
Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials

Abstract
1. Introduction
2. Material and Methods
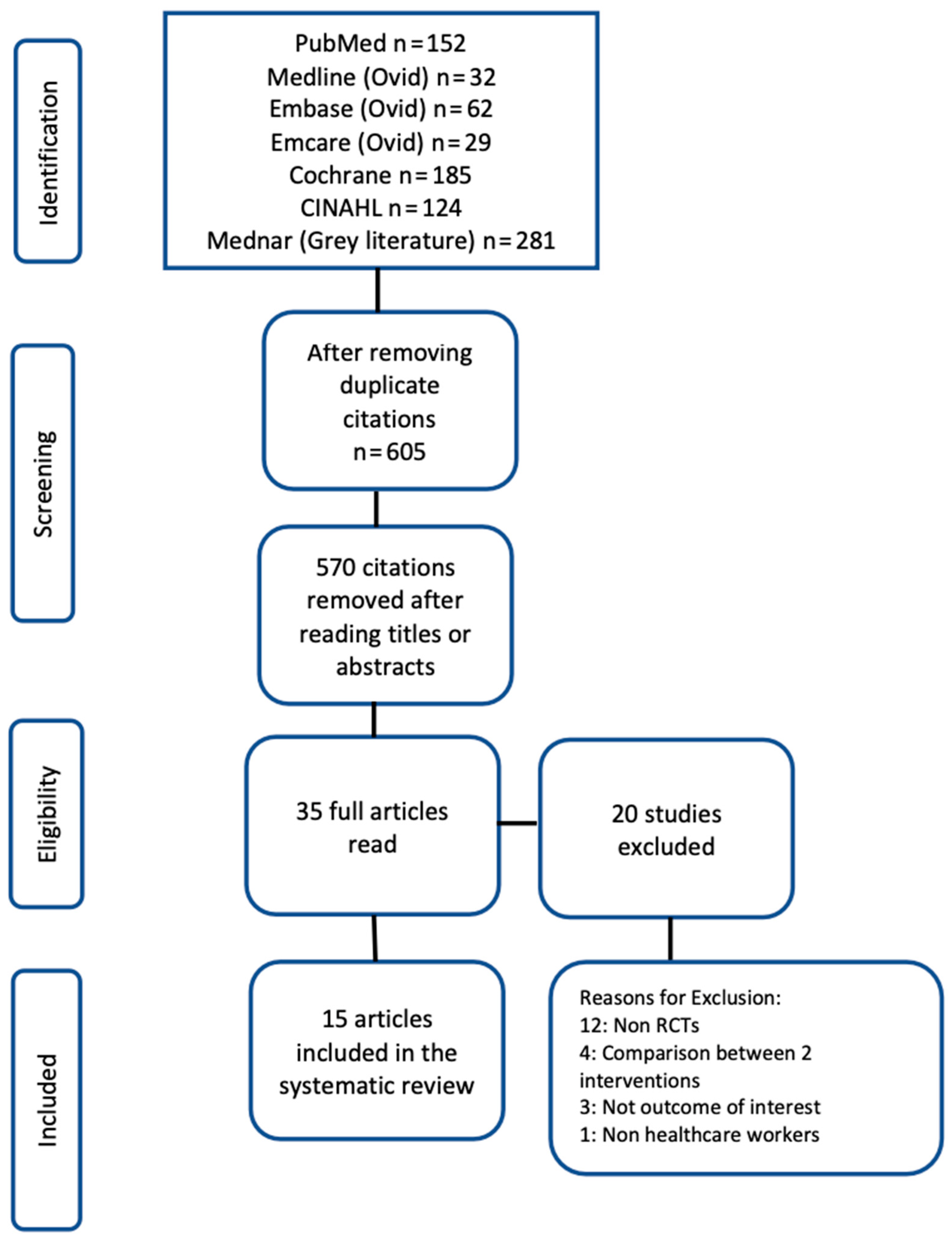
2.1. Literature Search
- (1)
- The above-mentioned databases were searched for systematic reviews on interventions for compassion fatigue. PubMed were searched using the search terms (“compassion fatigue”[MeSH Terms] OR (“compassion”[All Fields] AND “fatigue”[All Fields]) OR “compassion fatigue”[All Fields]) AND (meta-analysis [Filter] OR systematic review [Filter]). Similar terms were used for other databases.
- (2)
- All databases were searched again for individual RCTs on interventions for compassion fatigue. PubMed was searched using the following broad key words: ((compassion fatigue) OR (compassion satisfaction)) OR (empathy fatigue) Filters: Clinical Trial, Randomized Controlled Trial. That automatic mapping system of PubMed expanded it to cover all the following terms: (“compassion fatigue”[MeSH Terms] OR (“compassion”[All Fields] AND “fatigue”[All Fields]) OR “compassion fatigue”[All Fields] OR ((“empathy”[MeSH Terms] OR “empathy”[All Fields] OR “compassion”[All Fields]) AND (“personal satisfaction”[MeSH Terms] OR (“personal”[All Fields] AND “satisfaction”[All Fields]) OR “personal satisfaction”[All Fields] OR “satisfaction”[All Fields] OR “satisfactions”[All Fields] OR “satisfaction s”[All Fields])) OR ((“empathy”[MeSH Terms] OR “empathy”[All Fields]) AND (“fatiguability”[All Fields] OR “fatiguable”[All Fields] OR “fatigue”[MeSH Terms] OR “fatigue”[All Fields] OR “fatigued”[All Fields] OR “fatigues”[All Fields] OR “fatiguing”[All Fields] OR “fatigueability”[All Fields]))) AND (clinicaltrial[Filter] OR randomizedcontrolledtrial[Filter]). Similar terms were used for other databases.
2.2. Inclusion Criteria
2.3. Assessing the Risk of Bias (ROB)
2.4. Data Extraction
2.5. Data Synthesis
2.6. Assessment of Heterogeneity, Publication Bias and Certainty of the Evidence (CoE)
2.7. Exploring Heterogeneity
3. Results
3.1. Approach to Synthesis
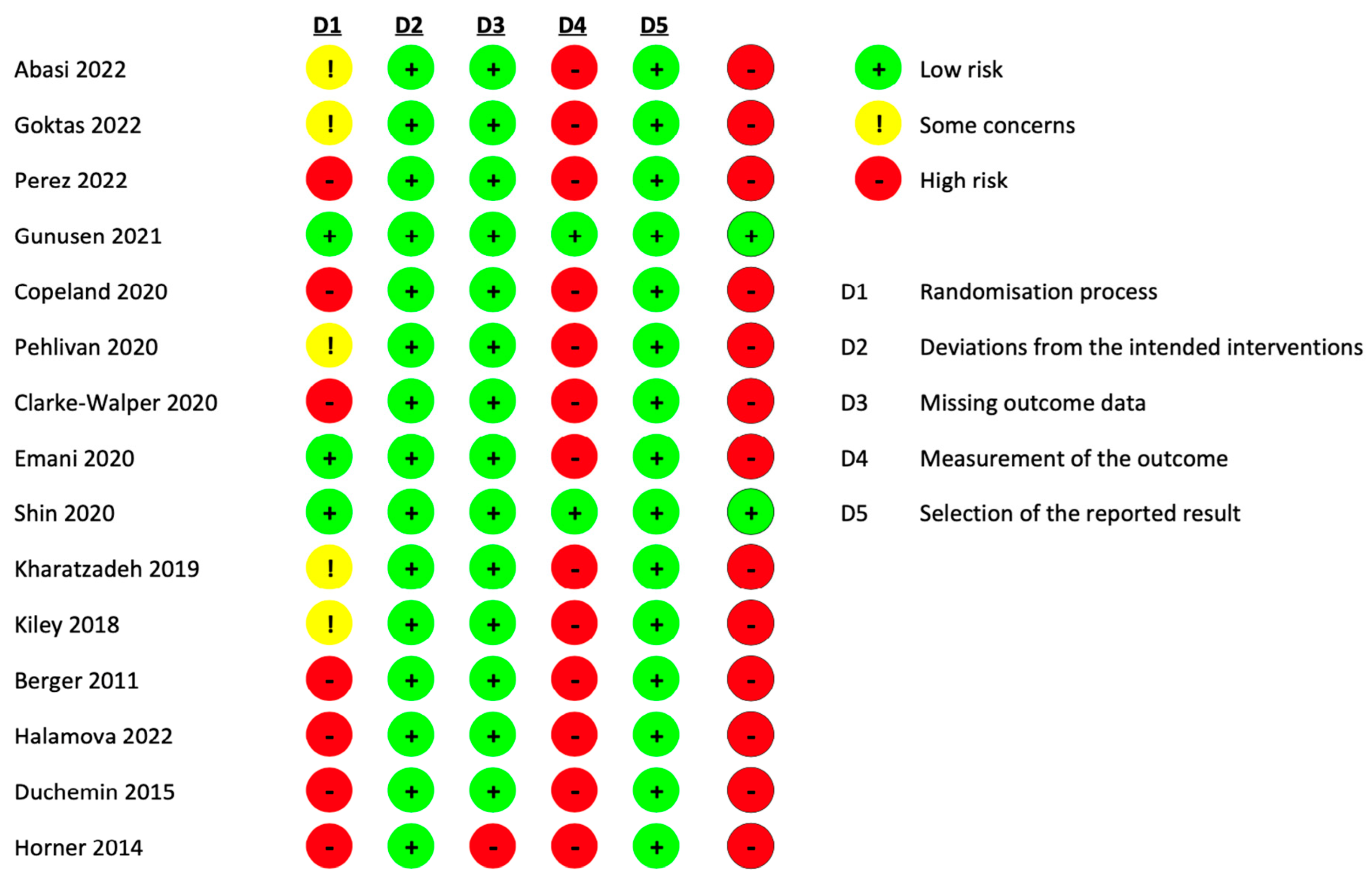
3.2. Risk of Bias Assessment (Figure 2)

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Decety, J.; Bartal, I.B.-A.; Uzefovsky, F.; Knafo-Noam, A. Empathy as a driver of prosocial behaviour: Highly conserved neurobehavioural mechanisms across species. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150077. [Google Scholar] [CrossRef]
- Irving, P.; Dickson, D. Empathy: Towards a conceptual framework for health professionals. Int. J. Health Care Qual. Assur. 2004, 17, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, D. Empathy, sympathy and compassion in healthcare: Is there a problem? Is there a difference? Does it matter? J. R. Soc. Med. 2016, 109, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, D. Clarifying empathy: The first step to more humane clinical care. Br. J. General. Pract. 2016, 66, e143–e145. [Google Scholar] [CrossRef] [PubMed]
- Moudatsou, M.; Stavropoulou, A.; Philalithis, A.; Koukouli, S. The role of empathy in health and social care professionals. Healthcare 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Moscrop, A.; Mebius, A.; Fanshawe, T.R.; Lewith, G.; Bishop, F.L.; Mistiaen, P.; Roberts, N.W.; Dieninytė, E.; Hu, X.-Y.; et al. Effects of empathic and positive communication in healthcare consultations: A systematic review and meta-analysis. J. R. Soc. Med. 2018, 111, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Dambha-Miller, H.; Feldman, A.L.; Kinmonth, A.L.; Griffin, S.J. Association between primary care practitioner empathy and risk of cardiovascular events and all-cause mortality among patients with type 2 diabetes: A population-based prospective cohort study. Ann. Fam. Med. 2019, 17, 311–318. [Google Scholar] [CrossRef]
- Sturzu, L.; Lala, A.; Bisch, M.; Guitter, M.; Dobre, D.; Schwan, R. Empathy and burnout–a cross-sectional study among mental healthcare providers in France. J. Med. Life 2019, 12, 21. [Google Scholar] [CrossRef] [PubMed]
- Doyle, C.; Lennox, L.; Bell, D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open 2013, 3, e001570. [Google Scholar] [CrossRef]
- Wilkinson, H.; Whittington, R.; Perry, L.; Eames, C. Examining the relationship between burnout and empathy in healthcare professionals: A systematic review. Burn. Res. 2017, 6, 18–29. [Google Scholar] [CrossRef]
- Babaei, S.; Taleghani, F.; Farzi, S. Components of Compassionate Care in Nurses Working in the Cardiac Wards: A Descriptive Qualitative Study. J. Caring Sci. 2022, 11, 240. [Google Scholar] [CrossRef]
- Chochinov, H.M. Dignity and the essence of medicine: The A, B, C, and D of dignity conserving care. BMJ 2007, 335, 184–187. [Google Scholar] [CrossRef]
- Goldberg, M.J. Compassionate Care: Making it a priority and the science behind it. J. Pediatr. Orthop. 2020, 40, S4–S7. [Google Scholar] [CrossRef]
- Perez-Bret, E.; Altisent, R.; Rocafort, J. Definition of compassion in healthcare: A systematic literature review. Int. J. Palliat. Nurs. 2016, 22, 599–606. [Google Scholar] [CrossRef]
- Frederick, C. Beyond empathy: The tree of compassion with malevolent ego states. Am. J. Clin. Hypn. 2016, 58, 331–346. [Google Scholar] [CrossRef]
- Sinclair, S.; Beamer, K.; Hack, T.F.; McClement, S.; Raffin Bouchal, S.; Chochinov, H.M.; Hagen, N.A. Sympathy, empathy, and compassion: A grounded theory study of palliative care patients’ understandings, experiences, and preferences. Palliat. Med. 2017, 31, 437–447. [Google Scholar] [CrossRef]
- Goetz, J.L.; Keltner, D.; Simon-Thomas, E. Compassion: An evolutionary analysis and empirical review. Psychol. Bull. 2010, 136, 351. [Google Scholar] [CrossRef]
- Hiçdurmaz, D.; İnci, F.A. Compassion fatigue: Description, causes and prevention. Curr. Approaches Psychiatry 2015, 7, 295–303. [Google Scholar] [CrossRef]
- Field, B. Can You Have too Much Empathy? 20 May 2022. Available online: https://www.verywellmind.com/can-you-have-too-much-empathy-5224139 (accessed on 12 April 2023).
- Oshberg, F. When Helping Hurts: The American Stress Institute. 2022. Available online: https://www.stress.org/military/for-practitionersleaders/compassion-fatigue (accessed on 12 April 2023).
- Haque, O.S.; Waytz, A. Why doctors should be more empathetic—But not too much more. Sci. Am. 2011, 26. Available online: https://www.scientificamerican.com/article/doctors-and-dehumanization-effect/ (accessed on 12 April 2023).
- Figley, C.R. Compassion fatigue as secondary traumatic stress disorder: An overview. In Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Psychosocial Stress Series; Figley, C.R., Ed.; Routledge Taylor and Francis Group: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- Figley, C.R. Compassion fatigue: Toward a new understanding of the costs of caring. In Secondary Traumatic Stress: Self-Care Issues for Clinicians, Researchers, and Educators, 2nd ed.; Stamm, B.H., Ed.; The Sidran Press: Baltimore, MD, USA, 1999; pp. 3–28. [Google Scholar]
- Watson, J. The theory of human caring: Retrospective and prospective. Nurs. Sci. Q. 1997, 10, 49–52. [Google Scholar] [CrossRef]
- Watson, J. Nursing: The Philosophy and Science of Caring, Rev. ed.; University Press of Colorado: Boulder, CO, USA, 2008. [Google Scholar]
- Joinson, C. Coping with compassion fatigue. Nursing 1992, 22, 116, 118–120. [Google Scholar]
- Figley, C.R.; Kleber, R.J. Beyond the “victim”: Secondary traumatic stress. In Beyond Trauma: Cultural and Societal Dynamics; Kleber, R.J., Figley, C.R., Gersons, B.P.R., Eds.; Plenum Press: New York, NY, USA, 1995; pp. 75–98. [Google Scholar]
- Essary, J.N.; Barza, L.; Thurston, R.J. Secondary traumatic stress among educators. Kappa Delta Pi Rec. 2020, 56, 116–121. [Google Scholar] [CrossRef]
- Saggar, I. Compassion Satisfaction, Compassion Fatigue and Mental-Well Being among Health Care Workers during COVID-19 outbreak. Int. J. Indian Psychȯl. 2021, 9, 888–895. [Google Scholar] [CrossRef]
- Stamm, B. The Concise ProQOL Manual, 2nd ed.; ProQOL.org: Pocatello, ID, USA, 2010. [Google Scholar]
- Bhutani, J.; Bhutani, S.; Balhara, Y.P.S.; Kalra, S. Compassion fatigue and burnout amongst clinicians: A medical exploratory study. Indian. J. Psychol. Med. 2012, 34, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C. Job burnout: New directions in research and intervention. Curr. Dir. Psychol. Sci. 2003, 12, 189–192. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Buunk, B.P. Burnout: An overview of 25 years of research and theorizing. Handb. Work. Health Psychol. 2003, 2, 282–424. [Google Scholar]
- Ormiston, H.E.; Nygaard, M.A.; Apgar, S. A Systematic Review of Secondary Traumatic Stress and Compassion Fatigue in Teachers. Sch. Ment. Health 2022, 14, 802–817. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.; Olanloye, E.; Hon, Y.; England, A.; McNair, H.; Cruickshank, S. Are radiographers suffering from symptoms of compassion fatigue due to occupational stress: A systematic review. Radiography 2022, 28, 857–864. [Google Scholar] [CrossRef]
- Cieslak, R.; Shoji, K.; Douglas, A.; Melville, E.; Luszczynska, A.; Benight, C.C. A meta-analysis of the relationship between job burnout and secondary traumatic stress among workers with indirect exposure to trauma. Psychol. Serv. 2014, 11, 75. [Google Scholar] [CrossRef]
- McCann, I.L.; Pearlman, L.A. Vicarious traumatization: A framework for understanding the psychological effects of working with victims. J. Trauma. Stress. 1990, 3, 131–149. [Google Scholar] [CrossRef]
- Laurie Anne pearlman KWS. Treating therapists with vicarious traumatization and secondary traumatic stress disorders. In Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Figley, C.R., Ed.; Routledge Taylor and Francis Group: New York, NY, USA, 1995; pp. 150–177. [Google Scholar]
- Marshman, C.; Hansen, A.; Munro, I. Compassion fatigue in mental health nurses: A systematic review. J. Psychiatr. Ment. Health Nurs. 2022, 29, 529–543. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Campos, E.; Vargas-Román, K.; Velando-Soriano, A.; Suleiman-Martos, N.; Cañadas-de la Fuente, G.A.; Albendín-García, L.; Gómez-Urquiza, J.L. Compassion fatigue, compassion satisfaction, and burnout in oncology nurses: A systematic review and meta-analysis. Sustainability 2019, 12, 72. [Google Scholar] [CrossRef]
- Sousa, L.; Ferreira, B.; Silva, P.; Tomás, M.; José, H.; Garcia-Navarro, E.B.; Ortega-Galán, Á. Bibliometric Analysis of the Scientific Production on Compassion Fatigue. J. Pers. Med. 2022, 12, 1574. [Google Scholar] [CrossRef]
- Van Mol, M.M.; Kompanje, E.J.; Benoit, D.D.; Bakker, J.; Nijkamp, M.D. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: A systematic review. PLoS ONE 2015, 10, e0136955. [Google Scholar] [CrossRef]
- Stoewen, D.L. Moving from compassion fatigue to compassion resilience Part 4: Signs and consequences of compassion fatigue. Can. Vet. J. 2020, 61, 1207. [Google Scholar]
- Hooper, C.; Craig, J.; Janvrin, D.R.; Wetsel, M.A.; Reimels, E. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J. Emerg. Nurs. 2010, 36, 420–427. [Google Scholar] [CrossRef]
- Mathieu, F. The Compassion Fatigue Workbook: Creative Tools for Transforming Compassion Fatigue and Vicarious Traumatization; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Cocker, F.; Joss, N. Compassion fatigue among healthcare, emergency and community service workers: A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 618. [Google Scholar] [CrossRef]
- Aluttis, C.; Bishaw, T.; Frank, M.W. The workforce for health in a globalized context–global shortages and international migration. Glob. Health Action 2014, 7, 23611. [Google Scholar] [CrossRef]
- Conversano, C.; Ciacchini, R.; Orrù, G.; Di Giuseppe, M.; Gemignani, A.; Poli, A. Mindfulness, compassion, and self-compassion among health care professionals: What’s new? A systematic review. Front. Psychol. 2020, 11, 1683. [Google Scholar] [CrossRef]
- Xie, W.; Chen, L.; Feng, F.; Okoli, C.T.; Tang, P.; Zeng, L.; Jin, M.; Zhang, Y.; Wang, J. The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 120, 103973. [Google Scholar] [CrossRef] [PubMed]
- Crego, A.; Yela, J.R.; Riesco-Matías, P.; Gómez-Martínez, M.; Vicente-Arruebarrena, A. The Benefits of Self-Compassion in Mental Health Professionals: A Systematic Review of Empirical Research. Psychol. Res. Behav. Manag. 2022, 15, 2599–2620. [Google Scholar] [CrossRef]
- Gillman, L.; Adams, J.; Kovac, R.; Kilcullen, A.; House, A.; Doyle, C. Strategies to promote coping and resilience in oncology and palliative care nurses caring for adult patients with malignancy: A comprehensive systematic review. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 131–204. [Google Scholar] [CrossRef]
- Greinacher, A.; Derezza-Greeven, C.; Herzog, W.; Nikendei, C. Secondary traumatization in first responders: A systematic review. Eur. J. Psychotraumatol. 2019, 10, 1562840. [Google Scholar] [CrossRef]
- Hasanpoor, E.; Hajebrahimi, S.; Janati, A.; Abedini, Z.; Haghgoshayie, E. Barriers, facilitators, process and sources of evidence for evidence-based management among health care managers: A qualitative systematic review. Ethiop. J. Health Sci. 2018, 28. [Google Scholar] [CrossRef]
- Chen, X.; Chen, M.; Zheng, H.; Wang, C.; Chen, H.; Wu, Q.; Liao, H.; Zhu, J.; Lin, J.; Ou, X.; et al. Effects of psychological intervention on empathy fatigue in nurses: A meta-analysis. Front. Public. Health 2022, 10, 952932. [Google Scholar] [CrossRef]
- Xie, W.; Wang, J.; Luo, X.; Tang, P.; Zeng, L.; Jin, M. Meta-analysis of the effect of psychological intervention on compassion fatigue of nursing staff. Chin. J. Labor Health Occup. Dis. 2022, 40, 39–45. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: New York, NY, USA, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef]
- Deakin University, Master of Leadership, Unit MPP 703. Available online: https://www.deakin.edu.au/course/master-leadership (accessed on 12 April 2023).
- Bride, B.E.; Radey, M.; Figley, C.R. Measuring compassion fatigue. Clin. Social. Work. J. 2007, 35, 155–163. [Google Scholar] [CrossRef]
- Heritage, B.; Rees, C.S.; Hegney, D.G. The ProQOL-21: A revised version of the Professional Quality of Life (ProQOL) scale based on Rasch analysis. PLoS ONE 2018, 13, e0193478. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians: A systematic review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef]
- Yıldırım, S.; Cavcav, F. The Compassion Fatigue-Short Scale for healthcare professionals: A Turkish study of validity and reliability. Perspect. Psychiatr. Care 2021, 57, 1459–1465. [Google Scholar] [CrossRef]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Santesso, N.; Helfand, M.; Vist, G.; Kunz, R.; Brozek, J.; Norris, S.; Meerpohl, J.; Djulbegovic, B.; et al. GRADE guidelines: 12. Preparing summary of findings tables—Binary outcomes. J. Clin. Epidemiol. 2013, 66, 158–172. [Google Scholar] [CrossRef]
- Abasi, S.; Akbari, H.; Sabery, M. The effects of acupressure on sleep quality and compassion fatigue among emergency and critical care nurses during the coronavirus disease 2019 epidemic: A clinical trial. Nurs. Midwifery Stud. 2022, 11, 79–84. [Google Scholar]
- Goktas, S.; Gezginci, E.; Kartal, H. The effects of motivational messages sent to emergency nurses during the COVID-19 pandemic on job satisfaction, compassion fatigue, and communication skills: A randomized controlled trial. J. Emerg. Nurs. 2023, 48, 547–558, Erratum in: J. Emerg. Nurs. 2023, 49, 149. [Google Scholar] [CrossRef]
- Pérez, V.; Menéndez-Crispín, E.J.; Sarabia-Cobo, C.; de Lorena, P.; Fernández-Rodríguez, A.; González-Vaca, J. Mindfulness-based intervention for the reduction of compassion fatigue and burnout in nurse caregivers of institutionalized older persons with dementia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 11441. [Google Scholar] [CrossRef]
- Partlak Günüşen, N.; Şengün İnan, F.; Üstün, B.; Serttaş, M.; Sayin, S.; Yaşaroğlu Toksoy, S. The effect of a nurse-led intervention program on compassion fatigue, burnout, compassion satisfaction, and psychological distress in nurses: A randomized controlled trial. Perspect. Psychiatr. Care 2022, 58, 1576–1586. [Google Scholar] [CrossRef]
- Halamová, J.; Ondrejková, N.; Kováč, K. Randomized controlled trial of emotion-focused training for helping professionals. Front. Psychol. 2022, 13, 1024451. [Google Scholar] [CrossRef]
- Copeland, D. Brief workplace interventions addressing burnout, compassion fatigue, and teamwork: A pilot study. West. J. Nurs. Res. 2021, 43, 130–137. [Google Scholar] [CrossRef]
- Pehlivan, T.; Güner, P. Effect of a compassion fatigue resiliency program on nurses’ professional quality of life, perceived stress, resilience: A randomized controlled trial. J. Adv. Nurs. 2020, 76, 3584–3596. [Google Scholar] [CrossRef] [PubMed]
- Clarke-Walper, K.; Penix, E.A.; Trachtenberg, F.; Simon, E.; Coleman, J.; Magnavita, A.; Ortigo, K.; Regala, S.; Marceau, L.; Ruzek, J.I.; et al. Efficacy of a web-based tool in reducing burnout among behavioral health clinicians: Results from the PTSD Clinicians Exchange. Psychiatr. Res. Clin. Pract. 2020, 2, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Emani, R.; Ghavami, H.; Radfar, M.; Khalkhali, H.R. Impact of chromotherapy on professional quality of life in intensive care unit nurses: A randomized controlled trial. Fatigue Biomed. Health Behav. 2020, 8, 121–129. [Google Scholar] [CrossRef]
- Shin, Y.K.; Lee, S.Y.; Lee, J.M.; Kang, P.; Seol, G.H. Effects of short-term inhalation of Patchouli oil on professional quality of life and stress levels in emergency nurses: A randomized controlled trial. J. Altern. Complement. Med. 2020, 26, 1032–1038. [Google Scholar] [CrossRef]
- Kharatzadeh, H.; Alavi, M.; Mohammadi, A.; Visentin, D.; Cleary, M. Emotional regulation training for intensive and critical care nurses. Nurs. Health Sci. 2020, 22, 445–453. [Google Scholar] [CrossRef]
- Kiley, K.A.; Sehgal, A.R.; Neth, S.; Dolata, J.; Pike, E.; Spilsbury, J.C.; Albert, J.M. The effectiveness of guided imagery in treating compassion fatigue and anxiety of mental health workers. Social. Work. Res. 2018, 42, 33–43. [Google Scholar] [CrossRef]
- Duchemin, A.M.; Steinberg, B.A.; Marks, D.R.; Vanover, K.; Klatt, M. A small randomized pilot study of a workplace mindfulness-based intervention for surgical intensive care unit personnel: Effects on salivary α-amylase levels. J. Occup. Environ. Med. 2015, 57, 393. [Google Scholar] [CrossRef]
- Horner, J.K.; Piercy, B.S.; Eure, L.; Woodard, E.K. A pilot study to evaluate mindfulness as a strategy to improve inpatient nurse and patient experiences. Appl. Nurs. Res. 2014, 27, 198–201. [Google Scholar] [CrossRef]
- Berger, R.; Gelkopf, M. An intervention for reducing secondary traumatization and improving professional self-efficacy in well baby clinic nurses following war and terror: A random control group trial. Int. J. Nurs. Stud. 2011, 48, 601–610. [Google Scholar] [CrossRef]
- Stamm, B.H. Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL); ProQOL.org: Pocatello, ID, USA, 2009. [Google Scholar]
- Stamm, B.H. The ProQOL Manual: The Professional Quality of Life Scale: Compassion Satisfaction, Burnout & Compassion Fatigue/Secondary Trauma Scales; Sidran Press: Baltimore, MD, USA, 2005; pp. S1–S13. [Google Scholar]
- Hotchkiss, J.T.; Wong, M.Y.C. Factorial Structure of the ProQOL—Systematic Meta-analysis and Integration of 27 International Factor Analysis Studies. Trends Psychol. 2022, 1–32. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Cho, E. A comprehensive review of so-called Cronbach’s alpha. J. Product. Res. 2020, 38, 9–20. [Google Scholar]
- Sabery, M.; Tafreshi, M.Z.; Hosseini, M.; Mohtashami, J.; Ebadi, A. Development and psychometric evaluation of the nurses’ compassion fatigue inventory. J. Nurs. Meas. 2017, 25, 185–201. [Google Scholar] [CrossRef]
- Kang, H.; Bang, K. Development and evaluation of a self-reflection program for intensive care unit nurses who have experienced the death of pediatric patients. J. Korean Acad. Nurs. 2017, 47, 392. [Google Scholar] [CrossRef]
- Wylde, C.M.; Mahrer, N.E.; Meyer, R.M.; Gold, J.I. Mindfulness for novice pediatric nurses: Smartphone application versus traditional intervention. J. Pediatr. Nurs. 2017, 36, 205–212. [Google Scholar] [CrossRef]
- Slatyer, S.; Craigie, M.; Heritage, B.; Davis, S.; Rees, C. Evaluating the effectiveness of a brief mindful self-care and resiliency (MSCR) intervention for nurses: A controlled trial. Mindfulness 2018, 9, 534–546. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Evaluating Stress: A Book of Resources; Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1997; Volume 3, pp. 191–218. [Google Scholar]
- Wagnild, G.M.; Guinn, P.E.; Center, R. The Resilience Scale User’s Guide: For the Us English Version of the Resilience Scale and the 14-Item Resilience Scale (rs-14); Resilience Center: Billings, MT, USA, 2011. [Google Scholar]
- Flarity, K.; Gentry, J.E.; Mesnikoff, N. The effectiveness of an educational program on preventing and treating compassion fatigue in emergency nurses. Adv. Emerg. Nurs. J. 2013, 35, 247–258. [Google Scholar] [CrossRef]
- Hansen, E.M.; Eklund, J.H.; Hallén, A.; Bjurhager, C.S.; Norrström, E.; Viman, A.; Stocks, E.L. Does feeling empathy lead to compassion fatigue or compassion satisfaction? The role of time perspective. J. Psychol. 2018, 152, 630–645. [Google Scholar] [CrossRef] [PubMed]
- Wagaman, M.A.; Geiger, J.M.; Shockley, C.; Segal, E.A. The role of empathy in burnout, compassion satisfaction, and secondary traumatic stress among social workers. Soc. Work. 2015, 60, 201–209. [Google Scholar] [CrossRef]
- Cummings, C.; Singer, J.; Hisaka, R.; Benuto, L.T. Compassion satisfaction to combat work-related burnout, vicarious trauma, and secondary traumatic stress. J. Interpers. Violence 2021, 36, NP5304–NP5319. [Google Scholar] [CrossRef]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research: Study design: Randomised controlled trials. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef] [PubMed]
- Hannan, E.L. Randomized clinical trials and observational studies: Guidelines for assessing respective strengths and limitations. JACC Cardiovasc. Interv. 2008, 1, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Thadani, R. Formal trials versus observational studies. Chapter 14. In Fabry Disease: Perspectives from 5 Years of FOS.; Mehta, A., Beck, M., Sunder-Plassmann, G., Eds.; Oxford Pharma Genesis: Oxford, UK, 2006. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11597/ (accessed on 12 April 2023).
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef]
- Centre for Evaluation. London School of Hygiene and Tropical Medicine. Available online: https://www.lshtm.ac.uk/research/centres/centre-evaluation/cluster-randomised-trials#:~:text=In%20some%20circumstances%2C%20cluster%20randomisation,rather%20than%20at%20individual%20level (accessed on 18 April 2023).
- Taljaard, M.; Grimshaw, J.M. Concept, characteristics and implications of cluster randomization. Clin. Investig. 2014, 4, 1–4. [Google Scholar] [CrossRef]
- Elley, C.R.; Chondros, P.; Kerse, N.M. Randomised trials—Cluster versus individual randomisation Primary Care Alliance for Clinical Trials (PACT) network. Aust. Fam. Physician Sept. 2004, 33, 759–763. [Google Scholar]
- Hemming, K.; Eldridge, S.; Forbes, G.; Weijer, C.; Taljaard, M. How to design efficient cluster randomised trials. BMJ 2017, 358, j3064. [Google Scholar] [CrossRef] [PubMed]
- Hemming, K.; Girling, A.J.; Sitch, A.J.; Marsh, J.; Lilford, R.J. Sample size calculations for cluster randomised controlled trials with a fixed number of clusters. BMC Med. Res. Methodol. 2011, 11, 102, Erratum in: BMC Med. Res. Methodol. 2017, 17, 8.. [Google Scholar] [CrossRef]
- Campbell, M.K.; Grimshaw, J.M.; Elbourne, D.R. Intracluster correlation coefficients in cluster randomized trials: Empirical insights into how should they be reported. BMC Med. Res. Methodol. 2004, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Tishkovskaya, S.V.; Sutton, C.J.; Thomas, L.H.; Watkins, C.L. Determining the sample size for a cluster-randomised trial using knowledge elicitation: Bayesian hierarchical modelling of the intracluster correlation coefficient. Clin. Trials 2023, 10, 17407745231164569. [Google Scholar] [CrossRef]
- Tong, J.; Li, F.; Harhay, M.O.; Tong, G. Accounting for expected attrition in the planning of cluster randomized trials for assessing treatment effect heterogeneity. BMC Med. Res. Methodol. 2023, 23, 85. [Google Scholar] [CrossRef]
- Harrison, L.J.; Wang, R. Sample size calculation for randomized trials via inverse probability of response weighting when outcome data are missing at random. Stat. Med. 2023, 42, 1802–1821. [Google Scholar] [CrossRef]
- Davis-Plourde, K.; Taljaard, M.; Li, F. Power analyses for stepped wedge designs with multivariate continuous outcomes. Stat. Med. 2023, 42, 559–578. [Google Scholar] [CrossRef]
- Bolland, M.J.; Avenell, A.; Grey, A. Analysis of cluster randomised trials as if they were individually randomised. Lancet Diabetes Endocrinol. 2023, 11, 75. [Google Scholar] [CrossRef]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef]
- Dreischulte, T.; Grant, A.; Donnan, P.; Guthrie, B. Pro’s and con’s of the stepped wedge design in cluster randomised trials of quality improvement interventions: Two current examples. Trials 2013, 14 (Suppl. S1), O87. [Google Scholar] [CrossRef][Green Version]
- Lee, H.J.; Lee, M.; Jang, S.J. Compassion satisfaction, secondary traumatic stress, and burnout among nurses working in trauma centers: A cross-sectional study. Int. J. Env. Res. Public. Health 2021, 18, 7228. [Google Scholar] [CrossRef] [PubMed]
- Misouridou, E.; Pavlou, V.; Kasidi, K.; Apostolara, P.; Parissopoulos, S.; Mangoulia, P.; Fradelos, E. Translation and cultural adaptation of the Professional Quality of Life Scale (ProQOL V) for Greece. Mater. Sociomed. 2020, 32, 187–190. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| No | Study Details (Ref) | Participants (n) | Intervention | Control | Outcomes | Tool of Assessment |
|---|---|---|---|---|---|---|
| 1 | Abasi 2022, Iran [69] | Nurses in ED and ICU (80) | Acupressure on the Shenmen point (1 month) | No acupressure |
| NCFI, PSQI |
| 2 | Goktas 2022, Turkey [70] | Nurses working in ED (65) | Motivational messages (21 days) | No motivational messages |
| CFS, Job satisfaction scale, communication skills scale. |
| 3 | Perez 2022, Spain [71] | Nurses working in elderly care centre (74) | MBCT program (6 weeks) | No MBCT for 3-month study period (Wait list) |
| ProQoL (R-IV) |
| 4 | Gunusen 2022, Turkey [72] | Nurses in general inpatient units (48) | Nurse-led program based on CBT (4 weeks) | No CBT for 6-month study period (Wait list) |
| ProQoL (R-IV) |
| 5 | Halamova 2022, Slovakia [73] | Healthcare and allied professionals (253) | EFT-HP (2 weeks) | No EFT-HP |
| STS scale, OLBI, FSCRS, SOCS-S, SOCS-O |
| 6 | Copeland 2020, USA [74] | Nurses in level 1 trauma centre (23) | Meditation, Outing, Gratitude and Journaling (6 weeks) | No change in work practice for 6-week study period |
| ProQoL |
| 7 | Pehlivan 2020, Turkey [75] | Nurses in oncology haematology inpatient services, outpatient chemotherapy units, and bone marrow transplant units (125) | CFRP (5 weeks) | No CFRP |
| ProQoL (R-IV), Perceived stress scale, Resilience scale |
| 8 | Clarke-Walper 2020, USA [76] | Behavioural health clinicians in the U.S. Department of Veterans Affairs, Department of Défense, and general community (605) | PTSD Clinicians Exchange (12 months) | Newsletter only |
| PTSD Clinicians Exchange that included ProQoL (R-V), Questions about clinical practice, EBPAS, new 7-point scale developed for assessing organisational support. |
| 9 | Emani 2020, Iran [77] | Nurses working in ICU (80) | Chromotherapy with educational sessions and individualised consulting sessions (3 months) | No chromotherapy, education or consulting |
| ProQoL |
| 10 | Shin 2020, Korea [78] | Nurses working in emergency department (60) | Short-term inhalation of Patchouli oil (24 h) | Pure sweet almond oil inhalation |
| ProQoL (R-V), visual analogues scale for stress, an electronic sphygmomanometer |
| 11 | Kharatzadeh 2019, Iran [79] | Nurses in the intensive and critical care units (60) | ERT sessions (six sessions × 2 h each) | No ERT sessions for the study period (Wait list) |
| ProQoL (R-V), Cognitive Emotion Regulation Questionnaire, Depression, Anxiety and Stress Scale |
| 12 | Kiley 2018, USA [80] | Mental health workers (69) | Guided imagery as a relaxation technique (4 weeks) | No guided imagery |
| ProQoL (R-V), Perceived Stress Scale, PSQI, State Trait Anxiety Inventory |
| 13 | Duchemin 2015, USA [81] | Personnel working in the SICU (32) | Group MBI (8 weeks) | No group mindfulness-based intervention (MBI) (wait list) |
| ProQOF, Maslach Burnout Inventory, PSS, DASS-21 |
| 14 | Horner 2014, USA [82] | Personnel working Medical–Surgical units providing intermediate intensity of care (86) | Mindfulness training program (10 weeks) | No mindfulness training program |
| ProQoL (R-V), MAAS, HCAHPS survey |
| 15 | Berger 2011, Israel [83] | Nurses in Well baby clinic (80) | Sessions on psycho-educational knowledge and stress management techniques (12 weeks) | No sessions on psycho-educational knowledge and stress management techniques till study end (Wait list) |
| DHSES, ProQoL, RSE, Self-rated Hope Scale, Mastery scale. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patole, S.; Pawale, D.; Rath, C. Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials. Healthcare 2024, 12, 171. https://doi.org/10.3390/healthcare12020171
Patole S, Pawale D, Rath C. Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials. Healthcare. 2024; 12(2):171. https://doi.org/10.3390/healthcare12020171
Chicago/Turabian StylePatole, Sanjay, Dinesh Pawale, and Chandra Rath. 2024. "Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials" Healthcare 12, no. 2: 171. https://doi.org/10.3390/healthcare12020171
APA StylePatole, S., Pawale, D., & Rath, C. (2024). Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials. Healthcare, 12(2), 171. https://doi.org/10.3390/healthcare12020171