Abstract
The improvement of health literacy (HL) is a critical issue for college students who are in the transitional period to adulthood and are establishing their subsequent lifestyles. The present study aimed to evaluate the current state of HL among college students and to explore the factors that influence HL. Moreover, it investigated the relationship between HL and health conditions. For this study, the researchers conducted an online survey of college students. The questionnaire consisted of the Japanese version of the 47-item European Health Literacy Survey Questionnaire (HLS-EU-Q47), which is a self-assessment tool for HL that covers the major health issues of college students and health-related quality of life. The study analyzed 1049 valid responses. Based on the HLS-EU-Q47 total score, 85% of the participants exhibited problematic or unsatisfactory HL levels. Participants who reported high levels of healthy lifestyles obtained high HL scores. High levels of HL were associated with high levels of subjective health. Results from quantitative text analysis suggested that specific mindsets were correlated with high levels of competency in appraising health information among male students. In the future, educational intervention programs for college students need to be established to improve HL levels.
1. Introduction
As the world faced unprecedented challenges during the COVID-19 pandemic, it also witnessed social unrest through social media. The displayed behaviors included food hoarding at supermarkets, prejudice and discrimination against medical staff and their family members, and excessive reactions to reports of the side effects of vaccines. Such situations are a reminder of the importance of obtaining accurate health information and making informed decisions before taking appropriate actions. However, such decision-making is not necessarily easy in the current situation, in which a tremendous amount of information is being disseminated through the Internet and social networking services by people who lack expertise.
According to the Oxford English Dictionary (https://www.oed.com/ accessed on 30 November 2022), literacy originally referred only to the ability to read and write. As the disease structure changed over time, even in developing countries (i.e., from communicable to noncommunicable diseases, such as diabetes), literacy clearly became the cornerstone of disease prevention and health management. Therefore, scholarly attention focused on literacy regarding health or health literacy (HL). In 2012, Sørensen et al. [1] defined HL as follows:
…people’s knowledge, motivation, and competencies to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention, and health promotion to maintain or improve quality of life during the life course.
Now, the concept of HL has become widely known. In other words, HL is a term that includes not only decision-making but also problem-solving skills in healthcare, disease prevention, and health promotion.
HL is required when addressing not only the COVID-19 pandemic but also various daily situations, to enable individuals to manage their health on their own initiative. The results of systematic reviews suggest the various effects of HL on health outcomes. Particularly, the lower the level of HL, the higher the rates of hospitalization and emergency outpatient use and the fewer the opportunities for cancer screening and vaccination [2]. Older adults tend to display poor overall health status and high mortality rates [2]. Low levels of HL also result in additional medical costs [3]. Conversely, high levels of HL promote healthy lifestyle habits, such as the increased consumption of vegetables and fruits and less smoking [4].
The Japanese Ministry of Health, Labor, and Welfare is working to maintain the world’s top level of health, in the face of a declining birthrate and an aging population, and to prevent future generations from being burdened by mounting medical costs. In 2015, it envisioned ideal healthcare policies for Japan and proposed “Health Care 2035” [5]. In this proposal, the Ministry mentions that promoting improvement in HL across the nation is important, such that citizens can proactively select the medical services that are suitable for them in cooperation with medical professionals [6]. However, at present, the government or schools lack such opportunities for acquiring HL through education or such efforts from medical professionals and insurers.
College students in the transitional period to adulthood are becoming independent from their parents and are establishing their subsequent lifestyles. At the same time, students are responsible for their education, face various conflicts, and experience health problems specific to the learning process as they establish a wider range of social and human relationships than ever before in their university life [7,8,9]. Thus, improving the HL of college students is expected not only to contribute to their health but also to promote the health of society through their future careers. In 2021, 82.9% of Japanese individuals used the Internet [10]; therefore, promoting the provision of health information via the Internet is necessary. However, because the vast range of health information available on the Internet is not necessarily reliable, college students need to acquire the skills to judge the health information obtained from the Internet for themselves. Therefore, elucidating the current situation of HL among college students and the resources for such health information would be beneficial for the construction of new schemes for health education that center on HL. However, few studies have reported on the HL of college students.
To address this concern, the present study intends to evaluate the current state of HL among Japanese university students. It also examines the factors that influence HL and explores the relationship between HL and health conditions.
2. Method
2.1. Participants
The study recruited students between the ages of 18 and 29 years. They were currently enrolled at Osaka City University (https://www.osaka-cu.ac.jp/en [11] accessed on 16 November 2022) and Osaka Prefecture University (https://www.osakafu-u.ac.jp/en/ [12] accessed on 16 November 2022); both universities were merged into Osaka Metropolitan University in April 2022 (https://www.omu.ac.jp/en/ accessed on 16 November 2022) [13]. The exclusion criterion was difficulty in participating in the online survey using smartphones. The Ethical Committee of the Graduate School of Medicine of Osaka City University approved the research protocol (approval number: 2020-206). Students who met the abovementioned eligibility criterion were invited to participate through a learning management system. After reading the document that explained the objective of the study on a website, consent was considered to be given if the participants had ticked on the check column.
2.2. Procedure
This study is cross-sectional in nature and was conducted using a web survey site designed for its objective in December 2020 and October 2021. The questionnaire consisted of six sections, namely, demographic characteristics, sources of information on health, the content of health information from the Internet, self-perceived HL, common health problems, and health-related quality of life. In addition, we set an open-ended question in which the participants can freely describe the aspects they consider when obtaining or using health information (including that on the Internet). They were allowed to skip any question. The time required to answer the questionnaire was ~30 min. We entrusted the design of the web questionnaire and the collection of the responses to Data Select Co., Ltd. (Toyoake City, Aichi, Japan).
2.3. Self-Perceived HL
The study assessed HL using the Japanese version of the 47-item European Health Literacy Survey Questionnaire (HLS-EU-Q47) [14]. It is a self-report rating scale of HL developed by the European Health Literacy Survey, which can comprehensively evaluate not only HL at the individual level but also social policies and the local environment [15]. Nakayama et al. [14] confirmed the reliability and validity of the Japanese version of the HLS-EU-Q47. It assesses four competencies in processing health information and decision-making in health issues, namely, accessing, understanding, appraising, and applying. These competencies are assessed across three domains, namely, healthcare (medical care), disease prevention, and health promotion. The 47 items are rated using a five-point Likert-type scale (very difficult = 1, fairly difficult = 2, fairly easy = 3, very easy = 4, and don’t know/not applicable). The study coded the response don’t know/not applicable as a missing value, and results with missing values in even one of the 47 items were excluded from the analysis. Based on the method of the developer [15], the mean scores of each competency in the three domains were standardized to a maximum of 5 points using the following formula: (mean − 1) × 5/3. The total score of the 47 items was also standardized to a maximum of 50 points using the formula: (mean − 1) × 50/3. Furthermore, the standardized total scores were used to categorize HL levels, as follows: inadequate (0–25 points), problematic (>25, ≤33 points), sufficient (>33, ≤42 points), and excellent (>42, ≤50 points).
2.4. Health Challenges Common to College Students
Aiming to investigate the relationship between lifestyle habits that affect health conditions and HL, we investigated the common health challenges faced by college students. The American College Health Association (ACHA) (https://www.acha.org/ [16] accessed on 5 June 2020) regularly conducts a National College Health Assessment (https://www.acha.org/ncha [17] accessed on 5 June 2020), which is a national survey on the health of college students from various institutions across the United States. The ACHA identifies critical health issues for college students based on the results of the survey [18]. With reference to the critical health issues for college students suggested by the ACHA, we formulated seven questions on general health, exercise habits, smoking, sleep, vaccination, diet, and friendship. Items were rated using a five-point Likert-type scale (from strongly disagree to strongly agree).
2.5. Health-Related Quality of Life
Aiming to investigate the relationship between HL and subjective health awareness or comprehensive health status, we investigated the health-related quality of life of the participants. The Japanese version of the short form, (SF)-36, was used to evaluate comprehensive health status, which is one of the most widely and internationally used comprehensive health scales. Fukuhara et al. [19] confirmed the reliability and validity of the Japanese version. It consists of 36 items for evaluating eight dimensions of health (subdomains; see Table 1), which are rated using a Likert-type scale. Based on raw scores, the study calculated norm-based scores (from 0 = worst to 100 = best) using a web-based scoring system provided by iHope International Inc., in which the mean and standard deviation of the Japanese national standard value in 2007 were set as 50 and 10, respectively [20].

Table 1.
Concepts of the eight health dimensions of SF-36.
2.6. Quantitative Text Analysis
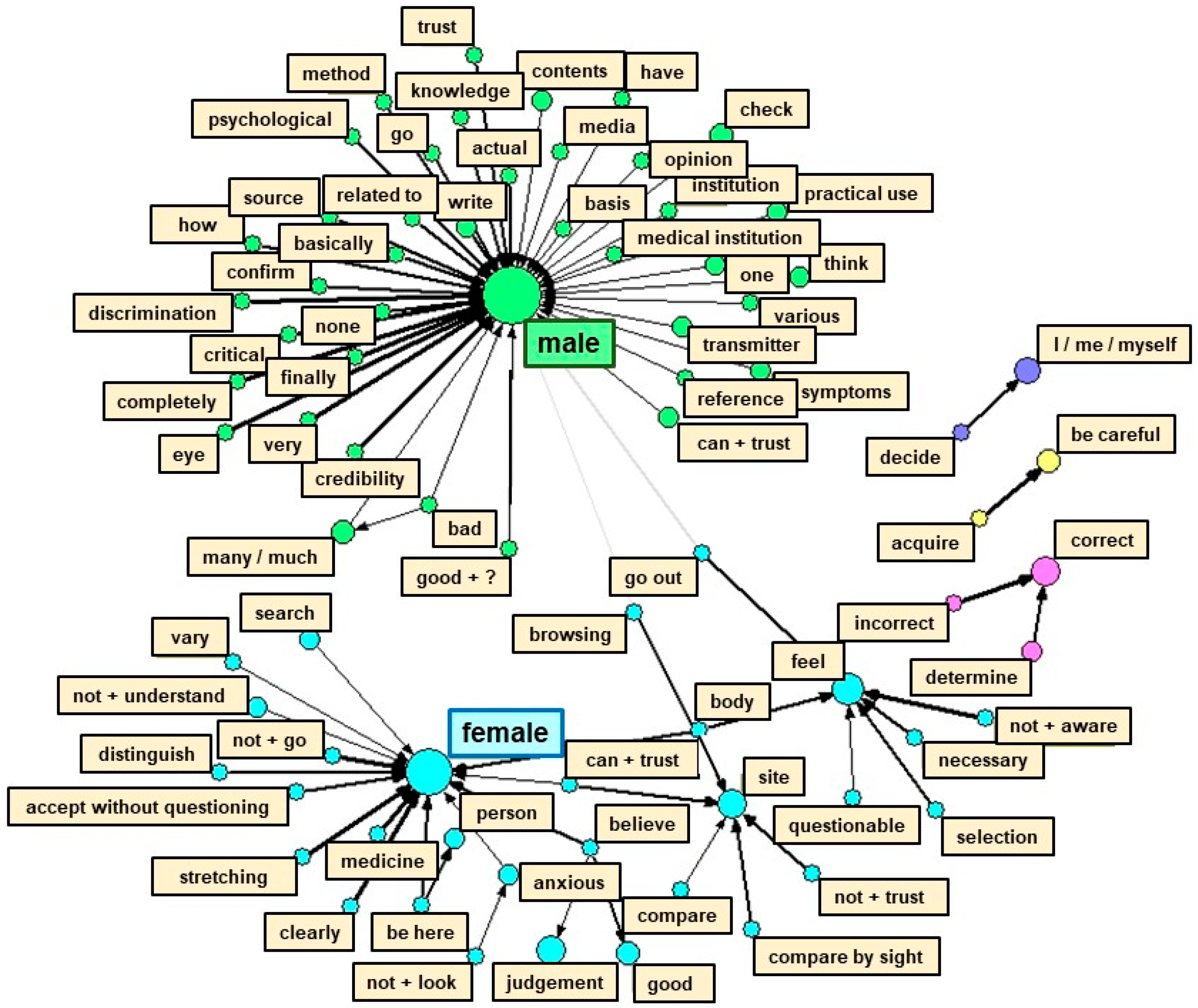
Among the open-ended responses, text data were quantified using the text mining method via language analysis software, Text Mining Studio version 6.4 (NTT Data Mathematical Systems, Tokyo, Japan). First, the researchers performed a morphological analysis of the text data by dividing sentences into the smallest grammatically meaningful components. A word relationship network was then created to visualize the characteristic terms that frequently appear in relation to gender. In this figure, arrows connected the co-occurring terms (frequently used together in sentences and exhibiting similar appearance patterns), which were then divided into several clusters. The stronger the degree of co-occurrence, the thicker the arrow; the larger the circle, the more frequent the appearance of a word [21]. Furthermore, the co-occurrence network schema was used to categorize the text data. We referred back to the original sentences containing terms that comprised a cluster to elucidate issues when obtaining and analyzing health information by gender [22,23,24].
2.7. Statistical Analysis
The researchers examined all variables for normal distribution using the Kolmogorov–Smirnov test. They performed comparisons between the two groups using an unpaired t-test and the Mann–Whitney U-test for normal and non-normal distribution, respectively. In addition, the study used Spearman’s correlation analysis to explore the correlation between variables, including categorical ones, and the χ2 test to compare the proportions of each item between the two groups. The Mantel–Haenszel test was used to identify trends between demographic characteristics and the levels of HL. Data were analyzed using SPSS version 27.0 (IBM Corporation, Armonk, NY, United States). A p-value of < 5% was considered statistically significant.
3. Result
3.1. Characteristics and Acquisition Status of Health Information
A total of 1322 students (98.1%), out of the 1347 students invited to participate in the web survey through the classes, agreed to participate. Responses were excluded if the age of the participants was unknown, or if the results of the HLS-EU-Q47 contained incomplete or missing values. After screening the responses, responses from 1049 participants (male: 623, female: 413; preferred not to respond: 13) were used for analysis. First-year undergraduate students accounted for 63.5% of the participants, and the average age of the entire sample was 19.8 ± 1.9 years (standard deviation (SD); see Table 2). The participants were distributed across eight faculties, including humanities and social sciences, science, and medical faculties. The gender distribution also represented the Japanese college student population.
Table 2.
Demographic data of the participants.
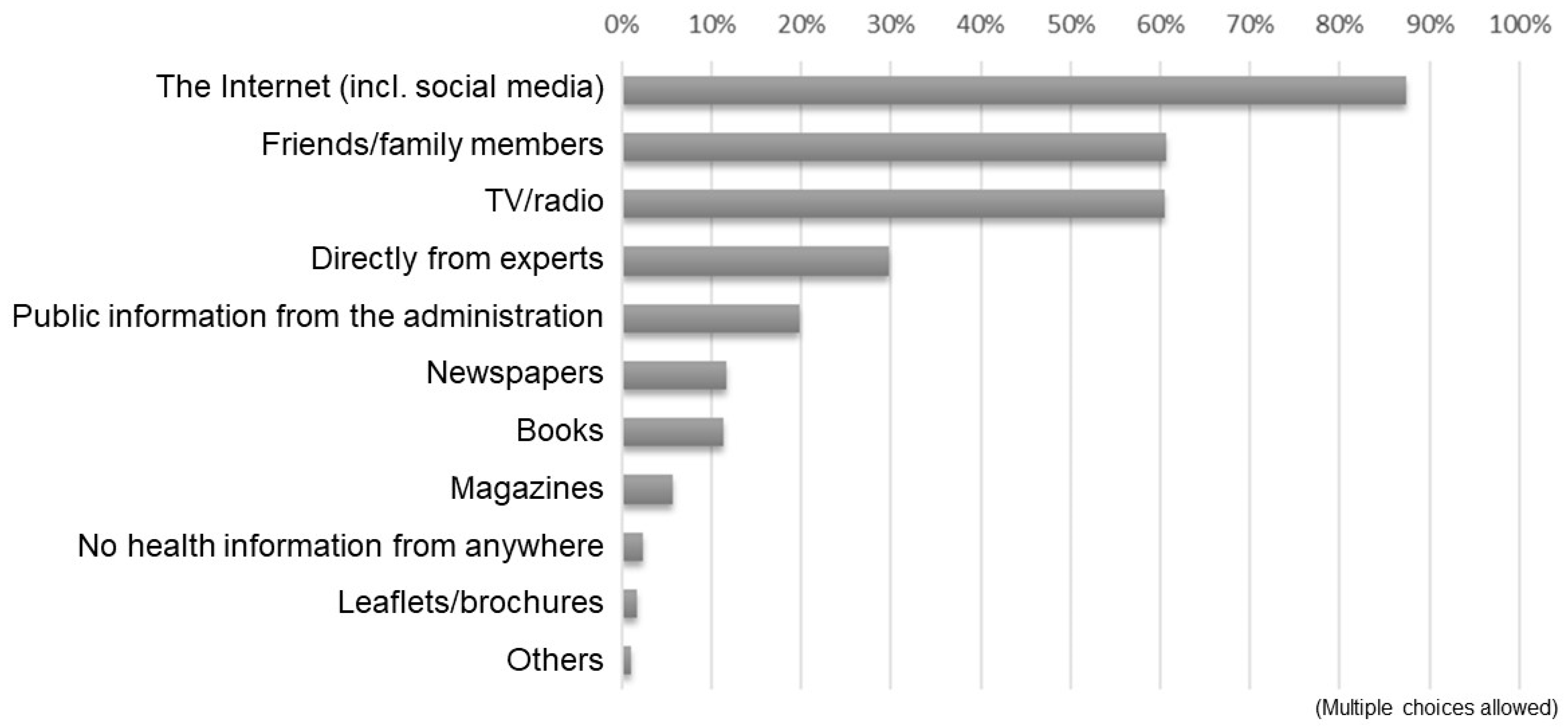
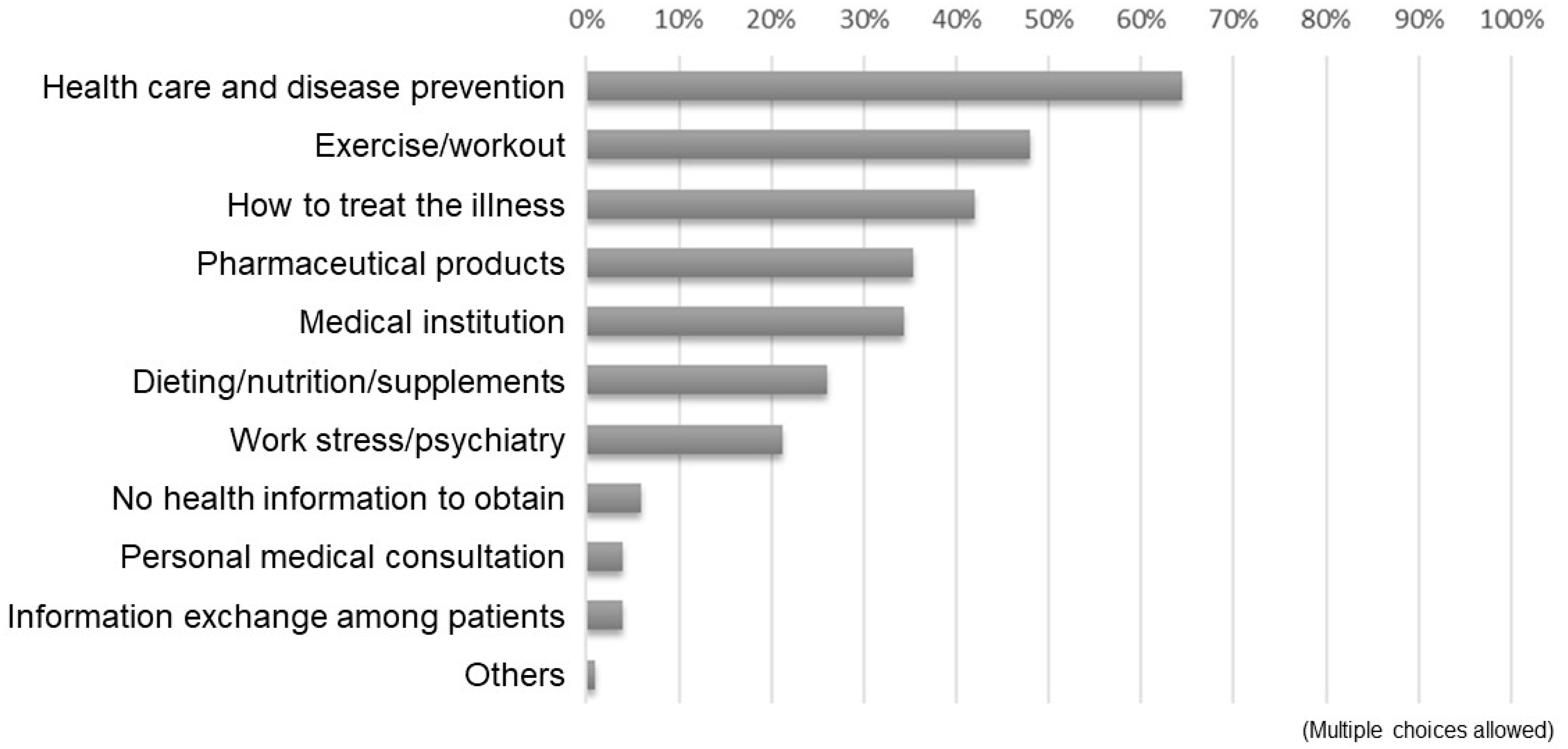
Figure 1 presents the results of the received responses to the question, “Which information source do you use when obtaining health information? (multiple choices allowed).” The majority used the Internet, including social media, as sources of health information, followed by friends/family members and TV/radio. Specific responses to “others” included university classes, academic papers, and ASMILE (a health app administered by the Osaka prefecture; https://www.asmile.pref.osaka.jp/ accessed on 14 January 2021), among others. Figure 2 depicts the results of the responses to the question, “What kind of health information do you obtain from the Internet? (multiple choices allowed).” The majority pointed to information on health management and disease prevention, followed by exercise and fitness, and therapeutic approaches for a disease.
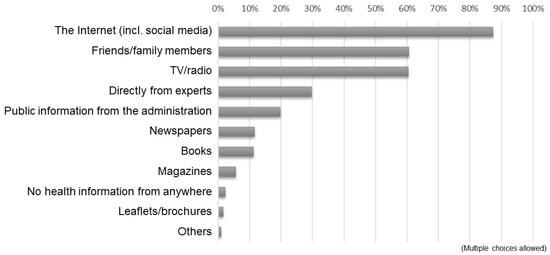
Figure 1.
Responses to the question, “Which information source do you use when obtaining health information?”.
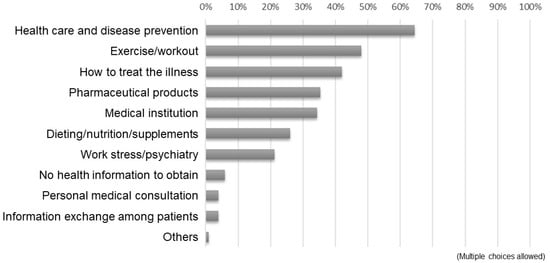
Figure 2.
Responses to the question, “What kind of health information do you obtain from the Internet?”.
3.2. Current State of HL
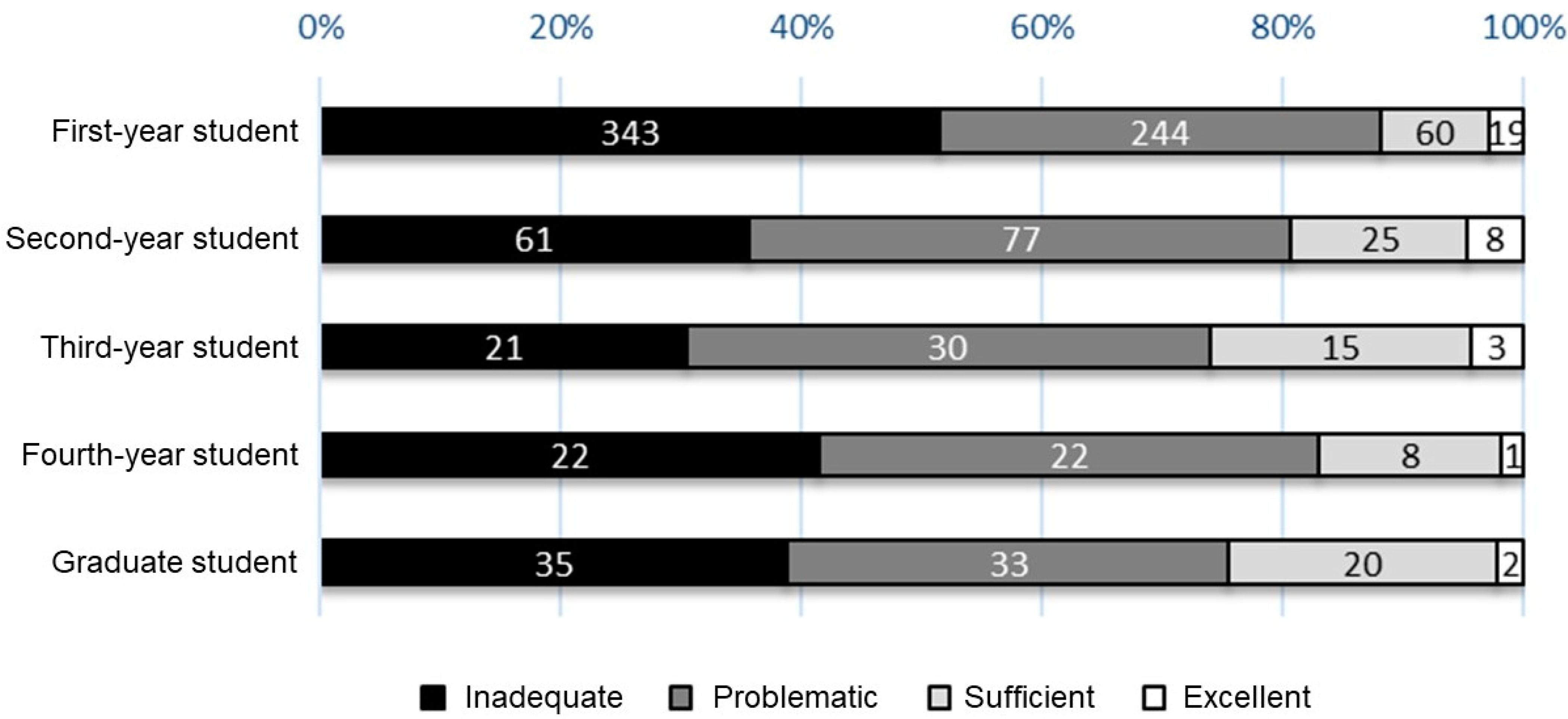
Table 3 displays the scores for each competency in the three domains of HLS-EU-Q47. Among the four competencies, appraising in all domains and applying in the field of health promotion resulted in lower scores, compared with those of other items. The average total score for HLS-EU-Q47 was 26.3 ± 7.7 points (out of 50 points); ~85% of the participants were categorized under an inadequate or problematic level of HL. Although no difference was noted in the total scores for HLS-EU-Q47 by gender (26.5 ± 8.3 points for male students, 26.0 ± 6.7 points for female students, p = 0.301), the distribution ratio of the levels of HL differed between men and women, in which the rates for inadequate and problematic were higher for female than for male students (p = 0.013). In addition, the distribution ratio differed according to their year of study, with inadequate being particularly high among first-year students (p-value for the trend < 0.001, Figure 3). Alternatively, the study observed no significant relationships in HL levels with the type of residence (living with family members, living alone, or living in a dormitory), annual household income, the presence or absence of current illnesses under treatment, or exercise habits.
Table 3.
Mean scores of each competency across the three domains of the HLS-EU-Q47.
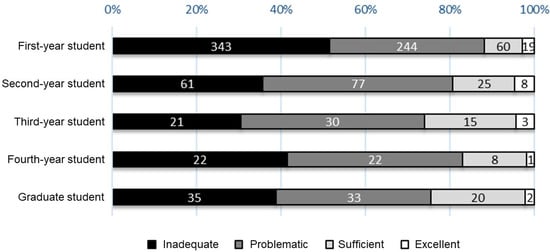
Figure 3.
HL levels according to the year level of participating students.
3.3. Relationships between Common Health Problems among College Students and HL
We examined the relationship between responses to questions about the major health issues of college students, as proposed by the ACHA, and the total scores for the HLS-EU-Q47. Participants who responded that they subjectively had a higher general health status showed higher total scores for HLS-EU-Q47 than those who did not (ρ = 0.128, p < 0.001). Similarly, participants who responded that they had acquired or practiced healthy lifestyle habits in terms of sleep (ρ = 0.078, p = 0.011), eating (ρ = 0.070, p = 0.024), and maintaining friendships (ρ = 0.064, p = 0.037) had higher total scores for HLS-EU-Q47 than those who did not. Surprisingly, the participants who answered that they had received the necessary vaccinations obtained lower total scores for HLS-EU-Q47 than those who did not (ρ = −0.097, p = 0.002). Neither the response to the question about regular physical activity nor about smoking habits were correlated to the total scores for HLS-EU-Q47 (see Figure S1A–G).
3.4. Association between HL Level and Health-Related QoL
We investigated the relationship between the levels of HL and calculated norm-based scores for each subdomain of the SF-36. The results indicated that high levels of HL were associated with high norm-based scores for physical functioning (ρ = 0.068, p = 0.027), role—physical (ρ = 0.121, p < 0.001), bodily pain (ρ = 0.091, p = 0.003), general health perceptions (ρ = 0.112, p < 0.001), vitality (ρ = 0.104, p < 0.001), role—emotional (ρ = 0.091, p = 0.003), and mental health (ρ = 0.078, p = 0.011). However, HL levels were not associated with a norm-based score for social functioning (See Figure S2A–H).
3.5. Quantitative Text Analysis of Open-Ended Responses
A total of 368 participants provided responses to the open-ended question, “What aspects do you carefully consider on a daily basis or find difficult when obtaining and applying health-related information (including that from the Internet)?” Table 4 presents basic data regarding the sentence composition of text data. To identify the terms that appeared in the responses, we conducted a frequency analysis to create a list of the top 20 most frequently used terms (Table 5). Specific items related to the content of information to be obtained, such as “disease” and “symptoms,” and those related to personal mindset when accessing and evaluating information, such as “multiple (websites),” “be careful,” and “confirmation,” frequently appeared. Terms that expressed opinions about health information, such as “(the amount of information is too) much” and “(it is difficult to judge) credibility,” were also included.
Table 4.
Sentence composition of text data in the open-ended responses.
Table 5.
Top 20 most frequent terms among the contents of the open-ended responses.
Figure 4 depicts the co-occurrence network schema. Since a difference in the distribution ratio of the levels of HL between males and females was found, we mapped the relationship between gender and the terms used to explore the characteristics of the responses by gender. We grouped terms with similar appearance patterns into several clusters. When referring to the original sentences in the responses on the basis of these clusters, we found that an extremely common opinion for the male and female students references the difficulty found in distinguishing reliable information in the vast amount of medical and health-related information on the Internet. As a characteristic of their responses, the male students provided many descriptions of specific behaviors or mindsets for improving HL, such as “comparing multiple pieces of information.” Similarly, many male participants responded that they “always look at information with a critical eye” and “always check the source of the information.” Conversely, many female students responded with “I’m not sure that information is believable, except in the case where the credibility of it is clearly questionable” and “I can’t judge whether information is applicable to me” (Table 6).
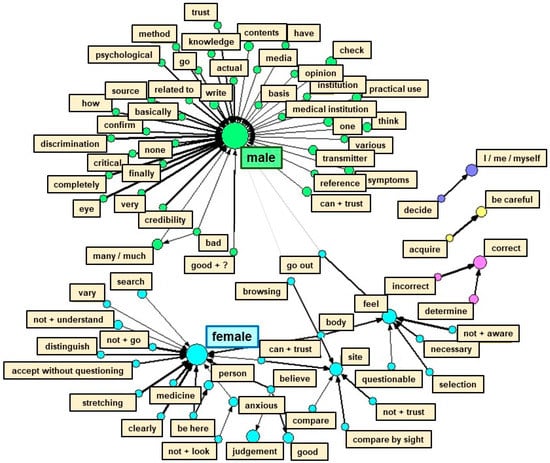
Figure 4.
Co-occurrence network schema for visualizing the characteristic terms that frequently appeared in relation to gender in the contents of the open-ended responses. The more frequently the terms appeared together in the sentences, the thicker the arrow; the larger the circle, the more frequently the term appeared.
Table 6.
Content categorization of details in the open-ended responses.
4. Discussion
The majority of the participants responded that they used the Internet, including social media, as the main source of health information. Female and lower-grade students were more likely to exhibit low levels of HL. In addition, these levels were low in comparison with those of college students in other countries. In particular, the scores for the HLS-EU-Q47 were low in the competencies appraising health information in all fields and applying health information in the field of health promotion. In contrast, high levels of HL were associated with positive lifestyle habits for health maintenance and positive subjective health status.
HL is the ability to make decisions about health maintenance and management, based on health information [1]. Researchers demonstrate that insufficient HL exerts a negative impact on health outcomes. People with inadequate HL are less likely to receive preventive services, such as health checkups [2], lack knowledge about diseases and treatments [25], experience difficulty in communicating their symptoms and concerns to medical staff [26], exhibit high rates of hospitalization and mortality [2], and are consequently obliged to spend extra money on medical costs [3]. In the current study, high levels of HL were associated with positive lifestyle habits for health maintenance and high subjective health status. This result is consistent with those of the abovementioned studies. In particular, for college students who are in the process of becoming socially and economically independent from their parents, improving HL is critical for acquiring and maintaining a healthy lifestyle for the rest of their lives.
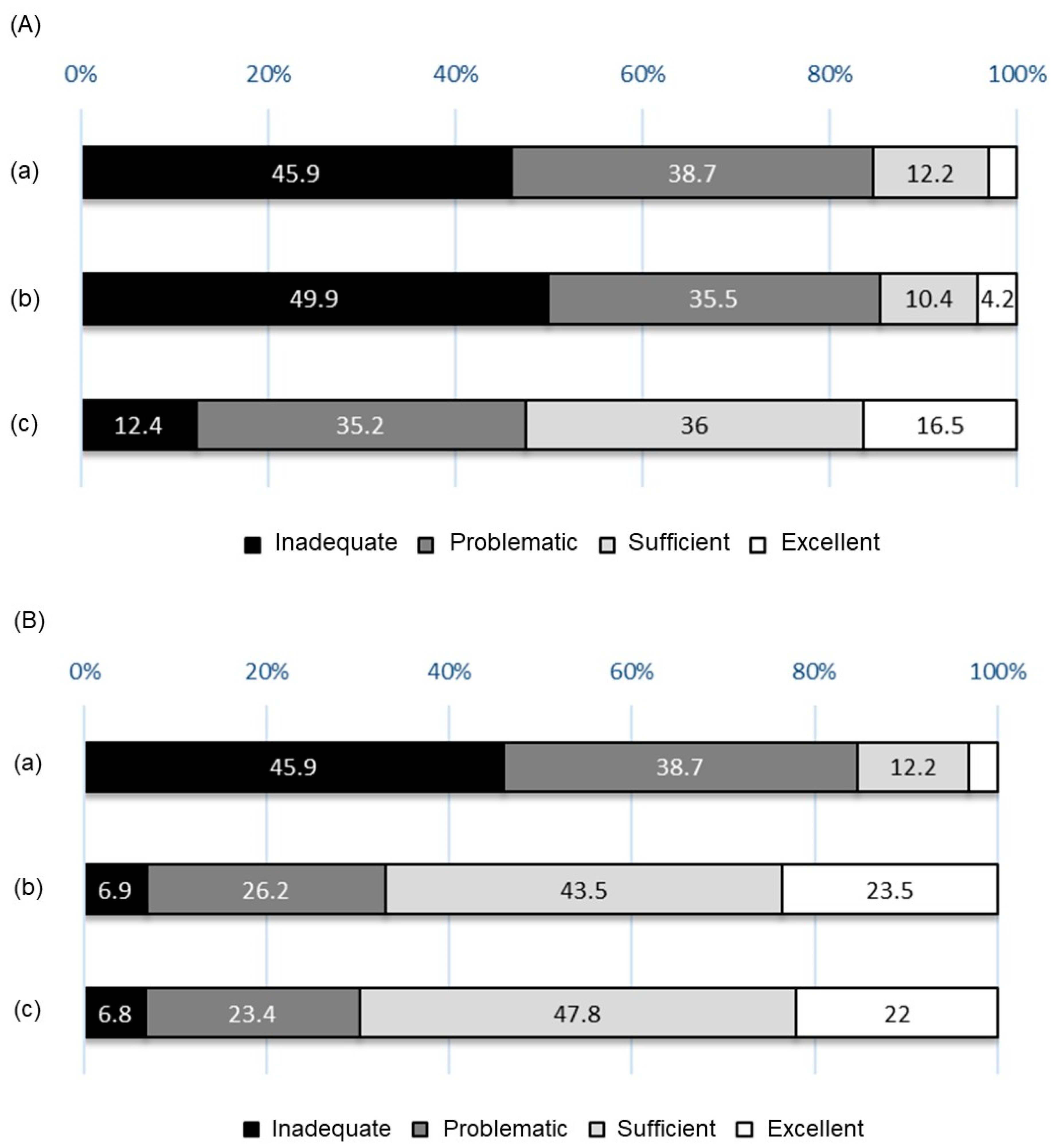
The levels of HL of the participants were low, and the distribution ratio of the levels of HL was similar to those from a previous survey by Nakayama et al., who reported that the levels of HL among the Japanese were lower than those of people in European countries (Figure 5A) [14]. Likewise, this pattern was observed when comparing the results with those of surveys that evaluated the HL levels of college students in other countries, using the HLS-EU-Q47 (Figure 5B) [27,28]. Japan was recognized as having a high literacy rate, despite the fact that no literacy survey was conducted in Japan for many years. In addition, the majority of Japanese people can read the labels on food packages/medicine and can understand explanations from medical staff without difficulty. Therefore, scholars considered that the Japanese possess sufficient levels of HL. However, Nakayama et al. concluded, and the current study confirmed, that these levels were inadequate when evaluated using the HLS-EU-Q47. Particularly, they exhibited difficulty in processing health information in terms of appraising the reliability of and applying health information. This result may be partially attributable to the lack of national online platforms that provide neutral, authoritative, comprehensive, and understandable health information. In June 2022, the government announced a policy to establish a Japanese version of the Centers for Disease Control and Prevention of the United States [29]; currently, however, none exists. Therefore, the demand of the Japanese people for appropriate health information has remained unmet. Even without such support, primary care physicians can initially play a role in understanding the healthcare needs of patients and in providing medical information. However, no public scheme exists for people to receive support from physicians or public health nurses as a way to implement primary care from childhood. In addition, the basic school education offered in Japan does not address the HL of students, which may contribute to the inadequate level of HL among the Japanese.
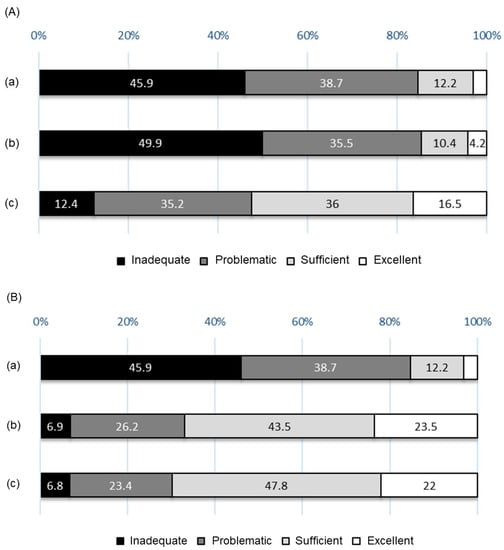
Figure 5.
(A) Comparison with previous reports on HL levels. (a) The results of this study; (b) the results from 927 Japanese individuals (age: 20–69 years; [14]); (c) the results from 8102 individuals aged 15 years or older, drawn from eight EU countries [14]. (B) Comparison with previous reports on HL levels among college students. (a) The results of this study; (b) the results of 912 students (excluding medical students) from four universities in central Lithuania [27]; (c) the results of 381 medical students at the University of Granada, Spain [28].
In the present study, being female and in the early stages of university studies were associated with inadequate levels of HL. In previous studies that investigated HL among college students, a few of the researchers concluded that no gender difference exists [30], whereas others found that female students displayed higher levels of HL compared with male students [27,31]. Thus, mixed evidence exists. The inclusion of medical faculties, such as nursing faculties, which have a high proportion of female students as survey targets, may have influenced the results of previous reports in which female students displayed higher levels of HL [31]. On the basis of the results of the quantitative text analysis conducted in the present survey, many female students responded, “Because there is too much information, I’m not sure which one is applicable to me.” Alternatively, the responses of the male students included many descriptions of attitudes toward the use of health information, such as “use multiple sources,” “examine information with a critical eye,” and “always check the source of information.” From these responses, female students appear less confident in judging the applicability of health information for themselves, especially when they obtain a plethora of information. In contrast, male students tend to try to confirm the credibility of the information by exploring a great deal of information. The difference between male and female students in dealing with health information may have contributed to the higher HL levels of male students, compared with those of female students.
One of the reasons that we decided to conduct this survey was concern about students’ perceptions of the COVID-19 vaccine. Few students could explain exactly what “95% vaccine efficacy rate” meant. Notably, some female students believed that they would experience infertility in the future if they received vaccinations for COVID-19. Interestingly, in the present study, the participants who reported receiving the necessary vaccinations exhibited low levels of HL. Previous studies have reported that high levels of HL were associated with high rates of vaccination intention and vaccination [32,33,34]; thus, the results of the current study were contrary to expectations. A recent survey in Brazil used the parental health literacy activities test, the PHLAT-8, to assess the HL of adolescents. The authors reported that the higher the level of HL, the higher the rate of recognition of COVID-19 as a threat. However, the authors found no association between HL level and the willingness to receive vaccinations [35]. The mass immunization of students against COVID-19 at the universities that the participants of the current study attended began in July 2021. Therefore, within the study period, the number of participants who considered the COVID-19 vaccine when responding to the question about vaccination is estimated at <30%. Suzuki et al. recently reported that female students’ willingness to receive a vaccination against human papillomavirus was not associated with HL regarding the HPV vaccine [36]. Their results may stem from the fact that the Japanese government stopped proactively recommending the HPV vaccine from 2013 to 2021. Furthermore, in Japan, people aged < 20 years demonstrated higher rates of vaccination against measles and rubella than those aged > 20 years [37]. Therefore, the government’s campaign to recommend vaccination is considered to have influenced the vaccination rate during the campaign period, which may have led to a high vaccination rate among younger participants with low HL levels in this study. Nevertheless, misinformation regarding the COVID-19 vaccine can discourage people from taking actions that benefit their own health and can unnecessarily inflame anxiety about their daily lives. By providing adequate, easy-to-understand information, the government can significantly help them to make informed decisions regarding vaccination.
As previously mentioned, promoting HL education according to the developmental stage, individual characteristics, and social conditions of the time is important for improving the HL of college students. School education plays a major role, especially during the period leading up to college. In particular, college students undertaking medical courses generally exhibit higher levels of HL than those in nonmedical departments [38,39]. In addition, the more the students undertake health education-related classes, the better their competency in accessing and understanding health information in the health promotion domain [27]. However, providing health education is insufficient for improving HL. According to a systematic review of HL among college students, although the majority responded that they used the Internet to obtain health information, they considered their competencies in searching for health information as low and answered that they were unable to find the health information they needed. In particular, they found that critically evaluating information and determining whether or not a data source provided primary or secondary information are difficult aspects to manage. As a result, they displayed negative attitudes toward participation in online health programs and online medical consultations [40]. To address these issues, educational programs that enhance the competencies of college students in examining the information necessary for health promotion, critical thinking about health, and communication skills in relation to health information should be developed. Moreover, practicing such programs that target students in the early grades as standard in educational settings is desirable.
This study has its limitations. First, the HLS-EU-Q47 is a self-reported evaluation tool; thus, the results may deviate from the actual situation in terms of HL. However, the majority of available objective assessment tools consist of questions on competency in reading the information on food labels or calculating accurate doses of medicines. In a case where such objective assessment tools were applied to the current participants, the overall rates of correct responses were expected to be extremely high; thus, individual differences in HL levels cannot be detected. The HLS-EU-Q47 is a widely and internationally used evaluation tool, and the validity of the Japanese version has been verified. Therefore, the study was able to compare HL levels among college students in different countries. We also believe that the results could highlight future challenges in improving HL levels among college students. Second, the HLS-EU-Q47 was conducted via a web survey. Therefore, students who encountered difficulties in responding using smartphones were excluded. This may have influenced the results of the self-assessment of HL regarding Internet use. Furthermore, the majority of the participants were recruited from liberal arts classes at Osaka City University and Osaka Prefectural University. Thus, > 60% were first-year undergraduate students, although they belonged to diverse departments. Generally, first-year college students have just become independent from their parents in terms of living; actually, they show lower levels of HL than those in higher grades of university. This might be the reason why the participants in this study had low levels of HL. Finally, because the survey aimed to evaluate the current state of HL and explore the association between lifestyle or comprehensive health status and HL among Japanese university students, we could not elucidate more details about their sociodemographic data. For example, although the participants were distributed across eight faculties, to what department each student belonged was not considered. However, attributes such as their department, as well as their previous health education, may affect the levels of HL to a non-negligible degree. In the future, clarifying the factors that contribute to HL after adjusting for the effects of such data may provide clues to identify effective intervention targets.
5. Conclusions
High levels of HL among college students were associated with more preferable lifestyle habits for health maintenance, along with high levels of subjective health status. The results revealed challenges in facilitating good decision-making for healthcare and promotion throughout life among students with low levels of HL. The challenges need to be kept in mind even as we are gradually returning to normality after the 3-year COVID-19 pandemic. Based on the accumulation of various cases and experiences during the COVID-19 pandemic in Japan and overseas, developing teaching materials for improving the competencies labeled appraising and applying health information is a necessary aspect. In addition, future studies should determine whether or not such interventions through educational programs can enhance the levels of HL among college students and whether enhancing HL levels can improve health outcomes.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare11050704/s1.
Author Contributions
Conceptualization, H.Y., D.I., Y.S. and A.O.; methodology, H.Y., D.I., Y.S. and A.O.; formal analysis, H.Y.; investigation, H.Y., D.I., Y.S., A.O., H.W., H.K., T.M., I.Y., S.T., Y.M. and K.O.; data curation, H.Y., D.I., Y.S. and A.O.; Writing—original draft preparation, H.Y.; Writing—review and editing, H.Y., D.I., Y.S., A.O., H.W., H.K., T.M., I.Y., S.T., Y.M. and K.O.; supervision, H.Y., D.I., Y.S. and A.O.; project administration, H.Y.; funding acquisition, H.Y., D.I., Y.S., A.O., H.W. and K.O. All authors have read and agreed to the published version of the manuscript.
Funding
The present study was funded in part by an Osaka City University Grant for Distinctive Education Programs in 2020 and 2021.
Institutional Review Board Statement
The Ethical Committee of the Graduate School of Medicine of Osaka City University (approval number: 2020-206) approved the research protocol.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are openly available on FigShare at doi:10.6084/m9.figshare.21874947.
Acknowledgments
We thank our participants for their time and cooperation in this investigation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Consortium Health Literacy Project E. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Viera, A.; Crotty, K.; Holland, A.; Brasure, M.; Lohr, K.N.; Harden, E.; et al. Health literacy interventions and outcomes: An updated systematic review. Evid. Rep. Technol. Assess (Full Rep.) 2011, 199, 1–941. [Google Scholar]
- Eichler, K.; Wieser, S.; Brügger, U. The costs of limited health literacy: A systematic review. Int. J. Public Health 2009, 54, 313–324. [Google Scholar] [CrossRef]
- von Wagner, C.; Knight, K.; Steptoe, A.; Wardle, J. Functional health literacy and health-promoting behaviour in a national sample of British adults. J. Epidemiol. Community Health 2007, 61, 1086–1090. [Google Scholar] [CrossRef] [PubMed]
- The Japan Vision: Health Care. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/hokabunya/shakaihoshou/hokeniryou2035/ (accessed on 7 December 2022).
- The Japan Vision: Health Care 2035 Executive Summary. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/hokabunya/shakaihoshou/hokeniryou2035/assets/file/healthcare2035_proposal_150609.pdf (accessed on 7 December 2022).
- Conley, C.; Kirsch, A.; Dickson, D.; Bryant, F. Negotiating the transition to college: Developmental trajectories and gender differences in psychological functioning, cognitive-affective strategies, and social well-being. Emerg Adulthood. 2014, 2, 195–210. [Google Scholar] [CrossRef]
- Deasy, C.; Coughlan, B.; Pironom, J.; Jourdan, D.; Mannix-McNamara, P. Psychological distress and coping amongst higher education students: A mixed method enquiry. PLoS ONE 2014, 9, e115193. [Google Scholar] [CrossRef] [PubMed]
- Bewick, B.; Koutsopoulou, G.; Miles, J.; Slaa, E.; Barkham, M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud. High Educ. 2010, 35, 633–645. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications. Trends in digital utilization in Japanese people. Available online: https://www.soumu.go.jp/johotsusintokei/whitepaper/ja/r04/html/nd238110.html (accessed on 8 February 2023).
- Osaka City University. Available online: https://www.osaka-cu.ac.jp/en (accessed on 7 December 2022).
- Osaka Prefecture University. Available online: https://www.osakafu-u.ac.jp/en/ (accessed on 7 December 2022).
- Osaka Metropolitan University. Available online: https://www.omu.ac.jp/en/ (accessed on 7 December 2022).
- Nakayama, K.; Osaka, W.; Togari, T.; Ishikawa, H.; Yonekura, Y.; Sekido, A.; Matsumoto, M. Comprehensive health literacy in Japan is lower than in Europe: A validated Japanese-language assessment of health literacy. BMC Public Health 2015, 15, 505. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed]
- The American College Health Association. Available online: https://www.acha.org/ (accessed on 8 December 2022).
- The National College Health Assessment. Available online: https://www.acha.org/ncha (accessed on 8 December 2022).
- Britt, R.K.; Collins, W.B.; Wilson, K.; Linnemeier, G.; Englebert, A.M. eHealth literacy and health behaviors affecting modern college students: A pilot study of issues identified by the American College Health Association. J. Med. Internet Res. 2017, 19, e392. [Google Scholar] [CrossRef]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Suzukamo, Y. Manual of SF-36v2 Japanese Version; iHope International Inc.: Kyoto, Japan, 2004; Volume 2019. [Google Scholar]
- Mabuchi, Y.; Okawara, C.; Mendez-Ferrer, S.; Akazawa, C. Cellular heterogeneity of mesenchymal stem/stromal cells in the bone marrow. Front. Cell Dev. Biol. 2021, 9, 689366. [Google Scholar] [CrossRef] [PubMed]
- Berry, M. Survey of Text Mining; Springer: New York, NY, USA, 2004. [Google Scholar]
- Deguchi, M.; Yokoyama, H.; Hongu, N.; Watanabe, H.; Ogita, A.; Imai, D.; Suzuki, Y.; Okazaki, K. Eating perception, nutrition knowledge and body image among para-athletes: Practical challenges in nutritional support. Nutrients 2021, 13, 3120. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Deguchi, M.; Hongu, N. The role of diets and dietitians for para-athletes: A pilot study based on interviews. Nutrients 2022, 14, 3720. [Google Scholar] [CrossRef]
- Wolf, M.S.; Davis, T.C.; Arozullah, A.; Penn, R.; Arnold, C.; Sugar, M.; Bennett, C.L. Relation between literacy and HIV treatment knowledge among patients on HAART regimens. AIDS Care 2005, 17, 863–873. [Google Scholar] [CrossRef]
- Kebede, B.G.; Abraha, A.; Andersson, R.; Munthe, C.; Linderholm, M.; Linderholm, B.; Berbyuk Lindström, N. Communicative challenges among physicians, patients, and family caregivers in cancer care: An exploratory qualitative study in Ethiopia. PLoS ONE 2020, 15, e0230309. [Google Scholar] [CrossRef]
- Sukys, S.; Cesnaitiene, V.J.; Ossowsky, Z.M. Is health education at university associated with students’ health literacy? Evidence from cross-sectional study applying HLS-EU-Q. Biomed. Res. Int. 2017, 2017, 8516843. [Google Scholar] [CrossRef]
- Rueda-Medina, B.; Gómez-Urquiza, J.L.; Tapia-Haro, R.; Casas-Barrágan, A.; Aguilar-Ferrándiz, M.E.; Correa-Rodríguez, M. Assessing health science students’ health literacy and its association with health behaviours. Health Soc. Care Community 2020, 28, 2134–2139. [Google Scholar] [CrossRef]
- The Japan News. Govt to Set Up Japanese Version of CDC. June 15. Available online: https://japannews.yomiuri.co.jp/politics/politics-government/20220615-37786/ (accessed on 14 December 2022).
- Elsborg, L.; Krossdal, F.; Kayser, L. Health literacy among Danish university students enrolled in health-related study programmes. Scand. J Public Health 2017, 45, 831–838. [Google Scholar] [CrossRef]
- Rababah, J.A.; Al-Hammouri, M.M.; Drew, B.L.; Aldalaykeh, M. Health literacy: Exploring disparities among college students. BMC Public Health 2019, 19, 1401. [Google Scholar] [CrossRef]
- Marzo, R.R.; Su, T.T.; Ismail, R.; Htay, M.N.N.; Essar, M.Y.; Chauhan, S.; Patalinghug, M.E.; Kucuk Bicer, B.; Respati, T.; Fitriyana, S.; et al. Digital health literacy for COVID-19 vaccination and intention to be immunized: A cross sectional multi-country study among the general adult population. Front. Public Health 2022, 10, 998234. [Google Scholar] [CrossRef] [PubMed]
- Popa, A.D.; Enache, A.I.; Popa, I.V.; Antoniu, S.A.; Dragomir, R.A.; Burlacu, A. Determinants of the hesitancy toward COVID-19 vaccination in Eastern European countries and the relationship with health and vaccine literacy: A literature review. Front. Public Health 2022, 10, 672. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Ando, S.; Fukuda, K. Knowledge and preventive actions toward COVID-19, vaccination intent, and health literacy among educators in Japan: An online survey. PLoS ONE 2021, 16, e0257552. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, S.M.; Avila, M.A.G.; Prata, R.A.; Nunes, H.R.C.; Silva, J.B.D. Association of health literacy, COVID-19 threat, and vaccination intention among Brazilian adolescents. Rev. Lat. Am. Enfermagem. 2022, 30, e3759. [Google Scholar] [CrossRef]
- Suzuki, T.; Ota, Y.; Sakata, N.; Fujita, N.; Kamatsuka, M.; Nagashima, K.; Hirayama, J.; Fujita, N.; Shiga, K.; Oyama, N.; et al. HPV vaccine intention among university students during suspension of active recommendation in Japan. Hum. Vaccin. Immunother. 2022, 18, 2116900. [Google Scholar] [CrossRef]
- Takeuchi, J.; Goto, M.; Kawamura, T.; Hiraide, A. Social regulations predispose people to complete vaccination for vaccine-preventable diseases. Tohoku J. Exp. Med. 2014, 234, 183–187. [Google Scholar] [CrossRef]
- Yang, S.C.; Luo, Y.F.; Chiang, C.H. The associations among individual factors, eHealth literacy, and health-promoting lifestyles among college students. J. Med. Internet Res. 2017, 19, e15. [Google Scholar] [CrossRef]
- Tsukahara, S.; Yamaguchi, S.; Igarashi, F.; Uruma, R.; Ikuina, N.; Iwakura, K.; Koizumi, K.; Sato, Y. Association of eHealth literacy with lifestyle behaviors in university students: Questionnaire-based cross-sectional study. J. Med. Internet Res. 2020, 22, e18155. [Google Scholar] [CrossRef]
- Stellefson, M.; Hanik, B.; Chaney, B.; Chaney, D.; Tennant, B.; Chavarria, E.A. eHealth literacy among college students: A systematic review with implications for eHealth education. J. Med. Internet Res. 2011, 13, e102. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).