 days or so as needed until control is achieved | 254 (35.1) | 128 (38.3) | 228 (35.9) |
| Initiate treatment with short-acting oral morphine at a dose of ½ tablet of 20 mg every 4 h + emergency analgesic dose and titrate until control is achieved | 196 (27.1) | 94 (28.1) | 180 (28.3) | |
| A coanalgesic, such as pregabalin, should be included first | 164 (22.7) | 58 (17.4) | 124 (19.5) | |
| Replace paracetamol with ketoprofen and give it twice daily at a dose of 100 mg | 39 (5.4) | 22 (6.6) | 36 (5.6) | |
| Increase the total dose of tramadol by 1/2 to a total of 600 mg in two divided doses | 29 (4.0) | 8 (2.4) | 22 (3.5) | |
| None (no treatment) | 62 (8.6) | 22 (6.6) | 44 (6.9) | |
| The patient, 57 years old, was treated about 3 months ago for hemiplegia of the facial area on the left side. Since then she is constantly accompanied by pain in this area 4/10 on the NRS scale treated with oral tramadol 2 × 100 mg, hypersensitivity and burning sensation. What treatment would you suggest (in accordance with Polish guidelines)? | You will join the treatment with pregabalin starting with a dose of 75 mg twice a day | 542 (74.7) | 232 (69.5) | 456 (71.2) |
| You will join the treatment with gabapentin trying to reach a dose of 3 × 300 mg | 160 (22.1) | 80 (24.0) | 146 (23.0) | |
| You will include a drug from step 3 of the analgesic ladder in the face of tramadol’s ineffectiveness | 21 (2.9) | 8 (2.4) | 8 (1.3) | |
| You will repeat treatment with acyclovir at a dose of 4 × 400 mg | 4 (0.6) | 8 (2.4) | 14 (2.2) | |
| None (no treatment) | 17 (2.3) | 4 (1.2) | 10 (1.6) | |
| Question | Answers | Total Group, N (%) | Only Family Medicine Specialists, N (%) | Only Participants with Work Experience of 1 Year or Longer, N (%) |
|---|---|---|---|---|
| 724 (100) | 334 (100) | 636 (100) | ||
| Most commonly used opioids in daily medical practice | Tramadol (oral) | 490 (67.7) | 192 (57.5) | 404 (63.6) |
| Buprenorphine in a patch | 170 (23.4) | 94 (28.1) | 160 (25.2) | |
| Oxycodone (oral) | 34 (4.7) | 26 (7.8) | 32 (5.0) | |
| Short-acting oral morphine | 27 (3.7) | 14 (4.2) | 20 (3.1) | |
| I do not use opioids in my medical practice | 24 (3.3) | 4 (1.2) | 12 (1.9) | |
| The stage of treatment at which coanalgetic drugs are introduced | At the time of diagnosis, that the pain is neuropathic in nature | 518 (71.5) | 226 (67.7) | 448 (70.4) |
| When drugs from step 3 of the analgesic ladder are ineffective | 129 (17.8) | 60 (18.0) | 108 (17.0) | |
| At the first signals from the patient regarding pain | 45 (6.2) | 24 (7.2) | 38 (7.1) | |
| Other | 14 (1.9) | 4 (1.2) | 8 (1.6) | |
| I never include coanalgesics in my practice | 37 (5.1) | 16 (4.8) | 24 (3.8) | |
| The most difficult part of pain management in daily PCP practice | Morphine titration in a primary health care/home treatment | 322 (43.4) | 138 (41.3) | 276 (43.4) |
| Replacing one painkiller with another (rotation) | 150 (20.7) | 76 (22.8) | 128 (21.1) | |
| Controlling breakthrough pain | 98 (13.5) | 46 (13.8) | 86 (13.5) | |
| Adding coanalgesics to pain management | 86 (11.9) | 38 (11.4) | 72 (11.3) | |
| Selecting non-steroidal anti-inflammatory drugs according to the type of pain | 51 (7.0) | 16 (48.0) | 38 (6.0) | |
| Other | 4 (0.6) | 2 (0.6) | 4 (0.6) | |
| None | 33 (4.6) | 16 (4.8) | 30 (4.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biesiada, A.M.; Ciałkowska-Rysz, A.; Mastalerz-Migas, A. Opioid Treatment in Primary Care: Knowledge and Practical Use of Opioid Therapy. Healthcare 2024, 12, 217. https://doi.org/10.3390/healthcare12020217
Biesiada AM, Ciałkowska-Rysz A, Mastalerz-Migas A. Opioid Treatment in Primary Care: Knowledge and Practical Use of Opioid Therapy. Healthcare. 2024; 12(2):217. https://doi.org/10.3390/healthcare12020217
Chicago/Turabian StyleBiesiada, Aleksander Michał, Aleksandra Ciałkowska-Rysz, and Agnieszka Mastalerz-Migas. 2024. "Opioid Treatment in Primary Care: Knowledge and Practical Use of Opioid Therapy" Healthcare 12, no. 2: 217. https://doi.org/10.3390/healthcare12020217
APA StyleBiesiada, A. M., Ciałkowska-Rysz, A., & Mastalerz-Migas, A. (2024). Opioid Treatment in Primary Care: Knowledge and Practical Use of Opioid Therapy. Healthcare, 12(2), 217. https://doi.org/10.3390/healthcare12020217