
Manual and Application-Based Carbohydrate Counting and Glycemic Control in Type 1 Diabetes Subjects: A Narrative Review


Abstract
1. Introduction
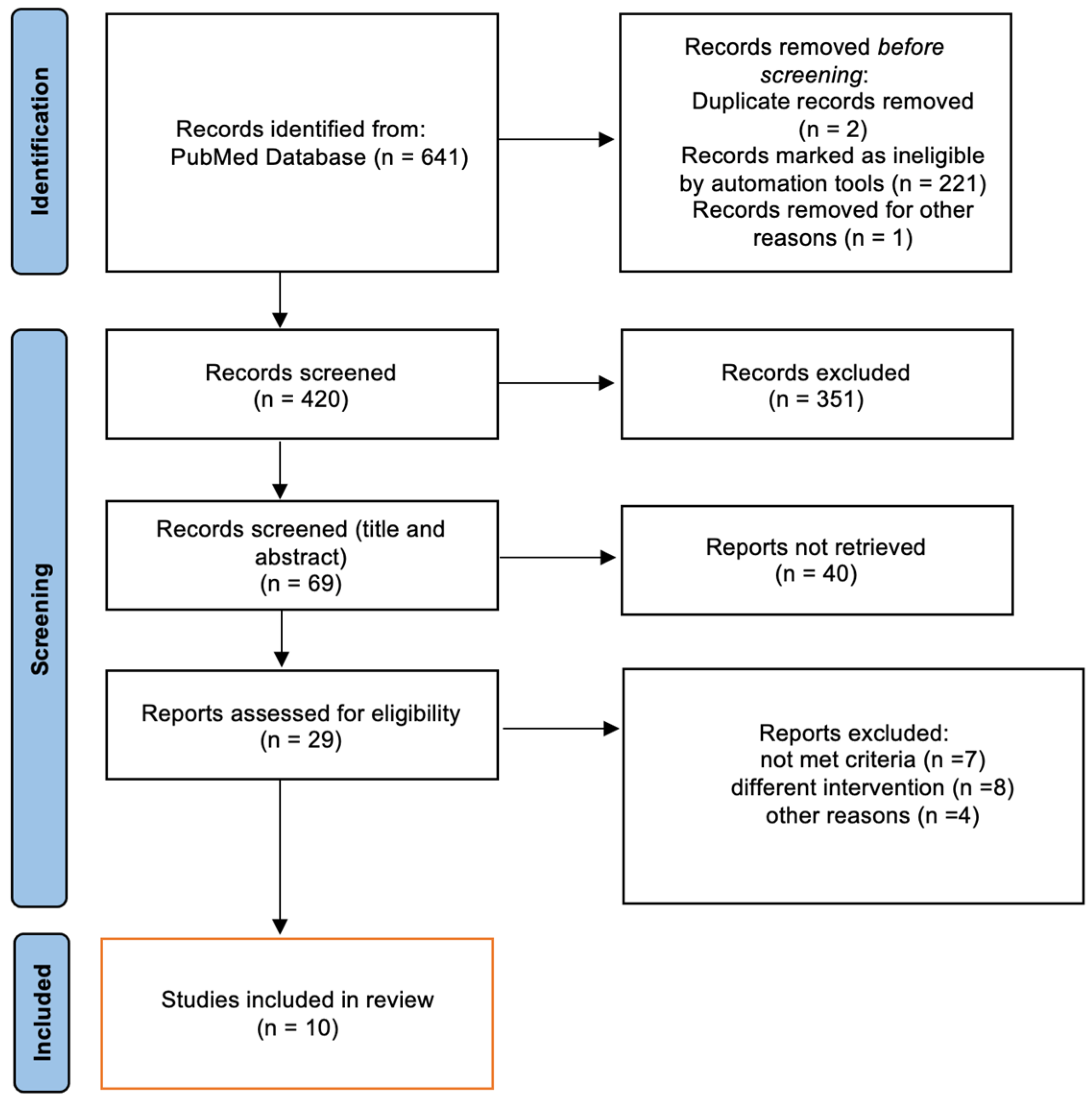
2. Materials and Methods
3. Results and Discussion

{kind=link}
| Author/Year | Country | No. of Patients | Intervention | Control | Result Intervention/Control | Follow-Up | ||
|---|---|---|---|---|---|---|---|---|
| HbA1c 1 % (M 2 ± SD 3) | Insulin Dose (U/kg 4) (M ± SD) | BMI 5 (kg/m2) (M ± SD) or BW | ||||||
| Adult | ||||||||
| Hommel E. et al., 2016 [25] | Denmark | 168 | n = 84, advanced CHOC using an automated bolus calculator | n = 84, advanced CHOC using mental calculations | (8.9 ± 0.7 to 8.4 ± 0.45) (9.0 ± 0.8 to 8.8 ± 0.25) | __ | No change in BW | 1 year |
| Schmidt et al., 2012 [16] | Denmark | 51 | n = 21, CarbCount Group: taught CHOC, ICRs, and ISFs were estimated; or n = 22, CarbCountABC: taught the same CarbCount group and instructed in the use of the automated bolus calculator (ABC) | n = 8, group diabetes education (food recommendations, self-monitoring techniques, and estimated insulin doses) | CarbCount (9.2 ± 0.6 to 8.4 ± 0.9) CarbCountABC (8.8 ± 0.7 to 8.1 ± 0.4) Control (9.10 ± 0.70 to 8.90 ± 1.10) | CarbCount (0.6 ± 0.2 to −0.03 ± 0.11) CarbCountABC (0.7 ± 0.2 to −0.03 ± 0.15) Control (0.7 ± 0.17 to 0.01 ± 0.07) | No change in BW | 16 weeks |
| Laurenzi et al., 2011 [26] | Italy | 61 | n = 28, CHOC education | n = 28, usual care | Similar in the two groups (p = 0.252) | No changes | BMI 23.7 (21–25.2) at 24 weeks, −0.32 (−0.65 to 0), and 23.8 (20.8–26.8) at 24 weeks, 0.15 (0–0.40) | 24 weeks |
| Scavone et al., 2010 [27] | Italy | 256 | n = 156, CHOC education (4 weeks), reassessed every 3 months | n = 73/100, usual care | 7.80 ± 1.30 to 7.40 ± 0.90 7.50 ± 0.80 to 7.50 ± 1.10 | At the end, 23.5 ± 10.9 vs. 27.7 ± 17.1 | No BW gain | 9 months |
| Trento et al., 2011 [28] | Italy | 56 | n = 27, CHOC program (8 sessions), and usual group care | n = 29, usual diabetes education and group care | 7.60 ± 1.30 to 7.20 ± 0.90 7.70 ± 1.24 to 7.90 ± 1.40 | No changes | BMI 24.4 ± 2.6 to 23.4 ± 5.3 23.5 ± 3.3 to 23.5 ± 2.9 | 30 months |
| Isaksson S. et al., 2021 [24] | Sweden | 159 | n = 51, food-based approach, and n= 52, CHOC | n = 55, routine care | FBS 8.1 ± 0.7 to 7.8 ± 0.7 CHOC 7.9 ± 0.7 to 7.8 ± 0.7 RC 8.0 ± 0.7 to 7.9 ± 0.8 | No changes | No change in BW | 12 months |
| Children and adolescents | ||||||||
| Alfonsi J. et al., 2020 [29] | Canada | 46 | n = 21, CHOC and iSpy app | n = 22, CHOC | 8.41 ± 1.84 to 8.06 ± 1.43, 8.35 ± 1.32 to 8.80 ± 1.60 | __ | __ | 3 months |
| Goksen et al., 2014 [30] | Turkey | 110 | n = 52, CHOC group | n = 32, usual nutritional and diabetic education | 8.10 ± 1.00 to 7.87 ± 1.38, 8.43 ± 1.52 to 8.76 ± 1.77 | 0.92 ± 0.29 to 1.01 ± 0.28, 0.96 ± 0.36 to 1.02 ± 0.31 | 19.61 ± 3.22 to 20.81 ± 3.38, 20.89 ± 3.31 to 21.80 ± 3.68, and no change | 2 years |
| Enander et al., 2012 [31] | Sweden | 40 | Group B: n = 12, manual CHOC; Group C: n = 14, CHOC with a bolus calculator | Group A: n = 14, traditional methodology (the plate exchange method) | Group B, 7.7 ± 1.0 to 7.8 ± 0.9; Group C, 7.2 ± 0.6 to 7.6 ± 1.1; and Group A, 7.70 ± 1.00 to 8.00 ± 1.00 | Group B, 0.42 ± 0.12 to 0.44 ± 0.14; Group C, 0.45 ± 0.19 to 0.42 ± 0.13; and Group A, 0.43 ± 0.10 to 0.46 ± 0.10 | At 12 months: Group C significantly decreased compared with baseline (+1.2 vs. +1.4 kg/m2) | 12 months |
| Donzeau A. et al., 2020 [32] | France | 87 | ACC group: n = 40, advanced CHOC | Control group: n = 47, standard nutrition | At 3 months, 7.8 ± 0.5 to 7.53 ± 0.61 and 7.8 ± 0.5 to 7.88 ± 0.56; at 12 months, no difference | __ | No difference in BMI | 52 weeks |
3.1. Primary Outcome
Glycemic Control Assessed by HbA1c
3.2. Secondary Outcome
3.2.1. Severe Hypoglycemia
3.2.2. Body Weight
3.2.3. Daily Insulin Dose
3.2.4. Quality of Life and Satisfaction Questionnaires
3.3. Carbohydrate-Counting Application Safety
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Green, A.; Hede, S.M.; Patterson, C.C.; Wild, S.H.; Imperatore, G.; Roglic, G.; Beran, D. Type 1 diabetes in 2017: Global estimates of incident and prevalent cases in children and adults Abbrevia-tions CM Child mortality rate EURODIAB Europe and Diabetes GBD Global Burden of Disease HIC High-income country LIC Low-income country. Diabetologia 2021, 64, 2741–2750. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Halim, S.; Gurudas, S.; Sivaprasad, S.; Owens, D. IDF Diabetes Atlas: A review of studies utilising retinal photography on the global prevalence of diabetes related retinopathy between 2015 and 2018. Diabetes Res. Clin. Pract. 2019, 157, 107840. [Google Scholar] [CrossRef]
- American Diabetes Association. Disclosures: Standards of Care in Diabetes—2023. Diabetes Care 2022, 46 (Suppl. S1), S281–S284. [Google Scholar] [CrossRef]
- Sticht, J.; Álvaro-Benito, M.; Konigorski, S. Type 1 Diabetes and the HLA Region: Genetic Association Besides Classical HLA Class II Genes. Front. Genet. 2021, 12, 683946. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.A.; Valdes, A.M. Genetics of the HLA Region in the Prediction of Type 1 Diabetes. Curr. Diabetes Rep. 2011, 11, 533–542. [Google Scholar] [CrossRef]
- Sapra, A.; Bhandari, P. Diabetes Mellitus; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tang, E.H.M.; Mak, I.L.; Tse, E.T.Y.; Wan, E.Y.F.; Yu, E.Y.T.; Chen, J.Y.; Chin, W.Y.; Chao, D.V.K.; Tsui, W.W.S.; Ha, T.K.H.; et al. Ten-Year Effectiveness of the Multidisciplinary Risk Assessment and Management Programme–Diabetes Mellitus (RAMP-DM) on Macrovascular and Microvascular Complications and All-Cause Mortality: A Population-Based Cohort Study. Diabetes Care 2022, 45, 2871–2882. [Google Scholar] [CrossRef]
- Vaz, E.C.; Porfírio, G.J.M.; Nunes, H.R.D.C.; Nunes-Nogueira, V.D.S. Effectiveness and safety of carbohydrate counting in the management of adult patients with type 1 diabetes mellitus: A systematic review and meta-analysis. Arq. Bras. de Endocrinol. Metabol. 2018, 62, 337–345. [Google Scholar] [CrossRef]
- Gupta, L.; Khandelwal, D.; Kalra, S. Carbohydrate counting-1: South Asian framework. J. Pak. Med. Assoc. 2017, 67, 1296–1298. [Google Scholar]
- Builes-Montaño, C.E.; Ortiz-Cano, N.A.; Ramirez-Rincón, A.; Rojas-Henao, N.A. Efficacy and safety of carbohydrate counting versus other forms of dietary advice in patients with type 1 diabetes mellitus: A systematic review and meta-analysis of randomised clinical trials. J. Hum. Nutr. Diet. 2022, 35, 1030–1042. [Google Scholar] [CrossRef]
- Tascini, G.; Berioli, M.G.; Cerquiglini, L.; Santi, E.; Mancini, G.; Rogari, F.; Toni, G.; Esposito, S. Carbohydrate Counting in Children and Adolescents with Type 1 Diabetes. Nutrients 2018, 10, 109. [Google Scholar] [CrossRef]
- Dimitriades, M.E.; Pillay, K. Carbohydrate counting in type 1 diabetes mellitus: Dietitians’ perceptions, training and barriers to use. S. Afr. J. Clin. Nutr. 2021, 35, 94–99. [Google Scholar] [CrossRef]
- Gillespie, S.J.; Kulkarni, K.D.; Daly, A.E. Using Carbohydrate Counting in Diabetes Clinical Practice. J. Am. Diet. Assoc. 1998, 98, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, G.; Piscopo, M.A.; Rigamonti, A.; Azzinari, A.; Bettini, S.; Bonfanti, R.; Viscardi, M.; Meschi, F.; Chiumello, G. Insulin therapy and carbohydrate counting. Acta Biomed. 2005, 76 (Suppl. S3), 44–48. [Google Scholar]
- Gupta, L.; Khandelwal, D.; Kalra, S. Applied carbohydrate counting. J. Pak. Med. Assoc. 2017, 67, 1456–1457. [Google Scholar]
- Schmidt, S.; Meldgaard, M.; Serifovski, N.; Storm, C.; Christensen, T.M.; Gade-Rasmussen, B.; Nørgaard, K. Use of an Automated Bolus Calculator in MDI-Treated Type 1 Diabetes. Diabetes Care 2012, 35, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Dias, V.M.; Pandini, J.A.; Nunes, R.R.; Sperandei, S.L.; Portella, E.S.; Cobas, R.A.; Gomes, M.D.B. Effect of the carbohydrate counting method on glycemic control in patients with type 1 diabetes. Diabetol. Metab. Syndr. 2010, 2, 54–57. [Google Scholar] [CrossRef]
- DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: Dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ 2002, 325, 746. [Google Scholar] [CrossRef]
- Fleming, G.A.; Petrie, J.R.; Bergenstal, R.M.; Holl, R.W.; Peters, A.L.; Heinemann, L. Diabetes digital app technology: Benefits, challenges, and recommendations. A consensus report by the European Association for the Study of Diabetes (EASD) and the American Diabetes Association (ADA) Diabetes Technology Working Group. Diabetologia 2019, 63, 229–241. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 7. Diabetes Technology: Standards of Care in Diabetes—2023. Diabetes Care 2022, 46, S111–S127. [Google Scholar] [CrossRef]
- Nolt, V.D.; Araya, A.; Ateya, M.B.; Chen, M.; Kelley, J.; Arnold, P.; Singer, K. Insulin Bolus Calculator: Lessons Learned from Institutional Experience. J. Diabetes Sci. Technol. 2020, 15, 265–270. [Google Scholar] [CrossRef]
- Deeb, A.; Al Hajeri, A.; Alhmoudi, I.; Nagelkerke, N. Accurate Carbohydrate Counting Is an Important Determinant of Postprandial Glycemia in Children and Adolescents with Type 1 Diabetes on Insulin Pump Therapy. J. Diabetes Sci. Technol. 2016, 11, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, S.S.; Bacos, M.B.; Eliasson, B.; Adolfsson, E.T.; Rawshani, A.; Lindblad, U.; Jendle, J.; Berglund, A.; Lind, M.; Axelsen, M. Effects of nutrition education using a food-based approach, carbohydrate counting or routine care in type 1 diabetes: 12 months prospective randomized trial. BMJ Open Diabetes Res. Care 2021, 9, e001971. [Google Scholar] [CrossRef] [PubMed]
- Hommel, E.; Schmidt, S.; Vistisen, D.; Neergaard, K.; Gribhild, M.; Almdal, T.; Norgaard, K. Effects of advanced carbohydrate counting guided by an automated bolus calculator in Type 1 diabetes mellitus (StenoABC): A 12-month, randomized clinical trial. Diabet. Med. 2016, 34, 708–715. [Google Scholar] [CrossRef]
- Laurenzi, A.; Bolla, A.M.; Panigoni, G.; Doria, V.; Uccellatore, A.; Peretti, E.; Saibene, A.; Galimberti, G.; Bosi, E.; Scavini, M. Effects of Carbohydrate Counting on Glucose Control and Quality of Life Over 24 Weeks in Adult Patients with Type 1 Diabetes on Continuous Subcutaneous Insulin Infusion. Diabetes Care 2011, 34, 823–827. [Google Scholar] [CrossRef]
- Scavone, G.; Manto, A.; Pitocco, D.; Gagliardi, L.; Caputo, S.; Mancini, L.; Zaccardi, F.; Ghirlanda, G. Effect of carbohydrate counting and medical nutritional therapy on glycaemic control in Type 1 diabetic subjects: A pilot study. Diabet. Med. 2010, 27, 477–479. [Google Scholar] [CrossRef]
- Trento, M.; Trinetta, A.; Kucich, C.; Grassi, G.; Passera, P.; Gennari, S.; Paganin, V.; Tedesco, S.; Charrier, L.; Cavallo, F.; et al. Carbohydrate counting improves coping ability and metabolic control in patients with Type 1 diabetes managed by Group Care. J. Endocrinol. Investig. 2010, 34, 101–105. [Google Scholar] [CrossRef]
- Alfonsi, J.E.; Choi, E.E.Y.; Arshad, T.; Sammott, S.-A.S.; Pais, V.; Nguyen, C.; Maguire, B.R.; Stinson, J.N.; Palmert, M.R. Carbohydrate Counting App Using Image Recognition for Youth with Type 1 Diabetes: Pilot Randomized Control Trial. JMIR mHealth uHealth 2020, 8, e22074. [Google Scholar] [CrossRef]
- Gökşen, D.; Altınok, Y.A.; Özen, S.; Demir, G.; Darcan, Ş. Effects of Carbohydrate Counting Method on Metabolic Control in Children with Type 1 Diabetes Mellitus. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 74–78. [Google Scholar] [CrossRef]
- Enander, R.; Gundevall, C.; Strömgren, A.; Chaplin, J.; Hanas, R. Carbohydrate counting with a bolus calculator improves post-prandial blood glucose levels in children and adolescents with type 1 diabetes using insulin pumps. Pediatr. Diabetes 2012, 13, 545–551. [Google Scholar] [CrossRef]
- Donzeau, A.; Bonnemaison, E.; Vautier, V.; Menut, V.; Houdon, L.; Bendelac, N.; Bismuth, E.; Bouhours-Nouet, N.; Quemener, E.; Baron, S.; et al. Effects of advanced carbohydrate counting on glucose control and quality of life in children with type 1 diabetes. Pediatr. Diabetes 2020, 21, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Bayless, M.; Cleary, P.; Genuth, S.; Gubitosi-Klug, R.; Lachin, J.M.; Lorenzi, G.; Zinman, B.; DCCT/EDIC Research Group. Diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: Advances and contributions. Diabetes Care 2013, 62, 3976–3986. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Volkening, L.K.; Laffel, L.M. Distinct Patterns of Daily Glucose Variability by Pubertal Status in Youth with Type 1 Diabetes. Diabetes Care 2019, 43, 22–28. [Google Scholar] [CrossRef]
- Abreu, C.; Miranda, F.; Felgueiras, P. Carbohydrate counting: How accurate should it be to achieve glycemic control in patients on intensive insulin regimens? AIP Conf. Proc. 2019, 2116, 250009. [Google Scholar] [CrossRef]
- Souto, D.L.; Zajdenverg, L.; Rodacki, M.; Rosado, E.L. Impact of advanced and basic carbohydrate counting methods on metabolic control in patients with type 1 diabetes. Nutrition 2014, 30, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Norgaard, K. Bolus Calculators. J. Diabetes Sci. Technol. 2014, 8, 1035–1041. [Google Scholar] [CrossRef]
- Anthimopoulos, M.; Dehais, J.; Shevchik, S.; Ransford, B.H.; Duke, D.; Diem, P.; Mougiakakou, S. Computer Vision-Based Carbohydrate Estimation for Type 1 Patients with Diabetes Using Smartphones. J. Diabetes Sci. Technol. 2015, 9, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Bloomgarden, Z. Beyond HbA1c. J. Diabetes 2017, 9, 1052–1053. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]

| Author/Year | Outcome | Definition of Hypoglycemia | Result |
|---|---|---|---|
| Adult | |||
| Hommel E. et al., 2016 [25] | Episodes of severe hypoglycemia | Less than 3.9 mmol/L | Not significant, p-value not reported |
| Schmidt et al., 2012 [16] | Frequency of hypoglycemia | Self-reported (scored 0–6, perceived frequency is higher with higher scores) | Comparing control with CarbCount and CarbCountABC group (1.8 ± 1.4, 2.2 ± 1.1, 1.6 ± 1.2, p = 0.197) 1 |
| Laurenzi et al., 2011 [26] | Frequency of hypoglycemia and episodes of severe hypoglycemia | ≤2.8 mmol/L requiring assistance from a third party | Not significant, no severe hypoglycemia events reported |
| Scavone et al., 2010 [27] | Number of hypoglycemia events | Blood glucose < 3.9 mmol/L | Less hypoglycemic events in the CHOC group vs. control group (4% vs. 7%), p < 0.05 |
| Trento et al., 2011 [28] | Severe hypoglycemic episodes | Hypoglycemia episodes requiring third-party help | CHOC vs. control (5 vs. 6 episodes), p-value not reported |
| Isaksson S. et al., 2021 [24] | The number of self-reported hypoglycemic events per month | Defined as glucose levels below 3.5 mmol/L | CHOC vs. control (0.05 vs. 0.07 events per month, p = 0.437) |
| Children and adolescents | |||
| Enander et al., 2012 [31] | Frequency of hypoglycemia | Defined as plasma glucose < 3.5 mmol/L | Compared with baseline, hypoglycemia episodes in control, manual CHOC, and CHOC with a bolus calculator significantly reduced after intervention (p = 0.011) with no significant differences between groups |
| Donzeau A. et al., 2020 [32] | Episodes of severe hypoglycemia | Coma and/or convulsion | Intervention vs. control (3% vs. 2% patient/year, p < 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlBabtain, S.A.; AlAfif, N.O.; AlDisi, D.; AlZahrani, S.H. Manual and Application-Based Carbohydrate Counting and Glycemic Control in Type 1 Diabetes Subjects: A Narrative Review. Healthcare 2023, 11, 934. https://doi.org/10.3390/healthcare11070934
AlBabtain SA, AlAfif NO, AlDisi D, AlZahrani SH. Manual and Application-Based Carbohydrate Counting and Glycemic Control in Type 1 Diabetes Subjects: A Narrative Review. Healthcare. 2023; 11(7):934. https://doi.org/10.3390/healthcare11070934
Chicago/Turabian StyleAlBabtain, Sara A., Nora O. AlAfif, Dara AlDisi, and Saad H. AlZahrani. 2023. "Manual and Application-Based Carbohydrate Counting and Glycemic Control in Type 1 Diabetes Subjects: A Narrative Review" Healthcare 11, no. 7: 934. https://doi.org/10.3390/healthcare11070934
APA StyleAlBabtain, S. A., AlAfif, N. O., AlDisi, D., & AlZahrani, S. H. (2023). Manual and Application-Based Carbohydrate Counting and Glycemic Control in Type 1 Diabetes Subjects: A Narrative Review. Healthcare, 11(7), 934. https://doi.org/10.3390/healthcare11070934