
Physical Activity, Alcohol, and Cigarette Use in Urological Cancer Patients over Time since Diagnosis

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
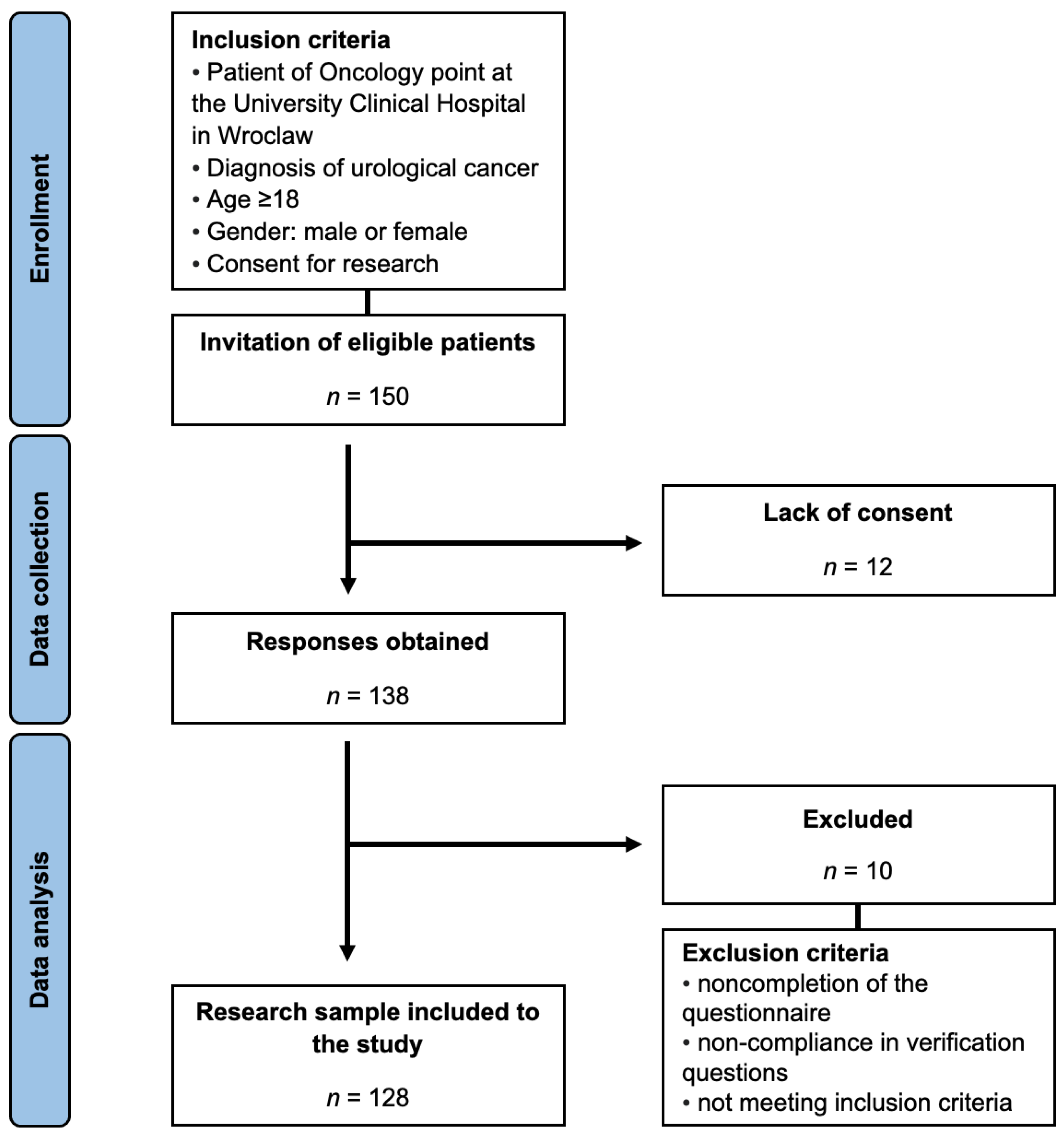
2.1. Study Design and Participants
2.2. International Physical Activity Questionnaire (IPAQ)
2.3. Alcohol Use Disorders Identification Test (AUDIT)
2.4. Fagerstrom Test for Nicotine Dependence (FTND)
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Physical Activity
3.3. Alcohol
3.4. Cigarettes Smoking
3.5. Multiple Logistic Regression Model
4. Discussion
4.1. Physical Activity
4.2. Alcohol Use and Abuse
4.3. Cigarette Smoking
4.4. Future Perspectives
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raporty|Krajowy Rejestr Nowotworów. Available online: http://onkologia.org.pl/pl/raporty (accessed on 4 November 2023).
- Leuteritz, K.; Richter, D.; Mehnert-Theuerkauf, A.; Stolzenburg, J.-U.; Hinz, A. Quality of Life in Urologic Cancer Patients: Importance of and Satisfaction with Specific Quality of Life Domains. Qual. Life Res. 2022, 31, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Davies, N. Lifestyle during and after Cancer Treatment. Clin. Oncol. (R. Coll. Radiol.) 2007, 19, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Luque-Reca, O.; Soriano-Maldonado, A.; Gavilán-Carrera, B.; Acosta-Manzano, P.; Ariza-Vega, P.; Del Paso, G.A.R.; Álvarez-Gallardo, I.C.; Estévez-López, F. Longitudinal Associations of Physical Fitness and Affect with Depression, Anxiety and Life Satisfaction in Adult Women with Fibromyalgia. Qual. Life Res. 2022, 31, 2047–2058. [Google Scholar] [CrossRef] [PubMed]
- Misiąg, W.; Piszczyk, A.; Szymańska-Chabowska, A.; Chabowski, M. Physical Activity and Cancer Care—A Review. Cancers 2022, 14, 4154. [Google Scholar] [CrossRef] [PubMed]
- Liska, T.M.; Kolen, A.M. The Role of Physical Activity in Cancer Survivors’ Quality of Life. Health Qual. Life Outcomes 2020, 18, 197. [Google Scholar] [CrossRef]
- Calvert, C.M.; Burgess, D.; Erickson, D.; Widome, R.; Jones-Webb, R. Cancer Pain and Alcohol Self-Medication. J. Cancer Surviv. 2023, 17, 1561–1570. [Google Scholar] [CrossRef]
- Shi, M.; Luo, C.; Oduyale, O.K.; Zong, X.; LoConte, N.K.; Cao, Y. Alcohol Consumption among Adults with a Cancer Diagnosis in the All of Us Research Program. JAMA Netw. Open 2023, 6, e2328328. [Google Scholar] [CrossRef]
- Fernandez, A.C.; Bohnert, K.M.; Bicket, M.C.; Weng, W.; Singh, K.; Englesbe, M. Adverse Surgical Outcomes Linked to Co-Occurring Smoking and Risky Alcohol Use Among General Surgery Patients. Ann. Surg. 2023, 278, 201–207. [Google Scholar] [CrossRef]
- Tønneson, H.; Petersen, K.R.; Nielsen, H.J.; Kehlet, H.; Højgaard, L.; Stokholm, K.H.; Knigge, U. Postoperative Morbidity among Symptom-Free Alcohol Misusers. Lancet 1992, 340, 334–337. [Google Scholar] [CrossRef]
- Duffy, S.A.; Louzon, S.A.; Gritz, E.R. Why Do Cancer Patients Smoke and What Can Providers Do about It? Community Oncol. 2012, 9, 344–352. [Google Scholar] [CrossRef]
- Taborelli, M.; Dal Maso, L.; Zucchetto, A.; Lamaj, E.; De Paoli, P.; Carbone, A.; Serraino, D. Prevalence and Determinants of Quitting Smoking after Cancer Diagnosis: A Prospective Cohort Study. Tumori 2022, 108, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Crivelli, J.J.; Shariat, S.F.; Chun, F.K.; Messing, E.M.; Soloway, M.S. Smoking and Bladder Cancer: A Systematic Review of Risk and Outcomes. Eur. Urol. Focus 2015, 1, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J. Lifestyle Factors in Cancer Survivorship. JCO 2012, 30, 3697–3704. [Google Scholar] [CrossRef] [PubMed]
- Carraro, E.; Schilirò, T.; Biorci, F.; Romanazzi, V.; Degan, R.; Buonocore, D.; Verri, M.; Dossena, M.; Bonetta, S.; Gilli, G. Physical Activity, Lifestyle Factors and Oxidative Stress in Middle Age Healthy Subjects. Int. J. Environ. Res. Public Health 2018, 15, 1152. [Google Scholar] [CrossRef]
- Jassem, J. Tobacco Smoking after Diagnosis of Cancer: Clinical Aspects. Transl. Lung Cancer Res. 2019, 8, S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A. Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ)—Wersja Polska. Wych. Fiz. Sport 2007, 51, 47–54. [Google Scholar]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Bergier, J.; Kapka-Skrzypczak, L.; Biliński, P.; Paprzycki, P.; Wojtyła, A. Physical Activity of Polish Adolescents and Young Adults According to IPAQ: A Population Based Study. Ann. Agric. Environ. Med. 2012, 19, 109–115. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Klimkiewicz, A.; Jakubczyk, A.; Mach, A.; Abramowska, M.; Szczypiński, J.; Berent, D.; Skrzeszewski, J.; Witkowski, G.; Wojnar, M. Psychometric Properties of the Polish Version of the Alcohol Use Disorders Identification Test (AUDIT). Drug Alcohol Depend. 2021, 218, 108427. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A Revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Samochowiec, J.; Rogoziński, D.; Hajduk, A.; Skrzypińska, A.; Arentowicz, G. Diagnostyka, Mechanizm Uzależnienia i Metody Leczenia Uzależnienia Od Nikotyny. Alkohol. Narkom. 2001, 14, 323–340. [Google Scholar]
- Wojnar, M.; Wierzbiński, P.; Samochowiec, J.; Rymaszewska, J.; Filipiak, K.J.; Wichniak, A.; Mróz, R.; Mamcarz, A.; Dudek, D. Management of Nicotine Dependence in Patients with Psychiatric Disorders—Recommendations of the Polish Psychiatric Association—Part II. Psychiatr. Pol. 2023, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.; Guan, Y.; Li, H.; Chen, W.; Zhu, G. Urologic Cancer in China. Jpn. J. Clin. Oncol. 2016, 46, 497–501. [Google Scholar] [CrossRef]
- Bladder Cancer—Treatment. Available online: https://www.nhs.uk/conditions/bladder-cancer/treatment/ (accessed on 30 October 2023).
- Stone, P.C.; Minton, O. Cancer-Related Fatigue. Eur. J. Cancer 2008, 44, 1097–1104. [Google Scholar] [CrossRef]
- Hesketh, P.J. Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2008, 358, 2482–2494. [Google Scholar] [CrossRef]
- Zraik, I.M.; Heß-Busch, Y. Management of chemotherapy side effects and their long-term sequelae. Urol. A 2021, 60, 862–871. [Google Scholar] [CrossRef]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Próchnicki, M.; Rudzki, S.; Laskowska, B.; Brudniak, J. Quality of Life of Cancer Patients Treated with Chemotherapy. Int. J. Environ. Res. Public Health 2020, 17, 6938. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Bland, K.A.; Zucker, D.S.; Bovard, J.; Shenkier, T.; McKenzie, D.C.; Davis, M.K.; Gelmon, K.A.; Campbell, K.L. “Chemotherapy-Periodized” Exercise to Accommodate for Cyclical Variation in Fatigue. Med. Sci. Sports Exerc. 2020, 52, 278–286. [Google Scholar] [CrossRef]
- Teixeira, A.; Wender, M.; Gonçalves, A.; Freitas, C.; Santos, A.; Soldera, C. Dizziness, Physical Exercise, Falls, and Depression in Adults and the Elderly. Int. Arch. Otorhinolaryngol. 2015, 20, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, D.P.; Lad, N.L.; Koniaris, L.G.; Zimmers, T.A. Bone Pain and Muscle Weakness in Cancer Patients. Curr. Osteoporos. Rep. 2017, 15, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Li, J.-Q.; Shi, J.-F.; Que, J.-Y.; Liu, J.-J.; Lappin, J.M.; Leung, J.; Ravindran, A.V.; Chen, W.-Q.; Qiao, Y.-L.; et al. Depression and Anxiety in Relation to Cancer Incidence and Mortality: A Systematic Review and Meta-Analysis of Cohort Studies. Mol. Psychiatry 2020, 25, 1487–1499. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Dishman, R.K.; Gordon, B.R.; Herring, M.P. Physical Activity and Anxiety: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Am. J. Prev. Med. 2019, 57, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.L.; Audrey, S.; Gunnell, D.; Cooper, A.; Campbell, R. The Relationship between Physical Activity, Mental Wellbeing and Symptoms of Mental Health Disorder in Adolescents: A Cohort Study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 138. [Google Scholar] [CrossRef] [PubMed]
- Gjerset, G.M.; Fosså, S.D.; Courneya, K.S.; Skovlund, E.; Jacobsen, A.B.; Thorsen, L. Interest and Preferences for Exercise Counselling and Programming among Norwegian Cancer Survivors. Eur. J. Cancer Care 2011, 20, 96–105. [Google Scholar] [CrossRef]
- Karvinen, K.H.; Courneya, K.S.; Venner, P.; North, S. Exercise Programming and Counseling Preferences in Bladder Cancer Survivors: A Population-Based Study. J. Cancer Surviv. 2007, 1, 27–34. [Google Scholar] [CrossRef]
- Nyrop, K.A.; Callahan, L.F.; Cleveland, R.J.; Arbeeva, L.L.; Hackney, B.S.; Muss, H.B. Randomized Controlled Trial of a Home-Based Walking Program to Reduce Moderate to Severe Aromatase Inhibitor-Associated Arthralgia in Breast Cancer Survivors. Oncologist 2017, 22, 1238–1249. [Google Scholar] [CrossRef]
- Chen, H.-M.; Tsai, C.-M.; Wu, Y.-C.; Lin, K.-C.; Lin, C.-C. Effect of Walking on Circadian Rhythms and Sleep Quality of Patients with Lung Cancer: A Randomised Controlled Trial. Br. J. Cancer 2016, 115, 1304–1312. [Google Scholar] [CrossRef]
- Lee, I.-M.; Buchner, D.M. The Importance of Walking to Public Health. Med. Sci. Sports Exerc. 2008, 40, S512–S518. [Google Scholar] [CrossRef]
- Bull, F.C.; Hardman, A.E. Walking: A Best Buy for Public and Planetary Health. Br. J. Sports Med. 2018, 52, 755–756. [Google Scholar] [CrossRef]
- Jones, L.W.; Courneya, K.S. Exercise Counseling and Programming Preferences of Cancer Survivors. Cancer Pract. 2002, 10, 208–215. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Malone, J.; Rao, K.; Courneya, K.S.; Fogleman, A.; Tippey, A.; Markwell, S.J.; Robbins, K.T. Exercise Preferences among Patients with Head and Neck Cancer: Prevalence and Associations with Quality of Life, Symptom Severity, Depression, and Rural Residence. Head Neck 2009, 31, 994–1005. [Google Scholar] [CrossRef]
- Toohey, K.; Pumpa, K.; McKune, A.; Cooke, J.; Semple, S. High-Intensity Exercise Interventions in Cancer Survivors: A Systematic Review Exploring the Impact on Health Outcomes. J. Cancer Res. Clin. Oncol. 2018, 144, 1–12. [Google Scholar] [CrossRef]
- Philip, E.J.; Coups, E.J.; Feinstein, M.B.; Park, B.J.; Wilson, D.J.; Ostroff, J.S. Physical Activity Preferences of Early-Stage Lung Cancer Survivors. Support Care Cancer 2014, 22, 495–502. [Google Scholar] [CrossRef]
- Wong, J.N.; McAuley, E.; Trinh, L. Physical Activity Programming and Counseling Preferences among Cancer Survivors: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 48. [Google Scholar] [CrossRef]
- Harrison, S.; Hayes, S.C.; Newman, B. Level of Physical Activity and Characteristics Associated with Change Following Breast Cancer Diagnosis and Treatment. Psychooncology 2009, 18, 387–394. [Google Scholar] [CrossRef]
- Fassier, P.; Zelek, L.; Partula, V.; Srour, B.; Bachmann, P.; Touillaud, M.; Druesne-Pecollo, N.; Galan, P.; Cohen, P.; Hoarau, H.; et al. Variations of Physical Activity and Sedentary Behavior between before and after Cancer Diagnosis. Medicine 2016, 95, e4629. [Google Scholar] [CrossRef]
- Coups, E.J.; Park, B.J.; Feinstein, M.B.; Steingart, R.M.; Egleston, B.L.; Wilson, D.J.; Ostroff, J.S. Physical Activity among Lung Cancer Survivors: Changes across the Cancer Trajectory and Associations with Quality of Life. Cancer Epidemiol. Biomark. Prev. 2009, 18, 664–672. [Google Scholar] [CrossRef]
- Chung, J.Y.; Lee, D.H.; Park, J.-H.; Lee, M.K.; Kang, D.-W.; Min, J.; Kim, D.-I.; Jeong, D.H.; Kim, N.K.; Meyerhardt, J.A.; et al. Patterns of Physical Activity Participation across the Cancer Trajectory in Colorectal Cancer Survivors. Support Care Cancer 2013, 21, 1605–1612. [Google Scholar] [CrossRef]
- Littman, A.J.; Tang, M.-T.; Rossing, M.A. Longitudinal Study of Recreational Physical Activity in Breast Cancer Survivors. J. Cancer Surviv. 2010, 4, 119–127. [Google Scholar] [CrossRef]
- Koebnick, C.; Michaud, D.; Moore, S.C.; Park, Y.; Hollenbeck, A.; Ballard-Barbash, R.; Schatzkin, A.; Leitzmann, M.F. Body Mass Index, Physical Activity, and Bladder Cancer in a Large Prospective Study. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1214–1221. [Google Scholar] [CrossRef]
- Edwards, E.S.; Sackett, S.C. Psychosocial Variables Related to Why Women Are Less Active than Men and Related Health Implications: Supplementary Issue: Health Disparities in Women. Clin. Med. Insights Womens Health 2016, 9, CMWH-S34668. [Google Scholar] [CrossRef]
- Do, K.-A.; Johnson, M.M.; Doherty, D.A.; Lee, J.J.; Wu, X.F.; Dong, Q.; Hong, W.K.; Khuri, F.R.; Fu, K.K.; Spitz, M.R. Second Primary Tumors in Patients with Upper Aerodigestive Tract Cancers: Joint Effects of Smoking and Alcohol (United States). Cancer Causes Control 2003, 14, 131–138. [Google Scholar] [CrossRef]
- LoConte, N.K.; Brewster, A.M.; Kaur, J.S.; Merrill, J.K.; Alberg, A.J. Alcohol and Cancer: A Statement of the American Society of Clinical Oncology. JCO 2018, 36, 83–93. [Google Scholar] [CrossRef]
- Allison, P.J. Factors Associated with Smoking and Alcohol Consumption Following Treatment for Head and Neck Cancer. Oral Oncol. 2001, 37, 513–520. [Google Scholar] [CrossRef]
- Gritz, E.R.; Carmack, C.L.; de Moor, C.; Coscarelli, A.; Schacherer, C.W.; Meyers, E.G.; Abemayor, E. First Year after Head and Neck Cancer: Quality of Life. J. Clin. Oncol. 1999, 17, 352–360. [Google Scholar] [CrossRef]
- Miller, P.M.; Day, T.A.; Ravenel, M.C. Clinical Implications of Continued Alcohol Consumption after Diagnosis of Upper Aerodigestive Tract Cancer. Alcohol. Alcohol. 2006, 41, 140–142. [Google Scholar] [CrossRef]
- Sanford, N.N.; Sher, D.J.; Xu, X.; Ahn, C.; D’Amico, A.V.; Aizer, A.A.; Mahal, B.A. Alcohol Use among Patients with Cancer and Survivors in the United States, 2000–2017. J. Natl. Compr. Cancer Netw. 2020, 18, 69–79. [Google Scholar] [CrossRef]
- Parker, A.S.; Cerhan, J.R.; Lynch, C.F.; Ershow, A.G.; Cantor, K.P. Gender, Alcohol Consumption, and Renal Cell Carcinoma. Am. J. Epidemiol. 2002, 155, 455–462. [Google Scholar] [CrossRef][Green Version]
- Bagnardi, V.; Blangiardo, M.; La Vecchia, C.; Corrao, G. Alcohol Consumption and the Risk of Cancer. Alcohol. Res. Health 2001, 25, 263–270. [Google Scholar]
- Trias-Llimós, S.; Janssen, F. Alcohol and Gender Gaps in Life Expectancy in Eight Central and Eastern European Countries. Eur. J. Public Health 2018, 28, 687–692. [Google Scholar] [CrossRef]
- Iwamoto, D.K.; Cheng, A.; Lee, C.S.; Takamatsu, S.; Gordon, D. “Man-Ing” up and Getting Drunk: The Role of Masculine Norms, Alcohol Intoxication and Alcohol-Related Problems among College Men. Addict. Behav. 2011, 36, 906–911. [Google Scholar] [CrossRef]
- Falk, R.T.; Pickle, L.W.; Brown, L.M.; Mason, T.J.; Buffler, P.A.; Fraumeni, J.F. Effect of Smoking and Alcohol Consumption on Laryngeal Cancer Risk in Coastal Texas. Cancer Res. 1989, 49, 4024–4029. [Google Scholar]
- Deleyiannis, F.W.; Thomas, D.B.; Vaughan, T.L.; Davis, S. Alcoholism: Independent Predictor of Survival in Patients with Head and Neck Cancer. J. Natl. Cancer Inst. 1996, 88, 542–549. [Google Scholar] [CrossRef]
- Spies, C.D.; Rommelspacher, H. Alcohol Withdrawal in the Surgical Patient: Prevention and Treatment. Anesth. Analg. 1999, 88, 946–954. [Google Scholar] [CrossRef]
- Spies, C.D.; Neuner, B.; Neumann, T.; Blum, S.; Müller, C.; Rommelspacher, H.; Rieger, A.; Sanft, C.; Specht, M.; Hannemann, L.; et al. Intercurrent Complications in Chronic Alcoholic Men Admitted to the Intensive Care Unit Following Trauma. Intensive Care Med. 1996, 22, 286–293. [Google Scholar] [CrossRef]
- Dikshit, R.P.; Boffetta, P.; Bouchardy, C.; Merletti, F.; Crosignani, P.; Cuchi, T.; Ardanaz, E.; Brennan, P. Risk Factors for the Development of Second Primary Tumors among Men after Laryngeal and Hypopharyngeal Carcinoma. Cancer 2005, 103, 2326–2333. [Google Scholar] [CrossRef]
- Chow, W.-H.; Dong, L.M.; Devesa, S.S. Epidemiology and Risk Factors for Kidney Cancer. Nat. Rev. Urol. 2010, 7, 245–257. [Google Scholar] [CrossRef]
- Burris, J.L.; Studts, J.L.; DeRosa, A.P.; Ostroff, J.S. Systematic Review of Tobacco Use after Lung or Head/Neck Cancer Diagnosis: Results and Recommendations for Future Research. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1450–1461. [Google Scholar] [CrossRef]
- Islami, F.; Torre, L.A.; Jemal, A. Global Trends of Lung Cancer Mortality and Smoking Prevalence. Transl. Lung Cancer Res. 2015, 4, 327–338. [Google Scholar] [CrossRef]
- Lundborg, P.; Andersson, H. Gender, Risk Perceptions, and Smoking Behavior. J. Health Econ. 2008, 27, 1299–1311. [Google Scholar] [CrossRef]
- Torres, O.V.; O’Dell, L.E. Stress Is a Principal Factor That Promotes Tobacco Use in Females. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 65, 260–268. [Google Scholar] [CrossRef]
- Allen, A.M.; Oncken, C.; Hatsukami, D. Women and Smoking: The Effect of Gender on the Epidemiology, Health Effects, and Cessation of Smoking. Curr. Addict. Rep. 2014, 1, 53–60. [Google Scholar] [CrossRef]
- Branstetter, S.A.; Blosnich, J.; Dino, G.; Nolan, J.; Horn, K. Gender Differences in Cigarette Smoking, Social Correlates and Cessation among Adolescents. Addict. Behav. 2012, 37, 739–742. [Google Scholar] [CrossRef]
- Tabei, S.Z.; Heydari, S.T.; Mehrabani, D.; Shamsina, S.J.; Ahmadi, J.; Firouzi, S.M. Current Substance Use in Patients with Gastric Cancer in Southern Iran. J. Cancer Res. Ther. 2006, 2, 182. [Google Scholar] [CrossRef]
- Garces, Y.I.; Yang, P.; Parkinson, J.; Zhao, X.; Wampfler, J.A.; Ebbert, J.O.; Sloan, J.A. The Relationship between Cigarette Smoking and Quality of Life after Lung Cancer Diagnosis. Chest 2004, 126, 1733–1741. [Google Scholar] [CrossRef]
- Cosgrove, K.P.; Wang, S.; Kim, S.-J.; McGovern, E.; Nabulsi, N.; Gao, H.; Labaree, D.; Tagare, H.D.; Sullivan, J.M.; Morris, E.D. Sex Differences in the Brain’s Dopamine Signature of Cigarette Smoking. J. Neurosci. 2014, 34, 16851–16855. [Google Scholar] [CrossRef]
- de Almeida, A.Á.; Bandeira, C.M.; Gonçalves, A.J.; Araújo, A.J. Nicotine Dependence and Smoking Habits in Patients with Head and Neck Cancer. J. Bras. Pneumol. 2014, 40, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Simmons, V.N.; Litvin, E.B.; Jacobsen, P.B.; Patel, R.D.; McCaffrey, J.C.; Oliver, J.A.; Sutton, S.K.; Brandon, T.H. Predictors of Smoking Relapse in Patients with Thoracic Cancer or Head and Neck Cancer. Cancer 2013, 119, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, L.R.; Meade, C.D.; Diaz, D.B.; Carrington, M.S.; Brandon, T.H.; Jacobsen, P.B.; McCaffrey, J.C.; Haura, E.B.; Simmons, V.N. Development of a Targeted Smoking Relapse-Prevention Intervention for Cancer Patients. J. Cancer Educ. 2018, 33, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.; Miller, L.-A.; Saad, A.; Abraham, J. Smoking Behaviors Among Cancer Survivors: An Observational Clinical Study. JOP 2009, 5, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Pudkasam, S.; Polman, R.; Pitcher, M.; Fisher, M.; Chinlumprasert, N.; Stojanovska, L.; Apostolopoulos, V. Physical Activity and Breast Cancer Survivors: Importance of Adherence, Motivational Interviewing and Psychological Health. Maturitas 2018, 116, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Azemmour, Y.; Boutayeb, S.; Beddaa, H.; Errihani, H. Physical Activity in Cancer Care: Barriers and Interventions. Pan Afr. Med. J. 2022, 43, 131. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, C.E.; Hyde, M.K.; Cooper, E.T.; Stennett, R.C.; Gomersall, S.R.; Skinner, T.L. Physical Activity Behaviour Change in People Living with and beyond Cancer Following an Exercise Intervention: A Systematic Review. J. Cancer Surviv. 2023, 17, 569–594. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.; Paul, R.; Marin-Chollom, A.M.; Ogden Gaffney, A.; Sepulveda, J.; Dominguez, N.; Gray, H.; Haase, A.M.; Hershman, D.L.; Koch, P.; et al. Developing a Diet and Physical Activity Intervention for Hispanic/Latina Breast Cancer Survivors. Cancer Control 2022, 29, 107327482211339. [Google Scholar] [CrossRef] [PubMed]
- Bertholet, N.; Daeppen, J.-B.; Wietlisbach, V.; Fleming, M.; Burnand, B. Reduction of Alcohol Consumption by Brief Alcohol Intervention in Primary Care: Systematic Review and Meta-Analysis. Arch. Intern. Med. 2005, 165, 986–995. [Google Scholar] [CrossRef]
- Scharer, J.L.; Funderburk, J.S.; De Vita, M.J.; Rother, Y.; Maisto, S.A. Treatment-As-Usual Control Groups in Brief Alcohol Intervention Trials: A Systematic Review and Meta-Analysis. J. Stud. Alcohol. Drugs 2022, 83, 934–943. [Google Scholar] [CrossRef]
- Barticevic, N.A.; Poblete, F.; Zuzulich, S.M.; Rodriguez, V.; Quevedo, D.; Sena, B.F.; Bradshaw, L. A Health Technician-Delivered Brief Intervention Linked to AUDIT for Reduction of Alcohol Use in Chilean Primary Care: A Randomized Controlled Trial. Addict. Sci. Clin. Pract. 2021, 16, 39. [Google Scholar] [CrossRef]
- Hartmann-Boyce, J.; Livingstone-Banks, J.; Ordóñez-Mena, J.M.; Fanshawe, T.R.; Lindson, N.; Freeman, S.C.; Sutton, A.J.; Theodoulou, A.; Aveyard, P. Behavioural Interventions for Smoking Cessation: An Overview and Network Meta-Analysis. Cochrane Database Syst. Rev. 2021, 1, CD013229. [Google Scholar] [CrossRef]
- Bricker, J.B.; Watson, N.L.; Mull, K.E.; Sullivan, B.M.; Heffner, J.L. Efficacy of Smartphone Applications for Smoking Cessation: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1472–1480. [Google Scholar] [CrossRef] [PubMed]
- Díaz, D.B.; Brandon, T.H.; Sutton, S.K.; Meltzer, L.R.; Hoehn, H.J.; Meade, C.D.; Jacobsen, P.B.; McCaffrey, J.C.; Haura, E.B.; Lin, H.-Y.; et al. Smoking Relapse-Prevention Intervention for Cancer Patients: Study Design and Baseline Data from the Surviving SmokeFree Randomized Controlled Trial. Contemp. Clin. Trials 2016, 50, 84–89. [Google Scholar] [CrossRef] [PubMed]
- GUS—Bank Danych Lokalnych. Available online: https://bdl.stat.gov.pl/bdl/dane/teryt/jednostka# (accessed on 22 December 2023).
- Deuker, M.; Stolzenbach, L.F.; Collà Ruvolo, C.; Nocera, L.; Tian, Z.; Roos, F.C.; Becker, A.; Kluth, L.A.; Tilki, D.; Shariat, S.F.; et al. Bladder Cancer Stage and Mortality: Urban vs. Rural Residency. Cancer Causes Control 2021, 32, 139–145. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total, N = 128 [IQR], (%) |
|---|---|
| Age | 51.5 [43.5–60.5] |
| Gender | |
| Male | 80 (62.5) |
| Female | 48 (37.5) |
| Place of residence | |
| Rural area | 18 (14.1) |
| City <50,000 * | 23 (18.0) |
| City 50,000–100,000 * | 34 (26.6) |
| City 100,000+ * | 53 (41.1) |
| Education | |
| Primary | 2 (1.6) |
| Vocational | 11 (8.6) |
| Secondary | 50 (39.1) |
| Higher | 65 (50.8) |
| Employment situation | |
| Employed | 99 (77.3) |
| Unemployed | 21 (16.4) |
| Retired | 4 (3.1) |
| Studying | 4 (3.1) |
| Time since diagnosis | |
| <1 year | 35 (27.3) |
| 1–2 years | 40 (31.3) |
| 2–3 years | 38 (29.7) |
| >3 years | 15 (11.7) |
| <1 Year, N = 35 | 1–2 Years, N = 40 | 2–3 Years, N = 38 | >3 Years, N = 15 | p-Value | Effect Size | |
|---|---|---|---|---|---|---|
| Physical activity MET-m/w | ||||||
| Walking MET-m/w | 693.0 1 [346.5–1386.0 2] | 429.0 [346.5–693.0] | 462.0 [297.0–1039.0] | 462.0 [346.5–924.9] | p = 0.32 | η2 = 0.00 |
| Moderate MET-m/w | 180.0 [0.0–720.0] | 0 [0.0–210.0] | 0 [0.0–240.0] | 240.0 [0.0–560.0] | p = 0.01 | η2 = 0.06 |
| Vigorous MET-m/w | 0 [0.0–1440.0] | 0 [0.0–0.0] | 0 [0.0–0.0] | 0 [0.0–2000.0] | p < 0.0001 | η2 = 0.16 |
| Total MET-m/w | 2826.0 [471.0–3672.0] | 462.0 [346.5–993.0] | 629.0 [438.0–1386.0] | 693.0 [346.5–4266.0] | p = 0.01 | η2 = 0.07 |
| Physical activity level | ||||||
| Inactive | 11 (31.4 3) | 22 (55.0) | 17 (44.7) | 6 (40.0) | p < 0.0001 | |
| Minimally active | 7 (20.0) | 17 (42.5) | 17 (44.7) | 4 (26.7) | V = 0.19 | |
| HEPA | 17 (48.6) | 1 (2.5) | 4 (10.5) | 5 (33.3) |
| <1 Year, N = 35 | 1–2 Years, N = 40 | 2–3 Years, N = 38 | >3 Years, N = 15 | p-Value 1 | Effect Size | |
|---|---|---|---|---|---|---|
| Walking MET-m/w | ||||||
| Male | 1180.0 3 [693.0–2772.0 4] | 462.0 [346.5–693.0] | 462.0 [297.0–1039.0] | 462.0 [346.5–924.0] | p = 0.002 | η2 = 0.16 |
| Female | 330.0 [0.0–346.5] | 396.0 [346.5–693.0] | 346.5 [297.0–577.5] | 346.5 [231.0–693.0] | p = 0.03 | η2 = 0.13 |
| p-Value 2 | p < 0.0001 | p = 0.64 | p = 0.20 | p = 0.31 | ||
| Effect size | r = 0.36 | r = 0.04 | r = 0.11 | r = 0.09 | ||
| Moderate MET-m/w | ||||||
| Male | 300.0 [50.0–1320.0] | 0.0 [0.0–0.0] | 120.0 [0.0–180.0] | 420.0 [0.0–1000.0] | p = 0.004 | η2 = 0.14 |
| Female | 80.0 [0.0–240.0] | 0.0 [0.0–240.0] | 0.0 [0.0–240.0] | 0.0 [0.0–0.0] | p = 0.47 | η2 = 0.00 |
| p-Value | p = 0.04 | p = 0.27 | p = 0.36 | p = 0.08 | ||
| Effect size | r = 0.19 | r = 0.08 | r = 0.08 | r = 0.15 | ||
| Vigorous MET-m/w | ||||||
| Male | 800.0 [0.0–2040.0] | 0.0 [0.0–0.0] | 0.0 [0.0–0.0] | 0.0 [0.0–2200.0] | p < 0.0001 | η2 = 0.33 |
| Female | 0.0 [0.0–0.0] | 0.0 [0.0–0.0] | 0.0 [0.0–0.0] | 0.0 [0.0–0.0] | p = 0.52 | η2 = 0.00 |
| p-Value | p = 0.0006 | p = 0.68 | p = 0.21 | p = 0.23 | ||
| Effect size | r = 0.03 | r = 0.02 | r = 0.11 | r = 0.11 | ||
| Total MET-m/w | ||||||
| Male | 3273.0 [2599.5–6453.0] | 462.0 [346.5–693.0] | 636.0 [438.0–1546.5] | 882.0 [404.25–4799.0] | p < 0.0001 | η2 = 0.28 |
| Female | 330.0 [0.0–586.5] | 636.0 [346.5–1117.5] | 586.5 [577.5–857.5] | 346.5 [231.0–693.0 | p = 0.08 | η2 = 0.09 |
| p-Value | p < 0.0001 | p = 0.41 | p = 0.55 | p = 0.11 | ||
| Effect size | r = 0.38 | r = 0.07 | r = 0.05 | r = 0.14 |
| <1 Year, N = 35 | 1–2 Years, N = 40 | 2–3 Years, N = 38 | >3 Years, N = 15 | p-Value | Effect Size | |
|---|---|---|---|---|---|---|
| Physical activity level—male | ||||||
| Inactive | 2 (8.3 1) | 12 (63.2) | 10 (40.0) | 4 (33.3) | p < 0.0001 | |
| Minimally active | 5 (20.8) | 6 (31.6) | 11 (44.0) | 3 (25.0) | V = 0.24 | |
| HEPA | 17 (70.8) | 1 (5.3) | 4 (16.0) | 5 (41.7) | ||
| Physical activity level—female | ||||||
| Inactive | 9 (81.8) | 10 (47.6) | 7 (53.9) | 2 (66.7) | p = 0.30 | |
| Minimally active | 2 (18.2) | 11 (52.4) | 6 (46.2) | 1 (33.3) | V = 0.16 | |
| HEPA | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| <1 Year, N = 35 | 1–2 Years, N = 40 | 2–3 Years, N = 38 | >3 Years, N = 15 | p-Value 1 | Effect Size | |
|---|---|---|---|---|---|---|
| Do you ever drink alcohol? | ||||||
| Yes | 15 (42.9 5) | 22 (55.0) | 21 (55.3) | 12 (80.0) | p = 0.12 | V = 0.12 |
| No | 20 (57.1) | 18 (45.0) | 17 (44.7) | 3 (20.0) | ||
| AUDIT points | 4.20 3 (2.02–6.38 4) | 2.00 (1.57–2.43) | 3.33 (2.42–4.25) | 3.67 (2.84–4.49) | p = 0.01 | η2 = 0.12 |
| AUDIT points | ||||||
| Male | 4.92 3 (2.31–7.52 4) | 2.50 (1.86–3.14) | 3.35 (2.39–4.31) | 3.91 (3.21–4.61) | p = 0.12 | η2 = 0.05 |
| Female | 1.33 (0.0–2.78) | 1.40 (1.03–1.77) | 3.0 (3.0–3.0) | 1.0 (1.0–1.0) | p = 0.26 | η2 = 0.09 |
| p-Value 2 | p = 0.045 | p = 0.01 | p = 1.00 | p = 1.00 | ||
| Effect size | r = 0.52 | r = 0.54 | r = 0.00 | r = 0.00 | ||
| AUDIT level | ||||||
| Low risk drinking | 13 (86.7 5) | 12 (100.0) | 21 (100.0) | 12 (100.0) | p = 0.06 | V = 0.19 |
| Medium risk drinking | 2 (13.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| <1 Year, N = 35 | 1–2 Years, N = 40 | 2–3 Years, N = 38 | >3 Years, N = 15 | p-Value 1 | Effect Size | |
|---|---|---|---|---|---|---|
| Do you smoke cigarettes? | ||||||
| Yes | 6 (17.1 5) | 12 (30.0) | 12 (31.6) | 4 (26.7) | p = 0.51 | V = 0.08 |
| No | 29 (82.9) | 28 (70.0) | 26 (68.4) | 11 (73.3) | ||
| Fagerström points | 4.83 3 (2.80–6.87 4) | 2.42 (1.58–3.25) | 4.17 (2.54–5.79) | 3.75 (0.47–7.03) | p = 0.08 | η2 = 0.12 |
| Fagerström points | ||||||
| Male | 5.40 3 (3.52–7.28 4) | 2.29 (1.41.–3.17) | 4.80 (3.16–6.45) | 3.75 (0.47–7.03) | p = 0.02 | η2 = 0.30 |
| Female | 2.00 (2.00–2.00) | 2.60 (0.34–4.86) | 1.00 (1.00–1.00) | 0.0 (0.0–0.0) | p = 0.36 | η2 = 0.00 |
| p-Value 2 | p = 1.00 | p = 0.93 | p = 0.10 | p = 1.00 | ||
| Effect size | r = 0.00 | r = 0.02 | r = 0.48 | r = 0.00 | ||
| Fagerström level | ||||||
| Low dependence (0–3 points) | 1 (16.7 5) | 10 (83.3) | 4 (33.3) | 1 (25.0) | ||
| Moderate dependence (4–6 points) | 3 (50.0) | 2 (16.7) | 7 (58.3) | 3 (75.0) | p = 0.03 | V = 0.19 |
| High dependance (7–10 points) | 2 (33.3) | 0 (0.0) | 1 (8.3) | 0 (0.0) |
| Variables | Estimate | Standard Error | aOR | 95% CI for aOR | p-Value |
|---|---|---|---|---|---|
| Intercept | −2.780 | 1.025 | 0.062 | 0.008–0.463 | 0.007 |
| Age | 0.039 | 0.015 | 1.040 | 1.009–1.072 | 0.0120 |
| Gender | |||||
| Female | Reference | Reference | Reference | Reference | Reference |
| Male | −0.956 | 0.375 | 0.385 | 0.184–0.802 | 0.0108 |
| Place of residence | |||||
| City 100,000+ * | Reference | Reference | Reference | Reference | Reference |
| City 50,000–100,000 * | 0.303 | 0.444 | 1.354 | 0.568–3.232 | 0.4941 |
| City <50,000 * | −0.405 | 0.533 | 0.667 | 0.234–1.895 | 0.4469 |
| Rural area | 1.114 | 0.573 | 3.048 | 0.990–9.378 | 0.0520 |
| Time since diagnosis | |||||
| <1 year | Reference | Reference | Reference | Reference | Reference |
| 1–2 years | 0.981 | 0.483 | 2.667 | 1.034–6.877 | 0.0424 |
| 2–3 years | 0.569 | 0.489 | 1.766 | 0.677–4.605 | 0.2446 |
| >3 years | 0.375 | 0.641 | 1.455 | 0.414–5.105 | 0.5586 |
| Do you drink alcohol? | |||||
| No | Reference | Reference | Reference | Reference | Reference |
| Yes | −0.336 | 0.359 | 0.714 | 0.354–1.442 | 0.3481 |
| Do you smoke cigarettes? | |||||
| No | Reference | Reference | Reference | Reference | Reference |
| Yes | 0.344 | 0.402 | 1.410 | 0.642–3.100 | 0.3923 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamczak, B.B.; Kuźnik, Z.; Makles, S.; Wasilewski, A.; Kosendiak, A.A. Physical Activity, Alcohol, and Cigarette Use in Urological Cancer Patients over Time since Diagnosis. Healthcare 2024, 12, 59. https://doi.org/10.3390/healthcare12010059
Adamczak BB, Kuźnik Z, Makles S, Wasilewski A, Kosendiak AA. Physical Activity, Alcohol, and Cigarette Use in Urological Cancer Patients over Time since Diagnosis. Healthcare. 2024; 12(1):59. https://doi.org/10.3390/healthcare12010059
Chicago/Turabian StyleAdamczak, Bartosz Bogusz, Zofia Kuźnik, Szymon Makles, Andrzej Wasilewski, and Aureliusz Andrzej Kosendiak. 2024. "Physical Activity, Alcohol, and Cigarette Use in Urological Cancer Patients over Time since Diagnosis" Healthcare 12, no. 1: 59. https://doi.org/10.3390/healthcare12010059
APA StyleAdamczak, B. B., Kuźnik, Z., Makles, S., Wasilewski, A., & Kosendiak, A. A. (2024). Physical Activity, Alcohol, and Cigarette Use in Urological Cancer Patients over Time since Diagnosis. Healthcare, 12(1), 59. https://doi.org/10.3390/healthcare12010059