
Instrument-Assisted Soft Tissue Mobilization Technique versus Static Stretching in Patients with Pronated Dominant Foot: A Comparison in Effectiveness on Flexibility, Foot Posture, Foot Function Index, and Dynamic Balance

 , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
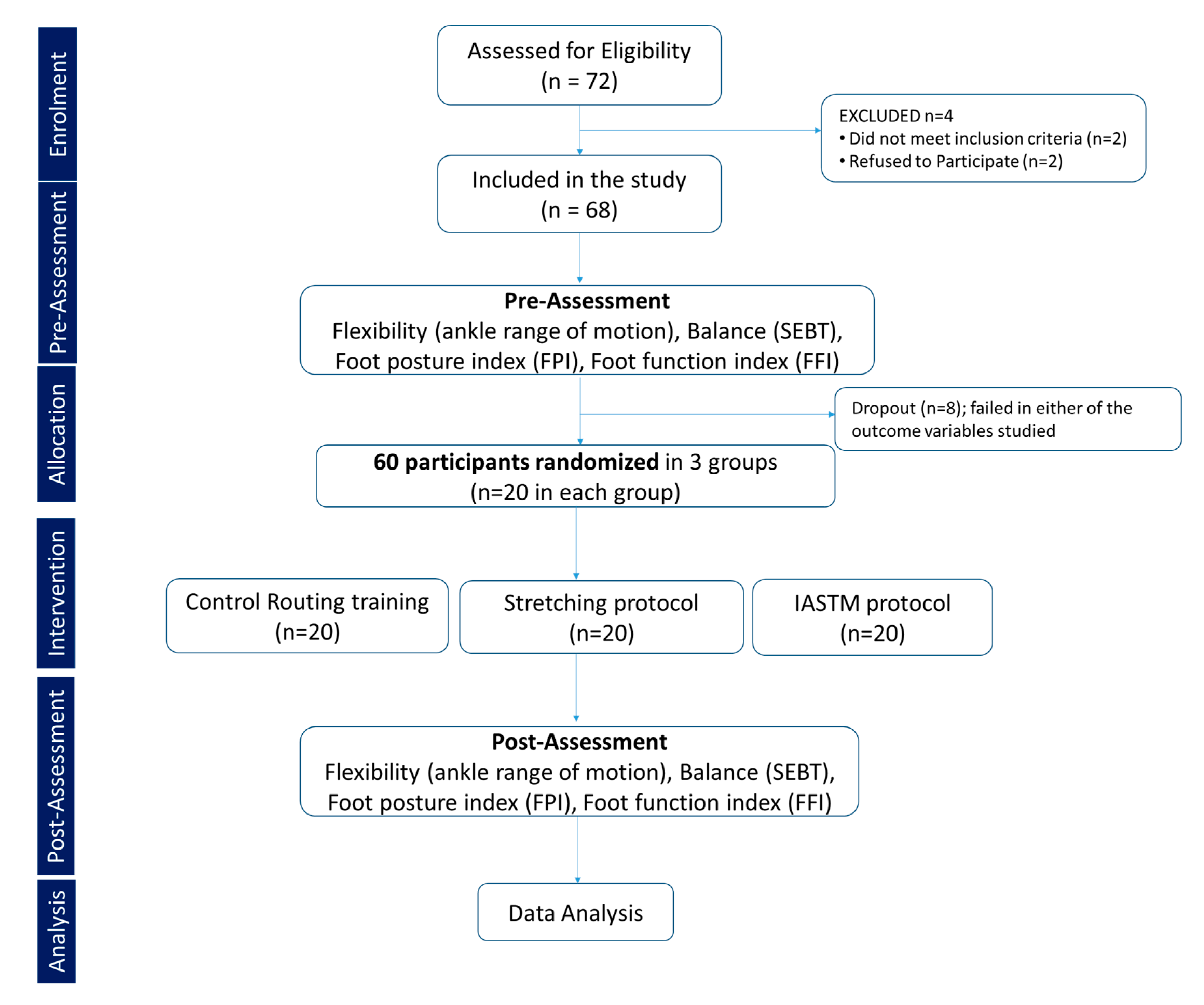
2.1. Sample Design: Pre and Posttest Experimental Comparative Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Assessment Tools
2.4.1. Morphologic Foot Assessment
2.4.2. Foot Function Index
2.4.3. Balance Assessment
2.4.4. Range of Motion (ROM)
2.5. The Interventions
IASTM Training
2.6. Stretching Exercise
2.7. Control Group
2.8. Statistical Analysis
3. Results
3.1. Subsection
3.1.1. Demographics
3.1.2. Ankle Joint Range of Motion
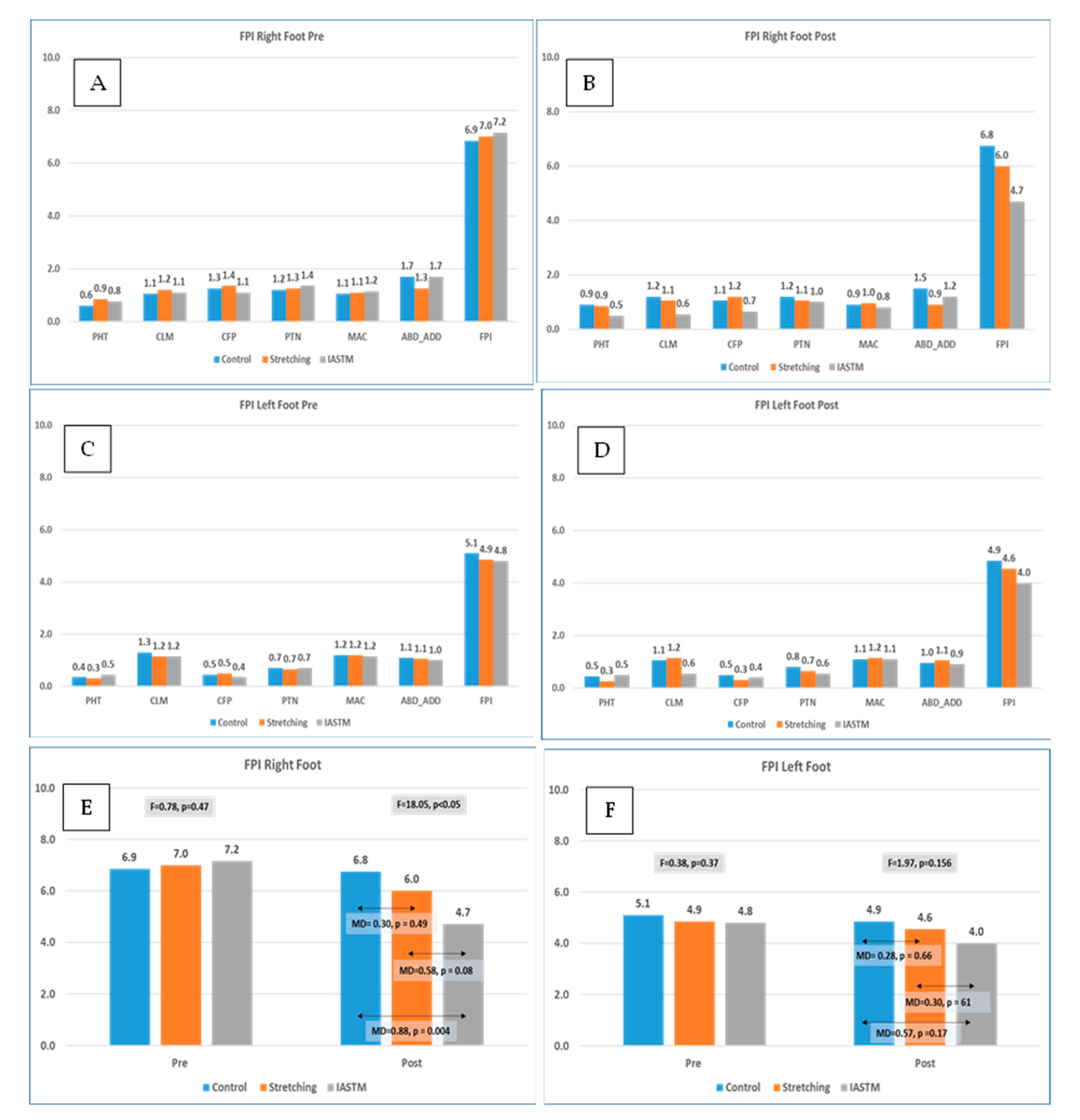
3.1.3. Foot Posture Index (FPI)
3.2. Figures, Tables, and Schemes
3.2.1. Foot Function Index (FFI) and Its Components
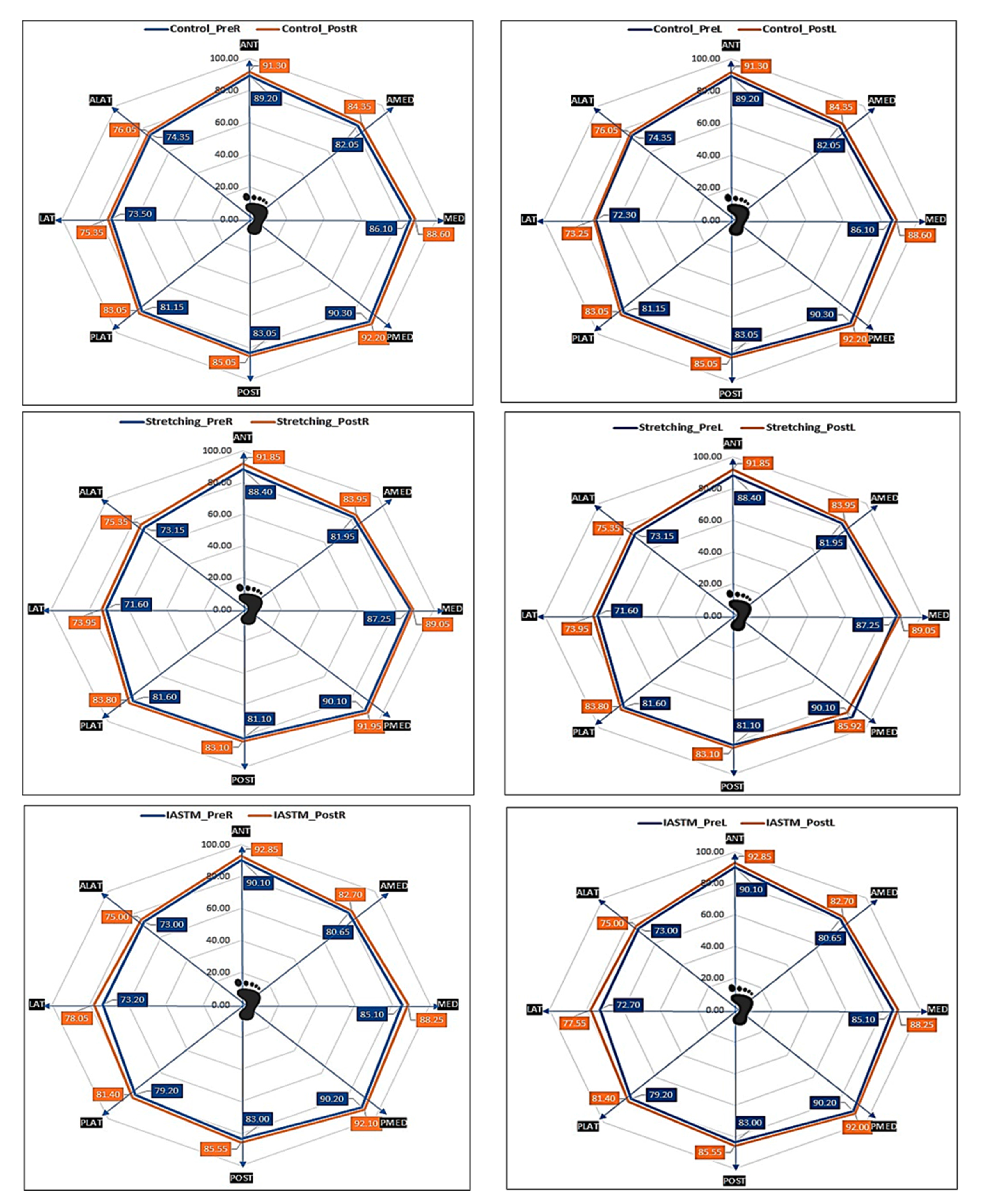
3.2.2. Dynamic Balance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haendlmayer, K.T.; Harris, N.J. (ii) Flatfoot deformity: An overview. Orthop. Trauma 2009, 23, 395–403. [Google Scholar] [CrossRef]
- Hollander, K.; Zech, A.; Rahlf, A.L.; Orendurff, M.S.; Stebbins, J.; Heidt, C. The relationship between static and dynamic foot posture and running biomechanics: A systematic review and meta-analysis. Gait Posture 2019, 72, 109–122. [Google Scholar] [CrossRef]
- Williams, D.S., III; McClay, I.S.; Hamill, J. Arch structure and injury patterns in runners. Clin. Biomech. 2001, 16, 341–347. [Google Scholar] [CrossRef]
- Ibeabuchi, M.; Obun, C.; Olabiyi, O.; Oluwabusola, E.; Adebayo, A. Prevalence of flat foot among 6-15-year-old Nigerian school children resident in Lagos. J. Anatom. Sci. 2020, 11, 153–158. [Google Scholar]
- Cheatham, S.W.; Baker, R.; Kreiswirth, E. Instrument Assisted Soft-Tissue Mobilization: A Commentary on Clinical Practice Guidelines for Rehabilitation Professionals. Int. J. Sports Phys. Ther. 2019, 14, 670–682. [Google Scholar] [CrossRef]
- Chawla, J.S.; Singh, M.; Ummat, A.; Goyal, M.; Kaur, H.; Verma, V. Effectiveness of Calf Stretching Exercises Versus Plantar Fascia Stretching Exercises in Plantar Fasciitis: An Experimental Study. Indian J. Public Health Res. Dev. 2020, 11, 890–895. [Google Scholar] [CrossRef]
- Sulowska-Daszyk, I.; Skiba, A. The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners. Int. J. Environ. Res. Public Health 2022, 19, 457. [Google Scholar] [CrossRef]
- Murley, G.; Menz, H.; Landorf, K.B. A protocol for classifying normal-and flat-arched foot posture for research studies using clinical and radiographic measurements. J. Foot Ankle Res. 2009, 2, 22. [Google Scholar] [CrossRef]
- Alahmari, K.A.; Kakaraparthi, V.N.; Reddy, R.S.; Samuel, P.S.; Tedla, J.S.; Rengaramanujam, K.; Ahmad, I.; Sangadala, D.R.; Mukherjee, D. Foot Posture Index Reference Values among Young Adults in Saudi Arabia and Their Association with Anthropometric Determinants, Balance, Functional Mobility, and Hypermobility. BioMed Res. Int. 2021, 2021, 8844356. [Google Scholar] [CrossRef]
- Ali, M.M.I.; Mohamed, M.S.E. Dynamic postural balance in subjects with and without flat foot. Bull. Fac. Phys. Ther. 2011, 16, 7–11. [Google Scholar]
- Rutkowski, R.; Gizińska, M.; Gałczyńska-Rusin, M.; Kasprzak, M.P.; Budiman-Mak, E. The Importance of Foot Function Assessment Using the Foot Function Index-Revised Short Form (FFI-RS) Questionnaire in the Comprehensive Treatment of Patients with Rheumatoid Arthritis. J. Clin. Med. 2022, 11, 2298. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D. Effects of Visual Feedback Short Foot Exercise on Foot Pressure in Adults with Flexible Flat Foot. J. Int. Acad. Phys. Ther. Res. 2019, 10, 1934–1939. [Google Scholar] [CrossRef]
- Ullah, H. Correlation of flexible flatfoot and q-angle among secondary school students by using dennis method. Pak. J. Rehabil. 2019, 8, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Redmond, A.C.; Crosbie, J.; Ouvrier, R.A. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index. Clin. Biomech. 2006, 21, 89–98. [Google Scholar] [CrossRef]
- Budiman-Mak, E.; Conrad, K.J.; Mazza, J.; Stuck, R.M. A review of the foot function index and the foot function index—Revised. J. Foot Ankle Res. 2013, 6, 5–37. [Google Scholar] [CrossRef]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the Star Excursion Balance Test to Assess Dynamic Postural-Control Deficits and Outcomes in Lower Extremity Injury: A Literature and Systematic Review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef]
- Lin, C.-H.; Chiang, S.-L.; Lu, L.-H.; Wei, S.-H.; Sung, W.-H. Validity of an ankle joint motion and position sense measurement system and its application in healthy subjects and patients with ankle sprain. Comput. Methods Programs Biomed. 2016, 131, 89–966. [Google Scholar] [CrossRef]
- Kim, J.; Sung, D.J.; Lee, J. Therapeutic effectiveness of instrument-assisted soft tissue mobilization for soft tissue injury: Mechanisms and practical application. J. Exerc. Rehabil. 2017, 13, 12–22. [Google Scholar] [CrossRef]
- Park, J.-H.; Rhyu, H.-S.; Rhi, S.-Y. The effects of instrument-assisted soft tissue mobilization rehabilitation exercise on range of motion, isokinetic strength, and balance in chronic ankle instability taekwondo players. J. Exerc. Rehabil. 2020, 16, 516–521. [Google Scholar] [CrossRef]
- Kato, E.; Kanehisa, H.; Fukunaga, T.; Kawakami, Y. Changes in ankle joint stiffness due to stretching: The role of tendon elongation of the gastrocnemius muscle. Eur. J. Sport Sci. 2010, 10, 111–119. [Google Scholar] [CrossRef]
- Fullam, K.; Caulfield, B.; Coughlan, G.F.; Delahunt, E. Kinematic Analysis of Selected Reach Directions of the Star Excursion Balance Test Compared with the Y-Balance Test. J. Sport Rehabil. 2014, 23, 27–35. [Google Scholar] [CrossRef]
- Rowlett, C.A.; Hanney, W.J.; Pabian, P.S.; McArthur, J.H.; Rothschild, C.E.; Kolber, M.J. Efficacy of instrument-assisted soft tissue mobilization in comparison to gastrocnemius-soleus stretching for dorsiflexion range of motion: A randomized controlled trial. J. Bodyw. Mov. Ther. 2019, 23, 233–240. [Google Scholar] [CrossRef]
- Cho, S.-H.; Kim, C.-H.; Lee, J.-H. Immediate Effect of Instrument Assisted Soft Tissue Mobilization and Self-Stretching on Gastrocnemius Muscle Thickness and the Range of Motion. JIAPTR 2021, 12, 2419–2425. [Google Scholar] [CrossRef]
- Radford, J.A.; Landorf, K.B.; Buchbinder, R.; Cook, C. Effectiveness of calf muscle stretching for the short-term treatment of plantar heel pain: A randomised trial. BMC Musculoskelet Disord. 2007, 8, 36. [Google Scholar] [CrossRef]
- Youdas, J.W.; Krause, D.A.; Egan, K.S.; Therneau, T.M.; Laskowski, E.R. The Effect of Static Stretching of the Calf Muscle-Tendon Unit on Active Ankle Dorsiflexion Range of Motion. J. Orthop. Sports Phys. Ther. 2003, 33, 408–417. [Google Scholar] [CrossRef]
- Macklin, K.; Healy, A.; Chockalingam, N. The effect of calf muscle stretching exercises on ankle joint dorsiflexion and dynamic foot pressures, force and related temporal parameters. Foot 2012, 22, 10–17. [Google Scholar] [CrossRef]
- Sivachandiran, S.; Kumar, G. Effect of corrective exercises programme among athletes with flat feet on foot alignment factors. Int. J. Phys. Educ. Sports Health 2016, 3, 193–196. [Google Scholar]
- Hirata, K.; Yamadera, R.; Akagi, R. Can static stretching reduce stiffness of the triceps surae in older men? Med. Sci. Sports Exerc. 2020, 52, 673. [Google Scholar] [CrossRef]
- Chiquet, M.; Tunc-Civelek, V.; Sarasa-Renedo, A. Gene regulation by mechanotransduction in fibroblasts. Appl. Physiol. Nutr. Metab. 2007, 32, 967–973. [Google Scholar] [CrossRef]
- Lambert M, Hitchcock R, Lavallee K; et al. The effects of instrument-assisted soft tissue mobilization compared to other interventions on pain and function: A systematic review. Phys Ther Review. 2017, 22, 76–85. [Google Scholar] [CrossRef]
- Cote, K.P.; Brunet, M.E.; Gansneder, B.M.; Shultz, S.J. Effects of Pronated and Supinated Foot Postures on Static and Dynamic Postural Stability. J. Athl. Train. 2005, 40, 41–46. [Google Scholar] [PubMed]
- Kim, J.A.; Lim, O.B.; Yi, C.H. Difference in static and dynamic stability between flexible flatfeet and neutral feet. Gait Posture 2015, 41, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Beak, H.J.; Yoon, E.-J.; Kim, J. Effect of Instrument-Assisted Soft Tissue Mobilization on Ankle of Range of Motion and Balance in Older Women: A Preliminary Study. Asian J. Kinesiol. 2021, 23, 2–8. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| FFI | Group | Pre | Post | Time Effect | Group Effect | Time x Group | Control vs. Stretching | Control vs. IASTM | IASTM vs. Stretching |
|---|---|---|---|---|---|---|---|---|---|
| Pain | Control | 37.95 ± 5.4 | 36.50 ± 4.1 | pη2 = 0.86, p < 0.001 | pη2 = 0.43, p < 0.001 | pη2 = 0.81, p < 0.001 | MD = 1.02, p = 0.69 | MD = 7.45, p < 0.001 | MD = 6.43, p < 0.001 |
| Stretching | 38.90 ± 4.5 | 33.50 ± 3.4 | |||||||
| IASTM | 38.05 ± 4.9 | 21.50 ± 1.9 | |||||||
| F value | 0.22 | 116.03 | |||||||
| p-value | 0.80 | p < 0.001 | |||||||
| Disability | Control | 45.8 ± 4.35 | 43.6 ± 3.4 | pη2 = 0.87, p < 0.001 | pη2 = 0.27, p < 0.001 | pη2 = 0.76, p < 0.001 | MD = −0.33, p = 0.95 | MD = 4.00, p = 0.001 | MD = 4.33, p < 0.001 |
| Stretching | 48.4 ± 3.79 | 41.8 ± 3.9 | |||||||
| IASTM | 48.5 ± 3.75 | 33 ± 2.62 | |||||||
| F value | 2.86 | 56.22 | |||||||
| p-value | 0.07 | p < 0.001 | |||||||
| Activity Limitations | Control | 27.90 ± 2 | 22.80 ± 2.4 | pη2 = 0.90, p < 0.001 | pη2 = 0.39, p < 0.001 | pη2 = 0.56, p < 0.001 | MD = 2.75, p < 0.001 | MD = 2.18, p < 0.001 | MD = −0.57, p = 0.45 |
| Stretching | 28.90 ± 2.2 | 16.25 ± 1.7 | |||||||
| IASTM | 27.00 ± 2 | 19.35 ± 2.2 | |||||||
| F value | 4.51 | 47.53 | |||||||
| p-value | 0.06 | p < 0.001 | |||||||
| Foot Function Index | Control | 48.5 ± 3.4 | 44.8 ± 2.4 | pη2 = 0.95 p < 0.001 | pη2 = 0.55 p < 0.001 | pη2 = 0.85 p < 0.001 | MD = 1.50 p = 0.12 | MD = 5.9 p < 0.001 | MD = 4.4 p < 0.001 |
| Stretching | 50.5 ± 2.9 | 39.8 ± 2.21 | |||||||
| IASTM | 49.3 ± 2.8 | 32.1 ± 1.6 | |||||||
| F value | 2.13 | 181.95 | |||||||
| p-value | 0.13 | p < 0.001 |
| Reach Direction | Pre vs. Post | Right-Leg Stance | ||||||
|---|---|---|---|---|---|---|---|---|
| Control | Stretching | IASTM | Mean Square | F | Sig. | η2 | ||
| ANT | Pre | 89.2 ± 3.89 | 88.5 ± 4.8 | 88.55 ± 3.85 | 3.05 | 0.173 | 0.84 | 0.01 |
| Post | 91.3 ± 3.42 | 91.85 ± 4.11 | 94.65 ± 2.28 | 64.55 | 5.737 | 0.01 * | 0.17 | |
| AMED | Pre | 80.1 ± 4.9 | 80.9 ± 3.48 | 80.65 ± 2.3 | 3.35 | 0.243 | 0.79 | 0.01 |
| Post | 82.55 ± 3.72 | 82.95 ± 3.66 | 85.55 ± 2.93 | 53.067 | 4.443 | 0.02 * | 0.14 | |
| Medial | Pre | 86.1 ± 6.32 | 87.25 ± 3.74 | 85.1 ± 2.15 | 23.15 | 1.185 | 0.31 | 0.04 |
| Post | 88.6 ± 6.13 | 89.05 ± 3.65 | 88.25 ± 2.38 | 3.217 | 0.171 | 0.84 | 0.01 | |
| PMED | Pre | 90.3 ± 3.4 | 90.1 ± 4.3 | 90.2 ± 4.11 | 0.2 | 0.013 | 0.99 | 0.00 |
| Post | 92.1 ± 3.92 | 91.95 ± 4.02 | 92.2 ± 2.95 | 0.32 | 0.024 | 0.98 | 0.00 | |
| POST | Pre | 83.05 ± 4.02 | 81.1 ± 3.18 | 83 ± 3.52 | 24.717 | 1.917 | 0.16 | 0.03 |
| Post | 85.05 ± 3.36 | 83.1 ± 3.26 | 87 ± 2.99 | 76.05 | 7.388 | 0.01 * | 0.21 | |
| PLAT | Pre | 81.15 ± 4.3 | 81.6 ± 3.86 | 79.2 ± 4.14 | 32.55 | 1.936 | 0.15 | 0.06 |
| Post | 83.05 ± 15.57 | 83.8 ± 3.82 | 81.4 ± 4.26 | 30.15 | 0.329 | 0.72 | 0.01 | |
| LAT | Pre | 73.5 ± 4.05 | 71.6 ± 5.40 | 73.2 ± 5.02 | 20.87 | 0.88 | 0.42 | 0.03 |
| Post | 75.35 ± 4.08 | 73.95 ± 5.84 | 78.05 ± 4.29 | 86.87 | 3.77 | 0.03 * | 0.12 | |
| ALAT | Pre | 74.35 ± 4.06 | 73.15 ± 3.66 | 73 ± 3.34 | 10.95 | 0.801 | 0.45 | 0.03 |
| Post | 76.05 ± 3.88 | 75.35 ± 3.44 | 75 ± 3.21 | 5.573 | 0.451 | 0.64 | 0.02 | |
| Reach Direction | Pre vs. Post | Left-Leg Stance | ||||||
|---|---|---|---|---|---|---|---|---|
| Control | Stretching | IASTM | Mean Square | F | Sig. | η2 | ||
| ANT | Pre | 89.20 ± 2.57 | 88.4 ± 5.54 | 90.1 ± 4.31 | 14.47 | 0.778 | 0.464 | 0.03 |
| Post | 91.3 ± 3.42 | 91.85 ± 4.11 | 92.85 ± 3.66 | 12.35 | 0.883 | 0.419 | 0.03 | |
| AMED | Pre | 82.05 ± 5.04 | 81.95 ± 3.57 | 80.65 ± 2.3 | 12.2 | 0.846 | 0.435 | 0.03 |
| Post | 84.35 ± 4.23 | 83.95 ± 3.67 | 82.7 ± 2.82 | 14.817 | 1.136 | 0.328 | 0.04 | |
| Medial | Pre | 86.1 ± 6.33 | 87.25 ± 3.74 | 85.1 ± 2.15 | 23.15 | 1.185 | 0.313 | 0.04 |
| Post | 88.6 ± 6.13 | 89.05 ± 3.65 | 88.25 ± 2.39 | 3.217 | 0.171 | 0.843 | 0.01 | |
| PMED | Pre | 90.3 ± 3.41 | 90.1 ± 4.31 | 90.2 ± 4.12 | 0.2 | 0.013 | 0.987 | 0.00 |
| Post | 92.2 ± 2.95 | 85.92 ± 12.7 | 92 ± 3.94 | 255.228 | 4.131 | 0.021 * | 0.13 | |
| POST | Pre | 83.05 ± 4.02 | 81.1 ± 3.18 | 83 ± 3.53 | 24.717 | 1.917 | 0.156 | 0.06 |
| Post | 85.05 ± 3.37 | 83.1 ± 3.26 | 85.55 ± 3.86 | 33.517 | 2.73 | 0.074 | 0.09 | |
| PLAT | Pre | 81.15 ± 4.3 | 81.6 ± 3.86 | 79.2 ± 4.14 | 32.55 | 1.936 | 0.154 | 0.06 |
| Post | 83.05 ± 15.57 | 83.8 ± 3.82 | 81.4 ± 4.26 | 30.15 | 0.329 | 0.721 | 0.01 | |
| LAT | Pre | 72.3 ± 3.6 | 71.6 ± 5.41 | 72.7 ± 4.39 | 6.2 | 0.303 | 0.74 | 0.01 |
| Post | 73.25 ± 4.36 | 73.95 ± 5.84 | 77.55 ± 5.22 | 106.467 | 3.983 | 0.024 * | 0.12 | |
| ALAT | Pre | 74.35 ± 4.06 | 73.15 ± 3.66 | 73 ± 3.34 | 10.95 | 0.801 | 0.454 | 0.03 |
| Post | 76.15 ± 3.81 | 75.35 ± 3.44 | 75 ± 3.22 | 6.95 | 0.57 | 0.57 | 0.02 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, U.; Sharma, A.; Rizvi, M.R.; Alqahtani, M.M.; Ahmad, F.; Kashoo, F.Z.; Miraj, M.; Asad, M.R.; Uddin, S.; Ahamed, W.M.; et al. Instrument-Assisted Soft Tissue Mobilization Technique versus Static Stretching in Patients with Pronated Dominant Foot: A Comparison in Effectiveness on Flexibility, Foot Posture, Foot Function Index, and Dynamic Balance. Healthcare 2023, 11, 785. https://doi.org/10.3390/healthcare11060785
Gupta U, Sharma A, Rizvi MR, Alqahtani MM, Ahmad F, Kashoo FZ, Miraj M, Asad MR, Uddin S, Ahamed WM, et al. Instrument-Assisted Soft Tissue Mobilization Technique versus Static Stretching in Patients with Pronated Dominant Foot: A Comparison in Effectiveness on Flexibility, Foot Posture, Foot Function Index, and Dynamic Balance. Healthcare. 2023; 11(6):785. https://doi.org/10.3390/healthcare11060785
Chicago/Turabian StyleGupta, Ujjwal, Ankita Sharma, Moattar R. Rizvi, Mazen M. Alqahtani, Fuzail Ahmad, Faizan Z. Kashoo, Mohammad Miraj, Mohammad R. Asad, Shadab Uddin, Waseem M. Ahamed, and et al. 2023. "Instrument-Assisted Soft Tissue Mobilization Technique versus Static Stretching in Patients with Pronated Dominant Foot: A Comparison in Effectiveness on Flexibility, Foot Posture, Foot Function Index, and Dynamic Balance" Healthcare 11, no. 6: 785. https://doi.org/10.3390/healthcare11060785
APA StyleGupta, U., Sharma, A., Rizvi, M. R., Alqahtani, M. M., Ahmad, F., Kashoo, F. Z., Miraj, M., Asad, M. R., Uddin, S., Ahamed, W. M., Nanjan, S., Hussain, S. A., & Ahmad, I. (2023). Instrument-Assisted Soft Tissue Mobilization Technique versus Static Stretching in Patients with Pronated Dominant Foot: A Comparison in Effectiveness on Flexibility, Foot Posture, Foot Function Index, and Dynamic Balance. Healthcare, 11(6), 785. https://doi.org/10.3390/healthcare11060785