
Interventions for School-Aged Children with Auditory Processing Disorder: A Scoping Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection of Sources of Evidence
2.6. Data Charting
2.7. Data Items
2.8. Critical Appraisal
2.9. Synthesis of Results
- Single-ability auditory training. The first method described in this review is AT, which focuses on a single auditory ability and includes structured listening activities tailored to enhance that specific auditory mechanism [15,28,36]. The fundamental aim of AT is to improve the neural processing of acoustic signals.
- Assistive devices (FM system). The use of the frequency modulation (FM) system, an assistive device, was another intervention method reported in the literature. According to the World Health Organization, assistive devices are products or piece of equipment that help maintain or improve a person’s functioning [23]. In the current review, the FM system was used in the classroom with the aim of enhancing the teacher’s voice and improving the student’s listening in the classroom.
- Hearing aids. These personal amplification devices, in which the receiver and microphone are both worn by the person who has difficulty hearing, can improve access to speech and environmental sounds and may improve SNRs for the person wearing the devices.
- Top-down interventions. These interventions focus on enhancing higher-order cognitive abilities (e.g., memory, attention, or problem-solving abilities), as well as language skills (e.g., vocabulary or metalinguistic abilities). Top-down interventions emphasize context and analysis of lower-order information, such as speech sounds. The aim is to improve listening abilities through compensatory and accommodative approaches [37].
- Multimodal interventions. These interventions incorporate a range of strategies aimed at enhancing AP abilities, listening skills and language skills and/or optimizing the listening environment. Multimodal interventions may involve a combination of bottom-up and top-down approaches addressing both fundamental auditory processes and higher-level cognitive functions. Additionally, multimodal interventions may include adaptations of the environment or the use of assistive devices with the goal of improving the listening experience.
3. Results
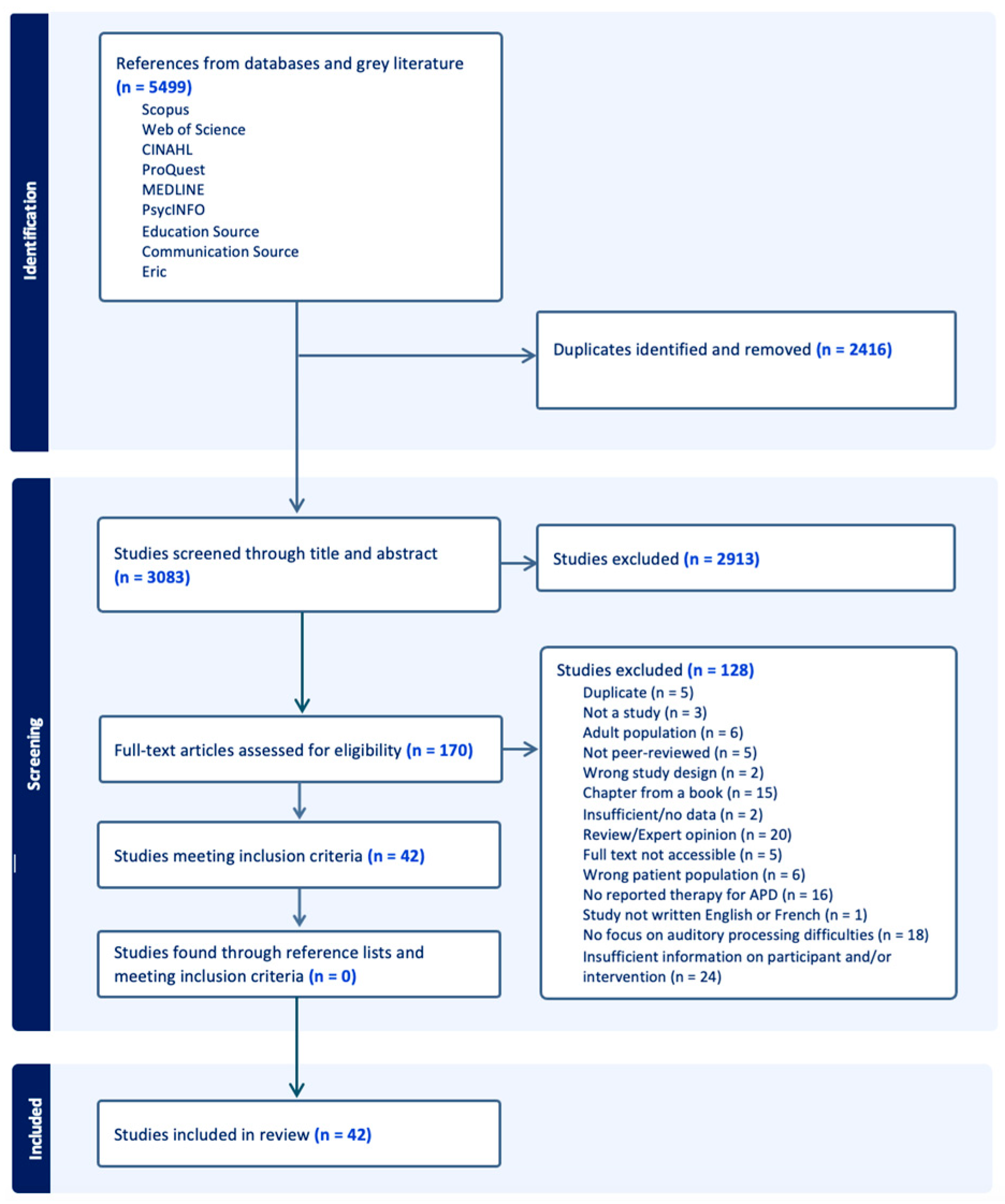
3.1. Selection of Sources of Evidence
3.2. Characteristics of Included Studies
3.3. Population Characteristics
3.4. Identification of Auditory Processing Disorder or Difficulties
- Dichotic listening (Dichotic Digits Test [DDT]) and temporal patterning (PPT) [52];
- Dichotic listening (DDT), temporal patterning (Pitch Pattern Sequence Test [PPST]), and auditory fusion (Auditory Fusion Test [AFT]) [53];
- Temporal resolution (RGDT), dichotic listening (Paediatric Speech Intelligibility—PSI test), and/or (Nonverbal Dichotic Test [NVDT]) [72];
- DDT with abnormal right ear advantage (REA), temporal patterning (PPST) and selective attention (Monaural Selective Auditory Attention Test [mSAAT]) [65];
- Temporal patterning (Frequency Pattern Test [FPT]) [47];
- Temporal patterning (Persian PST [P-PST]) and dichotic listening (Persian-SSW [P-SSW]) [61];
- Auditory figure ground (AFG test) [54];
- Dichotic listening, temporal patterning and selective memory (Multiple Auditory Processing Assessment [MAPA]), dichotic listening (Spectro-Temporal Modulation (STM) detection tasks) and SIN perception (Consonant–Vowel in Noise [CVN]) and Words in Noise Test [WIN]) [60];
- SIN perception (Monaural Speech Identification Test) [55];
- Temporal patterning (Duration Pattern Test [DPT]) [56].
3.5. Assessment Tools for Measuring Outcomes of Interventions
- Behavioural outcome measures. Behavioural measures are divided into AP measures and cognitive, language-based and academic measures. AP measures are subdivided based on the ability assessed, while cognitive, language-based and learning measures are categorized by the type of skill evaluated, including language, academic, reading, attention and memory skills.
- Neurophysiological outcome measures. Eleven AEP protocols were identified to measure outcomes following interventions. Neurophysiological changes were assessed following ATs focusing on single or multiple AP abilities, the use of an FM system, or multimodal interventions. In general, after an intervention, an improvement in neural signal transmission is indicated by an increase in wave amplitude and a decrease in wave latency [42,82]. However, reduced amplitudes and earlier latencies observed in speech-evoked cortical responses could indicate a shift toward a more mature morphology following an intervention [58,83]. There is some evidence that AEP is an objective measure that can document the neurophysiological changes in the auditory system [42,49,82].
- Questionnaires. Questionnaires are divided by respondent: teacher, parent, or child. Fifteen questionnaires were used as outcome measures, with parents and teachers being the most frequent respondents. Questionnaires answered by parents primarily focused on communication, auditory, and listening behaviours across various environments. Parents’ perceptions of changes in their child’s daily activities or listening abilities were assessed following various types of training, namely, SIN training, binaural processing training, AT targeting multiple abilities [70,72] and FM system use and fitting of binaural hearing aids. Significant changes were noted for binaural processing training and multiple-abilities training. One of the questionnaires, Mesure des habitudes de vie (MHAVIE; Translation: Assessment of life-habits) [50], assesses children’s lifestyle habits beyond listening and communication abilities by identifying specific activities of daily living that may pose challenges for them. Additionally, it helps determine whether the child requires help in performing these activities. The MHAVIE was utilized once for SIN training.
- Performance over the training sessions. Two studies evaluated the impact of binaural processing AT, while two others evaluated the effectiveness of SIN AT in terms of change across the training sessions. Improvement in performance during the training was significant [45,46,51] and non-significant [50], according to the authors.
- Statistical significance of the results. The statistical significance of the results at the different outcome measures listed in the studies is reported in Table A1. Results following the interventions were significant (S), non-significant (NS), or not different (ND) (indicating no discernable impact of the training on these measures) for the experimental group. One outcome measure (CNA) could not be analyzed because of the low return rate of questionnaires. For the sake of conciseness, the rating S or NS was assigned when the majority of subtests within a test battery measured S or NS changes, even if some subtests were ND. Conversely, the rating NS was assigned in the opposite situation. For neurophysiological tests, if changes were noted (regardless of whether the change was for latency or amplitude, with certain stimuli only, or in one or both ears), S or NS was assigned according to the results. Readers are directed to consult both the table of study characteristics and the individual studies for comprehensive details on the degree of change.
3.6. Intervention Characteristics
3.6.1. Single-Ability Auditory Training
- Dichotic listening training. The interventions aiming at improving dichotic listening used two approaches. The first one involved presenting different stimuli to both ears at various interaural time intervals [59,65,74,77,78]. As the training progresses and the child successfully completes tasks, the stimuli are gradually presented with decreased time intervals until they are eventually presented simultaneously. In some training programs, the stimuli start in the better ear [59], while in other programs, there is a variation in which the ear that receives the stimuli first (leading ear) may change [74]. Participants are asked to repeat what they hear in both ears (binaural integration tasks) or in one ear only (binaural separation tasks). Stimuli and presentation media vary from one program to another. Children completing interaural timing difference training have dichotic deficits, which are demonstrated by deficits in at least one ear at the DDT [59,74] or SSW and/or SCAN [77,78], or abnormal REA scores in the DDT [65].
- Localization and lateralization training. Two studies examined the impact of localization and lateralization training on spatial processing, localization and lateralization abilities [64,66]. The studies involved the same group of participants and the same intervention. The training focused on detecting and identifying sounds presented under headphones with various interaural time differences, which created the perception that the sounds were coming from distinct locations. To be included in the studies, results for the DDT (dichotic listening), PPS (temporal patterning) and mSAAT (auditory attention) had to be two standard deviations below the mean [64,66]. Following the intervention, the experimental group demonstrated significant improvements in auditory memory scores bilaterally [64,66], and in spatial word recognition in noisy conditions, when compared to the control group [64]. Noticeable neurophysiological changes were observed in the experimental group, compared to the control group. These changes were evidenced by a significant reduction in latency and an increase in amplitude, as measured by the BIC [66]. In summary, the benefits of the training were noted for binaural processing, SIN abilities and auditory memory.
- Spatial or binaural processing training. Three studies examined the efficacy of the Listening in Spatialized Noise Training (LiSN & Learn) [45,46,48]. This AT program is designed to enhance binaural processing through SIN activities, with target stimuli presented from the front, and the noise from various directions. This program aims to improve elements of binaural processing, such as interaural timing and intensity differences. These elements are crucial for spatial processing, allowing individuals to attend to stimuli originating from one direction while ignoring sounds or noises from other locations [46]. Participants had spatial processing disorder (SPD), diagnosed with the LiSN-S [45,46,48]. SPD is a subtype of APD and is “characterized as a reduced ability to utilize cues important for accurate localization and listening in noise” (p. 376, [46]).
- Musical training. The impact of singing lessons on the subcortical auditory response to the clicks and speech sounds of children who have an APD and, more precisely, difficulties with temporal processing, was investigated by Koravand et al. (2019) [49]. While no significant improvement was observed with click ABR post-training, the magnitude of various subcortical responses measured with speech stimuli showed improvement in the majority of the participants after training, suggesting the benefits of singing lessons for the central AP [49].
- Temporal patterning training. In their research, Maggu and Yathiraj (2010) aimed to improve temporal patterning abilities with temporal patterning training. The participants were children with low scores on the DPT [56]. The training activities involved discriminating and identifying tones based on variations in both frequency and duration [56]. Compared to a control group, the children who completed the training demonstrated significant improvements in the DPT, suggesting an amelioration of temporal patterning abilities [56]. The results in the other AP measures (auditory integration and separation, and gap detection) did not change post-training, but improvements were noted in auditory memory skills, suggesting that benefits generalized to other skills [56]. Improvements were maintained one month following training [56].
- Phonemic training. Negin et al. (2018) studied the effects of phonemic training on a child experiencing difficulties in phonemic awareness and decoding, as assessed by the P-PST and SSW. In this single-subject design study, a child learned various phonemes presented on their own, and eventually with other phonemes and in words. Different strategies were presented to the child to learn the phonemes. Positive effects of the training were observed in binaural integration abilities [61]. However, there was no improvement in phonemic awareness abilities [61]. Nevertheless, a significant reduction in the number of phoneme errors was noted [61]. Additionally, there were reported improvements in academic performance, particularly in spelling skills, following the training [61]. These improvements were sustained two months after the intervention [61].
- Speech in noise training. Nine identified studies investigated the impact of SIN training on noise tolerance and speech-recognition-in-noise abilities of children with AP difficulties or an APD, specifically those struggling with listening in noisy environments.
3.6.2. Multiple-Ability Auditory Training
3.6.3. Assistive Devices
3.6.4. Hearing Aids
3.6.5. Top-Down Intervention
3.6.6. Multimodal Approaches
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
| Auditory Training Single-Ability AP | Auditory Training Multiple Abilities AP | Assistive Device | Hearing Aids | TD | Multimodal | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Measures | DL [59,62,65,74,77,78,81] | Lat [64,66] | Bin P [45,46,48] | Music [47,49] | PhoT [61] | SIN [39,50,51,54,55,57,58,60,71] | Tem Pat [56] | TemP and PhoT [52,53] | BinInt, FG TemR [68] | SIN, DL, TemP [69] | FITT, DIID, Loc, SIN [70,72] | Personal FM System [41,73,75] | Binaural Mild Gain [80] | Working Memory [63] | TD and BU [42,44,67,76] |
| 1. Performance over the training sessions | |||||||||||||||
| S [45,46] | NS [50] S [51] | ||||||||||||||
| 2. BEHAVIORAL | |||||||||||||||
| 2.1 Auditory processing | |||||||||||||||
| 2.1.1 Spatial/binaural processing | |||||||||||||||
| LiSN-S | S [45,46,48] | S [39] | ND [41] | ||||||||||||
| Spatial WRS in noise | S [64] | ||||||||||||||
| CMAA | S [63] | ||||||||||||||
| MLD | ND [75] | ||||||||||||||
| 2.1.2 Temporal processing | |||||||||||||||
| DPT | S [54,57,58] | S [56] | |||||||||||||
| PPT, FPT, PPST | ND [81] | S [47] | S [71] | S [52,53] | S [68] | S [69] | S [75] | S [44] | |||||||
| GIN | NS [75] | ||||||||||||||
| GDT | S [57,58] | ND [56] | |||||||||||||
| AFT | S [53] | S [68] | |||||||||||||
| 2.1.3 Dichotic listening | |||||||||||||||
| DCV | ND [57,58] | ND [56] | |||||||||||||
| SSW (Persian, English) | S [62,77,78] | S [61] | S [71] | S [69] | S [70] | ||||||||||
| RDDT (Persian) | S [59] | ||||||||||||||
| NVDT | S [70] | ||||||||||||||
| DDT (Persian, English) | S [65,74,81] | S [52,53] | S [68] | S [69] | S [70] | NS [75] | NS [76] | ||||||||
| CST (Persian, English, Arabic) | S [59] | S [54] | NS [76] S/NS [67] | ||||||||||||
| CWT (Persian, English) | S [59,81] | ||||||||||||||
| DAT screening tool | S [77,78] | ||||||||||||||
| 2.1.4 Monaural low redundancy | |||||||||||||||
| LPFS (MLRT) | S [81] | NS [76] | |||||||||||||
| SSI-ICM (MLRT) | S [68] | ||||||||||||||
| SIN test | S [71] | S [69] | S [70] | ||||||||||||
| PSI (MLRT) | S [71] | S [70] | |||||||||||||
| mSAAT | S [64,66] | ||||||||||||||
| CVN (Persian) | S [60] | ||||||||||||||
| WIN (Persian, Indian English) | S [55,60] | S [67] | |||||||||||||
| AFG | NS [41] | ||||||||||||||
| CRW | S [75] | ||||||||||||||
| 2.1.5 SIN tests | |||||||||||||||
| Speech in spatial noise | NS [75] | ||||||||||||||
| HINT (French) | ND [50] NS [51] | ||||||||||||||
| HF-ESIT | S [55] | ||||||||||||||
| SIN (monosyllabic words, loudspeaker, Indian English) | S [55] | ||||||||||||||
| SPIN (English, Arabic, Indian English) | S [54,57,58] | ND [56] | |||||||||||||
| NU-6 in noise (loudspeaker) | ND [80] | ||||||||||||||
| HINT—reverberated/ compressed | ND [44] | ||||||||||||||
| 2.1.6 Test battery | |||||||||||||||
| SCAN-C/A | S [77] ND [78] | ||||||||||||||
| TAPS-3 | NS [46] | ||||||||||||||
| 2.1.7 Other | |||||||||||||||
| STMDT | S [60] | ||||||||||||||
| 2.2. Language/learning/cognitive | |||||||||||||||
| 2.2.1 Language | |||||||||||||||
| PAT | S [52,53] | ||||||||||||||
| C-TOPP | S [81] | ||||||||||||||
| CELF-4 | ND [47] | S [44] | |||||||||||||
| PST (Persian) | ND [61] | ||||||||||||||
| PEA (Persian) | S [61] | ||||||||||||||
| CASL | ND [44] | ||||||||||||||
| QUIL | S [44] | ||||||||||||||
| 2.2.2 Academic | |||||||||||||||
| SAT | NS [71] | ||||||||||||||
| CIBS-R | S [81] | ||||||||||||||
| 2.2.3 Reading | |||||||||||||||
| WARP | ND [47] | S [44] | |||||||||||||
| 2.2.4 Attention | |||||||||||||||
| IVA-CPT | ND [47] | ND [75] | |||||||||||||
| TOVA-A | ND [46] | ||||||||||||||
| TEACh | NS [41] | ||||||||||||||
| ACPT in noise | NS [80] | ||||||||||||||
| 2.2.5 Memory | |||||||||||||||
| R-AMST | ND [57,58] | ND [56] | |||||||||||||
| Auditory memory, vigilance, cognition (tests not specified) | S [54] | ||||||||||||||
| Digit Span tests | S [57] | ||||||||||||||
| AWMA | NS [41] | ||||||||||||||
| RAVLT | S [73] | ||||||||||||||
| Non-word repetition test (Persian) | S [63] | ||||||||||||||
| WISC (Digit Span) | S [63] | ||||||||||||||
| 3. NEUROPHYSIOLOGIC | |||||||||||||||
| 3.1 Brainstem auditory evoked potentials | |||||||||||||||
| Click ABR | ND [49] | ||||||||||||||
| cABR—/da/in silence | S [49] | ||||||||||||||
| cABR: /da/in silence and in ipsi white noise (+5 dB SNR) | S [69] | ||||||||||||||
| 3.2 Middle latency response | |||||||||||||||
| MLR (click) | S [70] | ||||||||||||||
| MLR (click)-BIC | S [66] | ||||||||||||||
| 3.3 Long-latency response | |||||||||||||||
| P1 latency | S [52,53] | ||||||||||||||
| P1-N1-P2-N2 (clicks) | NS [50,51] | ||||||||||||||
| P1-N1-P2-N2 (/ga/ipsi white noise.) | S [54] | ||||||||||||||
| P1-N1-P2-N2 (/da/in quiet and white noise, earphone) | S [58] | S [42] | |||||||||||||
| P1-N1-P2-N2 (/da/in quiet and white noise, loudspeaker) | ND [75] | ||||||||||||||
| LLAEP: frequent /ba/and rare /di/, bin. | S [72] | ||||||||||||||
| 4. QUESTIONNAIRES | |||||||||||||||
| 4.1 Parent | |||||||||||||||
| SAB | S [72] | ||||||||||||||
| Fisher (FAPC) | S [45,48] | ||||||||||||||
| ECA (French SAB) | ND [50] | ||||||||||||||
| MHAVIE | ND [50] | ||||||||||||||
| CHAPS | ND [41] | NS [80] | |||||||||||||
| CCC-2 | ND [41] | ||||||||||||||
| CELF-4 (pragmatic) | S [39] | ||||||||||||||
| 4.2 Child | |||||||||||||||
| LIFE-R/LIFE-UK | NS [45,48] | ND [47] | S [41,75] | ||||||||||||
| SSQ | S [46] | ||||||||||||||
| 4.3 Teacher | |||||||||||||||
| LIFE (teacher)/LIFE-UK | NS [45] | S [75] | |||||||||||||
| MHAVIE | ND [50] | ||||||||||||||
| TEAP | NS [48] | ||||||||||||||
| ECA | ND [50] NS [51] | ||||||||||||||
| SIFTER | ND [50] NS [51] | CAN [41] | |||||||||||||
| CHAPS | S [39] | NS [80] | |||||||||||||
| 4.4 Other | |||||||||||||||
| CAPD questionnaire | S [53] | ||||||||||||||
| 5. SUBJECTIVE FEEDBACK | |||||||||||||||
| NS [58] | NS [75] | NS [80] | |||||||||||||
Appendix B
| SINGLE-ABILITY AUDITORY TRAINING | |||
| Intervention Method | Reference | Description of the Intervention Methods and Name of Programs (If Applicable) | Training Schedule |
| Interaural time difference DITD: [59,74,77] DOT: [65] DAT: [78] | Barker and Bellis, 2018 [74]; Delphi et al., 2018 [65]; Mahdavi et al., 2021 [59]; Shoemaker, 2010 [77]; Stephenson, 2008 [78]. | Aim: improve DL abilities. [74] Zoo Caper Skyscraper (computer/tablet): Interactive video game played through stereo headphones. The program utilizes non-speech stimuli (animal noises), requiring participants to identify the animal. [65] DOT: Two letters or CVs are presented with 500-msec offset, which decreases as the participant achieves 80% or higher correct responses. Participants must repeat all four items in the correct order. [59] DITD: Initially uses one-digit pairs with varied onsets. Subsequent wks introduce two-pair and three-pair digits, two-word sentences and then longer sentences, all with diverse lags. The final wks focus on binaural separation, attention and auditory memory. [77] Monosyllabic words are presented dichotically. Training sessions increased in difficulty from 300 ms lead time to 0 ms lead time. [78] DAT: Each exercise contains dichotic presentations of NU-6 words, presented at different interaural timing differences. | [74] 15–20 min sessions, twice a wk, with at least 12 h between sessions. [65] 30 min sessions, 4 sessions/wk until ≤10% asymmetry at DDT. [59] 30 min sessions, 3 times/wk for 10 wks. [77] 2–45 min sessions/wk for 4 wks. 12 exercises/session. [78] 2–45 min sessions/wk for 4 wks; 12 activities/sessions. |
| Interaural intensity difference DIID: [62,65,81] | Delphi et al., 2018 [65]; Moncrieff and Wertz, 2008 [81]; Nazeri et al., 2020 [62]. | Aim: Improve DL abilities. [65] DIID: Stimuli, including consonant–vowels, sentences, or stories, are presented dichotically. Intensities are maintained for one wk as long as correct repetition is 80% or more. If performance is ≤80%, the IID is increased in 1 dB steps until the poorer ear reaches 80% accuracy. [81] Two speakers are placed on each side of the participant at a distance of 1 m. Dichotic material, including double or triple digits, words, sentences or text, is presented at 30 dB HL higher to the left ear compared to the right ear. When the participant scores 70%, intensity of the right ear is increased in 5, 2 or 1 dB steps. Activities are mostly binaural integration, but some are binaural separation. [62] DIID: The participants listen to dichotic stimuli which are presented at a higher level to the weaker ear (50 dBHL) and at a softer level to the stronger ear. The stimuli are digits. | [65] 30 min sessions, 4 sessions/wk until ≤10% asymmetry at DDT. [81] 30 min sessions, three times/wk for four wks. [62] 25–30 min, 2–3 sessions/wk for 10–12 sessions. |
| Localisation and lateralization training | Lotfi et al., 2016 [64]; Lotfi et al., 2018 [66]. | Aim: Improve spatial processing, localisation and lateralization abilities. [64,66] Consists of detecting and pointing to sound delivered with interaural time differences. Completed under headphones. A high-pass and low-pass noise with a 2 kHz cut-off point is presented through headphones and the child has to point to the perceived location of the sound source. | [64,66] 45 min/sessions, 2 sessions/wk for 6 wks. |
| SIN training with target stimuli presented from different directions | Cameron and Dillon, 2011 [46]; Cameron et al., 2012 [45]; Graydon et al., 2018 [48] | Aim: Improve spatial/binaural processing (e.g., interaural timing and intensity difference). [45,46,48] The LiSN & Learn AT software creates a three-dimensional auditory environment where a child identifies a word from a target sentence in background noise. The stimuli sound as though they are originating from various directions. The signal level is adjusted based on the participant’s responses. The training, conducted under headphones, takes place at home on a computer. | 15 min a day, 5 days a wk until completion of the 120 games (approx. 3 mos/60 sessions) [45,46] or 100 games (approx. 7 ± 3 mos) [48]. |
| Singing lessons | Koravand et al., 2019 [49]. | Aim: Improve pitch and rhythm development. [49] Lessons are collaborative with active participation from the child and instructor. The curriculum includes activities focusing on rhythmic abilities, pitch awareness and discrimination, and auditory memory. | [49] 24 lessons of 30 min, once per wk within 6 to 8 mos. |
| Musical pitch training | Tomlin and Vandali, 2019 [47]. | Aim: Improve discrimination of changes in pitch, spectral-timbre variations. [47] The aTune musical-pitch training program (modified version of aTune AT program) is computer game-based. Children match “acoustic tone patterns to visual representations of those patterns on the computer screen in a dynamic game format”. Activities are: discriminating changes in musical pitch (fundamental frequency) and spectral timbre (resonant frequency), as well as identifying pitch with spectral timbre variations and differentiating pitch and instrument type. The difficulty increases as the child progresses. | [47] At least 15 min per day, 5 times/wk (total of 10 to 12 h of training and approx. 16 wks). |
| Phonemic training | Negin et al., 2018 [61] | Aim: Improve phonemic awareness and decoding. [61] From one session to another, the child learns phonemes presented on their own and with other phonemes and in words. The child identifies the phonemes on cards. Different strategies are presented. | [61] 13 sessions, 20 to 30 min. |
| Temporal patterning training | Maggu and Yathiraj, 2010 [56]. | Aim: Improve temporal patterning and related AP abilities. [56] The training is on a computer and stimuli are presented monaurally through headphones. Stimuli are tones of 250 Hz, 1 kHz and 4 kHz, representing low, mid and high frequency signals. Tones have different duration (250 ms to 500 ms). The tasks consist of 2, 3 and 4 tone activities and increase in difficulty throughout the training. Activities comprised of discrimination and identification tasks. Scores of at least 80% are required to start the next level. | [56] 19 to 25 sessions. |
| SIN training | Brasil and Schochat, 2018 [71]; Jutras et al., 2015 [50]; Jutras et al., 2019 [51]; Loo et al., 2016 [39]; Hassaan and Ibraheem, 2016 [54]; Afshari et al., 2022 [60]; Kumar et al., 2021 [57]; Kumar et al., 2021 [58]; Maggu and Yathiraj, 2011 [55]. | Aim: Improve speech perception with background noise and noise tolerance [51,71] “Logiciel d’écoute dans le bruit” (LEB), “Programa de Escuta no Ruído” (PER is a Brazilian Portuguese version of the French Canadian LEB): Listening-in-noise software completed at home or at school, under headphones, with activities, in a babble noise, involving word discrimination, word and sentence identification, understanding directions, brain teasers, and stories. Verbal stimuli are spoken by a female or a male. Noise intensity adapts to the participant’s performance. [50] AT conducted in a clinic. This AT targets skills such as syllables or word discrimination, word identification, memorization, and understanding directions. Verbal stimuli, including syllables, words, sentences, and directives, are presented with background noise, such as babble, school conversation, city noise, and neighbourhood sounds, using a speaker connected to an audiometer and CD player. The difficulty varies with children’s responses, and when a child has at least 70% correct responses in an activity, the noise level increases by 2 dB. Each session has, on average, 3 to 4 activities. [39] Computer-based AT program at home. Activities were adaptive or fixed and comprised of speech-based listening tasks with competing sounds. Activities include discrimination, keyword extraction, speech understanding, dichotic speech listening. Noise includes theatre noise, steady-state speech-shaped noise, and competing speech. Each session has 2 tasks. [54] Semi-formal training with an examiner delivering simple material through an audiometer. A short story is presented live by the examiner with competing speech noise. The short story and the noise are presented through a speaker placed in front of the child. A new story is presented once the child can answer all the questions related to that story at a selected SNR. Each story has 5 questions with short answers. [60] The auditory spectro-temporal modulation (STM) training involves modulation identification games aimed at enhancing the encoding and detection of STMs to improve speech perception in noise. STMs are stimuli created by applying spectral and temporal modulation to broadband frequency carrier tones. In each trial, 3 sounds are presented randomly: 2 without modulation and 1 target sound with modulations. The child identifies the odd sound and the difficulty level increases gradually based on the performance. The intensity levels vary randomly to minimize intensity-related cues. Modulation depth decreases, and modulation rates increase to heighten the challenge. The training is binaural, under headphones and conducted in a quiet room. [57,58] Interactive computer-based noise desensitization training with headphones, focusing on word identification in noisy environments. Six images are displayed, and the child identifies a word presented in noise by selecting the corresponding image. The stimuli are monosyllabic and trisyllabic English words spoken by a female in speech-shaped noise or multitalker babble. SNR levels include 20, 10, 6, 4, 2, 0, −2, and −4 dB SNR. The SNR decreases as the child progresses (scores 80% or better in the current level). [55] Children are presented with 15 recorded English texts (80 to 100 words), accompanied by various noises at different SNR (+15 dB to 0 dB). The noises include fan noise, speech noise and babble (8 speakers). The material is presented binaurally and with a laptop. Four questions related to the text are posed to the children without background noise. A level was considered completed when the child answered three out of four questions correctly. A total of 35 to 60 texts were presented to the children. Authors did not specify if the training was performed with headphones or speakerphones. | [51] Two 30 min sessions per wk for 13 wks; [71] 12 wkly sessions of 50 min. [50] 60 min sessions, twice a wk for 9 wks. Total of 1080 h of intervention. [39] 30 min sessions, 5-day/wk for 3 mos. [54] 2–20 to 30 min sessions/wk for 8 wks. [60] 1 h sessions twice a wk for five wks. [57,58] 30 min/day 3 to 4 days a wk, until the child has completed the last level (total of 10 to 16 sessions). (28, 29) [55] 25 to 30 min sessions daily for 15 to 20 sessions. |
| MULTIPLE-ABILITIES AUDITORY TRAINING | |||
| Intervention method | Reference | Description of the intervention methods and names of programs (if applicable) | Training schedule |
| Temporal processing and phonemic awareness training | Ahmed et al., 2016 [52]; Oraky et al., 2017 [53] | Aim: Improving temporal processing and phonemic awareness abilities. [52,53] Formal training involves computer games designed for training temporal processing and phonemic awareness abilities. Informal training, guided by a therapist, emphasizes phonemic awareness and auditory directives. Both training forms were developed and standardized for Arabic-speaking children. | [52,53] 2 mos |
| DL, temporal processing, AFG/SIN training | Donadon et al., 2019 [68]; Filipini et al., 2012 [69] | Aim: Improve DL, temporal processing, and AFG/SIN. [68] AT under headphones, in an acoustic booth and through the Afinando o Cérebro website. Four exercises are performed every session. Activities focus on auditory processing skills, such as binaural integration, temporal resolution and ordering, as well as figure-ground. Activities are completed when the score is at least 80%. [69] AT completed in a sound booth through an audiometer and with an audiologist. Activities comprise competitive speech perception, SIN, dichotic speech perception, and frequency and duration patterns of discrimination and sequencing. Difficulty level is increased when answers are 70% correct. | [68] 40 to 45 min sessions once a wk for 8 wks. [69] 50 min sessions once a wk for 8 wks. |
| DL, temporal processing, AFG/SIN, localization training | Schochat et al., 2010 [70]; De Melo et al., 2018 [72] | Aim: Improve DL, temporal processing, AFG/SIN and localization. [70] The training comprises multiple components. Frequency training: Involves discriminating tones (same or different, labeling, relaying correct sequences). Intensity training: Involves activities similar to those of frequency training. Temporal training: Incorporates activities from frequency and intensity training, specifically emphasizing duration of tones and gap detection. DIID. Localization and speech perception: Involves presenting speech signals (words) and competing signals (babble or white noise) from different positions. [72] Computerized AT (called Escuta Activa). Stimuli are presented under headphones. Skills trained are: AFG skills, integration and binaural separation, temporal resolution, temporal standardization, localization and auditory discrimination. One activity is completed each session. | [70] Formal training: 50 min sessions every wk for 8 wks. [72] 30 min sessions, twice a wk for 12 wks. |
| ASSISTIVE DEVICES | |||
| Intervention method | Reference | Description of the intervention methods | Schedule |
| Personal FM System | Stavrinos et al., 2020 and Stavrinos, 2019 [41]; Umat et al., 2011 [73]; Smart et al., 2018 [75]; Reynolds et al., 2013 [79] | Aim: Improving acoustic signals and speech perception in class. [41] Remote microphone hearing aids (RMHA) are a wireless listening system. The speaker wears a microphone and the children wear ear receivers. Fitting of RMHAs is binaural with non-occluding open-ear domes. The teacher wears a microphone on a non-adjustable lanyard. Used only in lecture-based subjects at school. Connection range between the microphone and receivers was within 7–25 m. [73] Personal FM system used at school. Fitting was either monaural in the right ear or binaural. [75] Bilateral open-fitted personal FM receivers and transmitter (i.e., lapel microphone with directional and omnidirectional capabilities). Receivers have a volume control range of 0 to 15 dB and are set at the middle position. FM systems are only worn at school during English, math, science, and social studies classes. [79] In all studies: Personal FM devices, fitted binaurally. Device was used at school (for one study, use was encouraged at home also). Some studies reported regular monitoring. | [41] 5 days/wk for 3–6 mos. [73] 4–5 h per day for 12 wks. [75] 20 wks. [79] 4 wks to 8 mos, daily (4–6 h/day; 1–5 h/day; 45 min/day). |
| HEARING AIDS | |||
| Intervention method | Reference | Description of the intervention methods | Schedule |
| Fitting of binaural hearing aids | Kuk et al., 2008 [80]. | Aim: Improving acoustic signals and speech perception in class and at home. [80] Children are fitted with bilateral, mild-gain (approx. 10 dB insertion gain), behind-the-ear, wide dynamic range compression hearing aids fitted in an open-ear mode. Directional microphone and noise reduction are activated and children can switch between omnidirectional and directional microphones. | [80] At school and at home. |
| TOP-DOWN TRAINING | |||
| Intervention Method | Reference | Description of the intervention methods | Schedule |
| TDT (working memory) | Moossavi et al., 2015 [63]. | Aim: Improving auditory working memory and SIN abilities. [63] This formal TDT centers on improving auditory working memory, emphasizing a rehearsal strategy. Participants listen to a list of digits or words coming from various locations and must repeat the list. As new digits or words are introduced, participants restart the list from the beginning. The difficulty level for each session is dynamically adjusted based on the child’s performance, maintaining a target score of 70% correct. | [63] 12 training sessions of 45 min each, twice a wk. |
| MULTIMODAL TRAINING | |||
| Intervention method | Reference | Description of the intervention methods and name of programs (if applicable) | Training schedule |
| FM System, classroom modification and adaptation, AT, TDT. | Bellis and Anzalone, 2008 [76]. | Aim: Improving auditory processing abilities, top-down abilities and listening environment. [76] Modifications of classroom environment and preferential seating; teacher accommodation strategies, such as using visual cues and pre-teaching new vocabulary; use of a personal FM system and clear speech by parents and teachers; central resources training (active listening techniques and problem solving); attribution training (teaching the child to take responsibility of their own listening success); AT; Earobics. TDT included: auditory closure activities, using stimuli in which words, syllables, or phonemes were removed, context-based vocabulary building. AT: speech–sound discrimination (consonant–vowel syllables and words with minimal pair contrasts) and basic phonological awareness. | [76] Earobics: 30 min a day, for 5 days and for 6 wks. |
| FM System, TDT and BUT | Sharma et al., 2014 [42]; Sharma et al., 2012 [44]. | Aim: Improving discrimination, temporal processing, phonemic awareness, language abilities and listening environment. [42,44] Sessions were individual and had two to three activities repeated twice over the course of the intervention. BUT included adaptive listening tasks and computer-based activities focused on gap detection, frequency discrimination, intensity discrimination and phonological awareness (Earobics). TDT included language activities, such as reading aloud, imitating stress patterns in words and intonation within sentences, following directions, scrambled sentences, circumlocution, building stories, identification of key words. Homework focused on the skills introduced during the session. FM groups were fitted bilaterally with Edulinks FM units (Phonak) and Campus S transmitter worn with a lapel microphone. | [42,44] 12 h of intervention in total. One-hour session every wk for six wks and 15 min homework for five days each wk. |
| FM system, BUT and TDT | Putter-Katz et al., 2008 [67]. | Aim: Improving auditory processing abilities, top-down abilities and listening environment. [67] BUT comprises AT and enhancement of acoustic signals and listening environment with the use of FM system. Activities comprised listening to speech in noise or competing verbal stimuli, and selective and divided attention tasks. TDT includes learning coping strategies, auditory closure, speech-reading, metacognitive awareness, learning strategies at schools and home accommodations. Sessions are built so that activities are progressively more difficult. | [67] 45 min sessions per wk for 4 mos (13 to 15 sessions) |
| DL, temporal and binaural processing, SIN, language abilities training | Schochat and Alonso, 2009 [98] in Wilson et al., 2013 [43] | Aim: Improve DL, temporal processing, SIN, binaural processing, and language abilities. [43,98] Activities comprise discrimination, sequencing and labelling for frequency, intensity and duration; dichotic intensity differences; sound localisation; speech perception; and language-based informal training by the parents. | [43,98] 50 min/day, 1 day/wk, over 8 wks |
References
- Gheller, F.; Lovo, E.; Arsie, A.; Bovo, R. Classroom acoustics: Listening problems in children. Build. Acoust. 2020, 27, 47–59. [Google Scholar] [CrossRef]
- Purdy, S.C.; Sharma, M.; Morgan, A. Measuring Perceptions of Classroom Listening in Typically Developing Children and Children with Auditory Difficulties Using the LIFE-UK Questionnaire. J. Am. Acad. Audiol. 2018, 29, 656–667. [Google Scholar] [CrossRef] [PubMed]
- Howard, C.S.; Munro, K.J.; Plack, C.J. Listening effort at signal-to-noise ratios that are typical of the school classroom. Int. J. Audiol. 2010, 49, 928–932. [Google Scholar] [CrossRef] [PubMed]
- Prodi, N.; Visentin, C.; Peretti, A.; Griguolo, J.; Bartolucci, G.B. Investigating Listening Effort in Classrooms for 5- to 7-Year-Old Children. Lang. Speech Hear. Serv. Sch. 2019, 50, 196–210. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, M.A.; Hall, R.L.; Riley, A.; Moore, D.R. Communication, listening, cognitive and speech perception skills in children with auditory processing disorder (apd) or specific language impairment (sli). J. Speech Lang. Hear. Res. 2011, 54, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Purdy, S.C.; Kelly, A.S. Comorbidity of Auditory Processing, Language, and Reading Disorders. J. Speech Lang. Hear. Res. 2009, 52, 706–722. [Google Scholar] [CrossRef] [PubMed]
- Witton, C. Childhood auditory processing disorder as a developmental disorder: The case for a multi-professional approach to diagnosis and management. Int. J. Audiol. 2010, 49, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Dillon, H.; Cameron, S. Separating the Causes of Listening Difficulties in Children. Ear Hear. 2021, 42, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.G.; Tomlin, D.; Moore, D.R.; Dillon, H. Use of Questionnaire-Based Measures in the Assessment of Listening Difficulties in School-Aged Children. Ear Hear. 2015, 36, e300–e313. [Google Scholar] [CrossRef]
- Iliadou, V.; Ptok, M.; Grech, H.; Pedersen, E.R.; Brechmann, A.; Deggouj, N.; Kiese-Himmelel, C.; Śliwińska-Kowalska, M.; Nickisch, A.; Demanez, L.; et al. A European Perspective on Auditory Processing Disorder-Current Knowledge and Future Research Focus. Front. Neurol. 2017, 8, 622. [Google Scholar] [CrossRef]
- Christmann, C.A.; Lachmann, T.; Steinbrink, C. Evidence for a General Auditory Processing Deficit in Developmental Dyslexia From a Discrimination Paradigm Using Speech Versus Nonspeech Sounds Matched in Complexity. J. Speech Lang. Hear. Res. 2015, 58, 107–121. [Google Scholar] [CrossRef]
- Tomlin, D.; Dillon, H.; Sharma, M.; Rance, G. The Impact of Auditory Processing and Cognitive Abilities in Children. Ear Hear. 2015, 36, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Ferguson, M.A.; Edmondson-Jones, A.M.; Ratib, S.; Riley, A. Nature of Auditory Processing Disorder in Children. Pediatrics 2010, 126, e382–e390. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R. Listening difficulties in children: Bottom-up and top-down contributions. J. Commun. Disord. 2012, 45, 411–418. [Google Scholar] [CrossRef]
- CISGSLPA. Canadian Guidelines on Auditory Processing Disorder in Children and Adults: Assessment and Intervention; Canadian Interorganizational Steering Group for Speech-Language Pathology and Audiology: Ottawa, ON, Canada, 2012. [Google Scholar]
- Wilson, W.J. Evolving the concept of APD. Int. J. Audiol. 2018, 57, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Rosen, S.; Bamiou, D.-E.; Campbell, N.G.; Sirimanna, T. Evolving concepts of developmental auditory processing disorder (APD): A British Society of Audiology APD Special Interest Group ‘white paper’. Int. J. Audiol. 2012, 52, 3–13. [Google Scholar] [CrossRef] [PubMed]
- ASHA. Central Auditory Processing Disorder. American Speech-Language-Hearing Association. Available online: https://www.asha.org/practice-portal/clinical-topics/central-auditory-processing-disorder/#:~:text=ASHA%20(2005)%20uses%20the%20term,sound%20localization%20and%20lateralization (accessed on 2 December 2023).
- Bellis, T.J. The Nature of Central Auditory Processing Disorder. In Handbook of Central Auditory Processing Disorder. Auditory Neuroscience and Diagnosis, 2nd ed.; Plural Publishing Inc.: San Diego, CA, USA, 2014; Volumes 1–2, pp. 211–230. [Google Scholar]
- de Wit, E.; van Dijk, P.; Hanekamp, S.; Visser-Bochane, M.I.; Steenbergen, B.; van der Schans, C.P.; Luinge, M.R. Same or Different: The Overlap Between Children With Auditory Processing Disorders and Children With Other Developmental Disorders: A Systematic Review. Ear Hear. 2018, 39, 1–19. [Google Scholar] [CrossRef] [PubMed]
- AAA. Guidelines for the Diagnosis, Treatment and Management of Children and Adults with Central Auditory Processing Disorder. American Academy of Audiology, 2010. Available online: https://audiology-web.s3.amazonaws.com/migrated/CAPD%20Guidelines%208-2010.pdf_539952af956c79.73897613.pdf (accessed on 5 December 2023).
- BSA. Practice Guidance, An Overview of Current Management of Auditory Processing Disorder (APD). British Society of Audiology, 2011. Available online: https://www.thebsa.org.uk/wp-content/uploads/2023/10/Current-APD-Management-2.pdf (accessed on 5 December 2023).
- World Health Organization. Towards a Common Language for Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Bamiou, D.-E.; Campbell, N.; Sirimanna, T. Management of auditory processing disorders. Audiol. Med. 2006, 4, 46–56. [Google Scholar] [CrossRef]
- Fey, M.E.; Richard, G.J.; Geffner, D.; Kamhi, A.G.; Medwetsky, L.; Paul, D.; Ross-Swain, D.; Wallach, G.P.; Frymark, T.; Schooling, T. Auditory Processing Disorder and Auditory/Language Interventions: An Evidence-Based Systematic Review. Lang. Speech Hear. Serv. Sch. 2011, 42, 246–264. [Google Scholar] [CrossRef]
- Bellis, T.J.; Chermak, G.D.; Weihing, J.; Musiek, F.E.; Nippold, M.; Schwarz, I. Efficacy of Auditory Interventions for Central Auditory Processing Disorder: A Response to Fey et al. (2011)...‘Auditory Processing Disorder and Auditory/Language Interventions: An Evidence-Based Systematic Review’ by Fey et al. (2011). Lang. Speech Hear. Serv. Sch. 2012, 43, 381–386. [Google Scholar] [CrossRef]
- Fey, M.E.; Kamhi, A.G.; Richard, G.J.; Nippold, M.; Schwarz, I. Auditory Training for Children with Auditory Processing Disorder and Language Impairment: A Response to Bellis, Chermak, Weihing, and Musiek...‘Auditory Processing Disorder and Auditory/Language Interventions: An Evidence-Based Systematic Review’ by Fey et al. (2011). Lang. Speech Hear. Serv. Sch. 2012, 43, 387–392. [Google Scholar] [PubMed]
- Chermak, G.D.; Musiek, F.E.; Weihing, J. Auditory Training for Central Auditory Processing Disorder. Semin. Hear. 2015, 36, 199–215. [Google Scholar] [CrossRef]
- Gohari, N.; Dastgerdi, Z.H.; Rouhbakhsh, N.; Afshar, S.; Mobini, R. Training Programs for Improving Speech Perception in Noise: A Review. J. Audiol. Otol. 2023, 27, 1–9. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Canadian Agency for Drugs and Technologies in Health. Grey Matters: A Practical Tool for Searching Health-Related Grey Literature. Available online: https://greymatters.cadth.ca/ (accessed on 3 June 2021).
- Covidence. Melbourne: Veritas Health Innovation. Covidence Systematic Review Software. 28 June 2022. Available online: https://www.covidence.org/ (accessed on 13 October 2021).
- Peterson, P. Promoting generalization and maintenance of skills learned via natural language teaching. J. Speech Lang. Pathol. Appl. Behav. Anal. 2009, 4, 90–131. [Google Scholar] [CrossRef]
- Krasny-Pacini, A.; Evans, J. Single-case experimental designs to assess intervention effectiveness in rehabilitation: A practical guide. Ann. Phys. Rehabil. Med. 2018, 61, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Weihing, J.; Chermak, G.D.; Musiek, F.E.; Bellis, T.J. The efficacy of auditory training in children and adults with central auditory processing deficits. In Handbook of Central Auditory Processing Disorder: Comprehensive Intervention, Volume II, 2nd ed.; Plural Publishing: San Diego, CA, USA, 2010. [Google Scholar]
- Chermak, G.D. Central Resources Training: Cognitive, Metacognitive, and Metalinguistic Skills and Strategies. In Handbook of Central Auditory Processing Disorder: Comprehensive Intervention, 2nd ed.; Plural Publishing Inc.: San Diego, CA, USA, 2014; Volume II, pp. 243–309. [Google Scholar]
- Loo, H.Y.J. Management of Children with Auditory Processing Disorder; University of London, University College London (United Kingdom): London, UK, 2012; Available online: https://login.proxy.bib.uottawa.ca/login?url=https://www.proquest.com/dissertations-theses/management-children-with-auditory-processing/docview/1512406809/se-2?accountid=14701 (accessed on 6 August 2021).
- Loo, J.H.Y.; Rosen, S.; Bamiou, D.-E. Auditory Training Effects on the Listening Skills of Children With Auditory Processing Disorder. Ear Hear. 2016, 37, 38–47. [Google Scholar] [CrossRef]
- Stavrinos, G. Effects of Remote Microphone Hearing Aids (RMHAs) on Listening-in-Noise, Attention and Memory in School-Aged Children with A; University of London, University College London (United Kingdom): London, UK, 2019; Available online: https://login.proxy.bib.uottawa.ca/login?url=https://www.proquest.com/dissertations-theses/effects-remote-microphone-hearing-aids-rmhas-on/docview/2307392189/se-2?accountid=14701 (accessed on 6 August 2021).
- Stavrinos, G.; Iliadou, V.; Pavlou, M.; Bamiou, D.-E. Remote Microphone Hearing Aid Use Improves Classroom Listening, Without Adverse Effects on Spatial Listening and Attention Skills, in Children With Auditory Processing Disorder: A Randomised Controlled Trial. Front. Neurosci. 2020, 14, 904. [Google Scholar] [CrossRef]
- Sharma, M.; Purdy, S.C.; Kelly, A.S. The Contribution of Speech-Evoked Cortical Auditory Evoked Potentials to the Diagnosis and Measurement of Intervention Outcomes in Children with Auditory Processing Disorder. Semin. Hear. 2014, 35, 051–064. [Google Scholar] [CrossRef]
- Wilson, W.J.; Arnott, W.; Henning, C. A systematic review of electrophysiological outcomes following auditory training in school-age children with auditory processing deficits. Int. J. Audiol. 2013, 52, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Purdy, S.C.; Kelly, A.S. A randomized control trial of interventions in school-aged children with auditory processing disorders. Int. J. Audiol. 2012, 51, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.; Glyde, H.; Dillon, H. Efficacy of the LiSN & Learn Auditory Training Software: Randomized Blinded Controlled Study. Audiol. Res. 2012, 2, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.; Dillon, H. Development and Evaluation of the LiSN & Learn Auditory Training Software for Deficit-Specific Remediation of Binaural Processing Deficits in Children: Preliminary Findings. J. Am. Acad. Audiol. 2011, 22, 678–696. [Google Scholar] [CrossRef] [PubMed]
- Tomlin, D.; Vandali, A. Efficacy of a deficit specific auditory training program for remediation of temporal patterning deficits. Int. J. Audiol. 2019, 58, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Graydon, K.; Van Dun, B.; Tomlin, D.; Dowell, R.; Rance, G. Remediation of spatial processing disorder (SPD). Int. J. Audiol. 2018, 57, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Koravand, A.; Parkes, E.; Duquette-Laplante, F.; Bursch, C.; Tomaszewski, S. The effects of singing lessons on speech evoked brainstem responses in children with central auditory processing disorders. Can. Acoust.-Acoust. Can. 2019, 47, 31–40. [Google Scholar]
- Jutras, B.; Owliaey, M.; Gagnon, M.; Phoenix, C. Impact de l’entraînement auditif sur les habiletés d’écoute dans le bruit des enfants ayant un trouble de traitement auditif: Résultats d’une étude pilote. Can. J. Speech-Lang. Pathol. Audiol. 2015, 39, 346–361. [Google Scholar]
- Jutras, B.; Lafontaine, L.; East, M.-P.; Noël, M. Listening in noise training in children with auditory processing disorder: Exploring group and individual data. Disabil. Rehabil. 2019, 41, 2918–2926. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Tawfik, S.M.; Bakr, M.S.; Abdelhaleem, E.K.; Mohamed, E.S. Remediation of central auditory processing disorders in children with learning disability: A comparative study. J. Curr. Med. Res. Pract. 2016, 1, 86. [Google Scholar] [CrossRef]
- Oraky, S.M.; Tawfik, S.; Salama, M.; Mohamed, E.S. Comparing outcome of formal and informal remediation programs in children with central auditory processing disorder. Egypt. J. Otolaryngol. 2017, 33, 502–507. [Google Scholar] [CrossRef]
- Hassaan, M.R.; Ibraheem, O.A. Auditory training program for Arabic-speaking children with auditory figure-ground deficits. Int. J. Pediatr. Otorhinolaryngol. 2016, 83, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Maggu, A.R.; Yathiraj, A. Effect of Noise Desensitization Training on Children with Poor Speech-In-Noise Scores. Can. J. Speech-Lang. Pathol. Audiol. 2011, 35, 56–63. [Google Scholar]
- Maggu, A.; Yathiraj, A. Effect of Temporal Pattern Training on Specific Central Auditory Processes. Master’s Dissertation, AIISH, Mysore, India, 2011; p. 11. [Google Scholar]
- Kumar, P.; Singh, N.K.; Hussain, R.O. Effect of speech in noise training in the auditory and cognitive skills in children with auditory processing disorders. Int. J. Pediatr. Otorhinolaryngol. 2021, 146, 110735. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Singh, N.K.; Hussain, R.O. Efficacy of Computer-Based Noise Desensitization Training in Children With Speech-in-Noise Deficits. Am. J. Audiol. 2021, 30, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Mahdavi, M.E.; Rezaeian, M.; Zarrinkoob, H.; Rezaeian, M.; Akbarzadeh, A. Effect of a Dichotic Interaural Time Difference Program on Dichotic Listening Deficit of Children with Learning Difficulty. J. Am. Acad. Audiol. 2021, 32, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Afshari, P.J.; Lotfi, Y.; Moossavi, A.; Bakhshi, E.; Sadjedi, H. Auditory Spectro-Temporal Modulation Training in Children With Auditory Processing Disorder. Iran. Rehabil. J. 2022, 20, 185–198. [Google Scholar] [CrossRef]
- Negin, E.; Mohammadkhani, G.; Jalaie, S.; Jarollahi, F. Efficacy of phonemic training program in rehabilitation of Persian-speaking children with auditory processing disorder: A single subject study. Audit. Vestib. Res. 2018, 27, 116–125. [Google Scholar] [CrossRef]
- Nazeri, A.; Bagheri, H.; Baghban, A.A.; Negin, E. Comparison of Persian staggered spondaic word test’s scores before and after rehabilitation in children with amblyaudia. Audit. Vestib. Res. 2020, 29, 165–171. [Google Scholar] [CrossRef]
- Moossavi, A.; Mehrkian, S.; Lotfi, Y.; Faghihzadeh, S.; Sadjedi, H. The effect of working memory training on auditory stream segregation in auditory processing disorders children. Iran. Rehabil. J. 2015, 13, 22–27. [Google Scholar]
- Lotfi, Y.; Moosavi, A.; Abdollahi, F.Z.; Bakhshi, E.; Sadjedi, H. Effects of an Auditory Lateralization Training in Children Suspected to Central Auditory Processing Disorder. J. Audiol. Otol. 2016, 20, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Delphi, M.; Abdollahi, F.Z. Dichotic training in children with auditory processing disorder. Int. J. Pediatr. Otorhinolaryngol. 2018, 110, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, Y.; Moosavi, A.; Abdollahi, F.Z.; Bakhshi, E. Auditory Lateralization Training Effects on Binaural Interaction Component of Middle Latency Response in Children Suspected to Central Auditory Processing Disorder. Indian J. Otolaryngol. Head Neck Surg. 2018, 71, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Putter-Katz, H.; Adi-Bensaid, L.; Feldman, I.; Hildesheimer, M. Effects of Speech in Noise and Dichotic Listening Intervention Programs on Central Auditory Processing Disorders. J. Basic Clin. Physiol. Pharmacol. 2008, 19, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Donadon, C.; Sanfins, M.D.; Borges, L.R.; Colella-Santos, M.F. Auditory training: Effects on auditory abilities in children with history of otitis media. Int. J. Pediatr. Otorhinolaryngol. 2019, 118, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Filippini, R.; Befi-Lopes, D.M.; Schochat, E. Efficacy of Auditory Training Using the Auditory Brainstem Response to Complex Sounds: Auditory Processing Disorder and Specific Language Impairment. Folia Phoniatr. Logop. 2011, 64, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Schochat, E.; Musiek, F.; Alonso, R.; Ogata, J. Effect of auditory training on the middle latency response in children with (central) auditory processing disorder. Braz. J. Med. Biol. Res. 2010, 43, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Brasil, P.D.; Schochat, E. Eficácia do treinamento auditivo utilizando o software Programa de Escuta no Ruído (PER) em escolares com transtorno do processamento auditivo e baixo desempenho escolar. CoDAS 2018, 30, e20170227. [Google Scholar] [CrossRef] [PubMed]
- De Melo, Â.; Mezzomo, C.L.; Garcia, M.V.; Biaggio, E.P.V. Computerized Auditory Training in Students: Electrophysiological and Subjective Analysis of Therapeutic Effectiveness. Int. Arch. Otorhinolaryngol. 2018, 22, 23–32. [Google Scholar] [CrossRef]
- Umat, C.; Mukari, S.Z.; Ezan, N.F.; Din, N.C. Changes in auditory memory performance following the use of frequency-modulated system in children with suspected auditory processing disorders. Saudi Med. J. 2011, 32, 818–824. [Google Scholar]
- Barker, M.D.; Bellis, T.J. Effectiveness of a Novel Computer/Tablet-Based Auditory Training Program in Improving Dichotic Listening Skills in Children. J. Speech Pathol. Ther. 2018, 3, 129. [Google Scholar] [CrossRef]
- Smart, J.L.; Purdy, S.C.; Kelly, A.S. Impact of Personal Frequency Modulation Systems on Behavioral and Cortical Auditory Evoked Potential Measures of Auditory Processing and Classroom Listening in School-Aged Children with Auditory Processing Disorder. J. Am. Acad. Audiol. 2018, 29, 568–586. [Google Scholar] [CrossRef] [PubMed]
- Bellis, T.J.; Anzalone, A.M. Intervention Approaches for Individuals With (Central) Auditory Processing Disorder. Contemp. Issues Commun. Sci. Disord. 2008, 35, 143–153. [Google Scholar] [CrossRef]
- Shoemaker, S.S. The Impact of Dichotic Auditory Training in Children. Diss. Abstr. Int. Sect. B Sci. Eng. 2010, 71, 3567. [Google Scholar]
- Stephenson, K.E. Effects of dichotic auditory training on children with central auditory processing disorder. Diss. Abstr. Int. Sect. B Sci. Eng. 2008, 69, 1542. [Google Scholar]
- Reynolds, S.; Kuhaneck, H.M.; Pfeiffer, B. Systematic Review of the Effectiveness of Frequency Modulation Devices in Improving Academic Outcomes in Children with Auditory Processing Difficulties. Am. J. Occup. Ther. 2016, 70, 7001220030p1–7001220030p11. [Google Scholar] [CrossRef] [PubMed]
- Kuk, F.; Jackson, A.; Keenan, D.; Lau, C.-C. Personal Amplification for School-Age Children with Auditory Processing Disorders. J. Am. Acad. Audiol. 2008, 19, 465–480. [Google Scholar] [CrossRef] [PubMed]
- Moncrieff, D.W.; Wertz, D. Auditory rehabilitation for interaural asymmetry: Preliminary evidence of improved dichotic listening performance following intensive training. Int. J. Audiol. 2008, 47, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Tomlin, D.; Rance, G. Maturation of the Central Auditory Nervous System in Children with Auditory Processing Disorder. Semin. Hear. 2016, 37, 074–083. [Google Scholar] [CrossRef]
- Hayes, E.A.; Warrier, C.M.; Nicol, T.G.; Zecker, S.G.; Kraus, N. Neural plasticity following auditory training in children with learning problems. Clin. Neurophysiol. 2003, 114, 673–684. [Google Scholar] [CrossRef]
- Earobics Step 1 [CD-ROM]. Cognitive Concepts; Houghton Mifflin Harcourt: Boston, MA, USA, 2008. [Google Scholar]
- Vandali, A.; Sly, D.; Cowan, R.; van Hoesel, R. Training of Cochlear Implant Users to Improve Pitch Perception in the Presence of Competing Place Cues. Ear Hear. 2015, 36, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- Jutras, B.; Lafontaine, L. Logiciel d’écoute dans le bruit (LEB). Montréal, QC, Canada. Available online: http://monleb.com/ (accessed on 6 January 2024).
- Calarga, K.S. Tradução e Adaptação de um Software de Treinamento Auditivo para Escolares [Dissertação]. Master’s Thesis in Sciences, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil, 2016. [Google Scholar]
- Cognitive Concepts. Earobics [Computer Software]; Cognitive Concepts: Evanston, IL, USA, 1998; Available online: https://archive.org/details/Earobics_Step_2_Cognitive_Concepts_1998 (accessed on 6 January 2024).
- Liu, P.; Zhu, H.; Chen, M.; Hong, Q.; Chi, X. Electrophysiological Screening for Children With Suspected Auditory Processing Disorder: A Systematic Review. Front. Neurol. 2021, 12, 692840. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, T.S.; Lind, O.; Follestad, T.; Grøndahl, K.; Wilson, W.; Nicholas, J.; Nordgård, S.; Andersson, S. Electrophysiological characteristics in children with listening difficulties, with or without auditory processing disorder. Int. J. Audiol. 2019, 58, 704–716. [Google Scholar] [CrossRef] [PubMed]
- MacDermid, J.C.; Law, M.; Michlovitz, S.L. Outcome Measurement in Evidence-Based Rehabilitation. In Evidence-Based Rehabilitation: A Guide to Practice, 3rd ed.; Slack Incorporated: Thorofare, NJ, USA, 2014; pp. 65–104. [Google Scholar]
- Mattsson, T.S.; Follestad, T.; Andersson, S.; Lind, O.; Øygarden, J.; Nordgård, S. Normative data for diagnosing auditory processing disorder in Norwegian children aged 7–12 years. Int. J. Audiol. 2017, 57, 10–20. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.; Terwee, C.; de Vet, H. Key concepts in clinical epidemiology: Responsiveness, the longitudinal aspect of validity. J. Clin. Epidemiol. 2021, 140, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Crosby, R.D.; Kolotkin, R.L.; Williams, G.R. Defining clinically meaningful change in health-related quality of life. J. Clin. Epidemiol. 2003, 56, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Sturgess, J.; Rodger, S.; Ozanne, A. A Review of the Use of Self-Report Assessment with Young Children. Br. J. Occup. Ther. 2002, 65, 108–116. [Google Scholar] [CrossRef]
- Law, M.C.; Baptiste, S.; Carswell, A.; McColl, M.A.; Polatajko, H.J.; Pollock, N. Canadian Occupational Performance Measure, 5th ed. Revised; COPM: Ottawa, ON, Canada, 2019. [Google Scholar]
- Alonso, R.; Schochat, E. The efficacy of formal auditory training in children with (central) auditory processing disorder: Behavioral and electrophysiological evaluation. Braz. J. Otorhinolaryngol. 2009, 75, 726–732. [Google Scholar]
| # | Search Terms and Key Words |
|---|---|
| 1 | exp auditory perceptual disorders/ |
| 2 | (auditory adj4 perceptual adj4 (problem* or difficult* or disorder* or disease*)).ti,ab. |
| 3 | (speech adj4 noise adj4 (problem* or difficult*)).ti,ab. |
| 4 | (listening adj4 noise adj4 (problem* or difficult*)).ti,ab. |
| 5 | (Spatial adj4 processing adj4 (problem* or difficult* or disorder* or disease*)).ti,ab. |
| 6 | (auditory adj4 processing adj4 (problem* or difficult* or disorder*)).ti,ab. |
| 7 | (hearing adj4 noise adj4 (problem* or difficult*)).ti,ab. |
| 8 | 1 or 2 or 3 or 4 or 5 or 6 or 7 |
| 9 | exp Child/ |
| 10 | (child* or kid or kids or girl or girls or boy or boys or youth* or youngster* or kindergarten* or school* or minors or p?ediatric*).ti,ab. |
| 11 | limit 8 to “child (6 to 12 years)” |
| 12 | 9 or 10 or 11 |
| 13 | 8 and 12 |
| 14 | limit 13 to (yr = “2006 -Current” and English) |
| 15 | limit 13 to (yr = “2006 -Current” and French) |
| 16 | 14 OR 15 |
| 17 | 16 NOT (autis*).ti,ab. |
| Reference | |
|---|---|
| Country of study | |
| Australia | [42,43,44,45,46,47,48] |
| Canada | [49,50,51] |
| Egypt | [52,53,54] |
| India | [55,56,57,58] |
| Iran | [59,60,61,62,63,64,65,66] |
| Israel | [67] |
| Brazil | [68,69,70,71,72] |
| Malaysia | [73] |
| New Zealand | [74,75] |
| United Kingdom | [40,41] |
| United States of America | [76,77,78,79,80,81] |
| Singapore | [38,39] |
| Design | |
| 1. Pre–post studies | [46,47,48,49,50,51,52,53,54,57,59,62,67,70,71,72,73,74,75,77,78,80,81] |
| 1.1 Repeated baseline self-control measures | [47,48,71,74,75] |
| 1.2 Control group (no intervention) | [50,51,57,67,73,77] |
| 1.3 Control group (with intervention) | [52,53,70,72,77] |
| 1.4 Control group (neurotypical children) | [70] |
| 1.5 Long-term assessment (three months to one year) | [46,47,48,50,51,73,81] |
| 2. Randomized controlled trials (RCTs) | [38,39,40,41,42,44,45,55,56,58,60,64,65,66,68] |
| 2.1 Control group (no intervention) | [40,41,55,56,58,60,64,66] |
| 2.2 Control group (with intervention) | [38,39,42,44,45,65,68] |
| 2.3 Control group (neurotypical children) | [42] |
| 2.4 Long-term assessment (two weeks to three months) | [38,39,56,60,65] |
| 3. Non-randomized experimental study (Two control groups: with comparative intervention and neurotypical children) | [69] |
| 4. Non-randomized case-controlled trial (Control group: no intervention) | [63] |
| 5. Case report | [76] |
| 6. Single-subject design | [61] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bigras, J.; Lagacé, J.; El Mawazini, A.; Lessard-Dostie, H. Interventions for School-Aged Children with Auditory Processing Disorder: A Scoping Review. Healthcare 2024, 12, 1161. https://doi.org/10.3390/healthcare12121161
Bigras J, Lagacé J, El Mawazini A, Lessard-Dostie H. Interventions for School-Aged Children with Auditory Processing Disorder: A Scoping Review. Healthcare. 2024; 12(12):1161. https://doi.org/10.3390/healthcare12121161
Chicago/Turabian StyleBigras, Jacynthe, Josée Lagacé, Ahmed El Mawazini, and Héloïse Lessard-Dostie. 2024. "Interventions for School-Aged Children with Auditory Processing Disorder: A Scoping Review" Healthcare 12, no. 12: 1161. https://doi.org/10.3390/healthcare12121161
APA StyleBigras, J., Lagacé, J., El Mawazini, A., & Lessard-Dostie, H. (2024). Interventions for School-Aged Children with Auditory Processing Disorder: A Scoping Review. Healthcare, 12(12), 1161. https://doi.org/10.3390/healthcare12121161