
Comparing Actual and Rounded Serum Creatinine Concentration for Assessing the Accuracy of Vancomycin Dosing in Elderly Patients: A Single-Center Retrospective Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Place, and Setting
2.2. Criteria of Inclusion and Exclusion
2.3. Study Equations and Definitions
2.4. Endpoints
2.4.1. Primary Endpoints
- To determine the percentage of patients who achieved therapeutic vancomycin trough levels using the actual SCr.
- To predict the performance of vancomycin doses based on actual and rounded SCr to TMD using the following measuring tools: correlation, bias, precision, error, and accuracy.
2.4.2. Secondary Endpoints
- To evaluate the incidence of vancomycin-associated nephrotoxicity (VAN).
- To evaluate the risk factors of VAN.
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
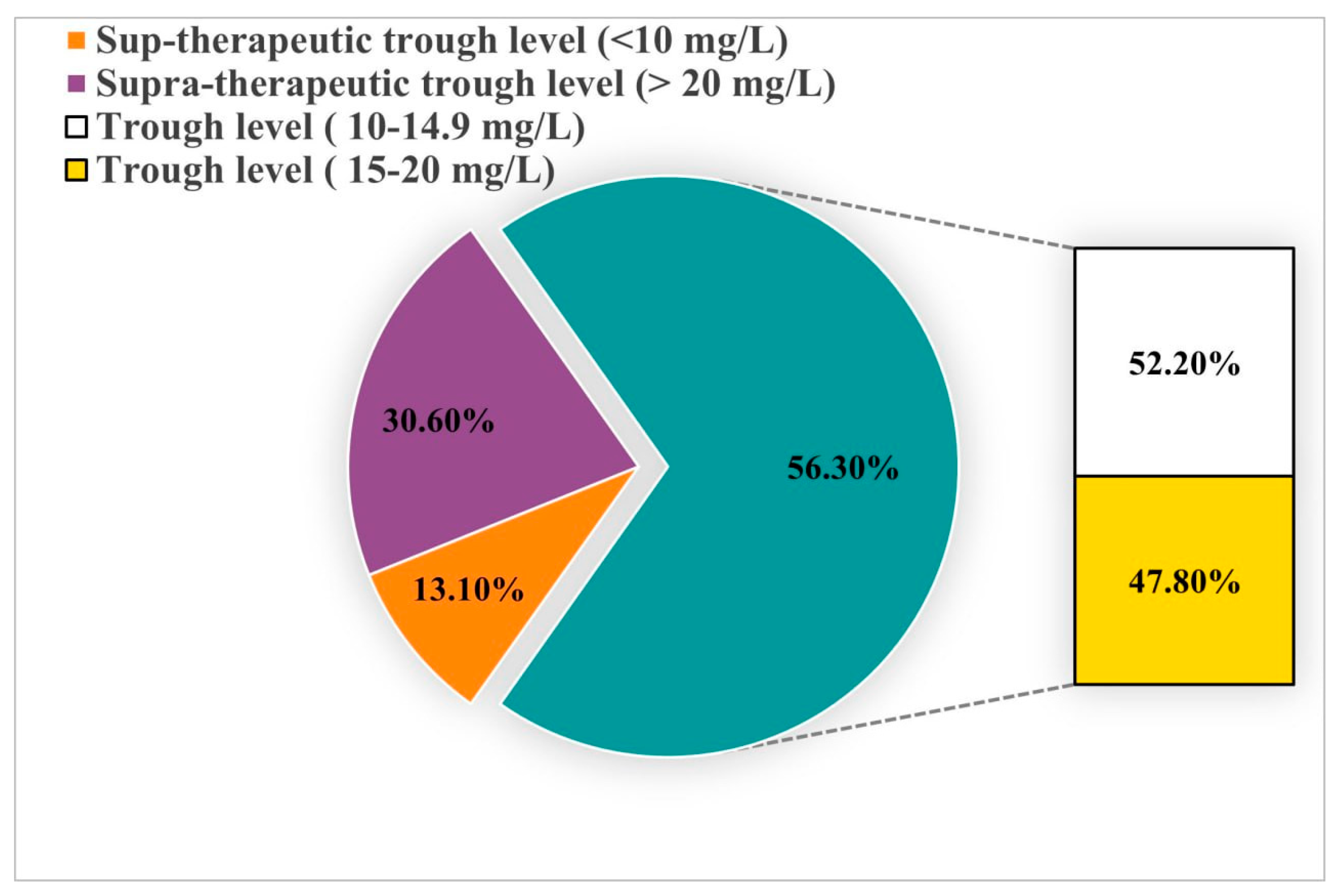
3.2. Percentage of Patients Who Achieved Therapeutic Vancomycin trough Levels Based on Actual SCr
3.3. Predictive Performance of Vancomycin Dosing Based on Actual and Rounded SCr Compared to TMD
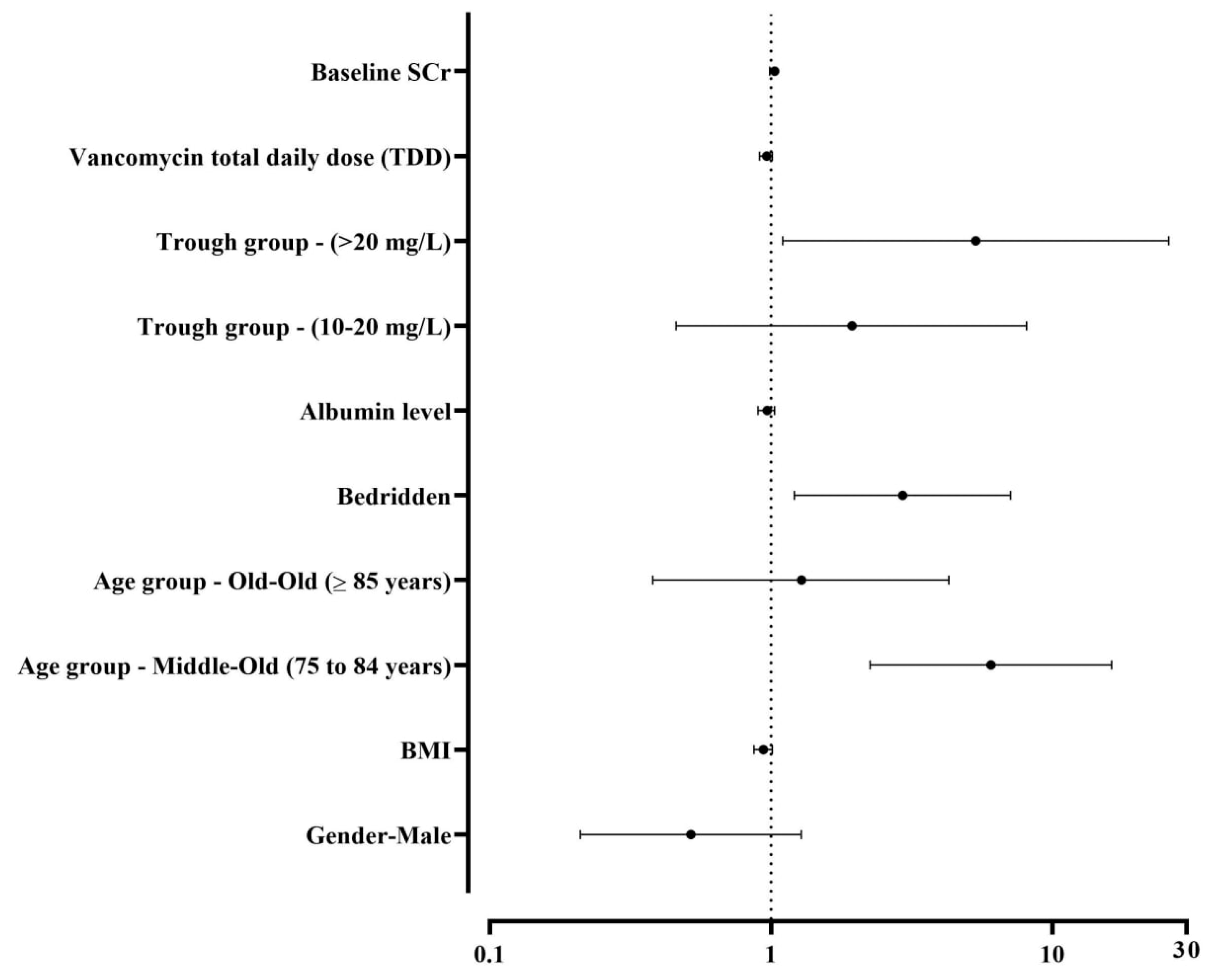
3.4. Incidence and Risk Factors of Vancomycin-Associated Nephrotoxicity (VAN)
4. Discussion
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 2227–2246. [Google Scholar] [CrossRef] [PubMed]
- Pottel, H.; Hoste, L.; Dubourg, L.; Ebert, N.; Schaeffner, E.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; et al. An Estimated Glomerular Filtration Rate Equation for the Full Age Spectrum. Nephrol. Dial. Transplant. 2016, 31, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Sobamowo, H.; Prabhakar, S.S. The Kidney in Aging: Physiological Changes and Pathological Implications. Prog. Mol. Biol. Transl. Sci. 2017, 146, 303–340. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Daniel, M.; Baumhover, S.; Eidson, D.; Green, J. Methodological Study of Vancomycin Dosing in Elderly Patients Using Actual Serum Creatinine Versus Rounded Serum Creatinine. Drugs R&D 2017, 17, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Finney, H.; Bates, C.J.; Price, C.P. Plasma Cystatin C Determinations in a Healthy Elderly Population. Arch. Gerontol. Geriatr. 1999, 29, 75–94. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Kale-Pradhan, P.B. Estimating Creatinine Clearance: A Meta-Analysis. Pharmacotherapy 2011, 31, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.A.; Guhr, K.N.; Berg, G.M. Impact of Various Body Weights and Serum Creatinine Concentrations on the Bias and Accuracy of the Cockcroft-Gault Equation. Pharmacotherapy 2012, 32, 604–612. [Google Scholar] [CrossRef]
- Smythe, M.; Hoffman, J.; Kizy, K.; Dmuchowski, C. Estimating Creatinine Clearance in Elderly Patients with Low Serum Creatinine Concentrations. Am. J. Hosp. Pharm. 1994, 51, 198–204. [Google Scholar] [CrossRef]
- Otani, T.; Kase, Y.; Kunitomo, K.; Shimooka, K.; Kawazoe, K.; Sato, Y.; Yamauchi, A. What Is the Correct Adjustment Protocol for Serum Creatinine Value to Reflect Renal Function in Bedridden Elderly Patients? Jpn J. Nephrol. Pharmacother. 2018, 7, 3–12. [Google Scholar] [CrossRef]
- Butranova, O.I.; Ushkalova, E.A.; Zyryanov, S.K.; Chenkurov, M.S.; Baybulatova, E.A. Pharmacokinetics of Antibacterial Agents in the Elderly: The Body of Evidence. Biomedicines 2023, 11, 1633. [Google Scholar] [CrossRef] [PubMed]
- Gounden, V.; Bhatt, H.; Jialal, I. Renal Function Tests. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Emily Mui, P. SHC Vancomycin Dosing Guide; Stanford Health Care: Stanford, CA, USA, 2015; pp. 1–10. [Google Scholar]
- Al-Dorzi, H.M.; Alsadhan, A.A.; Almozaini, A.S.; Alamri, A.M.; Tamim, H.; Sadat, M.; Al-Swaidan, L.; Elhassan, E.; Arabi, Y.M. The Performance of Equations That Estimate Glomerular Filtration Rate against Measured Urinary Creatinine Clearance in Critically Ill Patients. Crit. Care Res. Pract. 2021, 2021, 5520653. [Google Scholar] [CrossRef] [PubMed]
- Mizokami, F.; Shibasaki, M.; Yoshizue, Y.; Noro, T.; Mizuno, T.; Furuta, K. Pharmacodynamics of Vancomycin in Elderly Patients Aged 75 Years or Older with Methicillin-Resistant Staphylococcus aureus Hospital-Acquired Pneumonia. Clin. Interv. Aging 2013, 8, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dai, N.; Wei, W.; Jiang, C. Outcomes and Nephrotoxicity Associated with Vancomycin Treatment in Patients 80 Years and Older. Clin. Interv. Aging 2021, 16, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Bertino, J.S., Jr. Measured versus Estimated Creatinine Clearance in Patients with Low Serum Creatinine Values. Ann. Pharmacother. 1993, 27, 1439–1442. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Foster, Y.; Cekaj, S. Older Adult Kidney Function Assessment and Rounding Creatinine Led to Medication Dosing Error. Am. J. Ther. 2018, 25, e439–e446. [Google Scholar] [CrossRef] [PubMed]
- Van Hal, S.J.; Paterson, D.L.; Lodise, T.P. Systematic Review and Meta-Analysis of Vancomycin-Induced Nephrotoxicity Associated with Dosing Schedules That Maintain Troughs between 15 and 20 Milligrams per Liter. Antimicrob. Agents Chemother. 2013, 57, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Elyasi, S.; Khalili, H.; Dashti-Khavidaki, S.; Mohammadpour, A. Vancomycin-Induced Nephrotoxicity: Mechanism, Incidence, Risk Factors and Special Populations. A Literature Review. Eur. J. Clin. Pharmacol. 2012, 68, 1243–1255. [Google Scholar] [CrossRef]
- English, K.L.; Paddon-Jones, D. Protecting Muscle Mass and Function in Older Adults during Bed Rest. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 34–39. [Google Scholar] [CrossRef]
- De Rosa, S.; Greco, M.; Rauseo, M.; Annetta, M.G. The Good, the Bad, and the Serum Creatinine: Exploring the Effect of Muscle Mass and Nutrition. Blood Purif. 2023, 52, 775–785. [Google Scholar] [CrossRef]
- Roberts, G.W.; Ibsen, P.M.; Schiøler, C.T. Modified Diet in Renal Disease Method Overestimates Renal Function in Selected Elderly Patients. Age Ageing 2009, 38, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in Youngest-Old, Middle-Old, and Oldest-Old Patients Who Visit the Emergency Department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Toora, B.D.; Rajagopal, G. Measurement of Creatinine by Jaffe’s Reaction--Determination of Concentration of Sodium Hydroxide Required for Maximum Color Development in Standard, Urine and Protein Free Filtrate of Serum. Indian J. Exp. Biol. 2002, 40, 352–354. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | n (%), Mean ± SD, or Median [Q1, Q3] |
|---|---|
| Male | 189 (77) |
| Female | 56 (23) |
| Age (years) | 78.71 ± 9.09 |
| Young-Old (65 to 74 years) n (%) | 92 (37.6) |
| Middle-Old (75 to 84 years) n (%) | 92 (37.6) |
| Old-Old (≥85 years) n (%) | 61 (24.8) |
| TMD of vancomycin (mg) | 1505 ± 579 |
| TDD of vancomycin based on actual SCr (mg) | 1695 ± 583 |
| TDD of vancomycin based on round SCr (mg) | 1487 ± 702 |
| Height (cm) | 162.3 ± 10.7 |
| Median [Q1, Q3] | |
| Body weight (kg) | 65 (55–73.9) |
| BMI (kg/m2) | 24.6 (21–29.6) |
| Albumin (g/L) | 28 (24–31) |
| SCr (mg/dL) | 0.72 (0.62–0.84) |
| CrCl at baseline (mL/min) | 65 (54–83.5) |
| CrCl using rounded SCr (mL/min) | 48 (40–56) |
| Measured vancomycin trough (mg/L) | 16.6 (12.3–21.5) |
| Indicators | TMD | Dosing Based on Actual SCr | Dosing Based on Rounded SCr |
|---|---|---|---|
| Vancomycin dose (mg/day) | 1505 ± 579 | 1695 ± 583 | 1487 ± 702 |
| Coefficient of variation (%) | 38.4 | 34.3 | 47.2 |
| Correlation | 0.55 | 0.43 | |
| Bias (mg/day) | −190 | 17.4 | |
| Precision (mg/day) | ±552 | ±691 | |
| Error (%) | 69 | 92.3 | |
| Accuracy | |||
| ±10% | 57.6 | 40 | |
| ±15% | 58.4 | 40.4 | |
| ±30% | 65.7 | 56.7 | |
| Variable | Non-VAN (n = 201) | VAN (n = 44) | p-Value |
|---|---|---|---|
| Male, n (%) | 135 (67.2) | 30 (68.2) | 0.8 |
| Age, years (mean ± SD) | 78.2 ± 19.1 | 81.2 ± 8.5 | 0.04 |
| BMI (mean ± SD) | 26.3 ± 7.6 | 25.3 ± 5.8 | 0.44 |
| Trough level, mg/L (mean ± SD) | 17 ± 7.5 | 18.9 ± 7.3 | 0.13 |
| SCr, mg/dL (mean ± SD) | 0.69 ± 0.12 | 0.72 ± 0.13 | 0.054 |
| Albumin level, g/L (mean ± SD) | 28.14 ± 6.2 | 26.9 ± 5.8 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bukhari, R.; Hasan, H.; Aljefri, D.; Rambo, R.; AlSenaini, G.; Alzahrani, Y.A.; Alzahrani, A.M. Comparing Actual and Rounded Serum Creatinine Concentration for Assessing the Accuracy of Vancomycin Dosing in Elderly Patients: A Single-Center Retrospective Study. Healthcare 2024, 12, 1144. https://doi.org/10.3390/healthcare12111144
Bukhari R, Hasan H, Aljefri D, Rambo R, AlSenaini G, Alzahrani YA, Alzahrani AM. Comparing Actual and Rounded Serum Creatinine Concentration for Assessing the Accuracy of Vancomycin Dosing in Elderly Patients: A Single-Center Retrospective Study. Healthcare. 2024; 12(11):1144. https://doi.org/10.3390/healthcare12111144
Chicago/Turabian StyleBukhari, Rawan, Hani Hasan, Doaa Aljefri, Rawan Rambo, Ghusun AlSenaini, Yahya A. Alzahrani, and Abdullah M. Alzahrani. 2024. "Comparing Actual and Rounded Serum Creatinine Concentration for Assessing the Accuracy of Vancomycin Dosing in Elderly Patients: A Single-Center Retrospective Study" Healthcare 12, no. 11: 1144. https://doi.org/10.3390/healthcare12111144
APA StyleBukhari, R., Hasan, H., Aljefri, D., Rambo, R., AlSenaini, G., Alzahrani, Y. A., & Alzahrani, A. M. (2024). Comparing Actual and Rounded Serum Creatinine Concentration for Assessing the Accuracy of Vancomycin Dosing in Elderly Patients: A Single-Center Retrospective Study. Healthcare, 12(11), 1144. https://doi.org/10.3390/healthcare12111144