
The Prevalence of Cardiovascular Diseases in Paralympic Athletes



Abstract
1. Introduction
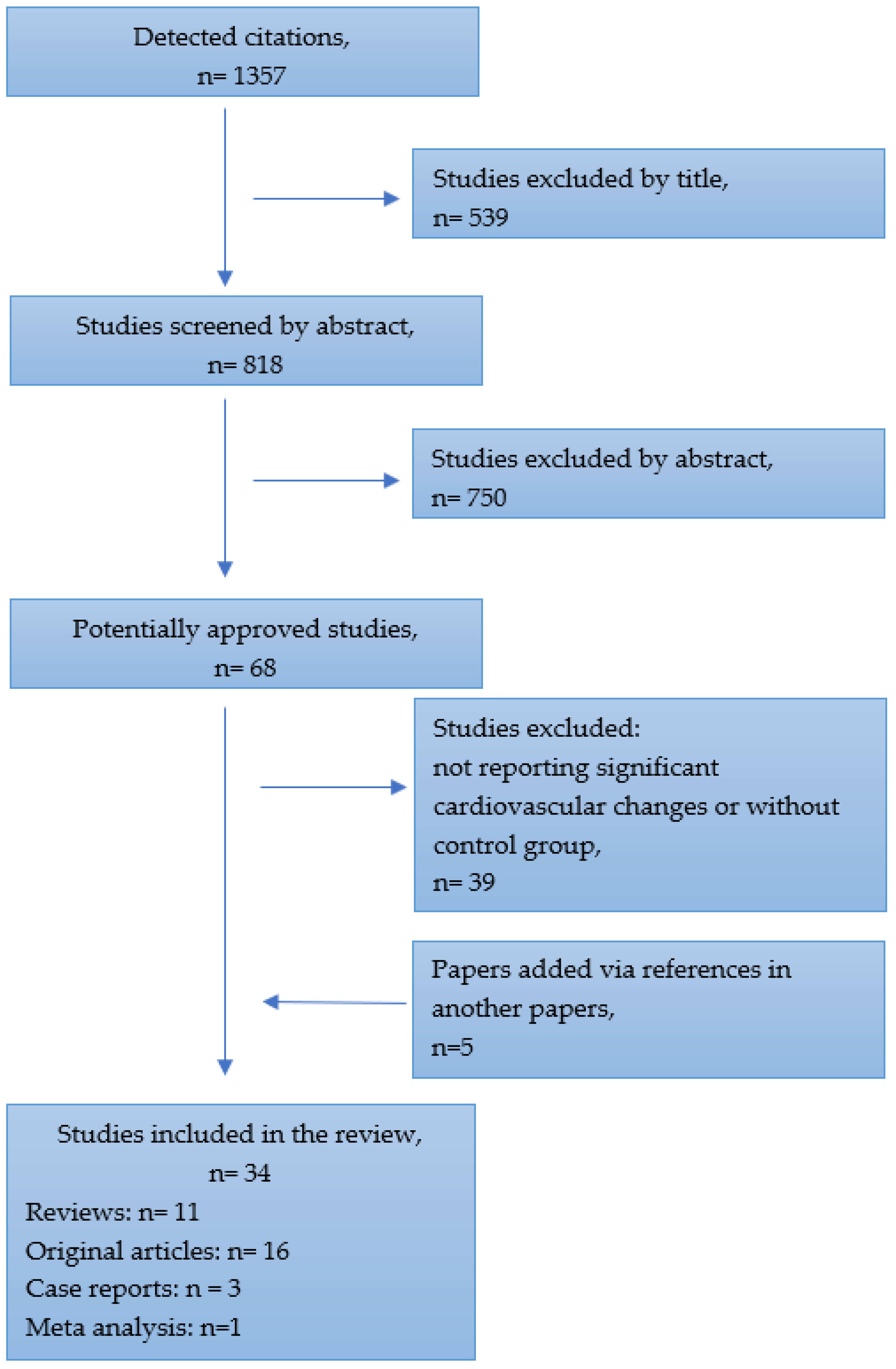
2. Materials and Methods
3. Results
3.1. General Characteristics of the Paralympian’s Cardiovascular System
- Prepare a plan for prolonging period of altitude acclimatisation;
- Monitor the load during training, competitions and daily life;
- Carefully monitor the competitors for hypothermia and deal with signs of it earlier in athletes with SCI than in able-bodied athletes [10].
3.2. Heart Rate and Electrocardiographic Features in Paralympian Group
3.3. Cardiovascular Abnormalities in Paralympians
4. Conclusions
5. Future Research Directions
6. Limitations of the Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theisen, D. Cardiovascular determinants of exercise capacity in the Paralympic athlete with spinal cord injury. Exp. Physiol. 2012, 97, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Adami, P.E.; Quattrini, F.; Squeo, M.R.; Caselli, S.; Verdile, L.; Maestrini, V.; Di Paolo, F.; Pisicchio, C.; Ciardo, R.; et al. Are Olympic athletes free from cardiovascular diseases? Systematic investigation in 2352 participants from Athens 2004 to Sochi 2014. Br. J. Sports Med. 2016, 51, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Fukushima, Y.; Fukao, K.; Shiozaki, M.; Hiki, M.; Aihara, K.; Daida, H. A comprehensive Approach for Preventing Cardiovascular Events During Olympic and Paralympic Games. Juntendo Med. J. 2020, 66, 38–49. [Google Scholar] [CrossRef]
- Kochi, A.N.; Vettor, G.; Dessanai, M.A.; Pizzamiglio, F.; Tondo, C. Sudden Cardiac Death in Athletes: From the Basics to the Practical Work-Up. Medicina 2021, 57, 168. [Google Scholar] [CrossRef] [PubMed]
- Yekutiel, M.; E Brooks, M.; Ohry, A.; Yarom, J.; Carel, R.S. The prevalence of hypertension, ischaemic heart disease and diabetes in traumatic spinal cord injured patients and amputees. Spinal Cord 1989, 27, 58–62. [Google Scholar] [CrossRef]
- Toresdahl, B.G.; Blauwet, C.; Chang, C.J.; I Ling, D.; Asif, I.M. Cardiovascular screening of Paralympic athletes reported by chief medical officers of the PyeongChang 2018 Paralympic Winter Games. Br. J. Sports Med. 2018, 53, 43–44. [Google Scholar] [CrossRef]
- Webborn, N.; Van de Villet, P. Paralympic medicine. Lancet 2012, 380, 65–71. [Google Scholar] [CrossRef]
- Pelliccia, A.; Quattrini, F.M.; Cavarretta, E.; Squeo, M.R.; Adami, P.E.; Di Paolo, F.M.; Spataro, A.; Bernardi, M. Physiologic and Clinical Features of the Paralympic Athlete’s Heart. JAMA Cardiol. 2021, 6, 30–39. [Google Scholar] [CrossRef]
- De Bosscher, R.; Dausin, C.; Janssens, K.; Bogaert, J.; Elliott, A.; Ghekiere, O.; Van De Heyning, C.M.; Sanders, P.; Kalman, J.; Fatkin, D.; et al. Rationale and design of the PROspective ATHletic Heart (Pro@Heart) study: Long-term assessment of the determinants of cardiac remodelling and its clinical consequences in endurance athletes. BMJ Open Sport Exerc. Med. 2022, 8, e001309. [Google Scholar] [CrossRef]
- Fagher, K.; Baumgart, J.K.; Solli, G.S.; Holmberg, H.C.; Lexell, J.; Sandbakk, Ø. Preparing for snow-sport events at the Paralympic Games in Beijing in 2022: Recommendations and remaining questions. BMJ Open Sport Exerc. Med. 2022, 8, e001294. [Google Scholar] [CrossRef]
- Handrakis, J.P.; Trbovich, M.; Hagen, E.M.; Price, M. Thermodysregulation in persons with spinal cord injury: Case series on use of the autonomic standards. Spinal Cord Ser. Cases 2017, 3, 17086. [Google Scholar] [CrossRef]
- Griggs, K.E.; Stephenson, B.T.; Price, M.J.; Goosey-Tolfrey, V.L. Heat-related issues and practical applications for Paralympic athletes at Tokyo 2020. Temperature 2019, 7, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Alkemade, P.; Daanen, H.A.M.; Janssen, T.W.J.; Broad, E.; Goosey-Tolfrey, V.L.; Ibusuki, T.; Kneepkens, H.; Périard, J.D.; Eijsvogels, T.M.H. Heat preparedness and exertional heat illness in Paralympic athletes: A Tokyo 2020 survey. Temperature 2022, 9, 1–12. [Google Scholar] [CrossRef]
- Cruz, S.; Blauwet, C.A. Implications of altered autonomic control on sports performance in athletes with spinal cord injury. Auton. Neurosci. 2017, 209, 100–104. [Google Scholar] [CrossRef]
- Coutinho, M.; Vigario, P.; Lopes, A.; Guimaraes, F. Heart rate response and recovery in wheelchair tetraplegic rugby athletes: A pilot study. J. Sports Med. Phys. Fit. 2018, 58, 1349–1353. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Lee, M.; Kiratli, J. Cardiovascular Disease in Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2007, 86, 142–152. [Google Scholar] [CrossRef]
- Krassioukov, A.; Claydon, V. The clinical problems in cardiovascular control following spinal cord injury: An overview. Prog. Brain Res. 2006, 152, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.; Krassioukov, A. Contemporary Cardiovascular Concern after Spinal Cord Injury: Mechanisms, Maladaptations and Management. J. Neurotrauma 2015, 32, 1927–1942. [Google Scholar] [CrossRef]
- Jacobs, P.L.; Nash, M.S. Exercise Recommendations for Individuals with Spinal Cord Injury. Sports Med. 2004, 34, 727–751. [Google Scholar] [CrossRef]
- Squair, J.W.; Phillips, A.A.; Currie, K.D.; Gee, C.; Krassioukov, A.V. Autonomic testing for prediction of competition performance in Paralympic athletes. Scand. J. Med. Sci. Sports 2017, 28, 311–318. [Google Scholar] [CrossRef]
- A Bauman, W.; Spungen, A.M. Coronary heart disease in individuals with spinal cord injury: Assessment of risk factors. Spinal Cord 2008, 46, 466–476. [Google Scholar] [CrossRef]
- Baumgart, J.K.; Gürtler, L.; Ettema, G.; Sandbakk, Ø. Comparison of peak oxygen uptake and exercise efficiency between upper-body poling and arm crank ergometry in trained paraplegic and able-bodied participants. Eur. J. Appl. Physiol. 2018, 118, 1857–1867. [Google Scholar] [CrossRef]
- Marais, G.; Dupont, L.; Maillet, M.; Weissland, T.; Vanvelcenaher, J.; Pelayo, P. Cardiorespiratory and efficiency responses during arm and leg exercise with spontaneously chosen crank and pedal rates. Ergonomics 2002, 45, 631–639. [Google Scholar] [CrossRef]
- Hou, S.; Rabchevsky, A. Autonomic consequences of spinal cord injury. Compr. Physiol. 2014, 4, 1419–1453. [Google Scholar] [CrossRef] [PubMed]
- Tom, V.J.; Partida, E.; Mironets, E.; Hou, S. Cardiovascular dysfunction following spinal cord injury. Neural Regen. Res. 2016, 11, 189–194. [Google Scholar] [CrossRef]
- Popa, C.; Popa, F.; Grigorean, V.; Onose, G.; Sandu, A.; Popescu, M.; Burnei, G.; Strambu, V.; Sinescu, C. Vascular dysfunctions following spinal cord injury. J. Med. Life 2010, 3, 275–285. [Google Scholar]
- Williams, A.M.; Gee, C.M.; Voss, C.; West, C.R. Cardiac consequences of spinal cord injury systematic review and meta-analysis. Heart 2019, 105, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Guerra, E.; DI Giacinto, B.; DI Cesare, A.; Castellano, V.; Bhambhani, Y. Field Evaluation of Paralympic Athletes in Selected Sports. Med. Sci. Sports Exerc. 2010, 42, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Culasso, F.; Di Paolo, F.M.; Maron, B.J. Physiologic Left Ventricular Cavity Dilatation in Elite Athletes. Ann. Intern. Med. 1999, 130, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Maron, B.J.; Spataro, A.; Proschan, M.A.; Spirito, P. The Upper Limit of Physiologic Cardiac Hypertrophy in Highly Trained Elite Athletes. N. Engl. J. Med. 1991, 324, 295–301. [Google Scholar] [CrossRef]
- Bernardi, M.; Guerra, E.; Rodio, A.; Dante, D.; Castellano, V.; Peluso, I.; Schena, F.; Bhambhani, Y. Assessment of Exercise Stroke Volume and Its Prediction From Oxygen Pulse in Paralympic Athletes With Locomotor Impairments: Cardiac Long-Term Adaptations Are Possible. Front. Physiol. 2020, 10, 1451. [Google Scholar] [CrossRef]
- Pelliccia, A.; Maron, B.J.; Culasso, F.; Di Paolo, F.M.; Spataro, A.; Biffi, A.; Caselli, G.; Piovano, P. Clinical Significance of Abnormal Electrocardiographic Patterns in Trained Athletes. Circulation 2000, 102, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Drezner, J.A.; Baggish, A.; Papadakis, M.; Wilson, M.G.; Prutkin, J.M.; La Gerche, A.; Ackerman, M.J.; Börjesson, M.; Salerno, J.C.; et al. International recommendations for electrocardiographic interpretation in athletes. Eur. Heart J. 2018, 39, 1466–1480. [Google Scholar] [CrossRef]
- Sheikh, N.; Papadakis, M.; Ghani, S.; Zaidi, A.; Gati, S.; Adami, P.E.; Carré, F.; Schnell, F.; Wilson, M.; Avila, P.; et al. Comparison of Electrocardiographic Criteria for the Detection of Cardiac Abnormalities in Elite Black and White Athletes. Circulation 2014, 129, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, M.; Basavarajaiah, S.; Rawlins, J.; Edwards, C.; Makan, J.; Firoozi, S.; Carby, L.; Sharma, S. Prevalence and significance of T-wave inversions in predominantly Caucasian adolescent athletes. Eur. Heart J. 2009, 30, 1728–1735. [Google Scholar] [CrossRef]
- Pelliccia, A.; Quattrini, F.M.; Squeo, M.R.; Caselli, S.; Culasso, F.; Link, M.S.; Spataro, A.; Bernardi, M. Cardiovascular diseases in Paralympic athletes. Br. J. Sports Med. 2016, 50, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Oliveira Filho, J.A.; Silva, A.C.; Lira Filho, E.; Luna Filho, B.; Covre, S.H.; Lauro, F.A.; Danucalov, M.A.; Leite, W.A.; Tuffik, S.; Andrade, J.L.; et al. Athlete’s heart in elite disabled athletes. Arq. Bras. Cardiol. 1997, 69, 385–388. [Google Scholar] [PubMed]
- Aidar, F.J.; Paz, D.A.; Gama, D.d.M.; de Souza, R.F.; Souza, L.M.V.; dos Santos, J.L.; Almeida-Neto, P.F.; Marçal, A.C.; Neves, E.B.; Moreira, O.C.; et al. Evaluation of the Post-Training Hypotensor Effect in Paralympic and Conventional Powerlifting. J. Funct. Morphol. Kinesiol. 2021, 6, 92. [Google Scholar] [CrossRef]
- Paz, D.A.; Aidar, F.J.; de Matos, D.G.; de Souza, R.F.; da Silva-Grigoletto, M.E.; Tillaar, R.V.D.; Ramirez-Campillo, R.; Nakamura, F.Y.; Costa, M.D.C.; Nunes-Silva, A.; et al. Comparison of Post-Exercise Hypotension Responses in Paralympic Powerlifting Athletes after Completing Two Bench Press Training Intensities. Medicina 2020, 56, 156. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Furberg, C.D.; Psaty, B.M.; Siscovick, D. Physical Activity and Incidence of Atrial Fibrillation in Older Adults. Circulation 2008, 118, 800–807. [Google Scholar] [CrossRef]
- Aizer, A.; Gaziano, J.M.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Albert, C. Relation of Vigorous Exercise to Risk of Atrial Fibrillation. Am. J. Cardiol. 2009, 103, 1572–1577. [Google Scholar] [CrossRef] [PubMed]
- Drca, N.; Wolk, A.; Jensen-Urstad, M.; Larsson, S.C. Atrial fibrillation is associated with different levels of physical activity levels at different ages in men. Heart 2014, 100, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Calvo, N.; Ramos, P.; Montserrat, S.; Guasch, E.; Coll-Vinent, B.; Domenech, M.; Bisbal, F.; Hevia, S.; Vidorreta, S.; Borras, R.; et al. Emerging risk factors and the dose–response relationship between physical activity and lone atrial fibrillation: A prospective case–control study. EP Eur. 2015, 18, 57–63. [Google Scholar] [CrossRef]
- Abdulla, J.; Nielsen, J.R. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace 2009, 11, 1156–1159. [Google Scholar] [CrossRef] [PubMed]
- Glaser, R.M. Exercise and locomotion for the spinal cord injured. Exerc. Sport Sci. Rev. 1985, 13, 263–303. [Google Scholar] [CrossRef]


{kind=link}
| Total cardiovascular abnormalities | 12% |
| Arrhythmogenic cardiomyopathies | 1.12% |
| Aortic root dilation | 1.12% |
| Valvular diseases | 2.62% |
| Systemic hypertension | 4% |
| Ventricular or supraventricular tachyarrhythmias (atrial flutter, paroxysmal atrial fibrillation or STV) | 3.34% |
| Pathophysiological Changes | Probable Patomechanism |
|---|---|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawczuk, D.; Gać, P.; Poręba, R.; Poręba, M. The Prevalence of Cardiovascular Diseases in Paralympic Athletes. Healthcare 2023, 11, 1027. https://doi.org/10.3390/healthcare11071027
Sawczuk D, Gać P, Poręba R, Poręba M. The Prevalence of Cardiovascular Diseases in Paralympic Athletes. Healthcare. 2023; 11(7):1027. https://doi.org/10.3390/healthcare11071027
Chicago/Turabian StyleSawczuk, Diana, Paweł Gać, Rafał Poręba, and Małgorzata Poręba. 2023. "The Prevalence of Cardiovascular Diseases in Paralympic Athletes" Healthcare 11, no. 7: 1027. https://doi.org/10.3390/healthcare11071027
APA StyleSawczuk, D., Gać, P., Poręba, R., & Poręba, M. (2023). The Prevalence of Cardiovascular Diseases in Paralympic Athletes. Healthcare, 11(7), 1027. https://doi.org/10.3390/healthcare11071027