
Exploring Determinants of HIV/AIDS Self-Testing Uptake in South Africa Using Generalised Linear Poisson and Geographically Weighted Poisson Regression

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.2. Spatial Autocorrelation—Global Moran’s I
2.3. Generalised Linear Poisson Regression Modelling of Factors Associated with HIV/AIDS Self-Testing Uptake
2.4. Geographically Weighted Poisson Regression Modelling of Factors Associated with HIV/AIDS Self-Testing Uptake
2.5. Model Diagnostic Indicators
3. Results
3.1. District Level Spatial Autocorrelation Assessment
3.2. Generalised Linear Poisson Regression—Global Model
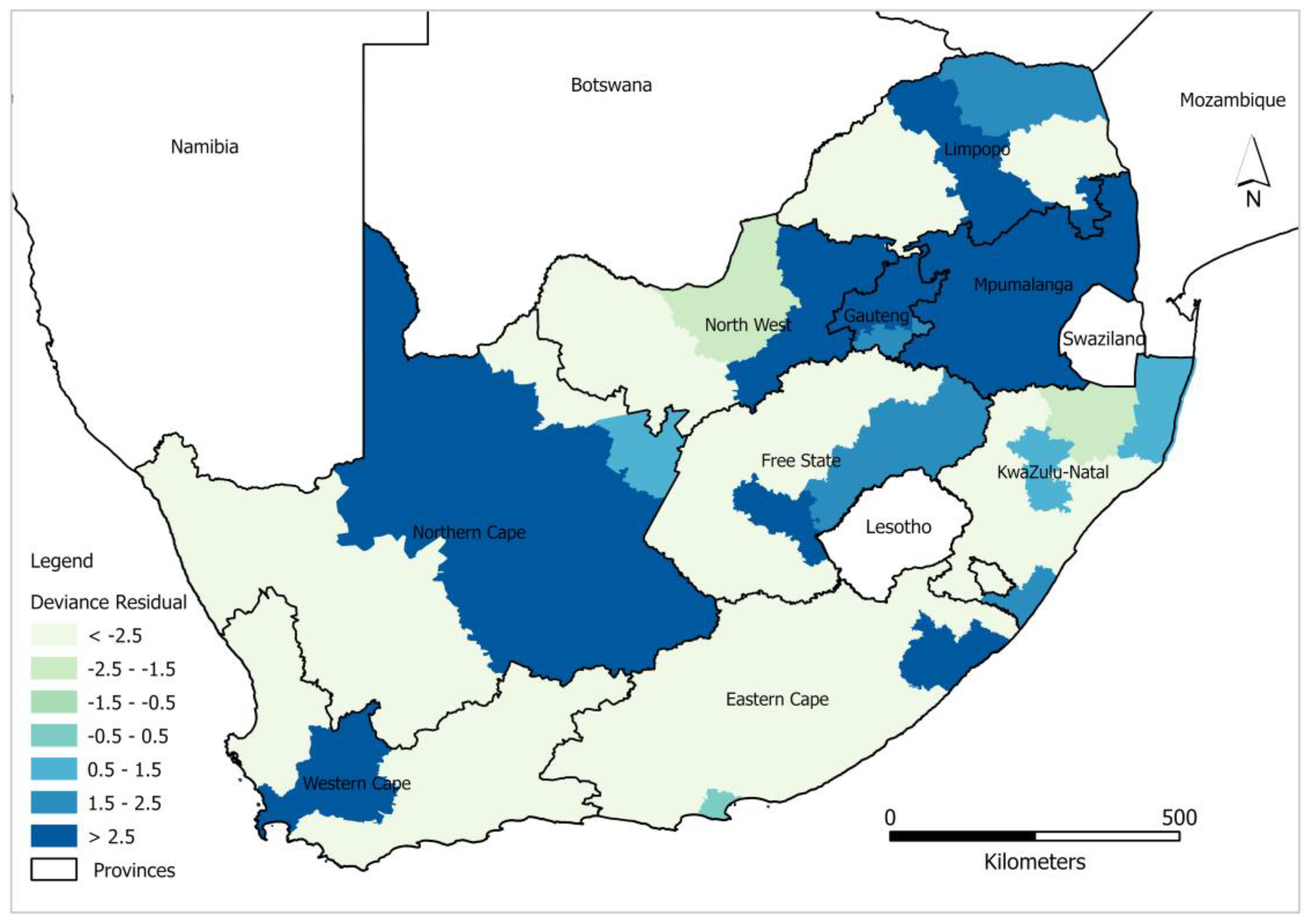
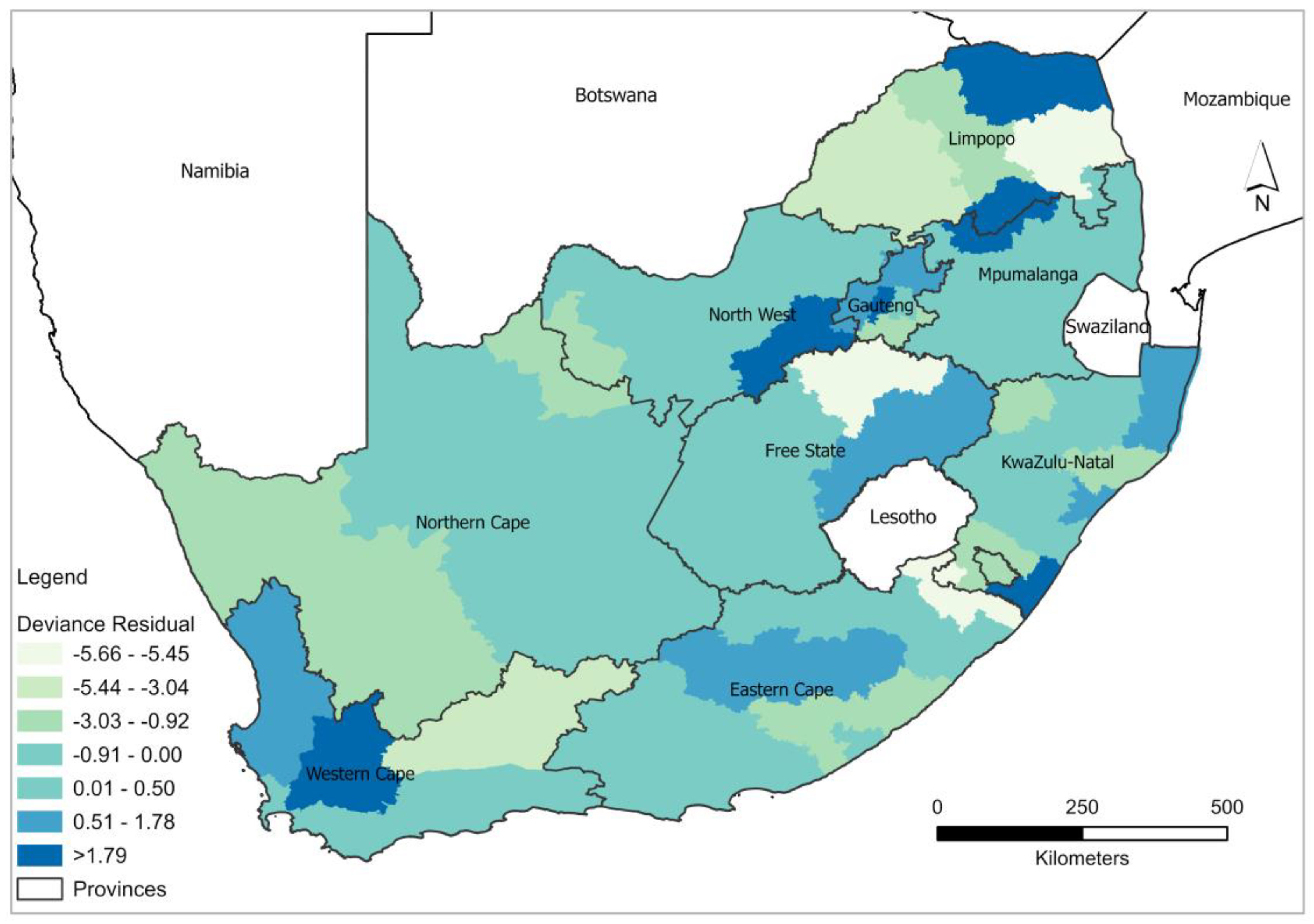
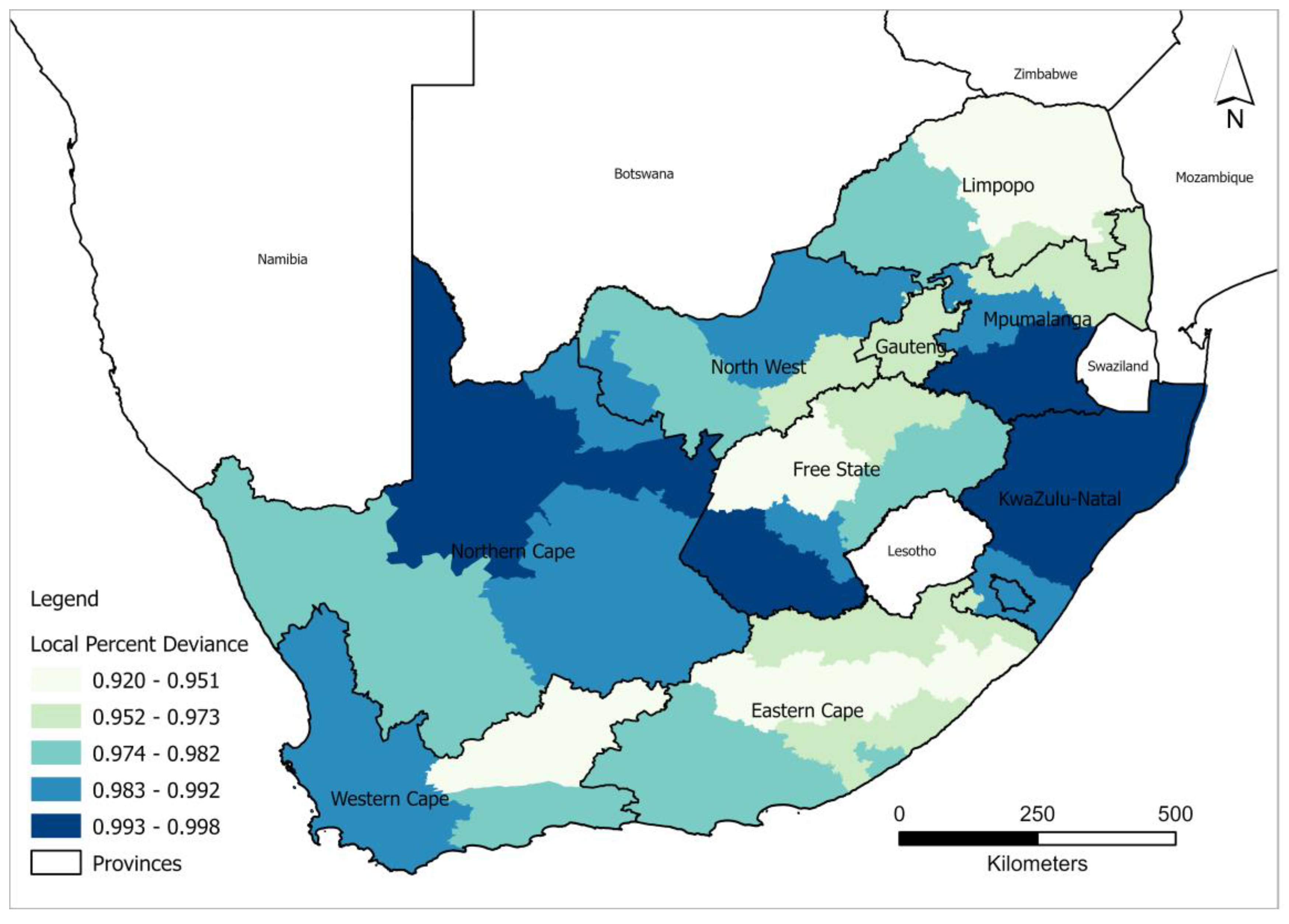
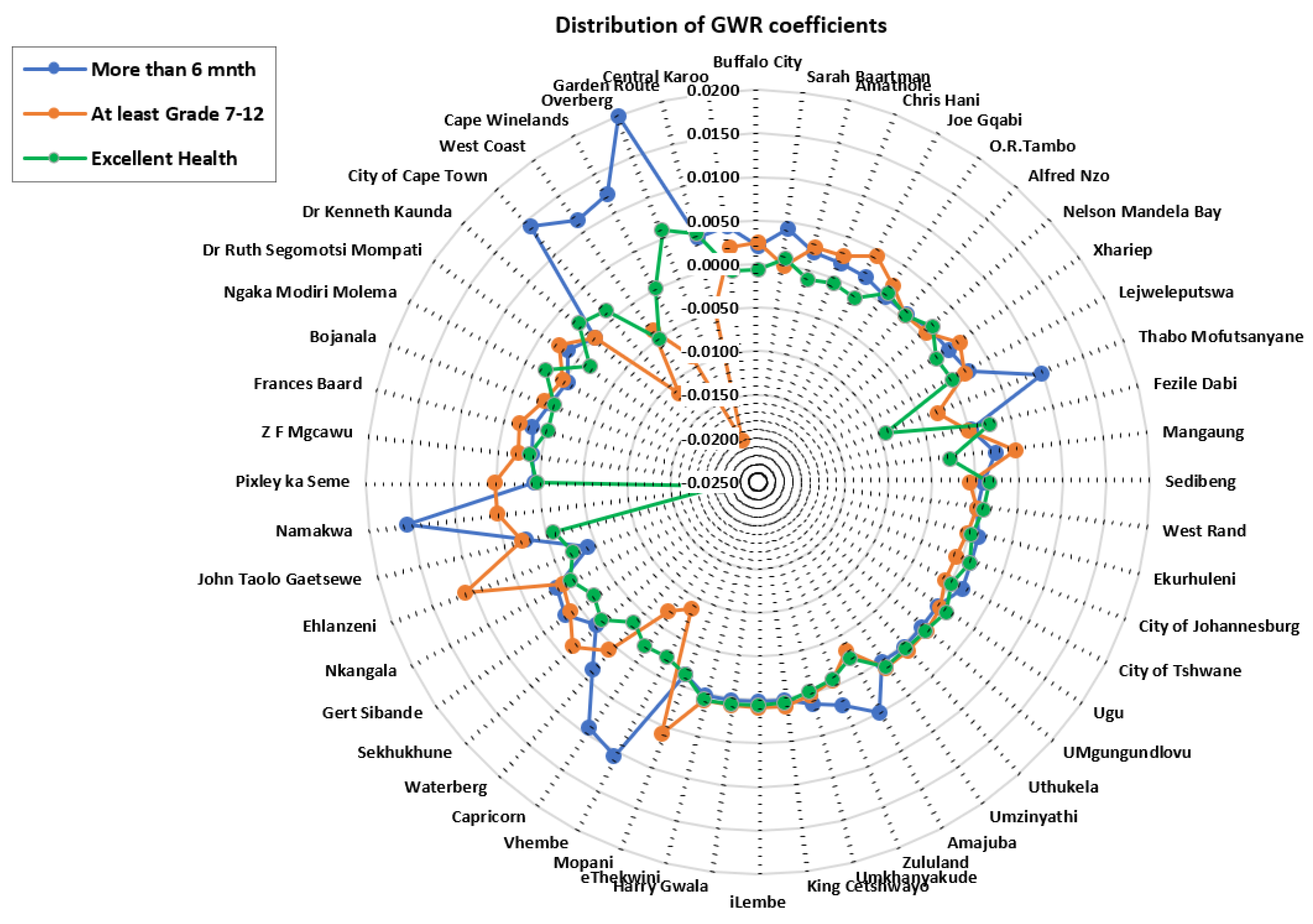
3.3. District Level Geographically Weighted Poisson Regression—Local Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, S.; Li, Z.; Zhang, H.; Jiang, H.; Hu, X. Analysis of HIV/AIDS Epidemic and Socioeconomic Factors in Sub-Saharan Africa. Entropy 2020, 22, 1230. [Google Scholar] [CrossRef] [PubMed]
- Jooste, S.; Mabaso, M.; Taylor, M.; North, A.; Shean, Y.; Simbayi, L.C. Socio-Economic Differences in the Uptake of HIV Testing and Associated Factors in South Africa. BMC Public Health 2021, 21, 1591. [Google Scholar] [CrossRef]
- Simbayi, L.; Zuma, K.; Zungu, N.; Moyo, S.; Marinda, E.; Jooste, S.; Mabaso, M.; Ramlagan, S.; North, A.; Van Zyl, J.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017: Towards Achieving the UNAIDS 90-90-90 Targets; HSRC Press: Cape Town, South Africa, 2019; ISBN 9780796924445. [Google Scholar]
- Ntsepe, Y.; Simbayi, L.C.; Shisana, O.; Rehle, T.; Mabaso, M.; Ncitakalo, N.; Davids, A.; Naidoo, Y.D. Perceptions about the Acceptability and Prevalence of HIV Testing and Factors Influencing Them in Different Communities in South Africa. SAHARA-J 2014, 11, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.F.; Dorrington, R.E.; Moolla, H. HIV Epidemic Drivers in South Africa: A Model-Based Evaluation of Factors Accounting for Inter-Provincial Differences in HIV Prevalence and Incidence Trends. South. Afr. J. HIV Med. 2017, 18, 1–9. [Google Scholar] [CrossRef]
- Zungu, N.; Mabaso, M.; Ramlagan, S.; Simbayi, L.; Moyo, S.; Shisana, O.; Murangandi, P.; Igumbor, E.; Sigida, S.; Jooste, S.; et al. Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey. Int. J. Environ. Res. Public Health 2022, 19, 6156. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. HIV Status, Knowledge, Attitudes and Behaviour of Persons with and without Disability in South Africa: Evidence from a National Population-Based Survey. Pan Afr. Med. J. 2019, 33, 302. [Google Scholar] [CrossRef]
- Mabaso, M.; Makola, L.; Naidoo, I.; Mlangeni, L.L.; Jooste, S.; Simbayi, L. HIV Prevalence in South Africa through Gender and Racial Lenses: Results from the 2012 Population-Based National Household Survey. Int. J. Equity Health 2019, 18, 167. [Google Scholar] [CrossRef] [PubMed]
- Nehl, E.J.; Klein, H.; Sterk, C.E.; Elifson, K.W. Prediction of HIV Sexual Risk Behaviors Among Disadvantaged African American Adults Using a Syndemic Conceptual Framework. AIDS Behav. 2016, 20, 449–460. [Google Scholar] [CrossRef]
- Chimoyi, L.; Matsena-Zingoni, Z.; Charalambous, S.; Marinda, E.; Manda, S.; Musenge, E. Assessing Spatial Patterns of HIV Prevalence and Interventions in Semi-Urban Settings in South Africa. Implications for Spatially Targeted Interventions. Geospat. Health 2022, 17. [Google Scholar] [CrossRef]
- Jooste, S.; Mabaso, M.; Taylor, M.; North, A.; Shean, Y.; Simbayi, L.C.; Reddy, T.; Mwandingi, L.; Schmidt, T.; Nevhungoni, P.; et al. Geographical Variation in HIV Testing in South Africa: Evidence from the 2017 National Household HIV Survey. South. Afr. J. HIV Med. 2021, 22. [Google Scholar] [CrossRef]
- Wand, H.; Morris, N.; Reddy, T. Temporal and Spatial Monitoring of HIV Prevalence and Incidence Rates Using Geospatial Models: Results from South African Women. Spat. Spatiotemporal. Epidemiol. 2021, 37, 100413. [Google Scholar] [CrossRef]
- Probst, C.; Parry, C.D.H.; Rehm, J. HIV/AIDS Mortality Attributable to Alcohol Use in South Africa: A Comparative Risk Assessment by Socioeconomic Status. BMJ Open 2018, 8, e017955. [Google Scholar] [CrossRef]
- Aavani, P.; Allen, L.J.S. The Role of CD4 T Cells in Immune System Activation and Viral Reproduction in a Simple Model for HIV Infection. Appl. Math. Model. 2019, 75, 210–222. [Google Scholar] [CrossRef]
- Alem, A.Z.; Liyew, A.M.; Guadie, H.A. Spatial Pattern and Associated Factors of HIV Testing and Counselling among Youths (15–24 Years) in Ethiopia. BMC Public Health 2021, 21, 644. [Google Scholar] [CrossRef] [PubMed]
- Gous, N.; Fischer, A.E.; Rhagnath, N.; Phatsoane, M.; Majam, M.; Lalla-Edward, S.T. Evaluation of a Mobile Application to Support HIV Self-Testing in Johannesburg, South Africa. South. Afr. J. HIV Med. 2020, 21, 1–7. [Google Scholar] [CrossRef]
- Harichund, C.; Moshabela, M.; Kunene, P.; Abdool Karim, Q. Acceptability of HIV Self-Testing among Men and Women in KwaZulu-Natal, South Africa. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2019, 31, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Jiang, Y.; Wedow, R.; Li, Y.; Brazel, D.M.; Chen, F.; Datta, G.; Davila-Velderrain, J.; McGuire, D.; Tian, C.; et al. Association Studies of Up to 1.2 Million Individuals Yield New Insights into the Genetic Etiology of Tobacco and Alcohol Use. Nat. Genet. 2019, 51, 237–244. [Google Scholar] [CrossRef]
- Mokgatle, M.M.; Madiba, S. High Acceptability of HIV Self-Testing among Technical Vocational Education and Training College Students in Gauteng and North West Province: What Are the Implications for the Scale up in South Africa? PLoS ONE 2017, 12, e0169765. [Google Scholar] [CrossRef]
- Nutor, J.J.; Duah, H.O.; Duodu, P.A.; Agbadi, P.; Alhassan, R.K.; Darkwah, E. Geographical Variations and Factors Associated with Recent HIV Testing Prevalence in Ghana: Spatial Mapping and Complex Survey Analyses of the 2014 Demographic and Health Surveys. BMJ Open 2021, 11, e045458. [Google Scholar] [CrossRef]
- Lippman, S.A.; Lane, T.; Rabede, O.; Gilmore, H.; Chen, Y.-H.; Mlotshwa, N.; Maleke, K.; Marr, A.; McIntyre, J.A. High Acceptability and Increased HIV-Testing Frequency After Introduction of HIV Self-Testing and Network Distribution Among South African MSM. JAIDS 2018, 77, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Tanser, F.C.; Kim, H.Y.; Mathenjwa, T.; Shahmanesh, M.; Seeley, J.; Matthews, P.; Wyke, S.; McGrath, N.; Adeagbo, O.; Sartorius, B.; et al. Home-Based Intervention to Test and Start (HITS): A Community-Randomized Controlled Trial to Increase HIV Testing Uptake among Men in Rural South Africa. J. Int. AIDS Soc. 2021, 24, e25665. [Google Scholar] [CrossRef]
- Zimmermann, H.M.L.; van Bilsen, W.P.H.; Boyd, A.; Prins, M.; van Harreveld, F.; Davidovich, U. Prevention Challenges with Current Perceptions of HIV Burden among HIV-Negative and Never-Tested Men Who Have Sex with Men in the Netherlands: A Mixed-Methods Study. J. Int. AIDS Soc. 2021, 24, e25715. [Google Scholar] [CrossRef]
- Witzel, T.C.; Rodger, A.J.; Burns, F.M.; Rhodes, T.; Weatherburn, P. HIV Self-Testing among Men Who Have Sex with Men (MSM) in the UK: A Qualitative Study of Barriers and Facilitators, Intervention Preferences and Perceived Impacts. PLoS ONE 2016, 11, e0162713. [Google Scholar] [CrossRef]
- Figueroa, C.; Johnson, C.; Verster, A.; Baggaley, R. Attitudes and Acceptability on HIV Self-Testing Among Key Populations: A Literature Review. AIDS Behav. 2015, 19, 1949–1965. [Google Scholar] [CrossRef] [PubMed]
- Human Science Research Council, S. South African National HIV Prevalence, HIV Incidence, Behaviour and Communication Survey (SABSSM) 2017: Combined—All Provinces. 2020. Available online: http://curation.hsrc.ac.za/doi-10.14749-1585345902 (accessed on 10 September 2022).
- Zuma, K.; Simbayi, L.; Zungu, N.; Moyo, S.; Marinda, E.; Jooste, S.; North, A.; Nadol, P.; Aynalem, G.; Igumbor, E.; et al. The HIV Epidemic in South Africa: Key Findings from 2017 National Population-Based Survey. Int. J. Environ. Res. Public Health 2022, 19, 8125. [Google Scholar] [CrossRef] [PubMed]
- Berendes, S.; Rimal, R.N. Addressing the Slow Uptake of HIV Testing in Malawi: The Role of Stigma, Self-Efficacy, and Knowledge in the Malawi BRIDGE Project. J. Assoc. Nurses AIDS Care 2011, 22, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Gumede, S.D.; Sibiya, M.N. Health Care Users’ Knowledge, Attitudes and Perceptions of Hiv Self-Testing at Selected Gateway Clinics at Ethekwini District, Kwazulu-Natal Province, South Africa. SAHARA-J 2018, 15, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Hoagland, B.; Torres, T.S.; Bezerra, D.R.B.; Benedetti, M.; Pimenta, C.; Veloso, V.G.; Grinsztejn, B. High Acceptability of PrEP Teleconsultation and HIV Self-Testing among PrEP Users during the COVID-19 Pandemic in Brazil. Braz. J. Infect. Dis. 2021, 25, 101037. [Google Scholar] [CrossRef]
- Mathews, A.; Conserve, D.; Mason, H.; Alston, L.M.; Rennie, S.; Tucker, J. ‘Informed and Empowered’: A Mixed-Methods Study of Crowdsourcing Contests to Promote Uptake of HIV Self-Testing Kits among African Americans. J. Virus Erad. 2020, 6, 74–80. [Google Scholar] [CrossRef]
- Muwanguzi, P.A.; Nasuuna, E.M.; Namimbi, F.; Osingada, C.P.; Ngabirano, T.D. Venues and Methods to Improve Professional Men’s Access to HIV Self-Testing and Linkage to HIV Prevention or Treatment: A Qualitative Study. BMC Health Serv. Res. 2021, 21, 1217. [Google Scholar] [CrossRef]
- Obiezu-Umeh, C.; Gbajabiamila, T.; Ezechi, O.; Nwaozuru, U.; Ong, J.J.; Idigbe, I.; Oladele, D.; Musa, A.Z.; Uzoaru, F.; Airhihenbuwa, C.; et al. Young People’s Preferences for HIV Self-Testing Services in Nigeria: A Qualitative Analysis. BMC Public Health 2021, 21, 67. [Google Scholar] [CrossRef]
- Sonko, I.; Chung, M.H.; Hou, W.H.; Chen, W.T.; Chang, P.C. Predictors of HIV Testing among Youth Aged 15–24 Years in The Gambia. PLoS ONE 2022, 17, e0263720. [Google Scholar] [CrossRef]
- Moran, P.A. Notes on Continuous Stochastic Phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Kianfar, N.; Mesgari, M.S. GIS-Based Spatio-Temporal Analysis and Modeling of COVID-19 Incidence Rates in Europe. Spat. Spatiotemporal. Epidemiol. 2022, 41, 100498. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, P.; Zhao, K.; Zhao, S. The Geographical Distribution and Influencing Factors of COVID-19 in China. Trop. Med. Infect. Dis. 2022, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Mollalo, A.; Tatar, M. Spatial Modeling of COVID-19 Vaccine Hesitancy in the United States. Int. J. Environ. Res. Public Health 2021, 18, 9488. [Google Scholar] [CrossRef]
- Powers, S.L.; Matthews, S.A.; Mowen, A.J. Does the Relationship between Racial, Ethnic, and Income Diversity and Social Capital Vary across the United States? A County-Level Analysis Using Geographically Weighted Regression. Appl. Geogr. 2021, 130, 102446. [Google Scholar] [CrossRef]
- Wang, S.; Wu, J. Spatial Heterogeneity of the Associations of Economic and Health Care Factors with Infant Mortality in China Using Geographically Weighted Regression and Spatial Clustering. Soc. Sci. Med. 2020, 263, 113287. [Google Scholar] [CrossRef]
- Wedderburn, R.W.M. Generalized Linear Models Specified in Terms of Constraints. J. R. Stat. Soc. Ser. B 1974, 36, 449–454. [Google Scholar] [CrossRef]
- Lambert, D. Zero-Inflated Poisson Regression, with an Application to Defects in Manufacturing. Technometrics 1992, 34, 1–14. [Google Scholar] [CrossRef]
- Wu, Z. Generalized Linear Models in Family Studies. J. Marriage Fam. 2005, 67, 1029–1047. [Google Scholar] [CrossRef]
- Lotfata, A.; Tomal, M. Exploring Housing Determinants of Obesity Prevalence Using Multiscale Geographically Weighted Regression in Chicago, Illinois. Prof. Geogr. 2022, 1–10. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically Weighted Regression: A Method for Exploring Spatial Nonstationarity. Geogr. Anal. 1996, 28, 431–443. [Google Scholar] [CrossRef]
- Tang, J.; Gao, F.; Liu, F.; Han, C.; Lee, J. Spatial Heterogeneity Analysis of Macro-Level Crashes Using Geographically Weighted Poisson Quantile Regression. Accid. Anal. Prev. 2020, 148, 105833. [Google Scholar] [CrossRef] [PubMed]
- Nakaya, T.; Nakase, K.; Osaka, K. Spatio-Temporal Modelling of the HIV Epidemic in Japan Based on the National HIV/AIDS Surveillance. J. Geogr. Syst. 2005, 7, 313–336. [Google Scholar] [CrossRef]
- Munira, S.; Sener, I.N. A Geographically Weighted Regression Model to Examine the Spatial Variation of the Socioeconomic and Land-Use Factors Associated with Strava Bike Activity in Austin, Texas. J. Transp. Geogr. 2020, 88, 102865. [Google Scholar] [CrossRef]
- Aikaike, H. Information Theory and an Extension of the Maximum Likelihood Principle. In 2nd International Symposium on Information Theory; Petrov, B.N., Csaki, F., Eds.; Akadémiai Kiadó: Budapest, Hungary, 1973; pp. 267–281. [Google Scholar]
- Wabiri, N.; Shisana, O.; Zuma, K.; Freeman, J. Assessing the Spatial Nonstationarity in Relationship between Local Patterns of HIV Infections and the Covariates in South Africa: A Geographically Weighted Regression Analysis. Spat. Spatiotemp. Epidemiol. 2016, 16, 88–99. [Google Scholar] [CrossRef]
- Sambisa, W.; Curtis, S.; Mishra, V. AIDS Stigma as an Obstacle to Uptake of HIV Testing: Evidence from a Zimbabwean National Population-Based Survey. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2010, 22, 170–186. [Google Scholar] [CrossRef]
- Wood, B.R.; Ballenger, C.; Stekler, J.D. Arguments for and against HIV Self-Testing. HIV/AIDS-Res. Palliat. Care 2014, 6, 117–126. [Google Scholar] [CrossRef]
- Rahman, A.K.M.A.; Islam, S.K.S.; Sufian, M.A.; Talukder, M.H.; Ward, M.P.; Martínez-López, B. Foot-and-Mouth Disease Space-Time Clusters and Risk Factors in Cattle and Buffalo in Bangladesh. Pathogens 2020, 9, 423. [Google Scholar] [CrossRef] [PubMed]
- Matthews, S.A.; Yang, T.C. Mapping the Results of Local Statistics: Using Geographically Weighted Regression. Demogr. Res. 2012, 26, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.J.; Moon, S.; Cho, S.M. Effects of Access to Food Retailers and Convenience of Public Transportation on Residents’ Fresh Food Intake and Body Mass Index. J. Transp. Health 2022, 26, 101408. [Google Scholar] [CrossRef]
- Nicholls, E.J.; Samba, P.; McCabe, L.; Gafos, M.; Philips, A.N.; Trevelion, R.; Rodger, A.J.; Burns, F.M.; Weatherburn, P.; Witzel, T.C. Experiences of and Attitudes towards HIV Testing for Asian, Black and Latin American Men Who Have Sex with Men (MSM) in the SELPHI (HIV Self-Testing Public Health Intervention) Randomized Controlled Trial in England and Wales: Implications for HIV Self-Te. BMC Public Health 2022, 22, 809. [Google Scholar] [CrossRef] [PubMed]
- Sam-Agudu, N.A.; Folayan, M.O.; Ezeanolue, E.E. Seeking Wider Access to HIV Testing for Adolescents in Sub-Saharan Africa. Pediatr. Res. 2016, 79, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Morris-Paxton, A.A.; Reid, S.; Ewing, R.M.G. Primary Healthcare Services in the Rural Eastern Cape, South Africa: Evaluating a Service-Support Project. Afr. J. Prim. Health Care Fam. Med. 2020, 12, a2207. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description of Covariates | |
|---|---|---|
| Outcome Variable | Self-testing uptake | If an HIV self-test kit was available to you, would you be willing to use it to test yourself? |
| Explanatory Variables | Excellent health | In general, would you say that your health is excellent? |
| More than 6 months | When was the last time you went to see a health professional? | |
| At least Grade 7 up to Grade 12 | What is the highest educational level that you obtained? |
| Model Type | AICc | Percentage Deviance Explained |
|---|---|---|
| Global Model—GLRP | 2552 | 0.88 |
| Local Model—GWRP | 390 | 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fundisi, E.; Dlamini, S.; Mokhele, T.; Weir-Smith, G.; Motolwana, E. Exploring Determinants of HIV/AIDS Self-Testing Uptake in South Africa Using Generalised Linear Poisson and Geographically Weighted Poisson Regression. Healthcare 2023, 11, 881. https://doi.org/10.3390/healthcare11060881
Fundisi E, Dlamini S, Mokhele T, Weir-Smith G, Motolwana E. Exploring Determinants of HIV/AIDS Self-Testing Uptake in South Africa Using Generalised Linear Poisson and Geographically Weighted Poisson Regression. Healthcare. 2023; 11(6):881. https://doi.org/10.3390/healthcare11060881
Chicago/Turabian StyleFundisi, Emmanuel, Simangele Dlamini, Tholang Mokhele, Gina Weir-Smith, and Enathi Motolwana. 2023. "Exploring Determinants of HIV/AIDS Self-Testing Uptake in South Africa Using Generalised Linear Poisson and Geographically Weighted Poisson Regression" Healthcare 11, no. 6: 881. https://doi.org/10.3390/healthcare11060881
APA StyleFundisi, E., Dlamini, S., Mokhele, T., Weir-Smith, G., & Motolwana, E. (2023). Exploring Determinants of HIV/AIDS Self-Testing Uptake in South Africa Using Generalised Linear Poisson and Geographically Weighted Poisson Regression. Healthcare, 11(6), 881. https://doi.org/10.3390/healthcare11060881