
A Culture of Early Mobilization in Adult Intensive Care Units: Perspective and Competency of Physicians

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Method
2.1. Study Design
2.2. Participants and Setting
2.3. Development of the Survey
2.4. Data Analysis
3. Results
3.1. Description of the Participants
3.2. Theoretical Knowledge about Early Mobilization in the ICU
3.3. Clinical Competency of Physicians Working in ICU about EM
3.4. Determining Theoretical and Clinical Competency of Physicians Working in Adults ICU Settings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
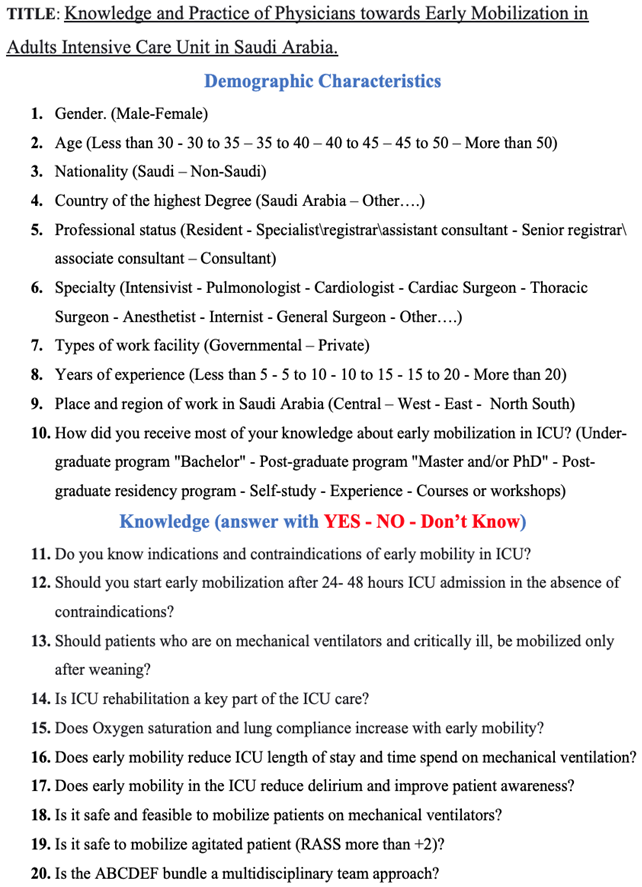
Appendix A. The Survey of Knowledge and Practice toward EM

References
- Brower, R.G. Consequences of Bed Rest. Crit. Care Med. 2009, 37, S422–S428. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ren, D.; Liu, Y.; Wang, Y.; Zhang, B.; Xiao, Q. Effects of Early Mobilization on the Prognosis of Critically Ill Patients: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2020, 110, 103708. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hu, W.; Cai, Z.; Liu, J.; Wu, J.; Deng, Y.; Yu, K.; Chen, X.; Zhu, L.; Ma, J. Early Mobilization of Critically Ill Patients in the Intensive Care Unit: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0223185. [Google Scholar] [CrossRef] [PubMed]
- Schaller, S.J.; Scheffenbichler, F.T.; Bose, S.; Mazwi, N.; Deng, H.; Krebs, F.; Seifert, C.L.; Kasotakis, G.; Grabitz, S.D.; Latronico, N. Influence of the Initial Level of Consciousness on Early, Goal-Directed Mobilization: A Post Hoc Analysis. Intensive Care Med. 2019, 45, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Waldauf, P.; Jiroutková, K.; Krajčová, A.; Puthucheary, Z.; Duška, F. Effects of Rehabilitation Interventions on Clinical Outcomes in Critically Ill Patients: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2020, 48, 1055–1065. [Google Scholar] [CrossRef]
- Lord, R.K.; Mayhew, C.R.; Korupolu, R.; Mantheiy, E.C.; Friedman, M.A.; Palmer, J.B.; Needham, D.M. ICU Early Physical Rehabilitation Programs: Financial Modeling of Cost Savings. Crit. Care Med. 2013, 41, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.E.; Goad, A.; Thompson, C.; Taylor, K.; Harry, B.; Passmore, L.; Ross, A.; Anderson, L.; Baker, S.; Sanchez, M. Early Intensive Care Unit Mobility Therapy in the Treatment of Acute Respiratory Failure. Crit. Care Med. 2008, 36, 2238–2243. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.E.; Berry, M.J.; Files, D.C.; Thompson, J.C.; Hauser, J.; Flores, L.; Dhar, S.; Chmelo, E.; Lovato, J.; Case, L.D. Standardized Rehabilitation and Hospital Length of Stay among Patients with Acute Respiratory Failure: A Randomized Clinical Trial. JAMA 2016, 315, 2694–2702. [Google Scholar] [CrossRef]
- Jones, S.; Carley, S.; Harrison, M. An Introduction to Power and Sample Size Estimation. Emerg. Med. J. 2003, 20, 453–458. [Google Scholar] [CrossRef]
- Qutub, H.O.; Matani, A.S.; Farooqi, F.A. Survey of Respiratory Care Professionals’ Knowledge in Early Mobilization: A Pilot Study. J. Epidemiol. Glob. Health 2018, 8, 208. [Google Scholar] [CrossRef]
- Hodgson, C.L.; Capell, E.; Tipping, C.J. Early Mobilization of Patients in Intensive Care: Organization, Communication and Safety Factors That Influence Translation into Clinical Practice. Crit. Care 2018, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Zheng, Q.; Zuo, D.; Zhang, C.; Gan, X. Safety Assessment Criteria for Early Active Mobilization in Mechanically Ventilated ICU Subjects. Respir. Care 2021, 66, 307–315. [Google Scholar] [CrossRef]
- Lang, J.K.; Paykel, M.S.; Haines, K.J.; Hodgson, C.L. Clinical Practice Guidelines for Early Mobilization in the ICU: A Systematic Review. Crit. Care Med. 2020, 48, e1121. [Google Scholar] [CrossRef]
- Zão, A. The Role of Early Mobilization in the Intensive Care. Int. J. Physiatry 2018, 4, 014. [Google Scholar]
- Adler, J.; Malone, D. Early Mobilization in the Intensive Care Unit: A Systematic Review. Cardiopulm. Phys. Ther. J. 2012, 23, 5. [Google Scholar] [CrossRef]
- Fontela, P.C.; Forgiarini Jr, L.A.; Friedman, G. Clinical Attitudes and Perceived Barriers to Early Mobilization of Critically Ill Patients in Adult Intensive Care Units. Rev. Bras. Ter. Intensiv. 2018, 30, 187–194. [Google Scholar] [CrossRef]
- Fleming, L.M.; Zhao, X.; DeVore, A.D.; Heidenreich, P.A.; Yancy, C.W.; Fonarow, G.C.; Hernandez, A.F.; Kociol, R.D. Early Ambulation among Hospitalized Heart Failure Patients Is Associated with Reduced Length of Stay and 30-Day Readmissions. Circ. Heart Fail. 2018, 11, e004634. [Google Scholar] [CrossRef]
- Rosa, R.G.; Teixeira, C.; Sjoding, M. Novel Approaches to Facilitate the Implementation of Guidelines in the ICU. J. Crit. Care 2020, 60, 1–5. [Google Scholar] [CrossRef]
- MacIntyre, N.R. Early Mobilization of Patients on Mechanical Ventilation: Worth the Effort and Expense? Respir. Care 2019, 64, 112–113. [Google Scholar] [CrossRef]
- Clini, E.; Ambrosino, N. Early Physiotherapy in the Respiratory Intensive Care Unit. Respir. Med. 2005, 99, 1096–1104. [Google Scholar] [CrossRef]
- Taito, S.; Shime, N.; Ota, K.; Yasuda, H. Early Mobilization of Mechanically Ventilated Patients in the Intensive Care Unit. J. Intensive Care 2016, 4, 1–7. [Google Scholar] [CrossRef]
- Akinremi, A.A.; Ogwu, S.; Sanya, A.O.; Sanusi, A.A.; Osinaike, B. Early Mobilization in the ICU: A Multicenter Survey of Clinicians’ Knowledge, Attitude and Practices in Resource-Limited Hospital Settings. Ann. Med. Health Sci. Res. 2020, 10, 778–784. [Google Scholar]
- Akhtar, P.M.; Deshmukh, P.K. Knowledge, Attitudes, and Perceived Barriers of Healthcare Providers toward Early Mobilization of Adult Critically Ill Patients in Intensive Care Unit. Indian J. Crit. Care Med. 2021, 25, 512. [Google Scholar] [CrossRef]
- Koo, K.K.; Choong, K.; Cook, D.J.; Herridge, M.; Newman, A.; Lo, V.; Guyatt, G.; Priestap, F.; Campbell, E.; Burns, K.E. Early Mobilization of Critically Ill Adults: A Survey of Knowledge, Perceptions and Practices of Canadian Physicians and Physiotherapists. Can. Med. Assoc. Open Access J. 2016, 4, E448–E454. [Google Scholar] [CrossRef]
- Li, Z.; Peng, X.; Zhu, B.; Zhang, Y.; Xi, X. Active Mobilization for Mechanically Ventilated Patients: A Systematic Review. Arch. Phys. Med. Rehabil. 2013, 94, 551–561. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
| Country of the Highest Degree | ||
| Saudi Arabia | 181 | 76.7 |
| Other | 55 | 23.3 |
| Total | 236 | 100.0 |
| Professional Status | ||
| Senior Resident | 139 | 58.9 |
| Specialist | 71 | 30.1 |
| Consultant | 26 | 11.0 |
| Total | 236 | 100.0 |
| Specialty | ||
| Intensivist | 129 | 54.7 |
| Pulmonologist | 2 | 0.8 |
| Cardiologist | 12 | 5.1 |
| Cardiac surgeon | 5 | 2.1 |
| Thoracic surgeon | 7 | 3.0 |
| Anesthetist | 14 | 5.9 |
| Internist | 53 | 22.5 |
| General surgeon | 14 | 5.9 |
| Experience (years) | ||
| Less than 5 | 143 | 60.6 |
| 5–10 | 22 | 9.3 |
| 10–15 | 50 | 21.2 |
| 15–20 | 18 | 7.6 |
| More than 20 | 3 | 1.3 |
| Knowledge | Provided Correct Answer | Failed | Do Not Know |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Know (contra)indications of EM in the ICU | 224 (94.9) | 5 (2.1) | 7(3.0) |
| Start EM 24–48 h after ICU admission | 225 (95.3) | 6 (2.5) | 5 (2.1) |
| Start EM only if patients are weaned from ventilators | 89 (37.7) | 138 (58.5) | 9 (3.8) |
| ICU rehabilitation is a key part of ICU care | 234 (99.2) | 1 (0.4) | 1 (0.4) |
| EM increases oxygen saturation/lung compliance | 221 (93.6) | 6 (2.5) | 9 (3.8) |
| EM reduces ICU length of stay and time on ventilator | 228 (96.6) | 3 (1.3) | 5 (2.1) |
| EM reduces postoperative delirium | 224 (94.9) | 3 (1.3) | 9 (3.8) |
| It is safe and viable to mobilize patients on mechanical ventilators | 209 (88.6) | 18 (7.6) | 9 (3.8) |
| It is safe to mobilize agitated patients (RASS more than +2) | 96 (40.7) | 122 (51.7) | 18 (7.6) |
| The ABCDEF bundle is a multidisciplinary team approach | 120 (50.8) | 17 (7.2) | 99 (41.9) |
| Is the Patient a Candidate for Early Mobilization | Provided Correct Answer | Failed | Do Not Know |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Simple Cases | |||
| Case-1 | 225 (95.3) | 2 (0.8) | 9 (3.8) |
| Case-2 | 197 (83.5) | 27 (11.4) | 12 (5.1) |
| Case-3 | 199 (84.3) | 23 (9.7) | 14 (5.9) |
| Case-4 | 189 (80.1) | 33 (14) | 14 (5.9) |
| Difficult Cases | |||
| Case-5 | 100 (42.4) | 111 (47) | 25 (10.6) |
| Case-6 | 208 (88.1) | 16 (6.8) | 12 (5.1) |
| Challenging Cases | |||
| Case-7 | 97 (41.1) | 103 (43.6) | 36 (15.3) |
| Case-8 | 201 (85.2) | 25 (10.6) | 10 (4.2) |
| Complicated Cases | |||
| Case-9 | 80 (33.9) | 142 (60.2) | 14 (5.9) |
| Case-10 | 99 (41.9) | 86 (36.4) | 51 (21.6) |
| Specialty | Adequate Theoretical Knowledge | Adequate Clinical Decision |
|---|---|---|
| % | % | |
| Intensivist, n = 129 | 78 | 66 |
| Pulmonologist, n = 2 | 100 | 100 |
| Cardiologist, n = 12 | 92 | 92 |
| Cardiac surgeon, n = 5 | 100 | 100 |
| Thoracic surgeon, n = 7 | 86 | 100 |
| Anesthetist, n = 14 | 93 | 86 |
| Internist, n = 53 | 74 | 60 |
| General surgeon, n = 14 | 64 | 50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albarrati, A.; Aldhahi, M.I.; Almuhaid, T.; Alnahdi, A.; Alanazi, A.S.; Alqahtani, A.S.; Nazer, R.I. A Culture of Early Mobilization in Adult Intensive Care Units: Perspective and Competency of Physicians. Healthcare 2024, 12, 1300. https://doi.org/10.3390/healthcare12131300
Albarrati A, Aldhahi MI, Almuhaid T, Alnahdi A, Alanazi AS, Alqahtani AS, Nazer RI. A Culture of Early Mobilization in Adult Intensive Care Units: Perspective and Competency of Physicians. Healthcare. 2024; 12(13):1300. https://doi.org/10.3390/healthcare12131300
Chicago/Turabian StyleAlbarrati, Ali, Monira I. Aldhahi, Turki Almuhaid, Ali Alnahdi, Ahmed S. Alanazi, Abdulfattah S. Alqahtani, and Rakan I. Nazer. 2024. "A Culture of Early Mobilization in Adult Intensive Care Units: Perspective and Competency of Physicians" Healthcare 12, no. 13: 1300. https://doi.org/10.3390/healthcare12131300
APA StyleAlbarrati, A., Aldhahi, M. I., Almuhaid, T., Alnahdi, A., Alanazi, A. S., Alqahtani, A. S., & Nazer, R. I. (2024). A Culture of Early Mobilization in Adult Intensive Care Units: Perspective and Competency of Physicians. Healthcare, 12(13), 1300. https://doi.org/10.3390/healthcare12131300