
Low-Intensity Blood Flow Restriction Exercises Modulate Pain Sensitivity in Healthy Adults: A Systematic Review

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
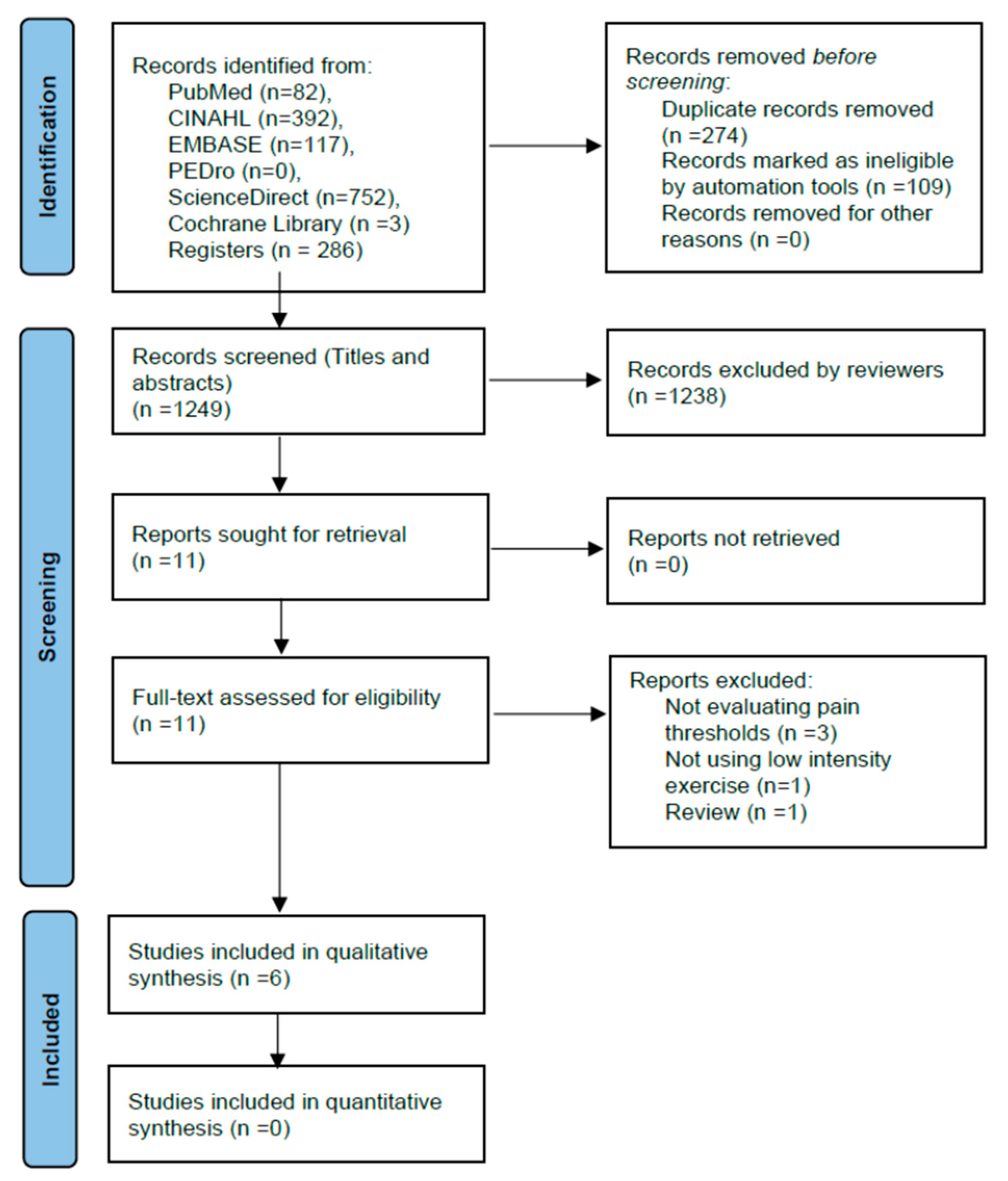
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Participants
2.2.2. Intervention
2.2.3. Comparison Groups
2.2.4. Outcome
2.2.5. Study Design
2.3. Study Selection and Data Extraction
2.4. Methodological Quality
2.5. Data Analysis, Summary and Synthesis of Findings
3. Results
3.1. Participants
3.2. Interventions
3.3. Outcome Measures
3.4. Methodological Quality
3.5. Effects on Pain Perception
4. Discussion
Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rice, D.; Nijs, J.; Kosek, E.; Wideman, T.; Hasenbring, M.I.; Koltyn, K.; Graven-Nielsen, T.; Polli, A. Exercise-Induced Hypoalgesia in Pain-Free and Chronic Pain Populations: State of the Art and Future Directions. J. Pain 2019, 20, 1249–1266. [Google Scholar] [CrossRef] [PubMed]
- Vaegter, H.B.; Jones, M.D. Exercise-induced hypoalgesia after acute and regular exercise: Experimental and clinical manifestations and possible mechanisms in individuals with and without pain. Pain Rep. 2020, 5, e823. [Google Scholar] [CrossRef] [PubMed]
- Hoeger Bement, M.K.; Dicapo, J.; Rasiarmos, R.; Hunter, S.K. Dose response of isometric contractions on pain perception in healthy adults. Med. Sci. Sport. Exerc. 2008, 40, 1880–1889. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D.; Shepanski, M.A.; Ruble, S.B.; Valic, Z.; Buckwalter, J.B.; Clifford, P.S. Intensity and duration threshold for aerobic exercise-induced analgesia to pressure pain. Arch. Phys. Med. Rehabil. 2004, 85, 1183–1187. [Google Scholar] [CrossRef]
- Hviid, J.T.; Thorlund, J.B.; Vaegter, H.B. Walking increases pain tolerance in humans: An experimental cross-over study. Scand. J. Pain 2019, 19, 813–822. [Google Scholar] [CrossRef]
- Vaegter, H.B.; Handberg, G.; Graven-Nielsen, T. Hypoalgesia After Exercise and the Cold Pressor Test is Reduced in Chronic Musculoskeletal Pain Patients With High Pain Sensitivity. Clin. J. Pain 2016, 32, 58–69. [Google Scholar] [CrossRef]
- Naugle, K.M.; Fillingim, R.B.; Riley, J.L., 3rd. A meta-analytic review of the hypoalgesic effects of exercise. J. Pain 2012, 13, 1139–1150. [Google Scholar] [CrossRef]
- Early, K.S.; Rockhill, M.; Bryan, A.; Tyo, B.; Buuck, D.; McGinty, J. Effect of blood flow restriction training on muscular performance, pain and vascular function. Int. J. Sport. Phys. Ther. 2020, 15, 892–900. [Google Scholar] [CrossRef]
- Takarada, Y.; Takazawa, H.; Sato, Y.; Takebayashi, S.; Tanaka, Y.; Ishii, N. Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans. J. Appl. Physiol. (1985) 2000, 88, 2097–2106. [Google Scholar] [CrossRef]
- Cook, S.B.; Clark, B.C.; Ploutz-Snyder, L.L. Effects of exercise load and blood-flow restriction on skeletal muscle function. Med. Sci. Sport. Exerc. 2007, 39, 1708–1713. [Google Scholar] [CrossRef]
- Cook, C.J.; Kilduff, L.P.; Beaven, C.M. Improving strength and power in trained athletes with 3 weeks of occlusion training. Int. J. Sport. Physiol Perform. 2014, 9, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Abe, T.; Nielsen, J.L.; Libardi, C.A.; Laurentino, G.; et al. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 533. [Google Scholar] [CrossRef] [PubMed]
- Stray-Gundersen, S.; Wooten, S.; Tanaka, H. Walking With Leg Blood Flow Restriction: Wide-Rigid Cuffs vs. Narrow-Elastic Bands. Front. Physiol. 2020, 11, 568. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Abe, T.; Wilson, J.M.; Ugrinowitsch, C.; Bemben, M.G. Blood flow restriction: How does it work? Front. Physiol. 2012, 3, 392. [Google Scholar] [CrossRef]
- Karanasios, S.; Koutri, C.; Moutzouri, M.; Xergia, S.A.; Sakellari, V.; Gioftsos, G. The Effect of Body Position and the Reliability of Upper Limb Arterial Occlusion Pressure Using a Handheld Doppler Ultrasound for Blood Flow Restriction Training. Sport. Health 2022, 14, 717–724. [Google Scholar] [CrossRef]
- Giles, L.; Webster, K.E.; McClelland, J.; Cook, J.L. Quadriceps strengthening with and without blood flow restriction in the treatment of patellofemoral pain: A double-blind randomised trial. Br. J. Sport. Med. 2017, 51, 1688–1694. [Google Scholar] [CrossRef]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sport. Med. 2019, 49, 1787–1805. [Google Scholar] [CrossRef]
- Korakakis, V.; Whiteley, R.; Giakas, G. Low load resistance training with blood flow restriction decreases anterior knee pain more than resistance training alone. A pilot randomised controlled trial. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sport. Med. 2018, 34, 121–128. [Google Scholar] [CrossRef]
- Ferraz, R.B.; Gualano, B.; Rodrigues, R.; Kurimori, C.O.; Fuller, R.; Lima, F.R.; De SÁ-Pinto, A.N.A.L.; Roschel, H. Benefits of Resistance Training with Blood Flow Restriction in Knee Osteoarthritis. Med. Sci. Sport. Exerc. 2018, 50, 897–905. [Google Scholar] [CrossRef]
- Charles, D.; White, R.; Reyes, C.; Palmer, D. A systematic review of the effects of blood flow restriction training on quadriceps muscle atrophy and circumference post acl reconstruction. Int. J. Sport. Phys. Ther. 2020, 15, 882–891. [Google Scholar] [CrossRef]
- Cuyul-Vásquez, I.; Leiva-Sepúlveda, A.; Catalán-Medalla, O.; Araya-Quintanilla, F.; Gutiérrez-Espinoza, H. The addition of blood flow restriction to resistance exercise in individuals with knee pain: A systematic review and meta-analysis. Braz. J. Phys. Ther. 2020, 24, 465–478. [Google Scholar] [CrossRef]
- Ferlito, J.V.; Pecce, S.A.P.; Oselame, L.; De Marchi, T. The blood flow restriction training effect in knee osteoarthritis people: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1378–1390. [Google Scholar] [CrossRef] [PubMed]
- Karanasios, S.; Korakakis, V.; Moutzouri, M.; Xergia, S.A.; Tsepis, Ε.; Gioftsos, G. Low-load resistance training with blood flow restriction is effective for managing lateral elbow tendinopathy: A randomized, sham-controlled trial. J. Orthop. Sport. Phys. Ther. 2022, 12, 803–825. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sport. Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Paton, B.; Haddad, F.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Comparison of the acute perceptual and blood pressure response to heavy load and light load blood flow restriction resistance exercise in anterior cruciate ligament reconstruction patients and non-injured populations. Phys. Ther. Sport 2018, 33, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Patterson, S.D. Low intensity blood flow restriction exercise: Rationale for a hypoalgesia effect. Med. Hypotheses 2019, 132, 109370. [Google Scholar] [CrossRef]
- Song, J.S.; Spitz, R.W.; Yamada, Y.; Bell, Z.W.; Wong, V.; Abe, T.; Loenneke, J.P. Exercise-induced hypoalgesia and pain reduction following blood flow restriction: A brief review. Phys. Ther. Sport 2021, 50, 89–96. [Google Scholar] [CrossRef]
- Hughes, L.; Grant, I.; Patterson, S.D. Aerobic exercise with blood flow restriction causes local and systemic hypoalgesia and increases circulating opioid and endocannabinoid levels. J. Appl. Physiol. 2021, 131, 1460–1468. [Google Scholar] [CrossRef]
- Hughes, L.; Patterson, S.D. The effect of blood flow restriction exercise on exercise-induced hypoalgesia and endogenous opioid and endocannabinoid mechanisms of pain modulation. J. Appl. Physiol. 2020, 128, 914–924. [Google Scholar] [CrossRef]
- Song, J.S.; Kataoka, R.; Yamada, Y.; Wong, V.; Spitz, R.W.; Bell, Z.W.; Loenneke, J.P. The Hypoalgesic Effect of Low-Load Exercise to Failure Is Not Augmented by Blood Flow Restriction. Res. Q. Exerc. Sport 2022, 1, 1–10. [Google Scholar] [CrossRef]
- Song, J.S.; Yamada, Y.; Wong, V.; Bell, Z.W.; Spitz, R.W.; Abe, T.; Loenneke, J.P. Hypoalgesia following isometric handgrip exercise with and without blood flow restriction is not mediated by discomfort nor changes in systolic blood pressure. J. Sport. Sci. 2022, 40, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Karanasios, S.; Sozeri, A.; Koumantakis, G.A.; Gioftsos, G. Exercised-Induced Hypoalgesia following An Elbow Flexion Low-Load Resistance Exercise with Blood Flow Restriction: A Sham-Controlled Randomized Trial in Healthy Adults. Healthcare 2022, 10, 2557. [Google Scholar] [CrossRef] [PubMed]
- Grantham, B.; Korakakis, V.; O’Sullivan, K. Does blood flow restriction training enhance clinical outcomes in knee osteoarthritis: A systematic review and meta-analysis. Phys. Ther. Sport 2021, 49, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Koc, B.B.; Truyens, A.; Heymans, M.; Jansen, E.J.P.; Schotanus, M.G.M. Effect of Low-Load Blood Flow Restriction Training After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Int. J. Sport. Phys. Ther. 2022, 17, 334–346. [Google Scholar] [CrossRef]
- Cook, K.F.; Dunn, W.; Griffith, J.W.; Morrison, M.T.; Tanquary, J.; Sabata, D.; Victorson, D.; Carey, L.M.; Macdermid, J.C.; Dudgeon, B.J.; et al. Pain assessment using the NIH Toolbox. Neurology 2013, 80, S49–S53. [Google Scholar] [CrossRef]
- Ravn, P.; Frederiksen, R.; Skovsen, A.P.; Christrup, L.L.; Werner, M.U. Prediction of pain sensitivity in healthy volunteers. J. Pain Res. 2012, 5, 313–326. [Google Scholar] [CrossRef]
- Nielsen, C.S.; Staud, R.; Price, D.D. Individual Differences in Pain Sensitivity: Measurement, Causation, and Consequences. J. Pain 2009, 10, 231–237. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011; Volume 5. [Google Scholar]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef]
- Macedo, L.G.; Elkins, M.R.; Maher, C.G.; Moseley, A.M.; Herbert, R.D.; Sherrington, C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J. Clin. Epidemiol. 2010, 63, 920–925. [Google Scholar] [CrossRef]
- Moseley, A.M.; Rahman, P.; Wells, G.A.; Zadro, J.R.; Sherrington, C.; Toupin-April, K.; Brosseau, L. Agreement between the Cochrane risk of bias tool and Physiotherapy Evidence Database (PEDro) scale: A meta-epidemiological study of randomized controlled trials of physical therapy interventions. PLoS ONE 2019, 14, e0222770. [Google Scholar] [CrossRef]
- O’Brien, A.T.; Deitos, A.; Triñanes Pego, Y.; Fregni, F.; Carrillo-de-la-Peña, M.T. Defective Endogenous Pain Modulation in Fibromyalgia: A Meta-Analysis of Temporal Summation and Conditioned Pain Modulation Paradigms. J. Pain 2018, 19, 819–836. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.; De Vet, H.; Bie, R.; Kessels, A.G.; Boers, M.; Bouter, L.; Knipschild, P. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1999, 51, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.; Hartvigsen, J.; Ferreira, M.L.; Refshauge, K.M.; Machado, A.F.; Lemes, Í.R.; Maher, C.G.; Ferreira, P.H. Advice to Stay Active or Structured Exercise in the Management of Sciatica: A Systematic Review and Meta-analysis. Spine 2015, 40, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Lemes, Í.R.; Ferreira, P.H.; Linares, S.N.; Machado, A.F.; Pastre, C.M.; Netto, J.J. Resistance training reduces systolic blood pressure in metabolic syndrome: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sport. Med. 2016, 50, 1438–1442. [Google Scholar] [CrossRef]
- Machado, A.F.; Ferreira, P.H.; Micheletti, J.K.; de Almeida, A.C.; Lemes, Í.R.; Vanderlei, F.M.; Netto Junior, J.; Pastre, C.M. Can Water Temperature and Immersion Time Influence the Effect of Cold Water Immersion on Muscle Soreness? A Systematic Review and Meta-Analysis. Sport. Med. 2016, 46, 503–514. [Google Scholar] [CrossRef]
- Hill, E.C.; Housh, T.J.; Smith, C.M.; Keller, J.L.; Schmidt, R.J.; Johnson, G.O. Eccentric and concentric blood flow restriction resistance training on indices of delayed onset muscle soreness in untrained women. Eur. J. Appl. Physiol. 2019, 119, 2363–2373. [Google Scholar] [CrossRef]
- Varangot-Reille, C.; Cuenca-Martínez, F.; Suso-Martí, L.; La Touche, R.; Rouquette, A.; Hamon, J.; Araldi, M.; de Asís-Fernández, F.; Herranz-Gómez, A. Hypoalgesic effects of a blood flow restriction technique at moderate intensity with or without motor imagery: A single-blind randomized controlled trial. Somatosens. Mot. Res. 2022, 39, 29–38. [Google Scholar] [CrossRef]
- Bobes Álvarez, C.; Issa-Khozouz Santamaría, P.; Fernández-Matías, R.; Pecos-Martín, D.; Achalandabaso-Ochoa, A.; Fernández-Carnero, S.; Martínez-Amat, A.; Gallego-Izquierdo, T. Comparison of Blood Flow Restriction Training versus Non-Occlusive Training in Patients with Anterior Cruciate Ligament Reconstruction or Knee Osteoarthritis: A Systematic Review. J. Clin. Med. 2020, 10, 68. [Google Scholar] [CrossRef]
- Callanan, M.C.; Christensen, K.D.; Plummer, H.A.; Torres, J.; Anz, A.W. Elevation of Peripheral Blood CD34+ and Platelet Levels After Exercise With Cooling and Compression. Arthrosc. Sport. Med. Rehabil. 2021, 3, e399–e410. [Google Scholar] [CrossRef] [PubMed]
- Gladden, J.; Wernecke, C.; Rector, S.; Tecson, K.; McCullough, P. Pilot safety study: The use of vasper TM, a novel blood flow restriction exercise in healthy adults. J. Exerc. Phys. 2016, 19, 99–106. [Google Scholar]
- Koltyn, K.F.; Brellenthin, A.G.; Cook, D.B.; Sehgal, N.; Hillard, C. Mechanisms of exercise-induced hypoalgesia. J. Pain 2014, 15, 1294–1304. [Google Scholar] [CrossRef]
- Starowicz, K.; Malek, N.; Przewlocka, B. Cannabinoid receptors and pain. Wiley Interdiscip. Rev. Membr. Transp. Signal. 2013, 2, 121–132. [Google Scholar] [CrossRef]
- Koltyn, K.F.; Knauf, M.T.; Brellenthin, A.G. Temporal summation of heat pain modulated by isometric exercise. Eur. J. Pain 2013, 17, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Vierck, C.J., Jr.; Staud, R.; Price, D.D.; Cannon, R.L.; Mauderli, A.P.; Martin, A.D. The effect of maximal exercise on temporal summation of second pain (windup) in patients with fibromyalgia syndrome. J. Pain 2001, 2, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Lemley, K.J.; Hunter, S.K.; Bement, M.K. Conditioned pain modulation predicts exercise-induced hypoalgesia in healthy adults. Med. Sci. Sport. Exerc. 2015, 47, 176–184. [Google Scholar] [CrossRef]
- Koltyn, K.F.; Arbogast, R.W. Perception of pain after resistance exercise. Br. J. Sport. Med. 1998, 32, 20–24. [Google Scholar] [CrossRef]
- Koltyn, K.F.; Umeda, M. Exercise, Hypoalgesia and Blood Pressure. Sport. Med. 2006, 36, 207–214. [Google Scholar] [CrossRef]
- Pertovaara, A.; Huopaniemi, T.; Virtanen, A.; Johansson, G. The influence of exercise on dental pain thresholds and the release of stress hormones. Physiol. Behav. 1984, 33, 923–926. [Google Scholar] [CrossRef]
- Jones, M.D.; Valenzuela, T.; Booth, J.; Taylor, J.L.; Barry, B.K. Explicit Education About Exercise-Induced Hypoalgesia Influences Pain Responses to Acute Exercise in Healthy Adults: A Randomized Controlled Trial. J. Pain 2017, 18, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, A.; Saitoh, Y.; Kishima, H.; Shimokawa, T.; Oshino, S.; Hirata, M.; Kato, A.; Yoshimine, T. Reduction of intractable deafferentation pain by navigation-guided repetitive transcranial magnetic stimulation of the primary motor cortex. Pain 2006, 122, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Misra, G.; Paris, T.A.; Archer, D.B.; Coombes, S.A. Dose-Response Effect of Isometric Force Production on the Perception of Pain. PLoS ONE 2014, 9, e88105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study (Year) | Design | Total Sample Size N (Mean Age ± SD, Sex) | Interventions | Equipment | Follow-Up | Outcome Measures | Results |
|---|---|---|---|---|---|---|---|
| Hill et al. (2019) [48] | Parallel design | 25 healthy individuals (25 women) Ecc LIE-BFR (n = 12; 21.7 years ± 1.0) Con LIE-BFR (n = 13; 22.0 years ± 1.6) | Unilateral isokinetic elbow flexion (120° s) (1) Ecc LIE-BFR(40% AOP) at 30% of eccentric peak torque (30-15-15-15 reps) (2) Con LIE-BFR(40% AOP) at 30% of concentric peak torque (30-15-15-15 reps) | Inflatable cuffs with a manual pump (KAATSU Master, Sato Sports Plaza, Tokyo, Japan) | Between 7 testing days | PPTs at the biceps brachii muscle | There was no significant group × testing day interaction (p = 0.682) |
| Hughes et al. (2020) [29] | Cross-over design | 12 healthy individuals (29 ± 6 years; 10 men and 2 women) | Unilateral leg press (1) LIE using at 30% 1RM (30-15-15-15 reps) (2) LIE-BFR(40% AOP) at 30% 1RM (30-15-15-15 reps) (3) LIE-BFR(80% AOP) at 30% 1RM (30-15-15-15 reps) (4) HIE at 70% 1RM (4 sets × 10 reps) | Personalized Tourniquet system (Delfi Medical Inc, Vancouver, BC, Canada) | 5 min post-exercise 24 h post-exercise | PPTs at the dominant and nondominant quadriceps, dominant biceps brachii, nondominant upper trapezius muscles | LIE-BFR (80% AOP) showed significantly higher PPTs compared to all trials (p < 0.05) at all measurements sites 5 min post-exercise LIE-BFR (40% AOP) showed significantly higher PPT compared to LIE (p < 0.05) at all measurements sites 5 min post-exercise HIE showed higher PPTs compared to LIE (p < 0.05) at all measurements sites 5 min post-exercise |
| Hughes et al. (2021) [28] | Cross-over design | 12 healthy individuals (27 ± 6 years; 12 men) | Static bicycle X 20 min (1) LIE (2) LIE-BFR(40% AOP) at 40% VO2max (3) LIE-BFR(80% AOP) at 40% VO2max (4) HIE at 70% VO2max | Personalized tourniquet system (Delfi Medical Inc, Vancouver, BC, Canada) | 5 min post-exercise 24 h post-exercise | PPTs at the dominant and nondominant quadriceps, dominant biceps brachii, nondominant upper trapezius muscles | PPTs were significantly increased following BFR (40% AOP) and BFR (80% AOP) compared with LIE (p < 0.05). BFR (80% AOP) presented higher increase in PPTs compared to BFR (40% AOP) (p < 0.05). BFR (80% AOP) and HI-AE presented increased PPTs in remote areas of the body. |
| Karanasios et al. (2022) [32] | Parallel design | 40 healthy individuals (26.6 years ± 6.8; 17 women and 23 men) | Elbow flexion with dumbbells (1) LIE-BFR(40% AOP) at 30% RM (30-15-15-15 reps) (2) HIE at 70% RM (4 sets × 10 reps) | Personalized tourniquet system (Mad-Up Pro, France) | 5 min post-exercise | PPTs at the dominant and nondominant quadriceps, biceps brachii and upper trapezius muscles | Non-significant between-group changes in PPTs at all measurement sites Statistically significant reductions between pre- and post-exercise in LIE–BFR and HIE at dominant biceps brachii |
| Song et al. (2022) [31] | Cross-over design | 60 healthy individuals (21.8 years ± 3.2; 21 men, 39 women) | Isometric handgrip contraction (1) LIE-BFR (50% AOP) at 30% of max strength (4 sets × 2 min contraction) (2) LIE at 30% of max strength (4 sets × 2 min contraction) (3) control | Inflatable cuffs with a manual pump (E20, Hokanson Inc., Bellevue, WA, USA) | 5 min post-exercise | PPTs at the dominant forearm and ipsilateral tibialis anterior | PPTs increased similarly in both exercise groups compared to control at a local and non-local site. Non-significant differences between exercise conditions. |
| Song et al. (2022) [30] | Cross-over design | 40 healthy individuals (23.7 years ± 4.3; 18 men, 22 women) | Unilateral knee extension (1) LIE-BFR (80% AOP) at 30% RM (to failure) (2) LIE at 70% RM (to failure) (3) control | Inflatable cuffs with a manual pump (E20, Hokanson Inc., Bellevue, WA, USA) | 5 min post-exercise | PPTs at the dominant forearm and ipsilateral tibialis anterior | Both exercise conditions presented greater changes in PPTs compared to control (p > 0.05) Non-significant differences between exercise conditions |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hill et al. (2019) [48] | + | + | − | − | − | − | − | − | − | + | + | 4/10 |
| Hughes et al. (2020) [29] | + | + | + | + | − | − | − | + | + | + | + | 7/10 |
| Hughes et al. (2021) [28] | + | + | + | + | − | − | − | + | + | + | + | 7/10 |
| Karanasios et al. (2022) [32] | + | + | + | + | + | − | + | + | + | + | + | 9/10 |
| Song et al. (2022) [31] | + | + | + | − | − | − | − | + | + | + | + | 6/10 |
| Song et al. (2022) [30] | + | + | + | + | + | − | − | + | + | + | + | 8/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karanasios, S.; Lignos, I.; Kouvaras, K.; Moutzouri, M.; Gioftsos, G. Low-Intensity Blood Flow Restriction Exercises Modulate Pain Sensitivity in Healthy Adults: A Systematic Review. Healthcare 2023, 11, 726. https://doi.org/10.3390/healthcare11050726
Karanasios S, Lignos I, Kouvaras K, Moutzouri M, Gioftsos G. Low-Intensity Blood Flow Restriction Exercises Modulate Pain Sensitivity in Healthy Adults: A Systematic Review. Healthcare. 2023; 11(5):726. https://doi.org/10.3390/healthcare11050726
Chicago/Turabian StyleKaranasios, Stefanos, Ioannis Lignos, Kosmas Kouvaras, Maria Moutzouri, and George Gioftsos. 2023. "Low-Intensity Blood Flow Restriction Exercises Modulate Pain Sensitivity in Healthy Adults: A Systematic Review" Healthcare 11, no. 5: 726. https://doi.org/10.3390/healthcare11050726
APA StyleKaranasios, S., Lignos, I., Kouvaras, K., Moutzouri, M., & Gioftsos, G. (2023). Low-Intensity Blood Flow Restriction Exercises Modulate Pain Sensitivity in Healthy Adults: A Systematic Review. Healthcare, 11(5), 726. https://doi.org/10.3390/healthcare11050726