

The Relationship between Working Night Shifts and Depression among Nurses: A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Methods
3. Literature Search Strategy
4. Study Selection and Data Extraction
5. Assessment of Risk of Bias and Grading the Evidence
6. Outcomes and Statistical Analysis
7. Results
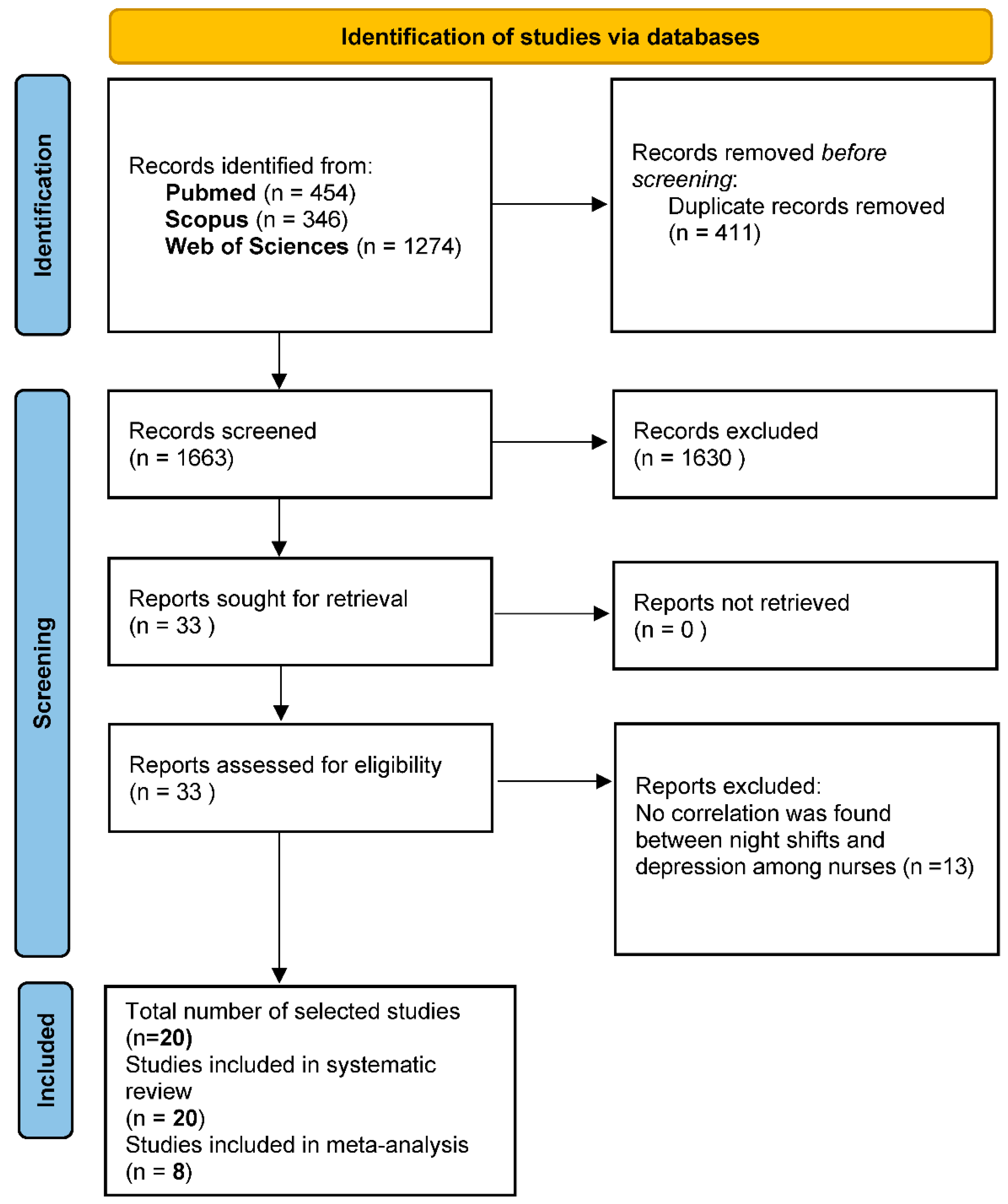
7.1. Study Identification and Selection
7.2. Study Characteristics
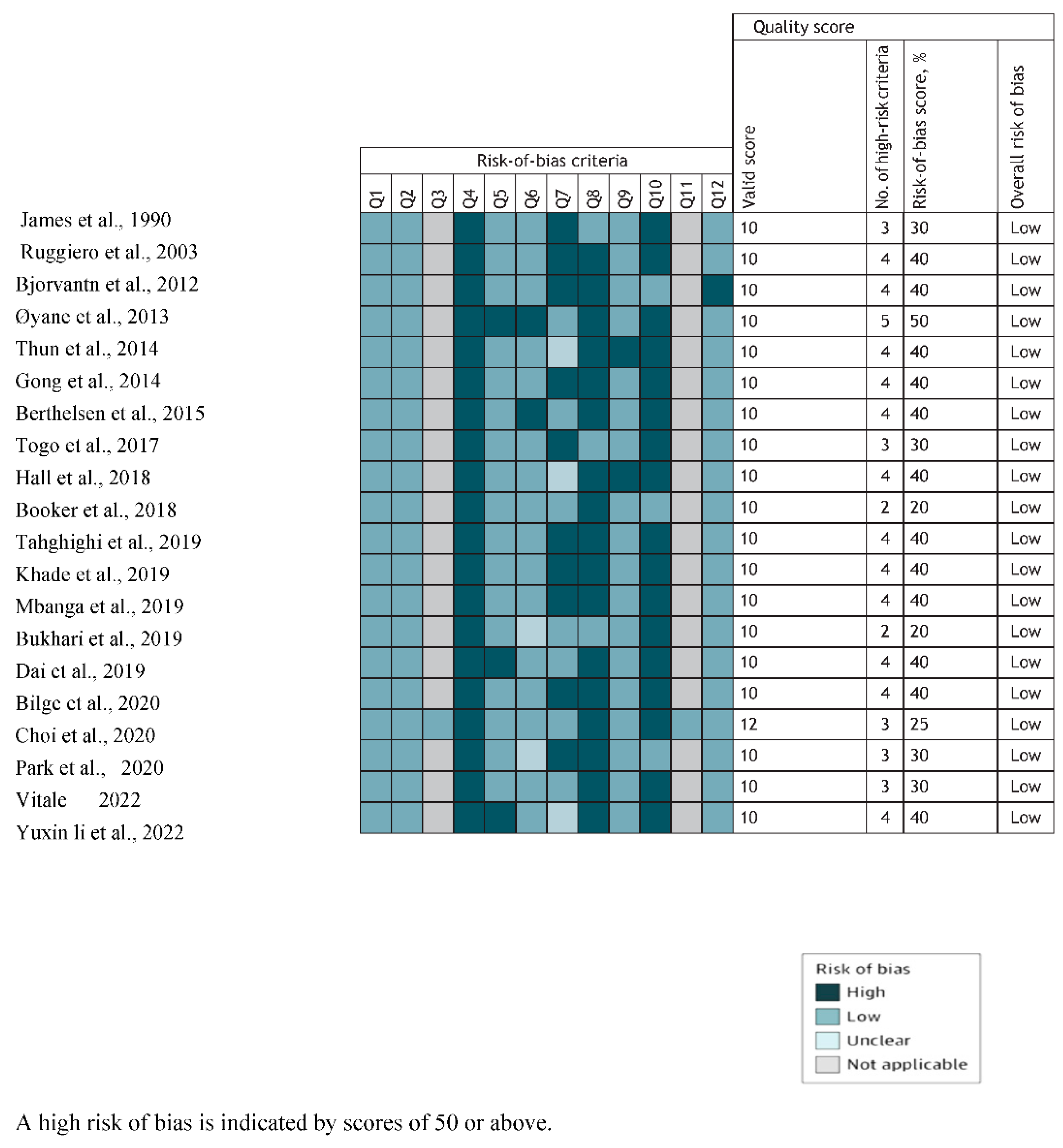
7.3. Outcome of Risk of Bias and Quality Assessment
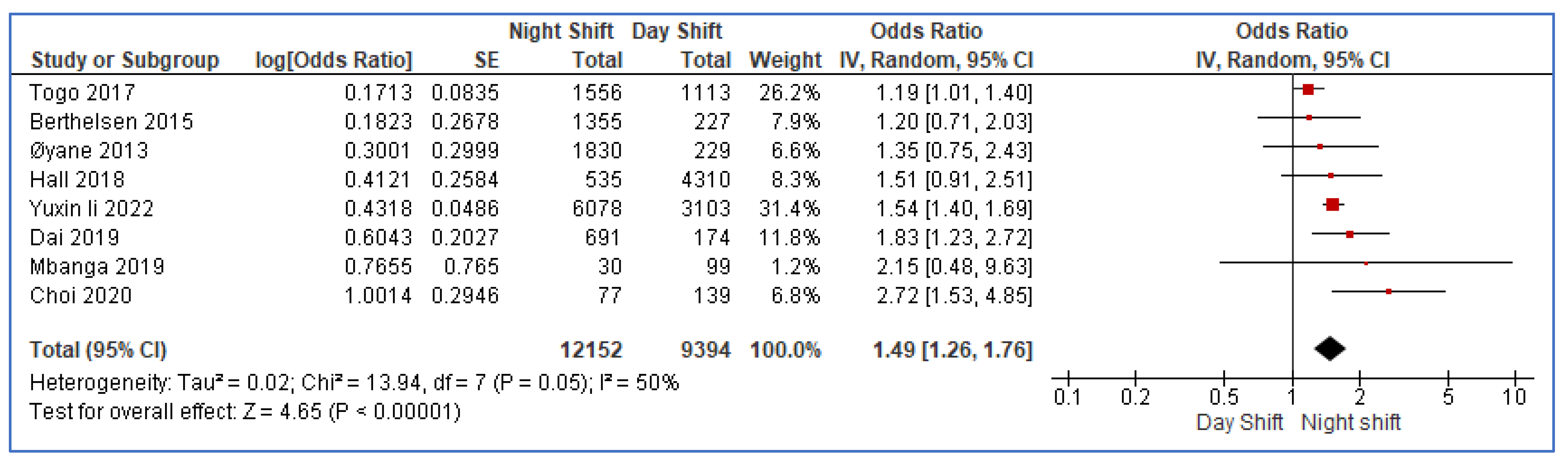
8. Meta-Analysis and Outcome
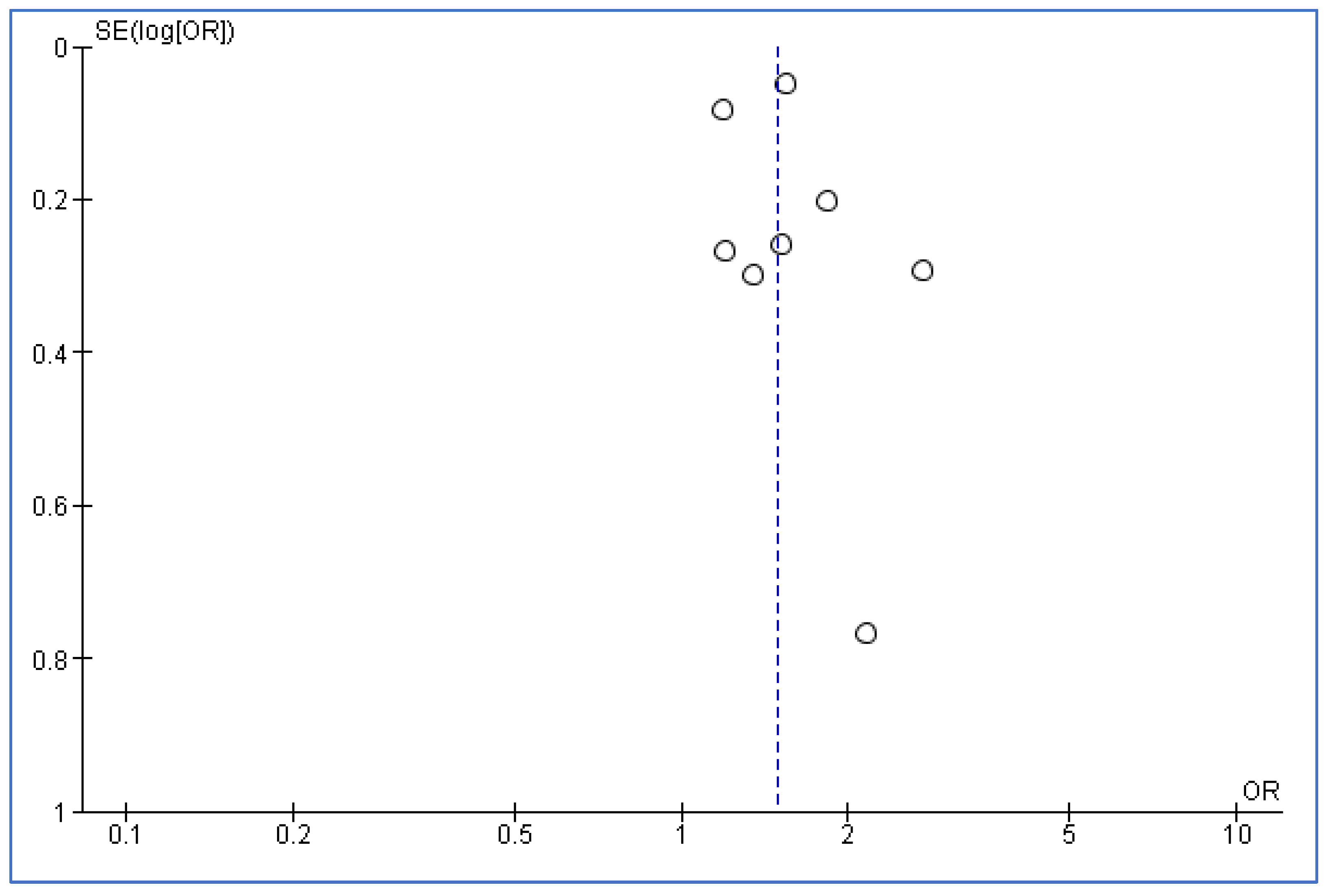
9. Publication Bias
10. GRADE Assessment of All Included Studies
11. Discussion
12. Strengths and Limitations
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Clinical Heterogeneity of Included Studies
| No | Author | Year | Population | Sex | Exposures | Comparator | Outcomes | Study Design | Mean Age (Years) |
| 1 | James [17] | 1990 | Nurses | B | Night shift | Other shifts | depression | cross-sectional | 35 |
| 2 | Ruggiero [18] | 2003 | Nurses | F | Night shift | Day shift | depression | cross-sectional | 44.9 |
| 3 | Bjorvantn [19] | 2012 | Nurses | B | Shift work | General population | depression | cross-sectional | 39.4 (9.1) |
| 4 | Øyane [20] | 2013 | Nurses | B | Current night shift | No night shift | depression | cross-sectional | 33.1 (8.2) |
| 5 | Thun [21] | 2014 | Nurses | F | Night shift | Day shift | depression | cross-sectional study | 33.1 (8.2) |
| 6 | Gong [22] | 2014 | Nurses | B | Night shift (>=2/week) | Night shift (<2/week) | depression | cross-sectional | 31.93 (7.55) |
| 7 | Berthelsen [23] | 2015 | Nurses | B | Night shift (current/previous) | No night shift | depression | cohort study | 30–39 |
| 8 | Togo [24] | 2017 | Nurses | B | Rotating shift | Day shift | depression | cross-sectional | Day worker = 41.5 (9.7), Rotating shift = 40.2 (10.4) |
| 9 | Hall [25] | 2018 | Nurses | B | High-precision work schedule (regular days) | High-precision work schedule (Rapid frequency rotating shifts) | depression | cross-sectional | 45–54 |
| 10 | Booker [26] | 2018 | Nurses | B | High-risk SWD | Low-risk SWD | depression | cross-sectional | 35.28 (12.02) |
| 11 | Tahghighi [27] | 2019 | Nurses | B | Shift work | Non-shift work | depression | cross-sectional | Shift work = 46.8 (11.50), Non-shift work = 50.0 (9.99) |
| 12 | Khade [28] | 2019 | Nurses | B | Number of night shifts in last 1 month | None | depression | cross-sectional | 25.3 (5.4) |
| 13 | Mbanga [29] | 2019 | Nurses | B | Number of night shifts in last 1 week | None | depression | cross-sectional | 29.8 (6.55) |
| 14 | Bukhari [30] | 2019 | Nurses | F | Rotating shift | Not stated | depression | cross-sectional | Not stated |
| 15 | Dai [31] | 2019 | Nurses | B | Night shift | Day shift | depression | cross-sectional | Not stated |
| 16 | Bilge [32] | 2020 | Nurses | F | Night shift | Day shift | depression | cross-sectional | 36.0 (6.37) |
| 17 | Choi [33] | 2020 | Nurses, Firefighters, Day workers | B | Nurses working 3-shift schedule | Other day workers | depression | cross-sectional | Nurses—28.7 (5.13), Firefighters—42.8 (9.38), Day workers—40.1 (8.30) |
| 18 | Park [34] | 2020 | Nurses | F | Shift work | Day shift | depression | cross-sectional | Shift work—28.1 (3.2), Day shift—30.8 (4.6) |
| 19 | Vitale [35] | 2022 | Nurses | B | Night shift | Day shift | depression | cross-sectional | Not stated |
| 20 | Yuxin li [36] | 2022 | Nurses | B | Shift work | No shift work | depression | cross-sectional | 33.24 (7.31) |
| B: both male and female, F: female only. | |||||||||
Appendix B. Methodological Heterogeneity of Included Studies
| No | Author | Year | Effect Measure | Study Group | Comparator Group | OR (95% CI)/B/r/π/p-Value | Statistical Adjustment | Direction of Effect |
| 1 | James [17] | 1990 | Regression coefficient | NA | NA | B = 0.09 | not done | negative |
| 2 | Ruggiero [18] | 2003 | Mean difference | 10.35 (7.89) | 7.18 (6.65) | p < 0.01 | not done | positive |
| 3 | Bjorvantn [19] | 2012 | Mean difference | 5.0 (2.3) | 3.5 (3.1) | p < 0.001 | not done | positive |
| 4 | Øyane [20] | 2013 | Odds ratio | Not stated | Not stated | 1.35 (0.75–2.42) | done | negative |
| 5 | Thun [21] | 2014 | Regression coefficient | NA | NA | B = −0.05 | done | negative |
| 6 | Gong [22] | 2014 | Regression Coefficient | NA | NA | B = 1.53 | done | positive |
| 7 | Berthelsen [23] | 2015 | Odds ratio | Not stated | Not stated | 1.20 (0.71–2.03) | not done | negative |
| 8 | Togo [24] | 2017 | Cohen’s d/odds ratio | 550/1006 | 351/762 | Cohens’ d = 0.084 | not done | positive |
| 9 | Hall [25] | 2018 | Odds ratio | Not stated | Not stated | 1.51 (0.91–2.51) | done | negative |
| 10 | Booker [26] | 2018 | Mean difference/R-squared | 7.54 (4.28) | 3.78 (3.24) | R2 = 0.184 | done | positive |
| 11 | Tahghighi [27] | 2019 | Mean difference | Not stated | Not stated | p = 0.514 | done | negative |
| 12 | Khade [28] | 2019 | Correlation coefficient | Not stated | Not stated | not stated | not done | negative |
| 13 | Mbanga [29] | 2019 | Odds ratio | Not stated | Not stated | 1.58 (1.01–2.48) | done | positive |
| 14 | Bukhari [30] | 2019 | Proportional difference | Not stated | Not stated | p = 0.012 | not done | positive |
| 15 | Dai [31] | 2019 | Odds ratio | Not stated | Not stated | 1.83 (1.23–2.72) | done | positive |
| 16 | Bilge [32] | 2020 | Mean difference | Not stated | Not stated | p < 0.001 | done | positive |
| 17 | Choi [33] | 2020 | Mean difference/Odds ratio | 7.64 (3.35), 41/36 | 6.30 (3.64), 41/98 | p = 0.014 | not done | positive |
| 18 | Park [34] | 2020 | Mean difference | 43.1 (6.4) | 35.3 (4.9) | p = 0.0003 | not done | positive |
| 19 | Vitale [35] | 2022 | Regression coefficient | NA | NA | B = −0.019 | done | negative |
| 20 | Yuxin li [36] | 2022 | Odds ratio | 2305/3773 | 1515/1588 | 1.54 (1.4–1.69) | done | positive |
| OR (95% CI): odds ratio (95% confidence interval), B: regression coefficient, r: correlation coefficient, π: prevalence/proportion, NA: not applicable. | ||||||||
Appendix C. Newcastle–Ottawa Quality Assessment Scale for the Cross-Sectional and Cohort Studies Included in the Systematic Review and Meta-Analysis
| Author (Year) | Selection | Comparability | Exposure/Outcome |
| Cross-Sectional studies (n = 18) | |||
| James, 1990 [17] | ***** | * | *** |
| Bjorvantn, 2012 [19] | **** | ** | *** |
| Øyane, 2013 [20] | ***** | ** | *** |
| Hall, 2018 [25] | ***** | * | *** |
| Booker, 2018 [26] | ***** | * | *** |
| Park, 2020 [34] | ***** | * | *** |
| Ruggiero, 2003 [18] | ***** | * | ** |
| Gong, 2014 [22] | ***** | * | ** |
| Thun, 2014 [21] | ***** | * | ** |
| Togo, 2017 [24] | ***** | * | ** |
| Dai, 2019 [31] | ***** | * | ** |
| Khade, 2019 [28] | ***** | * | ** |
| Mbanga, 2019 [29] | ***** | * | ** |
| Tahghighi, 2019 [27] | ***** | * | ** |
| Bilge, 2020 [32] | ***** | * | ** |
| Choi, 2020 [33] | ***** | * | ** |
| Yuxin li, 2022 [36] | ***** | * | ** |
| Bukhari, 2019 [30] | ** | * | ** |
| Cohort studies (n = 2) | |||
| Berthelsen, 2015 [23] | ***** | ** | *** |
| Vitale, 2022 [35] | ***** | * | ** |
| * = star. Green highlight = 9 stars or more. Yellow highlight = 7 or 8 stars. Red highlight = 6 stars or fewer. | |||
Appendix D. Percentage of Female Population and Mean Age in the Included Studies for the Meta-Analysis
| No | Author | Year | Population | Sex | Outcomes | Study Design | Tools | Validation | % Female | Mean Age (y) |
| 1 | Øyane [20] | 2013 | Nurses | B | depression | cross-sectional | HADS | Yes | 90.6 | 33.1 |
| 2 | Berthelsen [23] | 2015 | Nurses | B | depression | cohort study | HADS | Yes | 91 | 34.5 |
| 3 | Togo [24] | 2017 | Nurses | B | depression | cross-sectional | CES-D | Yes | 96.1 | 40.7 |
| 4 | Hall [25] | 2018 | Nurses | B | depression | cross-sectional | CIDI-SFMD | Yes | 94.7 | 41.5 |
| 5 | Mbanga [29] | 2019 | Nurses | B | depression | cross-sectional | PHQ-9 | Yes | 67.1 | 29.8 |
| 6 | Dai [31] | 2019 | Nurses | B | depression | cross-sectional | HADS | Yes | 98 | 29.2 |
| 7 | Choi [33] | 2020 | Nurses, Day workers | B | depression | cross-sectional | HADS | Yes | 55.1 | 36.0 |
| 8 | Yuxin li [36] | 2022 | Nurses | B | depression | cross-sectional | PHQ-9 | Yes | 94.8 | 33.2 |
| B = Both males and females, HADS = Hospital Anxiety and Depression Scale, CES-D = Center for Epidemiologic Studies Depression Scale, CIDI-SFMD = Composite International Diagnostic Interview Short Form, Major Depression section, PHQ-9 = 9-item Patient Health Questionnaire. | ||||||||||
References
- Wangsan, K.; Chaiear, N.; Sawanyawisuth, K.; Klainin-Yobas, P.; Simajareuk, K.; Boonsawat, W. Which Shiftwork Pattern Is the Strongest Predictor for Poor Sleep Quality in Nurses. Int. J. Environ. Res. Public Health 2022, 19, 13986. [Google Scholar] [CrossRef] [PubMed]
- Van Dongen, H.P.; Belenky, G. Individual differences in vulnerability to sleep loss in the work environment. Ind. Health 2009, 47, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; McCrae, C.S.; Cheung, J.; Martin, J.L.; Harrod, C.G.; Heald, J.L.; Carden, K.A. Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders: An American Academy of Sleep Medicine Systematic Review, Meta-Analysis, and GRADE Assessment. J. Clin. Sleep Med. 2018, 14, 1209–1230. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The Impact of Shift Work on Sleep, Alertness and Performance in Healthcare Workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef] [PubMed]
- Barger, L.K.; Lockley, S.W.; Rajaratnam, S.M.; Landrigan, C.P. Neurobehavioral, health, and safety consequences associated with shift work in safety-sensitive professions. Curr. Neurol. Neurosci. Rep. 2009, 9, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Gu, F.; Han, J.; Laden, F.; Pan, A.; Caporaso, N.E.; Stampfer, M.J.; Kawachi, I.; Rexrode, K.M.; Willett, W.C.; Hankinson, S.E.; et al. Total and cause-specific mortality of U.S. nurses working rotating night shifts. Am. J. Prev. Med. 2015, 48, 241–252. [Google Scholar] [CrossRef]
- Morrissette, D.A. Twisting the night away: A review of the neurobiology, genetics, diagnosis, and treatment of shift work disorder. CNS Spectr. 2013, 18 (Suppl. S1), 45–53. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/health-topics/depression#tab=tab_1 (accessed on 16 August 2022).
- Tahghighi, M.; Rees, C.S.; Brown, J.A.; Breen, L.J.; Hegney, D. What is the impact of shift work on the psychological functioning and resilience of nurses? An integrative review. J. Adv. Nurs. 2017, 73, 2065–2083. [Google Scholar] [CrossRef]
- Okechukwu, C.E.; Griffiths, M.D.; Carta, M.G.; Nwobodo, E.; Shariful Islam, S.M.; Forbes, M.; Berk, M.; Potenza, M.N.; Banach, M.; Amamihechineke Grace, O.; et al. Biological and practical considerations regarding circadian rhythm and mental health relationships among nurses working night shifts: A narrative review and recommendations. Riv. Psichiatr. 2022, 57, 67–79. [Google Scholar] [CrossRef]
- Okechukwu, C.E.; Okechukwu, C.E.; Torre, G.L. Effectiveness of bright light exposure, modafinil and armodafinil for improving alertness during working time among nurses on the night shift: A systematic review. Int. J. Healthc. Manag. 2022, 15, 336–346. [Google Scholar] [CrossRef]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Burton, N.W.; Kolbe-Alexander, T.L. Shift Work and Poor Mental Health: A Meta-Analysis of Longitudinal Studies. Am. J. Public Health 2019, 109, e13–e20. [Google Scholar] [CrossRef]
- Chidiebere Okechukwu, E.; Tibaldi, L.; La Torre, G. The impact of COVID-19 pandemic on mental health of Nurses. Clin. Ter. 2020, 171, e399–e400. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Viswanathan, M.; Berkman, N.D. Development of the RTI item bank on risk of bias and precision of observational studies. J. Clin. Epidemiol. 2012, 65, 163–178. [Google Scholar] [CrossRef]
- Skipper, J.K.; Jung, F.D.; Coffey, L.C. Nurses and shiftwork: Effects on physical health and mental depression. J. Adv. Nurs. 1990, 15, 835–842. [Google Scholar] [CrossRef]
- Ruggiero, J.S. Correlates of fatigue in critical care nurses. Res. Nurs. Health 2003, 26, 434–444. [Google Scholar] [CrossRef]
- Bjorvatn, B.; Dale, S.; Hogstad-Erikstein, R.; Fiske, E.; Pallesen, S.; Waage, S. Self-reported sleep and health among Norwegian hospital nurses in intensive care units. Nurs. Crit. Care. 2012, 17, 180–188. [Google Scholar] [CrossRef]
- Øyane, N.M.; Pallesen, S.; Moen, B.E.; Akerstedt, T.; Bjorvatn, B. Associations between night work and anxiety, depression, insomnia, sleepiness and fatigue in a sample of Norwegian nurses. PLoS ONE 2013, 8, e70228. [Google Scholar] [CrossRef]
- Thun, E.; Bjorvatn, B.; Torsheim, T.; Moen, B.E.; Magerøy, N.; Pallesen, S. Night work and symptoms of anxiety and depression among nurses: A longitudinal study. Work Stress 2014, 28, 376–386. [Google Scholar] [CrossRef]
- Gong, Y.; Han, T.; Yin, X.; Yang, G.; Zhuang, R.; Chen, Y.; Lu, Z. Prevalence of depressive symptoms and work-related risk factors among nurses in public hospitals in southern China: A cross-sectional study. Sci. Rep. 2014, 4, 7109. [Google Scholar] [CrossRef]
- Berthelsen, M.; Pallesen, S.; Magerøy, N.; Tyssen, R.; Bjorvatn, B.; Moen, B.E.; Knardahl, S. Effects of Psychological and Social Factors in Shiftwork on Symptoms of Anxiety and Depression in Nurses: A 1-Year Follow-Up. J. Occup. Environ. Med. 2015, 57, 1127–1137. [Google Scholar] [CrossRef]
- Togo, F.; Yoshizaki, T.; Komatsu, T. Association between depressive symptoms and morningness-eveningness, sleep duration and rotating shift work in Japanese nurses. Chronobiol. Int. 2017, 34, 349–359. [Google Scholar] [CrossRef]
- Hall, A.L.; Franche, R.L.; Koehoorn, M. Examining Exposure Assessment in Shift Work Research: A Study on Depression Among Nurses. Ann. Work Expo. Health 2018, 62, 182–194. [Google Scholar] [CrossRef]
- Booker, L.A.; Sletten, T.L.; Alvaro, P.K.; Barnes, M.; Collins, A.; Chai-Coetzer, C.L.; Naqvi, A.; McMahon, M.; Lockley, S.W.; Rajaratnam, S.M.W.; et al. Exploring the associations between shift work disorder, depression, anxiety and sick leave taken amongst nurses. J. Sleep Res. 2020, 29, e12872. [Google Scholar] [CrossRef]
- Tahghighi, M.; Brown, J.A.; Breen, L.J.; Kane, R.; Hegney, D.; Rees, C.S. A comparison of nurse shift workers’ and non-shift workers’ psychological functioning and resilience. J. Adv. Nurs. 2019, 75, 2570–2578. [Google Scholar] [CrossRef]
- Khade, Y.; Behera, S.; Koraddi, S.; Parvathi, R. A Study on Relationships Amongst Insomnia, Fatigue, Anxiety and Depression in Nurses. Indian J. Physiol. Pharmacol. 2019, 63, 246–251. [Google Scholar]
- Mbanga, C.; Makebe, H.; Tim, D.; Fonkou, S.; Toukam, L.; Njim, T. Burnout as a predictor of depression: A cross-sectional study of the sociodemographic and clinical predictors of depression amongst nurses in Cameroon. BMC Nurs. 2019, 18, 50. [Google Scholar] [CrossRef]
- Javaid Bukhari, G.M.; Habibullah, S.; Mushtaq, M.; Abbasi, J.; Malik, J.S. Occupational Factors Associated with Depression in Nurses Working in a Federal Government Tertiary Care Hospital in Islamabad. J. Ayub. Med. Coll. Abbottabad 2019, 31, 233–236. [Google Scholar]
- Dai, C.; Qiu, H.; Huang, Q.; Hu, P.; Hong, X.; Tu, J.; Xie, Q.; Li, H.; Ren, W.; Ni, S.; et al. The effect of night shift on sleep quality and depressive symptoms among Chinese nurses. Neuropsychiatr. Dis. Treat. 2019, 15, 435–440. [Google Scholar] [CrossRef]
- Bilge, C.; Mecdi Kaydirak, M.; Gür Avci, D.; Hotun Sahin, N. Effect of Shift Working on Depression Prevalence and Sexual Life of Female Nurses: A Correlational Study in Turkey. Int. J. Sex. Health 2020, 32, 357–364. [Google Scholar] [CrossRef]
- Choi, S.J.; Song, P.; Suh, S.; Joo, E.Y.; Lee, S.I. Insomnia Symptoms and Mood Disturbances in Shift Workers with Different Chronotypes and Working Schedules. J. Clin. Neurol. 2020, 16, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Bang, M.; Ahn, K.J.; Kim, W.J.; Shin, N.Y. Sleep disturbance-related depressive symptom and brain volume reduction in shift-working nurses. Sci. Rep. 2020, 10, 9100. [Google Scholar] [CrossRef] [PubMed]
- Vitale, E. Work Conditions of Italian Nurses and Their Related Risk Factors: A Cohort Investigatory Study. Diseases 2022, 10, 50. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, Y.; Lv, X.; Li, R.; Guan, X.; Li, L.; Li, J.; Cao, Y. Effects of Factors Related to Shift Work on Depression and Anxiety in Nurses. Front. Public Health 2022, 10, 926988. [Google Scholar] [CrossRef]
- Rogers, A.E. The Effects of Fatigue and Sleepiness on Nurse Performance and Patient Safety. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008; Chapter 40. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2645/ (accessed on 15 March 2023).
- Tsai, K.; Lee, T.Y.; Chung, M.H. Insomnia in female nurses: A nationwide retrospective study. Int. J. Occup. Saf. Ergon. 2017, 23, 127–132. [Google Scholar] [CrossRef]
- Huang, C.L.; Wu, M.P.; Ho, C.H.; Wang, J.J. Risks of treated anxiety, depression, and insomnia among nurses: A nationwide longitudinal cohort study. PLoS ONE 2018, 13, e0204224. [Google Scholar] [CrossRef]
- Cares, A.; Pace, E.; Denious, J.; Crane, L.A. Substance use and mental illness among nurses: Workplace warning signs and barriers to seeking assistance. Subst. Abus. 2015, 36, 59–66. [Google Scholar] [CrossRef]
- Hernandez, S.H.; Morgan, B.J.; Parshall, M.B. Resilience, Stress, Stigma, and Barriers to Mental Healthcare in U.S. Air Force Nursing Personnel. Nurs. Res. 2016, 65, 481–486. [Google Scholar] [CrossRef]
- Li, Y.; Lv, X.; Li, R.; Wang, Y.; Guan, X.; Li, L.; Li, J.; Xue, F.; Ji, X.; Cao, Y. Predictors of Shift Work Sleep Disorder Among Nurses During the COVID-19 Pandemic: A Multicenter Cross-Sectional Study. Front. Public Health 2021, 9, 785518. [Google Scholar] [CrossRef]
- Lee, A.; Myung, S.K.; Cho, J.J.; Jung, Y.J.; Yoon, J.L.; Kim, M.Y. Night Shift Work and Risk of Depression: Meta-analysis of Observational Studies. J. Korean Med. Sci. 2017, 32, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Angerer, P.; Schmook, R.; Elfantel, I.; Li, J. Night Work and the Risk of Depression. Dtsch. Arztebl. Int. 2017, 114, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Shen, B.; Li, P.; Wang, Y.; Liu, P.; Jiang, Y. Night shift work and depression among Chinese workers: The mediating role of sleep disturbances. Int. Arch. Occup. Environ. Health 2022, 95, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Behrens, T.; Burek, K.; Rabstein, S.; Wichert, K.; Erbel, R.; Eisele, L.; Arendt, M.; Dragano, N.; Brüning, T.; Jöckel, K.H. Impact of shift work on the risk of depression. Chronobiol. Int. 2021, 38, 1761–1775. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search String | Total Number of Results |
|---|---|---|
| Web of science |
| 1274 |
| Scopus |
| 346 |
| PubMed |
| 454 |
| N. | First Author | Year | Country | Study Design | Sample Size | Assessment Tool for Depression | Aim of the Study | Main Outcomes |
|---|---|---|---|---|---|---|---|---|
| 1 | James [17] | 1990 | United States | Cross-sectional study | 463 | Hospital Anxiety and Depression Scale | To determine the relationships between physical health and depression among nurses working shifts. | There was no significant correlation between shift work and signs of depression among nurses. |
| 2 | Ruggiero [18] | 2003 | United States | Cross-sectional study | 142 | Beck Depression Inventory-II | To evaluate shift-related variations in chronic fatigue and the influences of sleep quality, anxiety, and depression among female nurses. | Depression and poorer sleep quality were more prevalent in nurses that work night shifts than those that work day shifts. |
| 3 | Bjorvantn [19] | 2012 | Norway | Cross-sectional study | 267 | Hospital Anxiety and Depression Scale | To investigate sleep, sleepiness, fatigue, subjective health complaints (musculoskeletal, gastrointestinal), anxiety, and depression in a sample of Intensive Care Unit nurses. | 21.5% and 14.8% of the Intensive Care nurses scored above the cut-off values for anxiety and depression, respectively. |
| 4 | Øyane [20] | 2013 | Norway | Cross-sectional study | 2059 | Hospital Anxiety and Depression Scale | To determine the relationship between working the night shift with sleep problems and psychological wellbeing. | There was a significant positive correlation between insomnia and depression among night shift nurses. |
| 5 | Thun [21] | 2014 | Norway | Cross-sectional study | 633 | Hospital Anxiety and Depression Scale | To compare the developmental trajectories of anxiety and depressive symptoms among nurses working night shifts (night only or a three-shift schedule) with those of nurses working shifts that do not include nights (day only or a two-shift schedule). | Compared to day workers, nurses who switched from night to day shifts had a significant decline in anxiety and depressive symptoms over time. |
| 6 | Gong [22] | 2014 | China | Cross-sectional study | 3474 | Chinese version of the 20-item Zung Self-Rating Depression Scale | To investigate the association between working conditions and depressive symptoms among nurses using a cross-sectional study. | 1320 nurses reported having depressive symptoms, making the prevalence of depressive symptoms around 38% overall. A total of 20.82% of the nurses worked two or more night shifts each week. |
| 7 | Berthelsen [23] | 2015 | Norway | Cohort study | 2059 | Hospital Anxiety and Depression Scale | To investigate factors that may lead to shift work disorder in Norwegian nurses. | A reduction in the number of night shifts or cessation of working night shifts was associated with a decrease in depression and shift work disorder. |
| 8 | Togo [24] | 2017 | Japan | Cross-sectional study | 2669 | The Center for Epidemiologic Studies Depression Scale | To determine the relationships between depressive symptoms, morningness–eveningness, sleep duration, and rotating shift work among nurses. | Depression was more prevalent in rotating shift nurses compared to nurses who work only day shifts. |
| 9 | Hall [25] | 2018 | Canada | Cross-sectional study | 11,450 | Composite International Diagnostic Interview Short Form, Major Depression section | To investigate the relationships between work rota and depression among Canadian nurses. | There was a strong relationship between work rota and depression, which was very apparent among rotating and regular night shift nurses. |
| 10 | Booker [26] | 2018 | Australia | Cross-sectional study | 202 | Patient Health Questionnaire | To assess the relationship between shift work disorder risk, depression, and anxiety using validated tools. | Nurses who were at serious risk of shift work disorder had higher depression. |
| 11 | Tahghighi [27] | 2019 | Australia | Cross-sectional Study | 1369 | Depression, Anxiety, and Stress Scale—21 Items | To compare nurses who work shifts with nurses who work regular hours in order to comprehend the effects of shift work on psychological health and resilience. | There was relatively high levels of depression among both shift and non-shift nurses, but there was no significant difference between the two groups. |
| 12 | Khade [28] | 2019 | India | Cross-sectional study | 190 | Hospital Anxiety and Depression Scale | To determine the relationship between working the night shift with sleep problems and psychological wellbeing. | There was a significant positive correlation between insomnia and depression among night shift nurses. |
| 13 | Mbanga [29] | 2019 | Cameroon | Cross-sectional study | 143 | 9-item Patient Health Questionnaire | To determine the prevalence and predictors of depression among nurses in Cameroon. | Nurses who are working night shifts reported more depression and poorer sleep quality than day nurses. |
| 14 | Bukhari [30] | 2019 | Pakistan | Cross-sectional study | 250 | Agha Khan University Anxiety and Depression Scale | To determine the factors that were associated with depression among Pakistani nurses. | The prevalence of depression in nurses working rotating shifts was significantly higher. |
| 15 | Dai [31] | 2019 | China | Cross-sectional study | 865 | Hospital Anxiety and Depression Scale | To compare sleep quality as well as depressive symptoms in nurses working night shifts to those working day shifts only. | Among the 865 nurses, 353 (40.8%) were considered to have depressive symptoms. The logistic regression analysis demonstrated that night work was independently associated with the presence of depressive symptoms. |
| 16 | Bilge [32] | 2020 | Turkey | Cross-sectional study | 163 | Beck Depression Inventory | To determine the effect of nurses’ way of working on depression indicators and their sexual lives. | Nurses who worked night shifts had higher rates of depression and higher rates of sexual dysfunction. |
| 17 | Choi [33] | 2020 | South Korea | Cross-sectional study | 77 | Hospital Anxiety and Depression Scale | To examine the progression of depressed and anxiety symptoms in nurses working night shifts (night only or a three-shift schedule) with nurses working shifts without nights. | Depressive mood and anxiety symptoms were significantly worse in nurses working three-shift schedule. |
| 18 | Park [34] | 2020 | South Korea | Cross-sectional study | 39 | Hospital Anxiety and Depression Scale | To propose the mediating role of grey matter structures in the relationship between sleep disturbance and depressive symptoms. | All day-working nurses reported depressive symptoms within the normal range, whereas 39% of the shift-working nurses reported mild depression beyond the normal range. |
| 19 | Vitale [35] | 2022 | Italy | Cohort study | 408 | Depression, Anxiety, and Stress Scale—21 Items | To evaluate variations in body mass index features, shift, work history, and nurses’ levels of stress, anxiety, and depression. | There was no significant difference in the rate of depression between night shift nurses and their day shift colleagues. |
| 20 | Yuxin li [36] | 2022 | China | Cross-sectional study | 11,061 | 9-item Patient Health Questionnaire | To evaluate and describe the mental health status of Chinese nurses, including symptoms of depression and anxiety, while focusing on the effects of shift work-related characteristics. | Shift work correlated with higher levels of depression among all nurses. |
| Criteria | No of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Other Considerations | No of Subjects | Relative (95% CI) | Overall Quality of Evidence | Importance |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nurses, shift work, and depression | 20 | Cross-sectional studies and cohort studies | Low | Significant | Not significant | Not significant | Not significant | None | 37,983 | - | ⊕⊕⊕⊝ Moderate | Critical |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okechukwu, C.E.; Colaprico, C.; Di Mario, S.; Oko-oboh, A.G.; Shaholli, D.; Manai, M.V.; La Torre, G. The Relationship between Working Night Shifts and Depression among Nurses: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 937. https://doi.org/10.3390/healthcare11070937
Okechukwu CE, Colaprico C, Di Mario S, Oko-oboh AG, Shaholli D, Manai MV, La Torre G. The Relationship between Working Night Shifts and Depression among Nurses: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(7):937. https://doi.org/10.3390/healthcare11070937
Chicago/Turabian StyleOkechukwu, Chidiebere Emmanuel, Corrado Colaprico, Sofia Di Mario, Agbonvihele Gregrey Oko-oboh, David Shaholli, Maria Vittoria Manai, and Giuseppe La Torre. 2023. "The Relationship between Working Night Shifts and Depression among Nurses: A Systematic Review and Meta-Analysis" Healthcare 11, no. 7: 937. https://doi.org/10.3390/healthcare11070937
APA StyleOkechukwu, C. E., Colaprico, C., Di Mario, S., Oko-oboh, A. G., Shaholli, D., Manai, M. V., & La Torre, G. (2023). The Relationship between Working Night Shifts and Depression among Nurses: A Systematic Review and Meta-Analysis. Healthcare, 11(7), 937. https://doi.org/10.3390/healthcare11070937