



A Systematic Literature Review of Health Information Systems for Healthcare


Abstract
1. Introduction
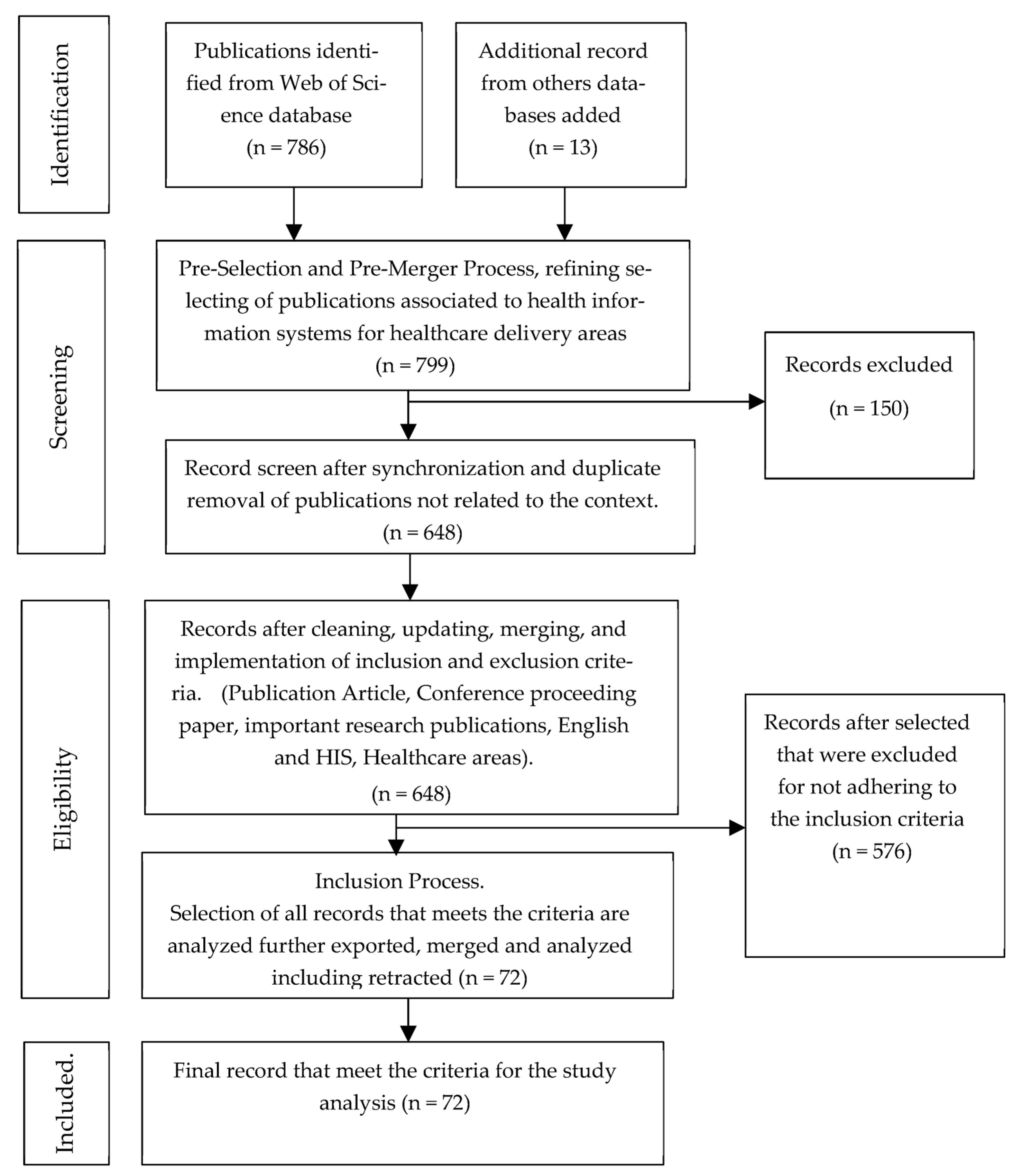
2. Material and Method
3. Discussion
3.1. The Evolution of Health Information Systems
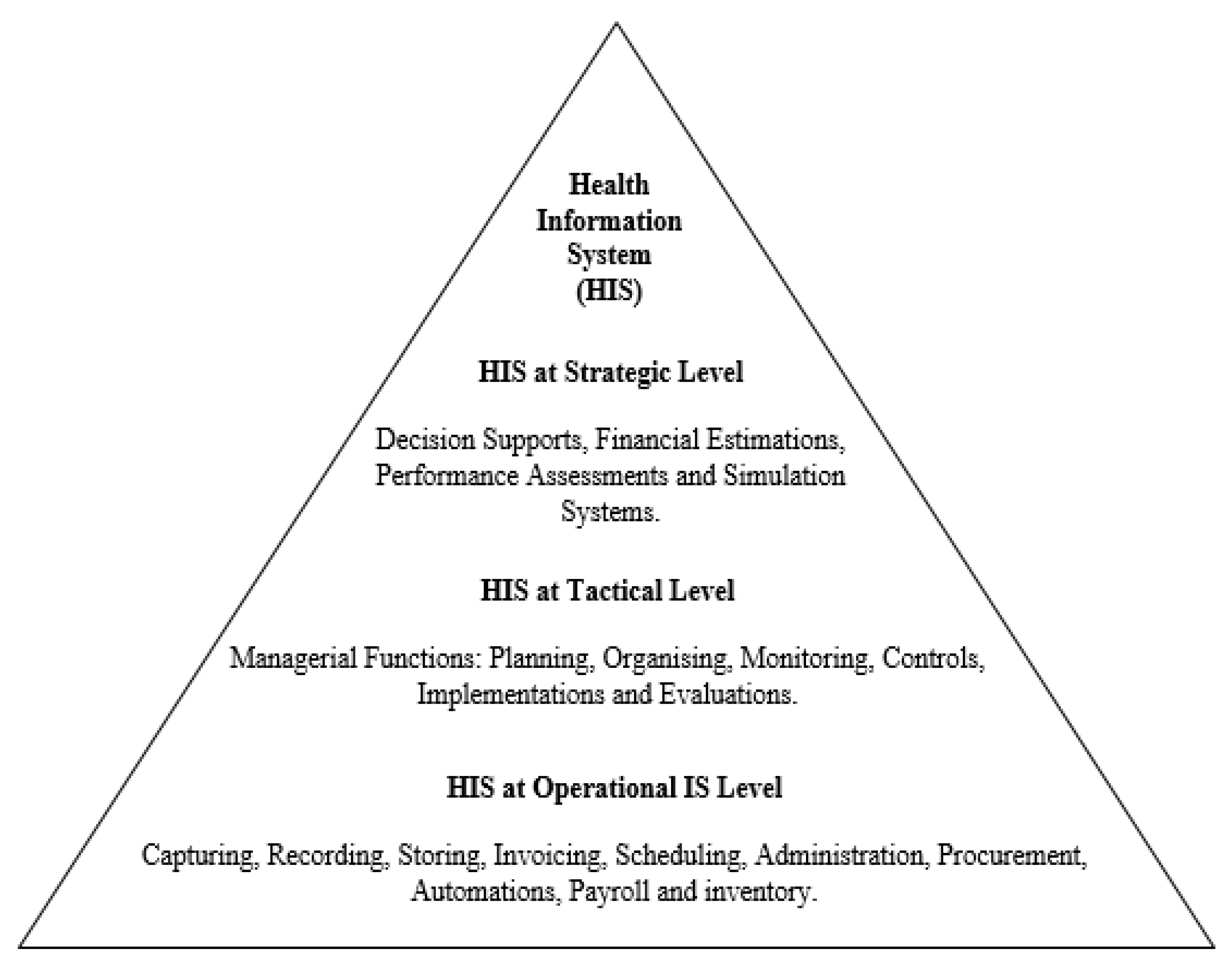
3.2. HIS Structural Deployment
3.3. Health Information Systems Benefits
3.4. Information System and Knowledge Management in the Healthcare Arena
3.4.1. Information System
3.4.2. Knowledge Management
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sahay, S.; Nielsen, P.; Latifov, M. Grand challenges of public health: How can health information systems support facing them? Health Policy Technol. 2018, 7, 81–87. [Google Scholar] [CrossRef]
- English, R.; Masilela, T.; Barron, P.; Schonfeldt, A. Health information systems in South Africa. S. Afr. Health Rev. 2011, 2011, 81–89. [Google Scholar]
- Bagayoko, C.O.; Tchuente, J.; Traoré, D.; Moukoumbi Lipenguet, G.; Ondzigue Mbenga, R.; Koumamba, A.P.; Ondjani, M.C.; Ndjeli, O.L.; Gagnon, M.P. Implementation of a national electronic health information system in Gabon: A survey of healthcare providers’ perceptions. BMC Med. Inform. Decis. Mak. 2020, 20, 202. [Google Scholar] [CrossRef] [PubMed]
- Berrueta, M.; Bardach, A.; Ciaponni, A.; Xiong, X.; Stergachis, A.; Zaraa, S.; Buekens, P. Maternal and neonatal data collection systems in low- and middle-income countries: Scoping review protocol. Gates Open Res. 2020, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Flora, O.C.; Margaret, K.; Dan, K. Perspectives on utilization of community based health information systems in Western Kenya. Pan Afr. Med. J. 2017, 27, 180. [Google Scholar] [CrossRef]
- Rachmani, E.; Lin, M.C.; Hsu, C.Y.; Jumanto, J.; Iqbal, U.; Shidik, G.F.; Noersasongko, E. The implementation of an integrated e-leprosy framework in a leprosy control program at primary health care centers in Indonesia. Int. J. Med. Inform. 2020, 140, 104155. [Google Scholar] [CrossRef]
- Almunawar, M.N.; Anshari, M. Health information systems (HIS): Concept and technology. arXiv 2012, arXiv:1203.3923. [Google Scholar]
- Haule, C.D.; Muhanga, M.; Ngowi, E. The what, why, and how of health information systems: A systematic review. Sub Sahar. J. Soc. Sci. Humanit. 2022, 1, 37–43. Available online: http://41.73.194.142/bitstream/handle/123456789/4398/Paper%205.pdf?sequence=1&isAllowed=y (accessed on 1 February 2023).
- Epizitone, A.; Moyane, S.P.; Agbehadji, I.E. Health Information System and Health Care Applications Performance in the Healthcare Arena: A Bibliometric Analysis. Healthcare 2022, 10, 2273. [Google Scholar] [CrossRef]
- Haux, R. Health information systems–past, present, future. Int. J. Med. Inform. 2006, 75, 268–281. [Google Scholar] [CrossRef]
- Malaquias, R.S.; Filho, I.M.B. Middleware for Healthcare Systems: A Systematic Mapping. In Proceedings of the 21st International Conference on Computational Science and Its Applications, ICCSA 2021, Cagliari, Italy, 13–16 September 2021; Gervasi, O., Murgante, B., Misra, S., Garau, C., Blecic, I., Taniar, D., Apduhan, B.O., Rocha, A.M., Tarantino, E., Torre, C.M., Eds.; Springer Science and Business Media Deutschland GmbH: Cham, Switzerland, 2021; Volume 12957, pp. 394–409. [Google Scholar] [CrossRef]
- Lippeveld, T. Routine health information systems: The glue of a unified health system. In Proceedings of the Keynote address at the Workshop on Issues and Innovation in Routine Health Information in Developing Countries, Potomac, MD, USA, 14–16 March 2001. [Google Scholar]
- AbouZahr, C.; Boerma, T. Health information systems: The foundations of public health. Bull. World Health Organ. 2005, 83, 578–583. [Google Scholar]
- Bogaert, P.; Van Oyen, H. An integrated and sustainable EU health information system: National public health institutes’ needs and possible benefits. Arch. Public Health 2017, 75, 3. [Google Scholar] [CrossRef]
- Bogaert, P.; van Oers, H.; Van Oyen, H. Towards a sustainable EU health information system infrastructure: A consensus driven approach. Health Policy 2018, 122, 1340–1347. [Google Scholar] [CrossRef]
- Panerai, R. Health Information Systems; Global Perspective of Heath; Department of Medical Physics, University of Leicester: Leicester, UK, 2014; pp. 1–6. [Google Scholar]
- Garcia, A.P.; De la Vega, S.F.; Mercado, S.P. Health Information Systems for Older Persons in Select Government Tertiary Hospitals and Health Centers in the Philippines: Cross-sectional Study. J. Med. Internet Res. 2022, 24, e29541. [Google Scholar] [CrossRef]
- Epizitone, A. Framework to Develop a Resilient and Sustainable Integrated Information System for Health Care Applications: A Review. Int. J. Adv. Comput. Sci. Appl. (IJACSA) 2022, 13, 477–481. [Google Scholar] [CrossRef]
- Walcott-Bryant, A.; Ogallo, W.; Remy, S.L.; Tryon, K.; Shena, W.; Bosker-Kibacha, M. Addressing Care Continuity and Quality Challenges in the Management of Hypertension: Case Study of the Private Health Care Sector in Kenya. J. Med. Internet Res. 2021, 23, e18899. [Google Scholar] [CrossRef]
- Malekzadeh, S.; Hashemi, N.; Sheikhtaheri, A.; Hashemi, N.S. Barriers for Implementation and Use of Health Information Systems from the Physicians’ Perspectives. Stud. Health Technol. Inform. 2018, 251, 269–272. [Google Scholar]
- Tossy, T. Major challenges and constraint of integrating health information systems in african countries: A Namibian experience. Int. J. Inf. Commun. Technol. 2014, 4, 273–279. Available online: https://www.researchgate.net/profile/Titus-Tossy-2/publication/272163842_Major_Challenges_and_Constraint_of_Integrating_Health_Information_Systems_in_African_Countries_A_Namibian_Experience/links/54dca52b0cf28a3d93f8233d/Major-Challenges-and-Constraint-of-Integrating-Health-Information-Systems-in-African-Countries-A-Namibian-Experience.pdf (accessed on 1 February 2023).
- Vaganova, E.; Ishchuk, T.; Zemtsov, A.; Zhdanov, D. Health Information Systems: Background and Trends of Development Worldwide and in Russia. In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies-Volume 5: HEALTHINF, (BIOSTEC 2017), Porto, Portugal, 21–23 February 2017; pp. 424–428. [Google Scholar] [CrossRef]
- Thomas, J.; Carlson, R.; Cawley, M.; Yuan, Q.; Fleming, V.; Yu, F. The Gap Between Technology and Ethics, Especially in Low-and Middle-Income Country Health Information Systems: A Bibliometric Study. Stud. Health Technol. Inform. 2022, 290, 902–906. [Google Scholar] [PubMed]
- Namageyo-Funa, A.; Aketch, M.; Tabu, C.; MacNeil, A.; Bloland, P. Assessment of select electronic health information systems that support immunization data capture—Kenya, 2017. BMC Health Serv. Res. 2018, 18, 621. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, M.H.; Venkateswaran, M.; Abu Khader, K.; Awwad, T.; Ghanem, B.; Hijaz, T.; Morkrid, K.; Froen, J.F. eRegTime, Efficiency of Health Information Management Using an Electronic Registry for Maternal and Child Health: Protocol for a Time-Motion Study in a Cluster Randomized Trial. JMIR Res. Protoc. 2019, 8, e13653. [Google Scholar] [CrossRef]
- Tummers, J.; Tekinerdogan, B.; Tobi, H.; Catal, C.; Schalk, B. Obstacles and features of health information systems: A systematic literature review. Comput. Biol. Med. 2021, 137, 104785. [Google Scholar] [CrossRef]
- Malik, M.; Kazi, A.F.; Hussain, A. Adoption of health technologies for effective health information system: Need of the hour for Pakistan. PLoS ONE 2021, 16, e0258081. [Google Scholar] [CrossRef]
- De Carvalho Junior, M.A.; Bandiera-Paiva, P. Health Information System Role-Based Access Control Current Security Trends and Challenges. J. Healthc Eng. 2018, 2018, 6510249. [Google Scholar] [CrossRef] [PubMed]
- Taye, G. Improving health care services through enhanced Health Information System: Human capacity development Model. Ethiop. J. Health Dev. 2021, 35, 42–49. Available online: https://www.ajol.info/index.php/ejhd/article/view/210752 (accessed on 1 February 2023).
- Sligo, J.; Gauld, R.; Roberts, V.; Villa, L. A literature review for large-scale health information system project planning, implementation and evaluation. Int. J. Med. Inform. 2017, 97, 86–97. [Google Scholar] [CrossRef]
- Bosch-Capblanch, X.; Oyo-Ita, A.; Muloliwa, A.M.; Yapi, R.B.; Auer, C.; Samba, M.; Gajewski, S.; Ross, A.; Krause, L.K.; Ekpenyong, N.; et al. Does an innovative paper-based health information system (PHISICC) improve data quality and use in primary healthcare? Protocol of a multicountry, cluster randomised controlled trial in sub-Saharan African rural settings. BMJ Open 2021, 11, e051823. [Google Scholar] [CrossRef]
- Suresh, L.; Singh, S.N. Studies in ICT and Health Information System. Int. J. Inf. Libr. Soc. 2014, 3, 16–24. [Google Scholar]
- Isleyen, F.; Ulgu, M.M. Data Transfer Model for HIS and Developers Opinions in Turkey. Stud. Health Technol. Inform. 2020, 270, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, C.; Pagano, M.; Hemingway, J.; Valadez, J.J. Hybrid prevalence estimation: Method to improve intervention coverage estimations. Proc. Natl. Acad. Sci. USA 2018, 115, 13063–13068. [Google Scholar] [CrossRef] [PubMed]
- Sawadogo-Lewis, T.; Keita, Y.; Wilson, E.; Sawadogo, S.; Téréra, I.; Sangho, H.; Munos, M. Can We Use Routine Data for Strategic Decision Making? A Time Trend Comparison Between Survey and Routine Data in Mali. Glob. Health Sci. Pract. 2021, 9, 869–880. [Google Scholar] [CrossRef]
- Kpobi, L.; Swartz, L.; Ofori-Atta, A.L. Challenges in the use of the mental health information system in a resource-limited setting: Lessons from Ghana. BMC Health Serv. Res. 2018, 18, 98. [Google Scholar] [CrossRef] [PubMed]
- Feteira-Santos, R.; Camarinha, C.; Nobre, M.D.; Elias, C.; Bacelar-Nicolau, L.; Costa, A.S.; Furtado, C.; Nogueira, P.J. Improving morbidity information in Portugal: Evidence from data linkage of COVID-19 cases surveillance and mortality systems. Int. J. Med. Inform. 2022, 163, 104763. [Google Scholar] [CrossRef]
- Ker, J.I.; Wang, Y.C.; Hajli, N. Examining the impact of health information systems on healthcare service improvement: The case of reducing in patient-flow delays in a US hospital. Technol. Forecast. Soc. Chang. 2018, 127, 188–198. [Google Scholar] [CrossRef]
- Alahmar, A.; AlMousa, M.; Benlamri, R. Automated clinical pathway standardization using SNOMED CT- based semantic relatedness. Digital Health 2022, 8, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Krasuska, M.; Williams, R.; Sheikh, A.; Franklin, B.; Hinder, S.; TheNguyen, H.; Lane, W.; Mozaffar, H.; Mason, K.; Eason, S.; et al. Driving digital health transformation in hospitals: A formative qualitative evaluation of the English Global Digital Exemplar programme. BMJ Health Care Inform. 2021, 28, e100429. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.J.; Browne, A.; Haworth, S.; Wurie, F.; Campos-Matos, I. Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement. Int. J. Environ. Res. Public Health 2021, 18, 10331. [Google Scholar] [CrossRef] [PubMed]
- See, E.J.; Bello, A.K.; Levin, A.; Lunney, M.; Osman, M.A.; Ye, F.; Ashuntantang, G.E.; Bellorin-Font, E.; Benghanem Gharbi, M.; Davison, S.; et al. Availability, coverage, and scope of health information systems for kidney care across world countries and regions. Nephrol. Dial. Transplant. 2022, 37, 159–167. [Google Scholar] [CrossRef]
- Nyangena, J.; Rajgopal, R.; Ombech, E.A.; Oloo, E.; Luchetu, H.; Wambugu, S.; Kamau, O.; Nzioka, C.; Gwer, S.; Ndirangu, M.N. Maturity assessment of Kenya’s health information system interoperability readiness. BMJ Health Care Inform. 2021, 28, e100241. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Duftschmid, G.; Al-Hamdan, Z.; Bawadi, H.; Cheung, N.T.; Cho, K.H.; Goldfarb, G.; Gulkesen, K.H.; Harel, N.; Kimura, M.; et al. International Comparison of Six Basic eHealth Indicators Across 14 Countries: An eHealth Benchmarking Study. Methods Inf. Med. 2020, 59, e46–e63. [Google Scholar] [CrossRef] [PubMed]
- Tummers, J.; Tobi, H.; Schalk, B.; Tekinerdogan, B.; Leusink, G. State of the practice of health information systems: A survey study amongst health care professionals in intellectual disability care. BMC Health Serv. Res. 2021, 21, 1247. [Google Scholar] [CrossRef]
- Steil, J.; Finas, D.; Beck, S.; Manzeschke, A.; Haux, R. Robotic Systems in Operating Theaters: New Forms of Team-Machine Interaction in Health Care On Challenges for Health Information Systems on Adequately Considering Hybrid Action of Humans and Machines. Methods Inf. Med. 2019, 58, E14–E25. [Google Scholar] [CrossRef]
- Sik, A.S.; Aydinoglu, A.U.; Son, Y.A. Assessing the readiness of Turkish health information systems for integrating genetic/genomic patient data: System architecture and available terminologies, legislative, and protection of personal data. Health Policy 2021, 125, 203–212. [Google Scholar] [CrossRef]
- Bernardi, R.; Constantinides, P.; Nandhakumar, J. Challenging Dominant Frames in Policies for IS Innovation in Healthcare through Rhetorical Strategies. J. Assoc. Inf. Syst. 2017, 18, 81–112. [Google Scholar] [CrossRef]
- Liu, G.; Tsui, E.; Kianto, A. An emerging knowledge management framework adopted by healthcare workers in China to combat COVID-19. Knowl. Process Manag. 2022, 29, 284–295. [Google Scholar] [CrossRef]
- Bernardi, R. Health Information Systems and Accountability in Kenya: A Structuration Theory Perspective. J. Assoc. Inf. Syst. 2017, 18, 931–958. [Google Scholar] [CrossRef]
- Epizitone, A. Critical Success Factors within an Enterprise Resource Planning System Implementation Designed to Support Financial Functions of a Public Higher Education Institution. Master’s Thesis, Durban University of Technology, Durban, South Africa, 2021. [Google Scholar]
- Ostern, N.; Perscheid, G.; Reelitz, C.; Moormann, J. Keeping pace with the healthcare transformation: A literature review and research agenda for a new decade of health information systems research. Electron. Mark. 2021, 31, 901–921. [Google Scholar] [CrossRef]
- Farnham, A.; Utzinger, J.; Kulinkina, A.V.; Winkler, M.S. Using district health information to monitor sustainable development. Bull. World Health Organ. 2020, 98, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Faujdar, D.S.; Sahay, S.; Singh, T.; Kaur, M.; Kumar, R. Field testing of a digital health information system for primary health care: A quasi-experimental study from India. Int. J. Med. Inform. 2020, 141, 104235. [Google Scholar] [CrossRef]
- Jabareen, H.; Khader, Y.; Taweel, A. Health information systems in Jordan and Palestine: The need for health informatics training. East. Mediterr. Health J. 2020, 26, 1323–1330. [Google Scholar] [CrossRef]
- Ayabakan, S.; Bardhan, I.; Zheng, Z.; Kirksey, K. The Impact of Health Information Sharing on Duplicate Testing. MIS Q. 2017, 41, 1083–1104. [Google Scholar] [CrossRef]
- Mayer, F.; Faglioni, L.; Agabiti, N.; Fenu, S.; Buccisano, F.; Latagliata, R.; Ricci, R.; Spiriti, M.A.A.; Tatarelli, C.; Breccia, M.; et al. A Population-Based Study on Myelodysplastic Syndromes in the Lazio Region (Italy), Medical Miscoding and 11-Year Mortality Follow-Up: The Gruppo Romano-Laziale Mielodisplasie Experience of Retrospective Multicentric Registry. Mediterr. J. Hematol. Infect. Dis. 2017, 9, e2017046. [Google Scholar] [CrossRef] [PubMed]
- Soltysik-Piorunkiewicz, A.; Morawiec, P. The Sustainable e-Health System Development in COVID 19 Pandemic–The Theoretical Studies of Knowledge Management Systems and Practical Polish Healthcare Experience. J. e-Health Manag. 2022, 2022, 1–12. [Google Scholar] [CrossRef]
- Seo, K.; Kim, H.N.; Kim, H. Current Status of the Adoption, Utilization and Helpfulness of Health Information Systems in Korea. Int. J. Environ. Res. Public Health 2019, 16, 2122. [Google Scholar] [CrossRef] [PubMed]
- Mahendrawathi, E. Knowledge management support for enterprise resource planning implementation. Procedia Comput. Sci. 2015, 72, 613–621. [Google Scholar]
- Kim, Y.M.; Newby-Bennett, D.; Song, H.J. Knowledge sharing and institutionalism in the healthcare industry. J. Knowl. Manag. 2012, 16, 480–494. [Google Scholar] [CrossRef]
- Nwankwo, B.; Sambo, M.N. Effect of Training on Knowledge and Attitude of Health Care Workers towards Health Management Information System in Primary Health Centres in Northwest Nigeria. West Afr. J. Med. 2020, 37, 138–144. [Google Scholar] [PubMed]
- Khader, Y.; Jabareen, H.; Alzyoud, S.; Awad, S.; Rumeileh, N.A.; Manasrah, N.; Mudallal, R.; Taweel, A. Perception and acceptance of health informatics learning among health-related students in Jordan and Palestine. In Proceedings of the 2018 IEEE/ACS 15th International Conference on Computer Systems and Applications (AICCSA), Aqaba, Jordan, 28 October–1 November 2018. [Google Scholar]
- Benis, A.; Harel, N.; Barak Barkan, R.; Srulovici, E.; Key, C. Patterns of Patients’ Interactions With a Health Care Organization and Their Impacts on Health Quality Measurements: Protocol for a Retrospective Cohort Study. JMIR Res. Protoc. 2018, 7, e10734. [Google Scholar] [CrossRef]
- Delnord, M.; Abboud, L.A.; Costa, C.; Van Oyen, H. Developing a tool to monitor knowledge translation in the health system: Results from an international Delphi study. Eur. J. Public Health 2021, 31, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Dixon, B.E.; McGowan, J.J.; Cravens, G.D. Knowledge sharing using codification and collaboration technologies to improve health care: Lessons from the public sector. Knowl. Manag. Res. Pract. 2009, 7, 249–259. [Google Scholar] [CrossRef]
- See, E.J.; Alrukhaimi, M.; Ashuntantang, G.E.; Bello, A.K.; Bellorin-Font, E.; Gharbi, M.B.; Braam, B.; Feehally, J.; Harris, D.C.; Jha, V.; et al. Global coverage of health information systems for kidney disease: Availability, challenges, and opportunitiesfor development. Kidney Int. Suppl. 2018, 8, 74–81. [Google Scholar] [CrossRef]
- Vicente, E.; Ruiz de Sabando, A.; García, F.; Gastón, I.; Ardanaz, E.; Ramos-Arroyo, M.A. Validation of diagnostic codes and epidemiologic trends of Huntington disease: A population-based study in Navarre, Spain. Orphanet J. Rare Dis. 2021, 16, 77. [Google Scholar] [CrossRef]
- Colais, P.; Agabiti, N.; Davoli, M.; Buttari, F.; Centonze, D.; De Fino, C.; Di Folco, M.; Filippini, G.; Francia, A.; Galgani, S.; et al. Identifying Relapses in Multiple Sclerosis Patients through Administrative Data: A Validation Study in the Lazio Region, Italy. Neuroepidemiology 2017, 48, 171–178. [Google Scholar] [CrossRef] [PubMed]
- De Sanjose, S.; Tsu, V.D. Prevention of cervical and breast cancer mortality in low- and middle-income countries: A window of opportunity. Int. J. Womens Health 2019, 11, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Aung, E.; Whittaker, M. Preparing routine health information systems for immediate health responses to disasters. Health Policy Plan. 2013, 28, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, C.; Mion, L.C.; Willens, D.E.; Roumie, C.L.; Kripalani, S. Implementing routine health literacy assessment in hospital and primary care patients. Jt. Comm. J. Qual. Patient Saf. 2014, 40, 68–76. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Source: Authors | Core Enabling HIS Components | Benefits |
|---|---|---|
| Malaquias and Filho [11] | Health ER eHealth mHealth | Ease of access to patient and medical information from records; Cost reduction; Enhance efficiency in patients’ data recovery and management; Enable stakeholders’ health information centralization and remote access. |
| Ammenwerth, Duftschmid [44] | eHealth | Upsurge in care efficacy and quality and condensed costs for clinical services; Lessen the health care system’s administrative costs; Facilitates novel models of health care delivery. |
| Tummers, Tobi [45] | HIS | Patient information management; Enable communication within the healthcare arena; Afford high-quality and efficient care. |
| Steil, Finas [46] | HIS | Enable inter- and multidisciplinary collaboration between humans and machines; Afford autonomous and intelligent decision capabilities for health care applications. |
| Nyangena, Rajgopal [43] | HIS | Enable seamless information exchange within the healthcare arena. |
| Sik, Aydinoglu [47] | HIS | Support precision medicine approaches and decision support. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Epizitone, A.; Moyane, S.P.; Agbehadji, I.E. A Systematic Literature Review of Health Information Systems for Healthcare. Healthcare 2023, 11, 959. https://doi.org/10.3390/healthcare11070959
Epizitone A, Moyane SP, Agbehadji IE. A Systematic Literature Review of Health Information Systems for Healthcare. Healthcare. 2023; 11(7):959. https://doi.org/10.3390/healthcare11070959
Chicago/Turabian StyleEpizitone, Ayogeboh, Smangele Pretty Moyane, and Israel Edem Agbehadji. 2023. "A Systematic Literature Review of Health Information Systems for Healthcare" Healthcare 11, no. 7: 959. https://doi.org/10.3390/healthcare11070959
APA StyleEpizitone, A., Moyane, S. P., & Agbehadji, I. E. (2023). A Systematic Literature Review of Health Information Systems for Healthcare. Healthcare, 11(7), 959. https://doi.org/10.3390/healthcare11070959