
Dentistry and Gender Gap: An Overview of the Italian Situation

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Description of the Objects of Investigation
2.2. Institutional Roles in National and Local Dental Boards
2.3. Roles in ANDI
2.4. CME Speakers
2.5. Statistical Analysis
- (1)
- Differences between the two genders’ distributions in the roles within the INSTITUTIONAL and UNION boards;
- (2)
- The representation of male and female dentists in the INSTITUTIONAL and UNION boards;
- (3)
- The influence of any discipline in the CME events on the gender distribution.
3. Results
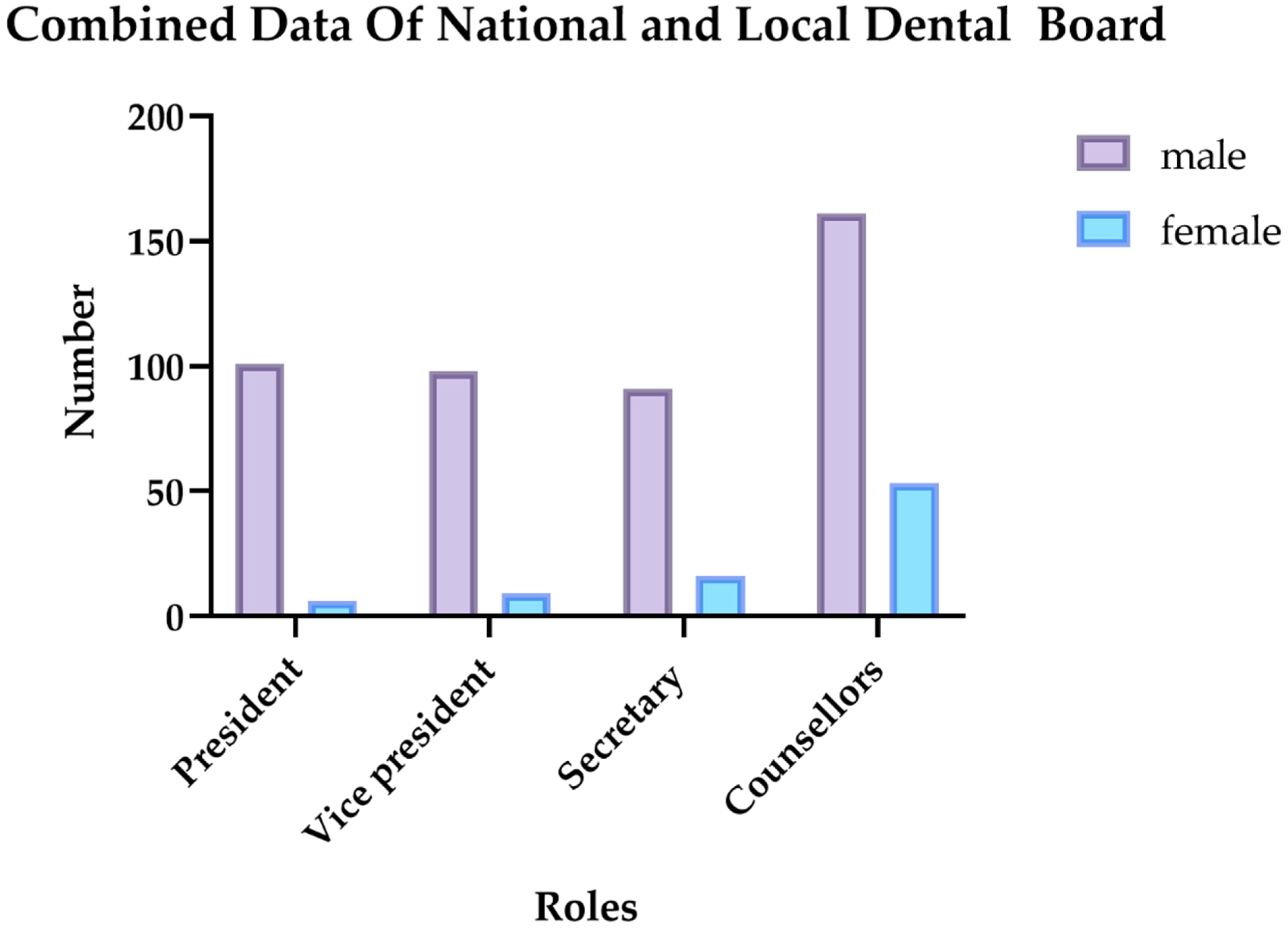
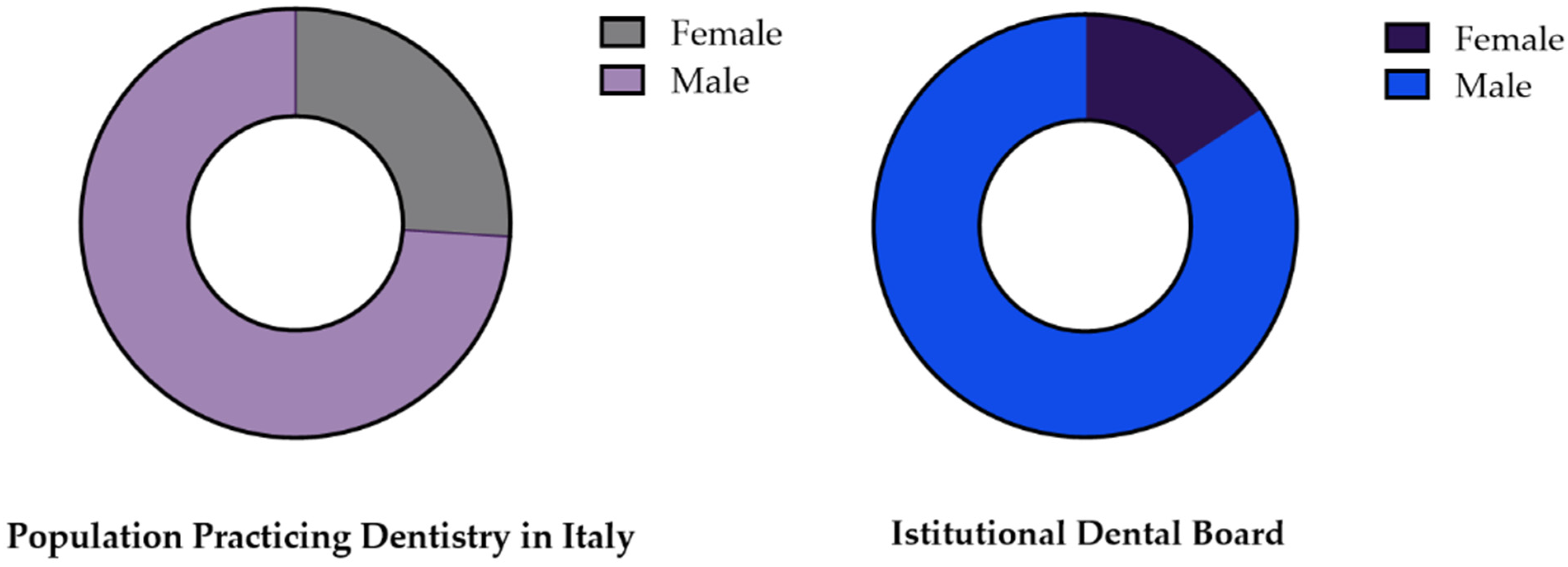
3.1. INSTITUTIONAL Roles in National and Local Dental Boards
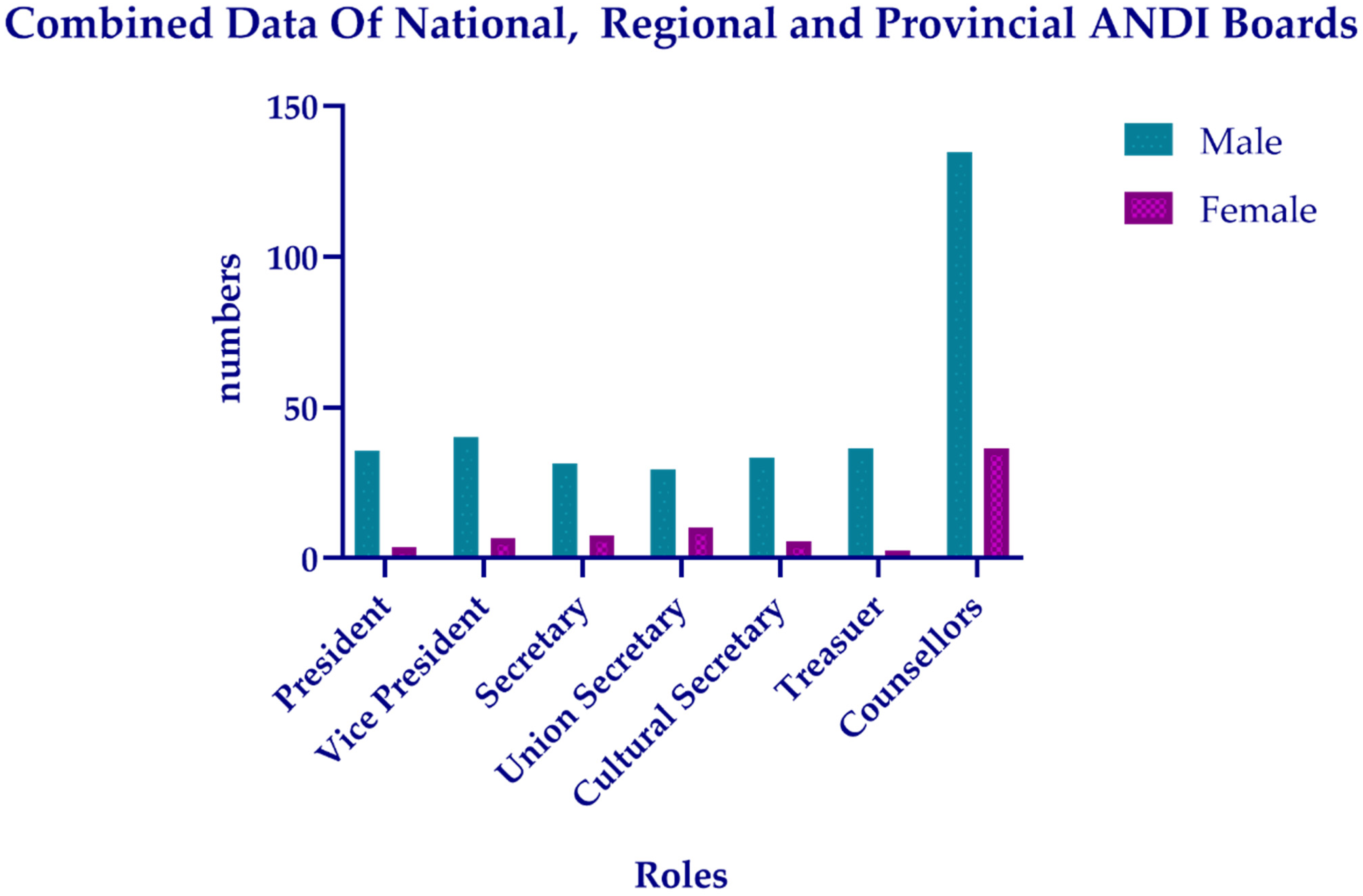
3.2. UNION Roles in ANDI
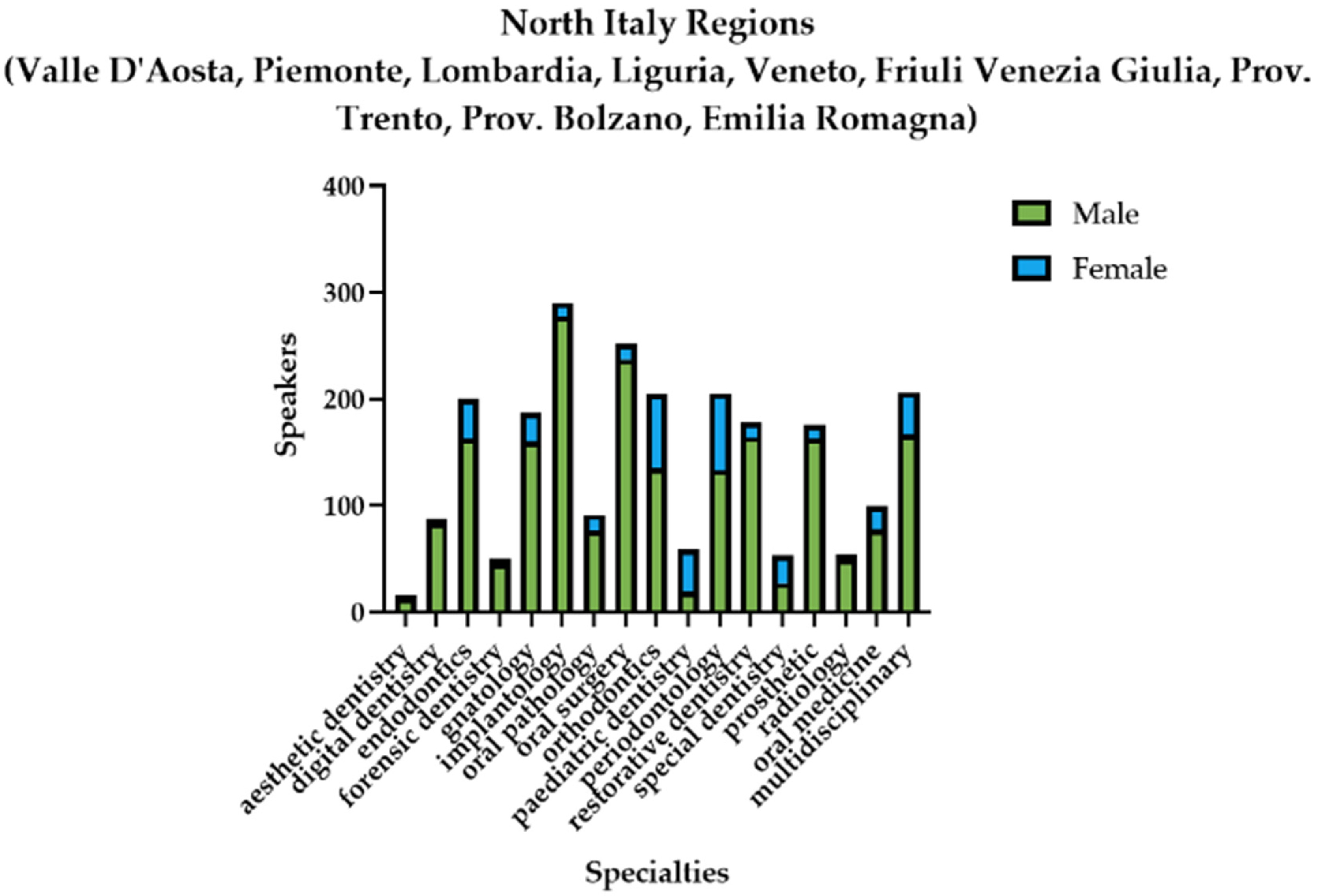
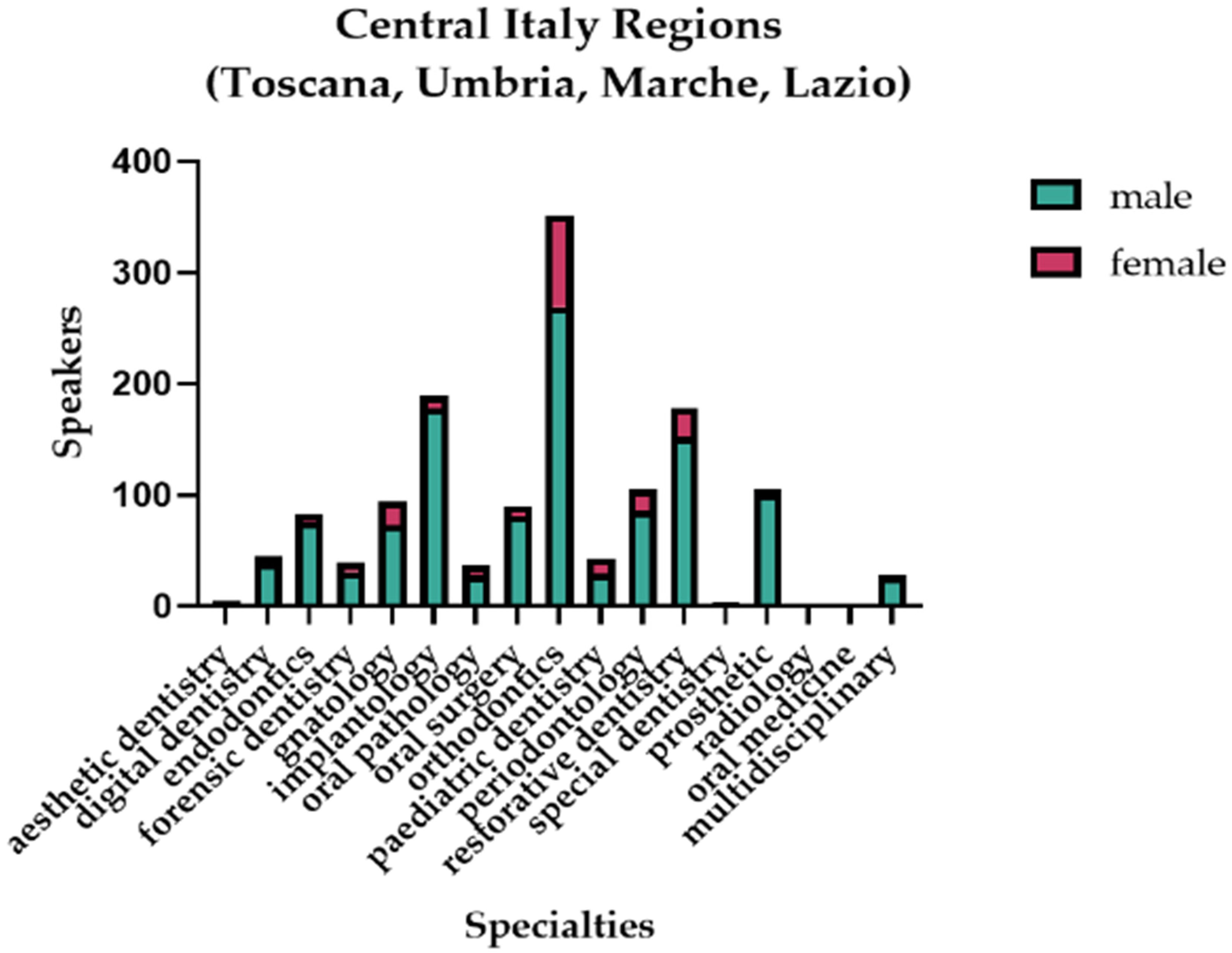
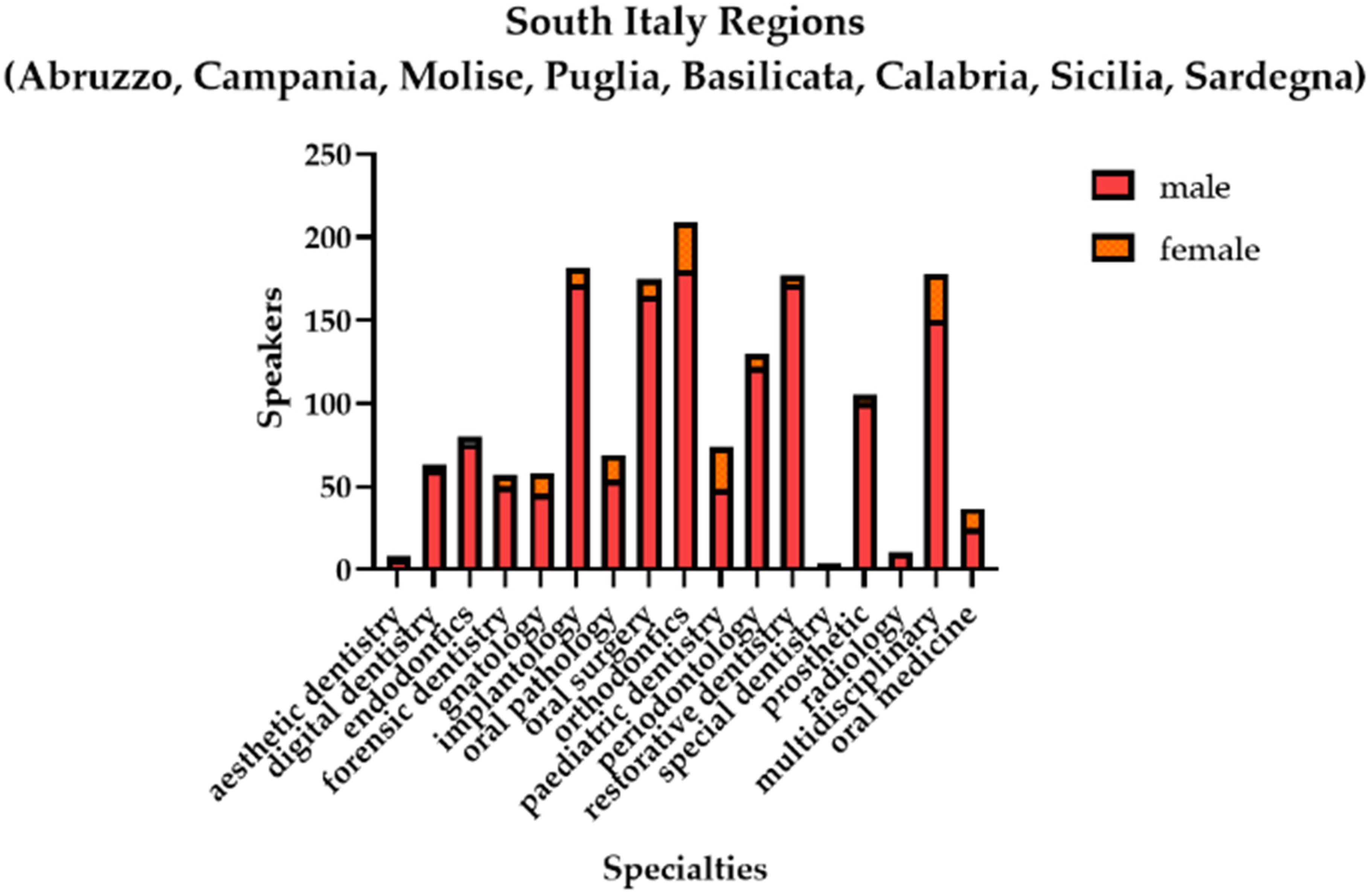
3.3. CME Speakers
4. Discussion
4.1. 2018–2021: Dental Boards and Category Association: The Glass Ceiling Effect
4.2. Invited Speakers Have Been Men-Made
4.3. Future Perspectives
- (1)
- The National Recovery and Resilience Plan (NRRP) has the aim of guaranteeing the same economic and social opportunities for men and women with reforms, education, and investments, with a view of gender mainstreaming by breaking down gender and generational discrimination. It fits into the path traced by the European Union Strategy and is built starting from a long-term vision [35]. The plan impacts dental professionals regarding female leadership and support in parenthood. In particular, NRRP includes the “Female enterprise fund” to support female entrepreneurship, impacting women in the third sector, such as private dental practices, and achieving more significant gender equality. The fund intends to financially support the creation of new women-owned businesses (of less than 12 months) and the development and consolidation of existing women-owned businesses (of more than 12 months). The expenses eligible for the fund are related to tangible fixed assets (machinery, plants, equipment, and building renovation work) for a maximum of 30% of the total eligible expense and intangible fixed assets (software, patents, licenses, and trademarks), cloud services (that are functional to the core processes of company management), employees (hired temporarily or permanently), working capital (raw materials, consumables, services, and rents), and leasing for a maximum of 20% of the total eligible expense (or 25% for enterprises of 36 months). The fund aims to finance 2400 companies by June 2026.
- (2)
- The Gender Equality Certification System started in 2021. The aim of the project is the definition of a national gender equality certification system that accompanies and encourages the adoption of adequate policies to reduce the gender gap in all the most “critical” areas “(growth opportunities, equal pay for equal jobs, gender difference management policies, and maternity protection) [36]. The project is coordinated by the Department for Equal Opportunities in collaboration with the Ministry of Labor and Social Policies and the Ministry of Economic Development [36]. The measures of this project can affect private dental clinics in the improvement of the quality of the work of their female dentists, offering equal growth and formation opportunities.
- (3)
- Establishment of a Parliamentary Commission for women’s rights and gender equality with “guideline and control” tasks (4 November 2019). The commission carries out investigations and monitoring activities on the presence of women in political-institutional life and in the world of public and private work in the country through the analysis of gender statistics elaborated by the responsible bodies, also promoting the balance between the professional and familial for women and men through the implementation of policies for the reconciliation between work and private life and the use of tools that encourage the sharing of family responsibilities [37]. This measure includes the possibility for new fathers to take “paternity leave” to allow the sharing of family responsibilities. In this case, dentists working in the public health system or working as employees can benefit from this measure to re-balance their working and career progression with family responsibilities.
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Gender and Health. Available online: https://www.who.int/health-topics/gender (accessed on 2 November 2022).
- Shannon, G.; Minckas, N.; Tan, D.; Haghparast-Bidgoli, H.; Batura, N.; Mannell, J. Feminisation of the health workforce and wage conditions of health professions: An exploratory analysis. Hum. Resour. Health 2019, 17, 84. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Ruiz, R.E.; Rosel-Gallardo, E.M.; Cifuentes-Jiménez, C.; González-López, S.; Bolaños-Carmona, M.V. Gender and Leadership Positions in Spanish Dentistry. Inquiry 2022, 59. [Google Scholar] [CrossRef]
- Phasuk, K.; Koka, S.; Kattadiyil, M.T.; Mutluay, M. Leadership diversity in prosthodontics: Number of women and nonwhite individuals serving as President of selected prosthodontic organizations in the last 20 years. J. Prosthet. Dent. 2021, 125, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; de Souza, R.; Esfandiari, S.; Feine, J. Have Women Broken the Glass Ceiling in North American Dental Leadership? Adv. Dent. Res. 2019, 30, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Cerutti, F. Odontoiatria, una Professione Sempre più Femminile? Available online: https://www.ildentistamoderno.com/odontoiatria-una-professione-sempre-piu-femminile/ (accessed on 20 November 2022).
- Di Fede, O.; Majorana, A.; Manfredi, M.; Pentenero, M.; Giuliani, M. Odontoiatria di genere: La condizione femminile nella pratica odontoiatrica. Dent. Cadmos 2014, 82, 31–48. [Google Scholar] [CrossRef]
- Heggie, C.; McKernon, S.L.; Gartshore, L. Speaking up for balance: Analysis of the gender of invited speakers at UK dental conferences. Br. Dent. J. 2021, 1–8. [Google Scholar] [CrossRef]
- Hay, K.; McDougal, L.; Percival, V.; Henry, S.; Klugman, J.; Wurie, H.; Raven, J.; Shabalala, F.; Fielding-Miller, R.; Dey, A.; et al. Disrupting gender norms in health systems: Making the case for change. Lancet 2019, 393, 2535–2549. [Google Scholar] [CrossRef]
- ANDI Change Happens Because People Make it Happen—Le Donne in Odontoiatria. Available online: https://www.andi.it/change-happens-because-people-make-it-happen-le-donne-in-odontoiatria/ (accessed on 20 November 2022).
- ANDI È Online il Nuovo Corso FAD “Dentista Sentinella” Aggiornato e Gratuito per i Soci ANDI. Available online: https://www.andi.it/e-online-il-nuovo-corso-fad-dentisti-sentinelle-aggiornato-e-gratuito-per-i-soci-andi/ (accessed on 20 November 2022).
- FDI Aio International Congress. Available online: https://fdiworlddental.org/aio-international-congress (accessed on 20 November 2022).
- Release Press. Dentsply Sirona Reaffirms Commitment to Driving Cultural Change and Empowering Women in Dentistry on International Women’s Day. Available online: https://news.dentsplysirona.com/en/corporate-news/2022/dentsply-sirona-reaffirms-commitment-to-driving-cultural-change-.html (accessed on 20 November 2022).
- Piasecki, M.E.; Mutluay, M.; Kattadiyil, M.T.; Koka, S. Leadership diversity in prosthodontics: The number and percentage of women speakers at recent annual scientific meetings of prosthodontic organizations. J. Prosthet. Dent. 2020, 123, 461–465. [Google Scholar] [CrossRef]
- Gross, D.; Schäfer, G. “Feminization” in German dentistry. Career paths and opportunities—A gender comparison. Womens. Stud. Int. Forum 2011, 34, 130–139. [Google Scholar] [CrossRef]
- Hernández-Ruiz, R.; Benavides-Reyes, C.; González-López, S.; Bolaños-Carmona, M. A gender- based approach to the current situation of Spanish dentists. J. Clin. Exp. Dent. 2021, 13, e873–e885. [Google Scholar] [CrossRef]
- O’Brien, K.; Ahmad, M.; Harrhy, L.; Wong, J.; McCaul, L.; Sharma, N.; Stevens, C.; Baker, S.R. Balancing the dental boards. Br. Dent. J. 2021, 230, 804–806. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K. An update on the gender balance of the UK Dental Boards. BDJ Pract. 2022, 35, 30–31. [Google Scholar] [CrossRef]
- Worthington, C.C.; Mihas, P.; Bocklage, C.; Frazier-Bowers, S.A.; Lin, F.-C.; Ko, C.-C.; Jacox, L.A. Educational debt and the gender gap: Understanding factors influencing orthodontists’ career decisions. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e20–e61. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.N.; Andrews, E.A.; White, C.C.; Dixon, D.A.; López, A.N.; Stewart, D. Advancing women, parity, and gender equity. J. Dent. Educ. 2022, 86, 1182–1190. [Google Scholar] [CrossRef]
- Gangwani, P.; Kolokythas, A. Gender Gap in Leadership in Academic Medicine and Dentistry: What Are the Barriers? What Can Be Done To Correct It? J. Oral Maxillofac. Surg. 2019, 77, 1536–1540. [Google Scholar] [CrossRef] [PubMed]
- Cain, L.; Brady, M.; Inglehart, M.R.; Istrate, E.C. Faculty diversity, equity, and inclusion in academic dentistry: Revisiting the past and analyzing the present to create the future. J. Dent. Educ. 2022, 86, 1198–1209. [Google Scholar] [CrossRef] [PubMed]
- Fleming, E.; Neville, P.; Muirhead, V.E. Are there more women in the dentist workforce? Using an intersectionality lens to explore the feminization of the dentist workforce in the UK and US. Community Dent. Oral Epidemiol. 2022, 1–8. [Google Scholar] [CrossRef]
- Bompolaki, D.; Bs, S.V.P.; Koka, S. Gender diversity and senior leadership in academic dentistry: Female representation at the dean position in the United States. J. Dent. Educ. 2022, 86, 401–405. [Google Scholar] [CrossRef]
- Bates, C.; Gordon, L.; Travis, E.; Chatterjee, A.; Chaudron, L.; Fivush, B.; Gulati, M.; Jagsi, R.; Sharma, P.; Gillis, M.; et al. Striving for gender equity in academic medicine careers: A call to action. Acad. Med. 2016, 91, 1050–1052. [Google Scholar] [CrossRef]
- Pallavi, S.K.; Rajkumar, G.C. Professional practice among woman dentist. J. Int. Soc. Prev. Community Dent. 2011, 1, 14–19. [Google Scholar] [CrossRef]
- Masur, S.K. Invisible woman? Trends Cell Biol. 2015, 25, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Buell, D.; Hemmelgarn, B.R.; Straus, S.E. Proportion of women presenters at medical grand rounds at major academic centres in Canada: A retrospective observational study. BMJ Open 2018, 8, e019796. [Google Scholar] [CrossRef] [PubMed]
- Boiko, J.R.; Anderson, A.; Gordon, R. Representation of Women Among Academic Grand Rounds Speakers. JAMA Intern. Med. 2017, 177, 722–724. [Google Scholar] [CrossRef]
- Koletsi, D.; Papadopoulou, A.K. Gender disparity in speakers of the European Orthodontic Society conferences held between 2015 and 2020: A cross-sectional report. Eur. J. Orthod. 2022, 44, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Martorell, L.B.; Silva, A.L.M.; Leles, C.R.; Silva, B.S.D.F.; dos Santos, C.V.M.; Finkler, M. Gender differences among dentistry conference speakers in Brazil. Saúde Debate 2021, 45, 73–82. [Google Scholar] [CrossRef]
- Nkenke, E.; Seemann, R.; Vairaktaris, E.; Schaller, H.-G.; Rohde, M.; Stelzle, F.; Knipfer, C. Gender trends in authorship in oral and maxillofacial surgery literature: A 30-year analysis. J. Cranio-Maxillofacial Surg. 2015, 43, 913–917. [Google Scholar] [CrossRef]
- Franco, M.C.; Sartori, L.; Queiroz, A.B.; Neppelenbroek, K.H.; Wang, L.; Sousa-Neto, M.D.; Paiva, S.M.; Correa, M.B.; Cenci, M.S.; de Moraes, R.R.; et al. Impact of COVID-19 on gender gap in dental publications: A retrospective cohort with three Brazilian journals. Braz. Oral Res. 2022, 36. [Google Scholar] [CrossRef]
- Lalloo, R. “You can’t be what you can’t see”: Equity, diversity and inclusivity of editorial teams of dental journals. Br. Dent. J. 2022. [Google Scholar] [CrossRef]
- Directorate-General for Trade (European Commission), European Commission. COMMUNICATION FROM THE COMMISSION TO THE EUROPEAN PARLIAMENT, THE COUNCIL, THE EUROPEAN ECONOMIC AND SOCIAL COMMITTEE AND THE COMMITTEE OF THE REGIONS A Union of Equality: Gender Equality Strategy 2020–2025. EUR-Lex 2020, 4. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A52020DC0152 (accessed on 20 December 2022).
- Dipartimeto per le pari Opportunità. GU Serie Generale n.152 del 01-07-2022; 2022; p. 78. Available online: https://www.gazzettaufficiale.it/eli/gu/2022/07/01/152/sg/pdf (accessed on 20 December 2022).
- Senatori, C.; Garavini, C.; Sbrollini, N. Disegno di legge Istituzione di una Commissione Parlamentare per i Diritti Della Donna e l’uguaglianza di Genere; 2019; pp. 1–8. Available online: https://www.senato.it/service/PDF/PDFServer/DF/350908.pdf (accessed on 20 December 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Role in National Dental Boards | Male (n) | Female (n) | Role in Local Dental Boards | Male (n) | Female (n) |
|---|---|---|---|---|---|
| President | 1 | 0 | President | 100 | 6 |
| Vice President | 1 | 0 | Vice President | 97 | 9 |
| Secretary | 1 | 0 | Secretary | 90 | 16 |
| Counselors | 4 | 1 | Counselors | 160 | 52 |
| Role | Male (n) | Female (n) | Chi-Square Test | dF | p-Value |
|---|---|---|---|---|---|
| President | 101 | 6 | 84.346 | 1 | <0.05 |
| Vice President | 98 | 9 | 74.028 | 1 | <0.05 |
| Secretary | 91 | 16 | 52.570 | 1 | <0.05 |
| Counselors | 164 | 53 | 56.779 | 1 | <0.05 |
| Gender | Expected % | Observed % | 95% CI of Observed % | Binomial Test | |
|---|---|---|---|---|---|
| Female | 26.00 | 15.82 | 12.96 to 19.17 | p (one-tailed) | <0.0001 |
| Male | 74.00 | 84.18 | 80.83 to 87.04 | p (two-tailed) | <0.0001 |
| TOTAL | 100.0 | 100.00 | Is discrepancy significant (p < 0.05)? | Yes | |
| Role | Male (n) | Female (n) | ||||
|---|---|---|---|---|---|---|
| National | Regional | Provincial | National | Regional | Provincial | |
| President | 1 | 19 | 87 | 0 | 2 | 9 |
| Vice President | 4 | 32 | 84 | 0 | 8 | 12 |
| Secretary | 0 | 17 | 77 | 1 | 4 | 18 |
| Union Secretary | 1 | 21 | 66 | 0 | 0 | 30 |
| Cultural Secretary | 1 | 19 | 80 | 0 | 2 | 15 |
| Treasurer | 1 | 21 | 87 | 0 | 0 | 8 |
| Counselors | 0 | 0 | 404 | 0 | 0 | 109 |
| Role | Male (n) | Female (n) | Chi-Square Test | dF | p-Value |
|---|---|---|---|---|---|
| President | 107 | 11 | 78.102 | 1 | <0.05 |
| Vice President | 120 | 20 | 71.429 | 1 | <0.05 |
| Secretary | 94 | 23 | 43.085 | 1 | <0.05 |
| Treasurer | 109 | 8 | 87.188 | 1 | <0.05 |
| Union Secretary | 88 | 30 | 28.508 | 1 | <0.05 |
| Cultural Secretary | 100 | 17 | 58.880 | 1 | <0.05 |
| Counselors | 404 | 109 | 169.639 | 1 | <0.05 |
| Gender | Expected % | Observed % | 95% CI of Observed % | Binomial Test | |
|---|---|---|---|---|---|
| Female | 26.00 | 16.98 | 14.98 to 19.18 | p (one-tailed) | <0.0001 |
| Male | 74.00 | 83.02 | 80.82 to 85.02 | p (two-tailed) | <0.0001 |
| TOTAL | 100.0 | 100.00 | Is discrepancy significant (p < 0.05)? | Yes | |
| Disciplines | Male (n) | Female (n) | Chi-Square | DF | p-Value |
|---|---|---|---|---|---|
| 16 | 4613 | 815 | 2657.480 | 1 | <0.0001 |
| Type of Discipline | Male (n) | Female (n) | Chi-Square | DF | p-Value |
| Aesthetic Dentistry | 24 | 5 | 12.448 | 1 | <0.0004 |
| Digital Dentistry | 183 | 13 | 147.449 | 1 | <0.0001 |
| Endodontics | 315 | 48 | 196.388 | 1 | <0.0001 |
| Forensic Dentistry | 126 | 20 | 76.96 | 1 | <0.0001 |
| Gnathology | 279 | 60 | 141.5 | 1 | <0.0001 |
| Implantology | 627 | 34 | 532.0 | 1 | <0.0001 |
| Multidisciplinary | 229 | 51 | 113.2 | 1 | <0.0001 |
| Oral Medicine | 218 | 53 | 100.5 | 1 | <0.0001 |
| Oral Pathology | 158 | 39 | 71.88 | 1 | <0.0001 |
| Oral Surgery | 483 | 34 | 389.9 | 1 | <0.0001 |
| Orthodontics | 584 | 181 | 212.3 | 1 | <0.0001 |
| Pediatric Dentistry | 97 | 79 | 1.841 | 1 | N.S. |
| Periodontology | 341 | 99 | 133.1 | 1 | <0.0001 |
| Prosthetic | 365 | 21 | 306.6 | 1 | <0.0001 |
| Radiology | 63 | 5 | 49.47 | 1 | <0.0001 |
| Restorative Dentistry | 488 | 45 | 368.2 | 1 | <0.0001 |
| Special Dentistry | 33 | 28 | 0.4098 | 1 | N.S. |
| Two-Way ANOVA for Northern Region of Italy | ||||
|---|---|---|---|---|
| Source of variation | % of total variation | p-value | p-value summary | 95% CI of difference |
| Specialties | 31.06 | 0.3958 | N.S. | 52.90 to 131.8 |
| Gender | 41.79 | 0.0001 | *** | |
| Two-Way ANOVA for Central Region of Italy | ||||
| Source of variation | % of total variation | p-value | p-value summary | 95% CI of difference |
| Specialties | 54.56 | 0.0546 | N.S. | 26.47 to 86.12 |
| Gender | 22.73 | 0.001 | ** | |
| Two-Way ANOVA for Southern Region of Italy | ||||
| Source of variation | % of total variation | p-value | p-value summary | 95% CI of difference |
| Specialties | 32.53 | 0.3112 | N.S. | 44.05 to 105.5 |
| Gender | 42.14 | <0.0001 | **** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardi, S.; Fulgenzi, M.B.; Rovera, A.; Rinaldi, F.; Trichilo, S.; Bianchi, S. Dentistry and Gender Gap: An Overview of the Italian Situation. Healthcare 2023, 11, 828. https://doi.org/10.3390/healthcare11060828
Bernardi S, Fulgenzi MB, Rovera A, Rinaldi F, Trichilo S, Bianchi S. Dentistry and Gender Gap: An Overview of the Italian Situation. Healthcare. 2023; 11(6):828. https://doi.org/10.3390/healthcare11060828
Chicago/Turabian StyleBernardi, Sara, Maria Bruna Fulgenzi, Angela Rovera, Fabiola Rinaldi, Sara Trichilo, and Serena Bianchi. 2023. "Dentistry and Gender Gap: An Overview of the Italian Situation" Healthcare 11, no. 6: 828. https://doi.org/10.3390/healthcare11060828
APA StyleBernardi, S., Fulgenzi, M. B., Rovera, A., Rinaldi, F., Trichilo, S., & Bianchi, S. (2023). Dentistry and Gender Gap: An Overview of the Italian Situation. Healthcare, 11(6), 828. https://doi.org/10.3390/healthcare11060828