

Patients and Healthcare Providers’ Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review


Abstract
1. Introduction
1.1. Theoretical Background
1.2. Research on PCC for PE Improvement
1.3. Study Aim and Research Questions
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Study Risk of Bias Assessment
2.8. Synthesis Methods
3. Results
3.1. Study Selection
3.2. Study Characteristics
General Findings
3.3. Risk of Bias in Studies
3.4. PE Factors Affecting PCC
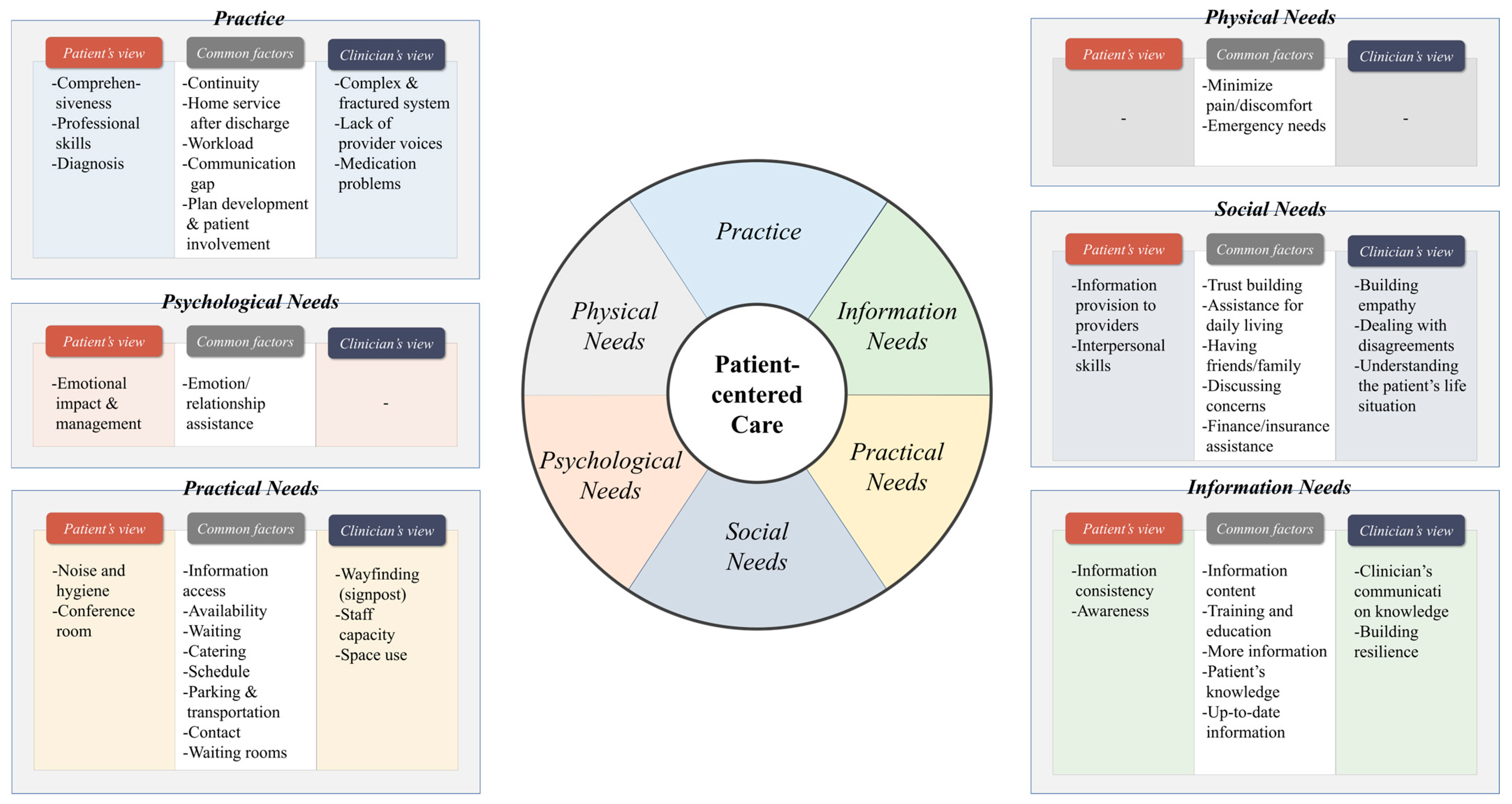
3.5. Patients and Healthcare Providers’ Perspectives on PE Factors
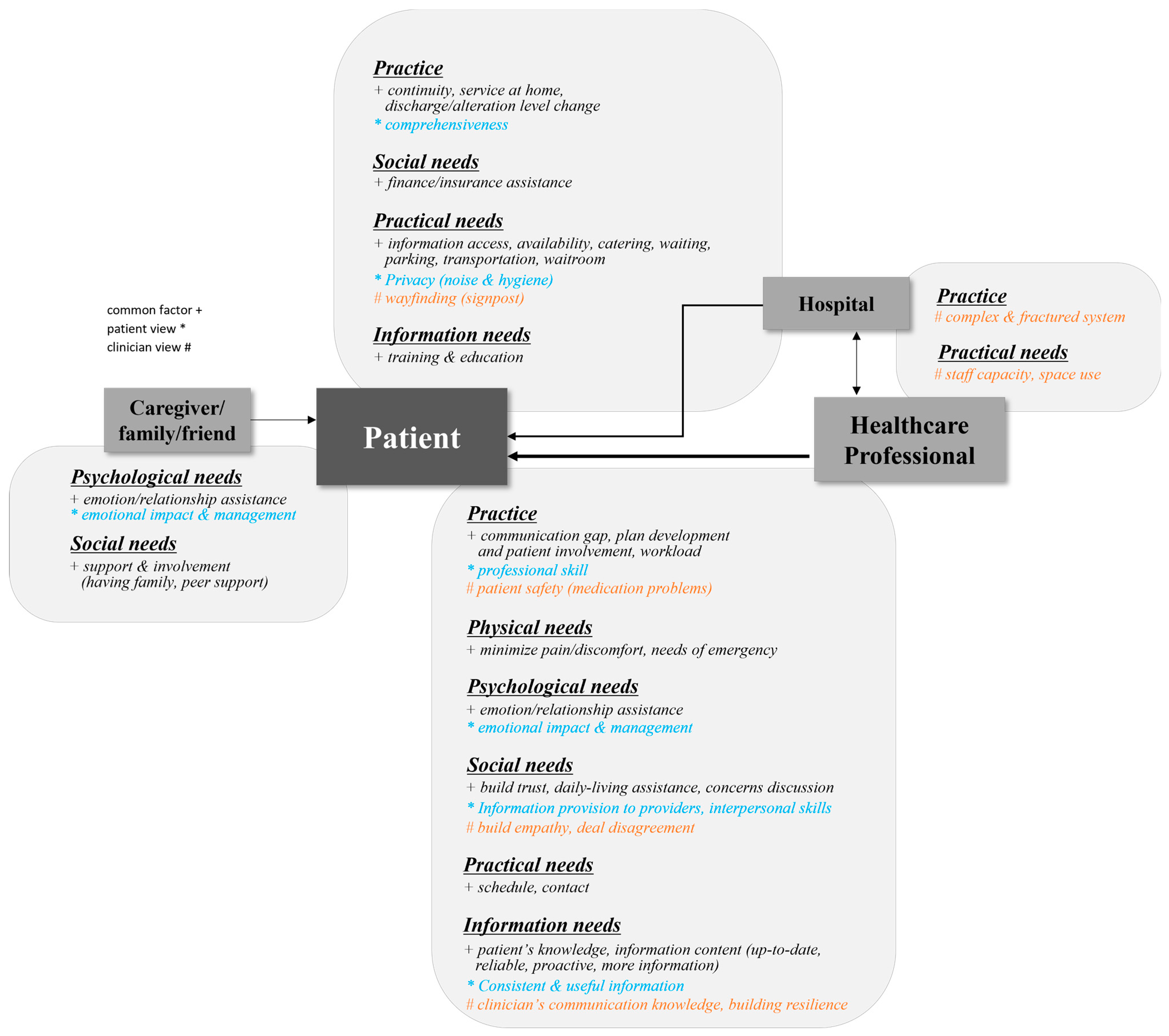
3.6. A Structured and Systematic Model for Explaining the Interaction and Workflow of PCC Delivery
4. Discussion
4.1. Main Findings
4.2. Importance of Understanding PE Factors and Reflecting Service Providers’ Perspectives
4.3. Systematic Model for PCC Delivery
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwame, A.; Petrucka, P.M. A literature-based study of patient-centered care and communication in nurse-patient interactions: Barriers, facilitators, and the way forward. BMC Nurs. 2021, 20, 158. [Google Scholar] [CrossRef]
- Berghout, M.; Van Exel, J.; Leensvaart, L.; Cramm, J.M. Healthcare professionals’ views on patient-centered care in hospitals. BMC Health Serv. Res. 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.; Candlin, S.; Roger, P. New perspectives on understanding cultural diversity in nurse-patient communication. Collegian 2017, 24, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Madula, P.; Kalembo, W.F.; Yu, H.; Kaminga, C.A. Healthcare provider-patient communication: A qualitative study of women’s perceptions during childbirth. Reprod. Health 2018, 15, 135. [Google Scholar] [CrossRef] [PubMed]
- Schöpf, A.C.; Martin, G.S.; Keating, M.A. Humor as a communication strategy in provider-patient communication in a chronic care setting. Qual. Health Res. 2017, 27, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A.; Ruddy, J. Improving patient-provider relationships to improve health care. Clin. Gastroenterol. Hepatol. 2020, 18, 1417–1426. [Google Scholar] [CrossRef]
- Oben, P. Understanding the patient experience: A conceptual framework. J. Patient Exp. 2020, 7, 906–910. [Google Scholar] [CrossRef]
- Tunçalp, Ö.; Were, W.M.; MacLennan, C.; Oladapo, O.T.; Gülmezoglu, A.M.; Bahl, R.; Daelmans, B.; Mathai, M.; Say, L.; Kristensen, F.; et al. Quality of care for pregnant women and newborns—The WHO vision. BJOG 2015, 122, 1045–1049. [Google Scholar] [CrossRef]
- Larson, E.; Sharma, J.; Bohren, M.A.; Tunçalp, Ö. When the patient is the expert: Measuring patient experience and satisfaction with care. Bull. World Health Organ. 2019, 97, 563–569. [Google Scholar] [CrossRef]
- Peimani, M.; Nasli-Esfahani, E.; Sadeghi, R. Patients’ perceptions of patient-provider communication and diabetes care: A systematic review of quantitative and qualitative studies. Chronic Illn. 2020, 16, 3–22. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B. Management of hyperglycaemia approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015, 58, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Deniz, S.; Akbolat, M.; Çimen, M.; Ünal, Ö. The mediating role of shared decision-making in the effect of the patient-physician relationship on compliance with treatment. J. Patient Exp. 2021, 8, 23743735211018066. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, R.; McMillan, C.; Ambrose-Miller, W.; McKee, R.; Brown, J.B. The emerging role of social work in primary health care: A survey of social workers in Ontario family health teams. Health Soc. Work 2018, 43, 109–117. [Google Scholar] [PubMed]
- Kurlander, J.E.; Chey, W.D.; Morris, C.B.; Hu, Y.J.; Padival, R.K.; Bangdiwala, S.I.; Norton, N.J.; Norton, W.F.; Drossman, D.A. Development and validation of the Patient-Physician Relationship Scale among patients with irritable bowel syndrome. Neurogastroenterol. Motil. 2017, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.; Oh, H.J. The effects of patient-centered communication: Exploring the mediating role of trust in healthcare providers. Health Commun. 2019, 35, 502–511. [Google Scholar] [CrossRef] [PubMed]
- McDermott, A.M.; Pedersen, A.R. Conceptions of patients and their roles in healthcare: Insights from everyday practice and service improvement. J. Health Organ. Manag. 2016, 30, 194–206. [Google Scholar] [CrossRef]
- Gartner, J.B.; Abasse, K.S.; Bergeron, F.; Landa, P.; Lemaire, C.; Côté, A. Definition and conceptualization of the patient-centered care pathway, a proposed integrative framework for consensus: A concept analysis and systematic review. BMC Health Serv. Res. 2022, 22, 558. [Google Scholar] [CrossRef] [PubMed]
- Valentijn, P.P.; Biermann, C.; Bruijnzeels, M.A. Value-based integrated (renal) care: Setting a development agenda for research and implementation strategies. BMC Health Serv. Res. 2016, 16, 330. [Google Scholar] [CrossRef] [PubMed]
- Brickley, B.; Williams, L.T.; Morgan, M.; Ross, A.; Trigger, K.; Ball, L. Putting patients first: Development of a patient advocate and general practitioner-informed model of patient-centred care. BMC Health Serv. Res. 2021, 21, 261. [Google Scholar] [CrossRef]
- Bravo, P.; Edwards, A.; Barr, P.J.; Scholl, I.; Elwyn, G.; McAllister, M. Conceptualising patient empowerment: A mixed methods study. BMC Health Serv. Res. 2015, 15, 252. [Google Scholar] [CrossRef]
- Ogden, K.; Barr, J.; Greenfield, D. Determining requirements for patient-centred care: A participatory concept mapping study. BMC Health Serv. Res. 2017, 17, 780. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Belur, J.; Tompson, L.; Thornton, A.; Simon, M. Interrater reliability in systematic review methodology: Exploring variation in coder decision-making. Sociol. Methods Res. 2021, 50, 837–865. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Shostack, G.L. Designing services that deliver. Harv. Bus. Rev. 1984, 62, 133–139. [Google Scholar]
- Powell, R.E.; Doty, A.; Casten, R.J.; Rovner, B.W.; Rising, K.L. A qualitative analysis of interprofessional healthcare team members’ perceptions of patient barriers to healthcare engagement. BMC Health Serv. Res. 2016, 16, 493. [Google Scholar] [CrossRef] [PubMed]
- Coy, K.; Brock, P.; Pomeroy, S.; Cadogan, J.; Beckett, K. A road less travelled: Using experience based co-design to map children’s and families’ emotional journey following burn injury and identify service improvements. Burns 2019, 45, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Litchfield, I.J.; Bentham, L.M.; Lilford, R.J.; McManus, R.J.; Hill, A.; Greenfield, S. Adaption, implementation and evaluation of collaborative service improvements in the testing and result communication process in primary care from patient and staff perspectives: A qualitative study. BMC Health Serv. Res. 2017, 17, 615. [Google Scholar] [CrossRef]
- Kværner, K.J.; Støme, L.N.; Romm, J.; Rygh, K.; Almquist, F.; Tornaas, S.; Berg, M.S. Coassessment framework to identify person-centred unmet needs in stroke rehabilitation: A case report in Norway. BMJ Innov. 2021, 7, 148–156. [Google Scholar] [CrossRef]
- Agha, A.Z.; Werner, R.M.; Keddem, S.; Huseman, T.L.; Long, J.A.; Shea, J.A. Improving patient-centered care. Med. Care 2018, 56, 1009–1017. [Google Scholar] [CrossRef]
- Scott, A.M.; Li, J.; Oyewole-Eletu, S.; Nguyen, H.Q.; Gass, B.; Hirschman, K.B.; Mitchell, S.; Hudson, S.M.; Williams, M.V.; Project ACHIEVE Team. Understanding facilitators and barriers to care transitions: Insights from project ACHIEVE site visits. Jt. Comm. J. Qual. Patient Saf. 2017, 43, 433–447. [Google Scholar] [CrossRef]
- Clarke, M.A.; Moore, J.L.; Steege, L.M.; Koopman, R.J.; Belden, J.L.; Canfield, S.M.; Kim, M.S. Toward a patient-centered ambulatory after-visit summary: Identifying primary care patients’ information needs. Inform. Health Soc. Care 2018, 43, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, V.; Rahman, A.; Zhu, Y.; Enguidanos, S. Reluctance to accept palliative care and recommendations for improvement: Findings from semi-structured interviews with patients and caregivers. Am. J. Hosp. Palliat. Care 2021, 39, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Twamley, J.; Monks, R.; Beaver, K. Using experience-based co-design to prioritise areas for improvement for patients recovering from critical illness. Intensive Crit. Care Nurs. 2023, 76, 103390. [Google Scholar] [CrossRef] [PubMed]
- Fitch, M.I.; Nicoll, I.; Lockwood, G.; Chan, R.J.; Grundy, P. Adolescent and young adult perspectives on challenges and improvements to cancer survivorship care: How are we doing? J. Adolesc. Young Adult Oncol. 2021, 10, 432–442. [Google Scholar] [CrossRef]
- Schäfer, W.L.; Boerma, W.G.; Murante, A.M.; Sixma, H.J.; Schellevis, F.G.; Groenewegen, P.P. Assessing the potential for improvement of primary care in 34 countries: A cross-sectional survey. Bull. World Health Organ. 2015, 93, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Fradgley, E.A.; Paul, C.L.; Bryant, J.; Collins, N.; Ackland, S.P.; Bellamy, D.; Levi, C.R. Collaborative patient-centered quality improvement: A cross-sectional survey comparing the types and numbers of quality initiatives selected by patients and health professionals. Eval. Health Prof. 2016, 39, 475–495. [Google Scholar] [CrossRef]
- Fradgley, E.A.; Paul, C.L.; Bryant, J.; Oldmeadow, C. Getting right to the point: Identifying Australian outpatients’ priorities and preferences for patient-centred quality improvement in chronic disease care. Int. J. Qual. Health Care 2016, 28, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Hovén, E.; Lannering, B.; Gustafsson, G.; Boman, K.K. Information needs of survivors and families after childhood CNS tumor treatment: A population-based study. Acta Oncol. 2018, 57, 649–657. [Google Scholar] [CrossRef]
- Hwang, A.; Warshaw, G. Joint AGS-CCEHI survey offers insights into patient engagement in geriatric clinical settings. J. Am. Geriatr. Soc. 2019, 67, 1791–1794. [Google Scholar] [CrossRef]
- Amoah, V.; Anokye, R.; Boakye, D.S.; Gyamfi, N. Perceived barriers to effective therapeutic communication among nurses and patients at Kumasi South Hospital. Cogent Med. 2018, 5, 1459341. [Google Scholar] [CrossRef]
- Hall, A.; Bryant, J.; Sanson-Fisher, R.; Grady, A.; Proietto, A.; Doran, C.M. Top priorities for health service improvements among Australian oncology patients. Patient Relat. Outcome Meas. 2021, 12, 83. [Google Scholar] [CrossRef]
- Fitch, M.; Zomer, S.; Lockwood, G.; Louzado, C.; Shaw Moxam, R.; Rahal, R.; Green, E. Experiences of adult cancer survivors in transitions. Support. Care Cancer 2019, 27, 2977–2986. [Google Scholar] [CrossRef]
- Fradgley, E.A.; Paul, C.L.; Bryant, J.; Roos, I.A.; Henskens, F.A.; Paul, D.J. Consumer participation in quality improvements for chronic disease care: Development and evaluation of an interactive patient-centered survey to identify preferred service initiatives. J. Med. Internet Res. 2014, 16, e3545. [Google Scholar] [CrossRef]
- Ågård, A.S.; Hofhuis, J.G.; Koopmans, M.; Gerritsen, R.T.; Spronk, P.E.; Engelberg, R.A.; Curtis, J.R.; Zijlstra, J.G.; Jensen, H.I. Identifying improvement opportunities for patient-and family-centered care in the ICU: Using qualitative methods to understand family perspectives. J. Crit. Care 2019, 49, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Guiu, J.; Arroyo-Fernández, I.; Rubio, R. Impact of patients’ attitudes and dynamics in needs and life experiences during their journey in COPD: An ethnographic study. Expert. Rev. Respir. Med. 2021, 16, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Creutzfeldt, C.J.; Engelberg, R.A.; Healey, L.; Cheever, C.S.; Becker, K.J.; Holloway, R.G.; Curtis, J.R. Palliative care needs in the neuro-ICU. Crit. Care Med. 2015, 43, 1677. [Google Scholar] [CrossRef] [PubMed]
- Bowie, P.; McNab, D.; Ferguson, J.; De Wet, C.; Smith, G.; MacLeod, M.; McKay, J.; White, C. Quality improvement and person-centredness: A participatory mixed methods study to develop the ‘always event’ concept for primary care. BMJ Open 2015, 5, e006667. [Google Scholar] [CrossRef]
- Stevens, M.C.; Beynon, P.; Cameron, A.; Cargill, J.; Cheshire, J.; Dolby, S. Understanding and utilizing the unmet needs of teenagers and young adults with cancer to determine priorities for service development: The Macmillan on target programme. J. Adolesc. Young Adult Oncol. 2018, 7, 652–659. [Google Scholar] [CrossRef]
- Rose, L.; Istanboulian, L.; Amaral, A.C.K.B.; Burry, L.; Cox, C.E.; Cuthbertson, B.H.; Iwashyna, T.J.; Dale, C.M.; Fraser, I. Co-designed and consensus based development of a quality improvement checklist of patient and family-centered actionable processes of care for adults with persistent critical illness. J. Crit. Care 2022, 72, 154153. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Electronic Databases | Search Terms |
|---|---|
| Google Scholar (n = 3260) | “healthcare service design” AND “co-design” OR “experience-based co-design” AND “quality healthcare” OR “quality improvement” AND “patient experience” OR “patient perspectives” OR “patient-centered care” |
| PubMed (n = 1343) | “healthcare, service design” AND “patient experience” OR “patient centered” OR “co-design” AND “quality improvement” |
| Web of Science (n = 6303) | ALL = (“healthcare, service design” AND “patient experience” OR “patient centered” OR “co-design” AND “quality improvement”) |
| Taylor and Francis Journal (n = 2578) | [All: “healthcare, service design”] AND [All: “patient experience”] OR [All: “patient centered”] OR [All: “co-design”] AND [All: “quality improvement”] |
| Total | N = 13,484 |
| No. | Authors (Year) | Country | Study Purpose | Target User (Perspective) | Participants | Methods | Analysis | Solutions | MMAT |
|---|---|---|---|---|---|---|---|---|---|
| Qualitative Study (n = 9) | |||||||||
| 1 | Powell et al. (2016) [26] | USA | Analysis of patient barriers to healthcare engagement and suggestions for improvement | Patients (general) | Interprofessional team members | Focus groups and semi-structured interviews | Content analysis | Suggestion of ideas | Moderate |
| 2 | Coy et al. (2019) [27] | UK | Insight identification to meet patient/families’ emotional needs | Children and families suffering from burn injury | Families, practitioners | Interviews, short films, focus group events | Video-based analysis, thematic analysis | Film and suggestion of ideas | High |
| 3 | Litchfield et al. (2017) [28] | UK | Development and implementation of strategies for patient satisfaction and efficiency of existing process | Patients and healthcare providers | Patients, medical staff | Focus groups | Thematic -framework analysis | Refinement of existing process | High |
| 4 | Kværner et al. (2020) [29] | Norway | Identification of unmet needs for person-centered care and insights for improvement | Patients and medical staff | Multidisciplinary stakeholders (patients and next of kin, health partner employees, decision-makers, representatives from health partners, user organizations, innovation advisors) | Workshops | Stakeholder analysis | Three categories of unmet needs (for scenario building) | High |
| 5 | Agha et al. (2018) [30] | USA | Identification of patient engagement barriers and solutions | Medical staff | Medical staff | Interviews, site visits | Thematic analysis | x | Moderate |
| 6 | Scott et al. (2017) [31] | USA | Identification of facilitators and barriers to implementation of transitional care services in health systems | Leaders of healthcare organizations, patients, families | Multidisciplinary team (the leadership team, transitional care team, internal stakeholders, community partners, patients and family caregivers) | Interviews, site visits, observations | Thematic analysis | x | High |
| 7 | Clarke et al. (2018) [32] | USA | Identification of information needs of primary care patients for the improvement of clinic visit notes (tool) | Primary care physician, patients | Outpatients | Interviews | Thematic analysis | x | High |
| 8 | Cardenas et al. (2021) [33] | USA | Identification of patients’ and caregivers’ barriers to home-based palliative care and their recommendations for improvement | Patients, caregivers eligible for palliative care | Patients, proxies, caregivers | Interviews | Thematic analysis | x | High |
| 9 | Twamley et al. (2023) [34] | UK | Prioritization areas for improvement in care and services for patients | Patients | Patients, family/friends, hospital staff | Experience-based codesign (EBCD), observation, interviews, film development, feedback/joint event | Thematic analysis | x | Moderate |
| Quantitative Study (n = 8) | |||||||||
| 10 | Fitch et al. (2021) [35] | Canada | Review of main challenges of adolescent and young adults (AYA) cancer survivors and their suggestions for care improvement | AYA cancer survivors (18–34 years) and patients | AYA cancer survivors (18–34 years) and patients | Survey | Content analysis | Suggestion of ideas | High |
| 11 | Schäfer et al. (2015) [36] | 31 European countries, Australia, Canada, and New Zealand | Investigation of patients’ perceptions of improvement potential in primary care | Patients | Patients of general practitioner | Survey | Statistics, evaluation questionnaire | x | High |
| 12 | Fradgley et al. (2016) (a) [37] | Australia | Identification of patients’ and health professionals’ quality improvement preferences | Patients and healthcare professionals | Outpatients, healthcare professionals | Survey | Statistics | x | High |
| 13 | Fradgley et al. (2016) (b) [38] | Australia | Identification of patients’ preferences of initiatives for change | Outpatients | Outpatients | Survey | Statistics | x | High |
| 14 | Hoven et al. (2018) [39] | Sweden | Identification of information needs and satisfaction with provided information | Survivors and families after childhood central nervous system (CNS) tumor treatment | Childhood CNS tumor survivors, parents | Self-report questionnaire | Statistics | x | Moderate |
| 15 | Hwang and Warshaw (2019) [40] | USA | Understanding the values and needs of the patients | Geriatric practitioners | American Geriatrics Society (AGS) members | Descriptive survey | Statistics | x | Moderate |
| 16 | Amoah et al. (2018) [41] | Ghana | Identification of the barriers to therapeutic communication among nurses and patients | Nurses, patients | Nurses and patients at local public hospital | Survey | Statistics | x | Moderate |
| 17 | Hall et al. (2021) [42] | Australia | Identification of the potential intervention to be improved for patient-centered care | Healthcare leaders, researchers, patients | Cancer patients with oncology treatment | Survey | Statistics | x | Moderate |
| Mixed-Methods Study (n = 8) | |||||||||
| 18 | Fitch et al. (2019) [43] | Canada | Identification of unmet needs and experiences of cancer survivors for survivorship program improvement | Healthcare providers, patients | Cancer survivors between 1 and 3 years post-treatment | Literature review, interviews, survey | Statistics | x | High |
| 19 | Fradgley et al. (2014) [44] | Australia | Development and testing of a web-based survey to identify and prioritize patient-centered initiatives in chronic disease outpatient services | Patients | Oncology patients | Literature review, feedback from expert, pilot study (survey) to test feasibility, survey | Statistics | x | Moderate |
| 20 | Agard et al. (2018) [45] | Denmark, Netherlands | Analysis of family perspectives for identifying improvement opportunities in the intensive care unit (ICU) | Family members of patients with ICU stay | Family members of patients with ICU stay | Survey (free text comments) | Content analysis | x | High |
| 21 | Martinez-Guiu et al. (2021) [46] | Spain | Identification of patients’ attitudes, experiences, and needs | Chronic obstructive pulmonary disease (COPD) patients | Patients, healthcare professionals | Interviews, survey | Statistics, inductive analysis | x | High |
| 22 | Creutzfeldt et al. (2015) [47] | USA | Identification of palliative care needs for patients and their families | Patients in neuro ICU and families | Clinical team in the neuro ICU | Literature review, expert discussion, cohort study | Thematic analysis | Screening tool as a checklist | Moderate |
| 23 | Bowie et al. (2015) [48] | UK | Review of existing criteria for selecting “always events” (AEs) and generating a candidate list of AE examples to introduce the concept of AE application | Patients | Patients of primary care settings from 13 practices | Interviews and questionnaire | Content analysis, statistics | x | High |
| 24 | Stevens et al. (2018) [49] | UK | Identification of unmet needs among AYA cancer patients for service development | Local healthcare leaders/administrators | AYA patients, families, networkers, professionals | Survey, interviews, focus groups | Requirement management method (engineering and software development system) | Intervention development areas (software) | High |
| 25 | Rose et al. (2022) [50] | Canada | Consensus based development of a quality improvement checklist for patients | Patients/family | ICU interprofessional team, patients, family members | EBCD, systematic review, semi-structured video/phone interviews, touchpoint video production, modified delphi, consensus meeting | Content analysis | A quality improvement checklist | High |
| Category | Results (Total n = 25) | |
|---|---|---|
| Country | USA (n = 7, 28%), UK (n = 5, 20%), Australia (n = 4, 16%), Canada (n = 3, 12%), multiple countries (n = 2, 8%), Ghana (n = 1, 4%), Norway (n = 1, 4%), Spain (n = 1, 4%), Sweden (n = 1, 4%) | |
| Target user | Patients/caregivers (n = 14, 56%), patients and healthcare providers (n = 6, 24%), healthcare administrators/organization leaders (n = 3, 12%), healthcare providers (n = 2, 8%) | |
| Participants | Patients (n = 10, 40%), patients and healthcare providers (n = 7, 28%), multidisciplinary teams (n = 4, 16%), healthcare providers (n = 2, 8%), healthcare professionals (n = 2, 8%) | |
| Study scope | Patients’ needs and perspectives (n = 19, 76%), patients’ engagement and interaction (n = 4, 16%), system improvement (n = 1, 4%), checklist development (n = 1, 4%) | |
| Methods and analysis (multiple methods were counted individually) | Qualitative | Interview (n = 7), focus group meeting (n = 3), site visit (n = 2), workshop (n = 1), short film (n = 2), observation (n = 2), feedback/joint event (n = 1) |
| Quantitative | Survey (n = 8) | |
| Mixed-methods | Literature review/interview/survey (n = 2), survey with free text comments (n = 1), interview/survey (n = 2), literature review/expert discussion/cohort study (n = 1), survey/interview/focus group meeting (n = 1), literature review/interview/video production/delphi/consensus meeting (n = 1) | |
| Solution | None (n = 17, 68%), suggestions of ideas (n = 3, 12%), hierarchy of needs/intervention area (n = 2, 8%), refinement to existing process (n = 1, 4%), screening tool development (n = 1, 4%), checklist (n = 1, 4%) | |
| Category | Subcategory | PE Factors |
|---|---|---|
| Practice (n = 22) | System (n = 6) | Complex and fractured system (lack of uniformity, out-of-date, slow system) [26,30] |
| Lack of expertise [29] | ||
| Underutilized care program/system [31] | ||
| Limited resources [31] | ||
| Workload, overwork, staffing (overburden) [30,34,41] | ||
| Bureaucratic culture (demands of national priority, lack of providers’ voices) [30] | ||
| Tool (n = 2) | Alert system/tool [28] | |
| Simplified tools and services [46,50] | ||
| Coordination (n = 4) | Continuity [34,36,38,42,43,44,45,48,49] | |
| Communication gap [26,31,37] | ||
| Uniform implementation [31] | ||
| Comprehensiveness [36] | ||
| Care plan (n = 6) | Service at home [26,27,31,34] | |
| Prioritizing care service [31] | ||
| Medicine management [26] | ||
| Plan development and patient involvement [32,34,50] | ||
| Care management [34,48] | ||
| Discharge/alteration level change [26,34,45] | ||
| Management (n = 2) | Information management [31,45] | |
| Evaluating and adapting care approaches [31,50] | ||
| Skill (n = 2) | Professional skills (care and treatment) [45] | |
| Diagnosis [46] | ||
| Physical Needs (n = 3) | Physical support (n = 2) | Minimize pain or discomfort, physical symptoms help [38,44,50] |
| Needs of emergency [34,46] | ||
| Physical symptoms (n = 1) | Physical symptoms; pain, physical discomfort [41,47] | |
| Psychological Needs (n = 5) | Emotional support (n = 2) | Assistance (emotion/relationship); emotional support [31,37,38,44,48,49,50] |
| Emotional management [46] | ||
| Psychological symptoms (n = 3) | Isolation; fear; anxiety; psychological symptoms; too overwhelmed [27,34,40,41,46,47] | |
| Feeling of patient insecurity [29] | ||
| Emotional impact [27] | ||
| Social Needs (n = 14) | Communication/interaction (n = 7) | Providers not understanding patients’ life situations [26] |
| Patient concerns discussion with clinician; all your concerns are addressed [37,38,44] | ||
| Form trusting relationships; interactions and relationships [26,31,34,36,38,43,44,48] | ||
| Talk about worries for the future [49] | ||
| Age difference [41] | ||
| Disagreement [47] | ||
| Providing information to professionals [45] | ||
| Support and involvement (n = 5) | Assistance (daily living) [34,37,38,44] | |
| Support and involvement [31,36,38,42,44] | ||
| Having friends or family; families to be present at the bedside [34,38,44,45] | ||
| Practical support, finance, and insurance [26,34,43] | ||
| Social/peer support [47,49] | ||
| Respect (n = 2) | Interpersonal skills [45] | |
| Share information, lack of empathy/interest/respect [30,41] | ||
| Practical Needs (n = 17) | Access to info (n = 1) | Information access [27,28,34,37,42,43,45] |
| Access to care (n = 8) | Timing [33] | |
| Waiting [28,37,38,42,44] | ||
| Schedule [28,37,38,44] | ||
| Parking [37,38,42,44] | ||
| Transportation (access) [37,38,40,44] | ||
| Contact [37,38,44] | ||
| Funding/staff capacity [40] | ||
| Availability [30,36,43,48,50] | ||
| Access to service (n = 1) | Catering [37,38,42,44,45] | |
| Environment (n = 7) | Waiting rooms [38,44,45] | |
| Treatment rooms [38,44] | ||
| Conference rooms [45] | ||
| Limited space (teams were not seated with each other, multiple teams were sharing rooms) [30] | ||
| Signposting [49] | ||
| Unfamiliar environment [41] | ||
| Noise and hygiene [45] | ||
| Information Needs (n = 19) | Knowledge (n = 6) | Knowledge/understanding; patients’ skills or knowledge [33,34,38,40,44] |
| Misconception [33] | ||
| Self-perception [33] | ||
| Invisible problems (cognitive) [29] | ||
| Awareness [46] | ||
| Clinicians’ communication knowledge [41] | ||
| Information (content and extent) (n = 10) | Up-to-date information [37,38,42,44] | |
| Information content [37,38,42,44,45,49,50] | ||
| Information consistency [27] | ||
| More information [34,38,39,44,49] | ||
| Alerting cognitive effects of treatment (care info) [49] | ||
| Information extent, insufficient information/too much information without proper explanation [26,39] | ||
| Information usefulness [34,39,49] | ||
| Information data [32] | ||
| Inadequate review (content) [31] | ||
| Proactive information [26] | ||
| Education (n = 3) | Training and education; education [30,31,43,46,49,50] | |
| Self-management skills/education [49,50] | ||
| Building resilience [49] |
| Category | Common Factors | Patient’s Perspective | Healthcare Provider’s Perspective |
|---|---|---|---|
| Practice | Lack of expertise [29], Underutilized care program/system [31], Limited resources [31], Workload [30,34,41], Alert system/tool [28], Simplified tools and services [46,50], Continuity [34,36,38,42,43,44,45,48,49], Communication gap [26,31,37], Uniform implementation [31], Information management [31,45], Evaluating and adapting care approaches [31,50], Service at home [26,27,31,34], Prioritizing care services [31], Plan development and patient involvement [32,34,50], Care management [34,48], Discharge/alteration level change [26,34,45] | Comprehensiveness [36], Professional skill [45], Diagnosis [46] | Complex and fractured system [26,30], Bureaucratic culture (lack of providers’ voices) [30], Medicine management [26] |
| Physical Needs | Minimize pain or discomfort [38,44,50], Emergency needs [34,46], Physical symptoms [41,47] | - | - |
| Psychological Needs | Assistance (emotion/relationship) [31,37,38,44,48,49,50], Psychological symptoms [27,34,40,41,46,47], Feeling of patient insecurity [29] | Emotional management [46], Emotional impact [27] | - |
| Social Needs | Patient concerns about discussions with clinicians [37,38,44], Form trusting relationships [26,31,34,36,38,43,44,48], Talk about future worries [49], Assistance (daily living) [34,37,38,44], Support and involvement [31,36,38,42,44], Having friends or family [34,38,44,45], Practical support (finance and insurance) [26,34,43], Social/peer support [47,49] | Providing information to professionals [45], Interpersonal skills [45] | Providers do not understand patients’ life situations [26], Dealing with disagreement [47] Age difference [41], Share information/lack of empathy [30,41] |
| PracticalNeeds | Information access [27,28,34,37,42,43,45], Timing [33], Waiting [28,37,38,42,44], Schedule [28,37,38,44], Parking [37,38,42,44], Transportation [37,38,40,44], Contact [37,38,44], Availability [30,36,43,48,50], Catering [37,38,42,44,45], Waiting rooms [38,44,45], Treatment room [38,44] | Conference room [45], Noise and hygiene [45] | Funding/staff capacity [40], Limited space [30], Signposting [49], Unfamiliar environment [41] |
| Information needs | Patient’s knowledge [33,34,38,40,44], Misconception [33], Self-perception [33], Cognitive problems [29], Up-to-date information [37,38,42,44], Information content [37,38,42,44,45,49,50], More information [34,38,39,44,49], Alerting cognitive effects of treatment [49], Information extent/insufficient information [26,39], Information usefulness [34,39,49], Inadequate review [31], Proactive information [28], Training and education [30,31,43,46,49,50], Self-management skills/education [49,50] | Awareness [46], Information consistency [27], Information data [32] | Clinician’s communication knowledge [41], Building resilience [49] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.-J.; Koo, Y.-R.; Nam, I.-C. Patients and Healthcare Providers’ Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review. Healthcare 2024, 12, 1090. https://doi.org/10.3390/healthcare12111090
Kim E-J, Koo Y-R, Nam I-C. Patients and Healthcare Providers’ Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review. Healthcare. 2024; 12(11):1090. https://doi.org/10.3390/healthcare12111090
Chicago/Turabian StyleKim, Eun-Jeong, Yoo-Ri Koo, and Inn-Chul Nam. 2024. "Patients and Healthcare Providers’ Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review" Healthcare 12, no. 11: 1090. https://doi.org/10.3390/healthcare12111090
APA StyleKim, E.-J., Koo, Y.-R., & Nam, I.-C. (2024). Patients and Healthcare Providers’ Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review. Healthcare, 12(11), 1090. https://doi.org/10.3390/healthcare12111090