
Collaborative Learning through a Virtual Community of Practice in Dementia Care Support: A Scoping Review




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy and Databases
2.3. Eligibility Criteria
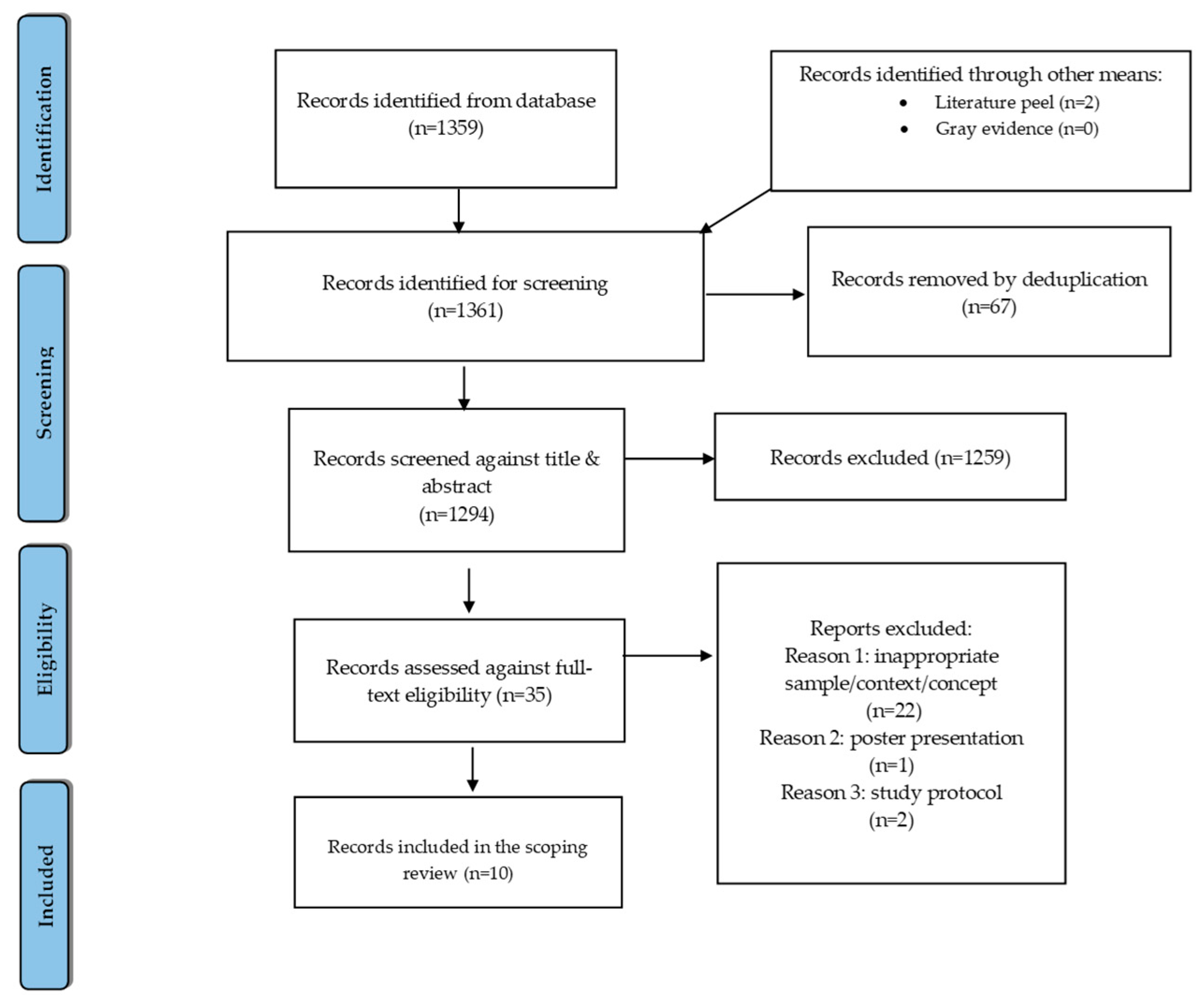
2.4. Selection of Sources of Evidence
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Study Characteristics
3.2. Themes
3.2.1. Knowledge Acquisition
3.2.2. Strengthening Resilience Capacity
4. Discussion
Strengths and Limitations
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1 & 2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and, if available, provide registration information, including the registration number. | NA |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3 |
| Information sources * | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 3 |
| Search | 8 | Present the full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 3 |
| Selection of sources of evidence † | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 3 |
| Data charting process ‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 5–8 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used, and how this information was used in any data synthesis (if appropriate). | NA |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 3 & 4 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 4 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 5 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | NA |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 5, 9–10 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 5, 9–10 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 11 & 12 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 12 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 12 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 13 |
References
- Vatanabe, I.P.; Manzine, P.R.; Cominetti, M.R. Historic concepts of dementia and Alzheimer’s disease: From ancient times to the present. Rev. Neurol. 2020, 176, 140–147. [Google Scholar] [CrossRef]
- Ricci, G. Social Aspects of Dementia Prevention from a Worldwide to National Perspective: A Review on the International Situation and the Example of Italy. Behav. Neurol. 2019, 2019, 8720904. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.; Orellana Rios, C.L.; Lahmann, C.; Rücker, G.; Bauer, J.; Boeker, M. Anxiety as a risk factor of Alzheimer’s disease and vascular dementia. Br. J. Psychiatry 2018, 213, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Thordardottir, B.; Malmgren Fänge, A.; Lethin, C.; Rodriguez Gatta, D.; Chiatti, C. Acceptance and Use of Innovative Assistive Technologies among People with Cognitive Impairment and Their Caregivers: A Systematic Review. BioMed Res. Int. 2019, 2019, 9196729. [Google Scholar] [CrossRef] [PubMed]
- Palesi, F.; De Rinaldis, A.; Vitali, P.; Castellazzi, G.; Casiraghi, L.; Germani, G.; Bernini, S.; Anzalone, N.; Ramusino, M.C.; Denaro, F.M.; et al. Specific Patterns of White Matter Alterations Help Distinguishing Alzheimer’s and Vascular Dementia. Front. Neurosci. 2018, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Lethin, C.; Leino-Kilpi, H.; Roe, B.; Soto, M.M.; Saks, K.; Stephan, A.; Zwakhalen, S.; Zabalegui, A.; Karlsson, S. Formal support for informal caregivers to older persons with dementia through the course of the disease: An exploratory, cross-sectional study. BMC Geriatr. 2016, 16, 32. [Google Scholar] [CrossRef]
- Dai, Y.; Zhao, J.; Li, S.; Zhao, C.; Gao, Y.; Johnson, C.E. Caregivers’ Dementia Knowledge and Care Approach in Residential Aged Care Facilities in China. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 1533317520937096. [Google Scholar] [CrossRef]
- Zhao, W.; Jones, C.; Wu, M.W.; Moyle, W. Healthcare professionals’ dementia knowledge and attitudes towards dementia care and family carers’ perceptions of dementia care in China: An integrative review. J. Clin. Nurs. 2022, 31, 1753–1775. [Google Scholar] [CrossRef]
- Romero-Mas, M.; Gómez-Zúñiga, B.; Cox, A.M.; Ramon-Aribau, A. Designing virtual communities of practice for informal caregivers of Alzheimer’s patients: An integrative review. Health Inform. J. 2020, 26, 2976–2991. [Google Scholar] [CrossRef]
- Zheng, W.; Zhao, C.; Liu, Z.; Wang, F. Research and Application of Collaborative Knowledge Building Model Based on Web2.0. In Proceedings of the 2009 First International Workshop on Education Technology and Computer Science, Wuhan, China, 7–8 March 2009; pp. 39–43. [Google Scholar]
- Lave, J.; Wenger, E. Situated Learning: Legitimate Peripheral Participation; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar] [CrossRef]
- Moen, P.J. Teachers’ Perspectives on a Virtual Community of Practice Professional Development Model; Northcentral University, Northcentral University ProQuest Dissertations Publishing: Scottsdale, AZ, USA, 2016. [Google Scholar]
- Haas, A.; Abonneau, D.; Borzillo, S.; Guillaume, L.P. Afraid of engagement? Towards an understanding of engagement in virtual communities of practice. Knowl. Manag. Res. Pract. 2021, 19, 169–180. [Google Scholar] [CrossRef]
- Sedighi, M.; Lukosch, S.; van Splunter, S.; Brazier, F.M.T.; Hamedi, M.; van Beers, C. Employees’ participation in electronic networks of practice within a corporate group: Perceived benefits and costs. Knowl. Manag. Res. Pract. 2017, 15, 460–470. [Google Scholar] [CrossRef]
- Jarke, J. Community by Template? Considering the Role of Templates for Enacting Membership in Digital Communities of Practice. In Community and Identity in Contemporary Technosciences; Kastenhofer, K., Molyneux-Hodgson, S., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 183–204. [Google Scholar]
- Babajani-Vafsi, S.; Mokhtari Nouri, J.; Ebadi, A.; Zolfaghari, M. Factors Influencing the Participation of Nurses in Knowledge-Sharing within Mobile Instant Messaging Based Virtual Communities of Practice: A Qualitative Content Analysis. Adv. Med. Educ. Pract. 2019, 10, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Grosik, S.; Kanno, Y. Peripheral or marginal participation? J. Int. Stud. 2021, 11, 914–931. [Google Scholar] [CrossRef]
- Commission, E. Long-term care in ageing societies—Challenges and policy options. In Social Investment Package. Commission Staff Working Document; Archive of European Integration (AEI): Brussels, Belgium, 2013. [Google Scholar]
- Toledo-Chávarri, A.; Ramos-García, V.; Koatz, D.; Torres-Castaño, A.; Perestelo-Pérez, L.; Ramírez-Puerta, A.B.; Tello-Bernabé, M.E.; García-García, J.M.; García-García, J.; Pacheco-Huergo, V.; et al. Co-Design Process of a Virtual Community of Practice for the Empowerment of People with Ischemic Heart Disease. Int. J. Integr. Care 2020, 20, 9. [Google Scholar] [CrossRef]
- Ziglio, E.; Azzopardi-Muscat, N.; Briguglio, L. Resilience and 21st century public health. Eur. J. Public Health 2017, 27, 789–790. [Google Scholar] [CrossRef] [PubMed]
- Hopia, H.; Heikkilä, J. Nursing research priorities based on CINAHL database: A scoping review. Nurs. Open 2020, 7, 483–494. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Libraries, U.O.A. Getting Started with PsycINFO. Available online: https://uark.libguides.com/psycinfo (accessed on 9 January 2023).
- Manca, A.; Moher, D.; Cugusi, L.; Dvir, Z.; Deriu, F. How predatory journals leak into PubMed. CMAJ Can. Med. Assoc. J. 2018, 190, E1042–E1045. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Lund, C. Covidence. Available online: https://www.covidence.org/ (accessed on 9 January 2023).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Schmidt, U.; Frewer, A.; Sprumont, D. Ethical Research: The Declaration of Helsinki, and the Past, Present, and Future of Human Experimentation; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research: Appraising Evidence for Nursing Practice; Wolters Kluwer: Philadelphia, PA, USA, 2022. [Google Scholar]
- Vergnes, J.N.; Marchal-Sixou, C.; Nabet, C.; Maret, D.; Hamel, O. Ethics in systematic reviews. J. Med. Ethics 2010, 36, 771. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, P. Caregivers’ Experience of Caring for a Family Member with Alzheimer’s Disease: A Content Analysis of Longitudinal Social Media Communication. Int. J. Environ. Res. Public Health 2020, 17, 4412. [Google Scholar] [CrossRef] [PubMed]
- Efthymiou, A.; Middleton, N.; Charalambous, A.; Papastavrou, E. Health literacy and eHealth literacy and their association with other caring concepts among carers of people with dementia: A descriptive correlational study. Health Soc. Care Community 2022, 30, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- Fauth, E.B.; Novak, J.R.; Levin, M.E. Outcomes from a pilot online Acceptance and Commitment Therapy program for dementia family caregivers. Aging Ment. Health 2022, 26, 1620–1629. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.C.; Kovaleva, M.; Higgins, M.; Langston, A.H.; Hepburn, K. Tele-Savvy: An Online Program for Dementia Caregivers. Am. J. Alzheimer’s Dis. Other Dement.® 2018, 33, 269–276. [Google Scholar] [CrossRef]
- Kajiyama, B.; Fernandez, G.; Carter, E.A.; Humber, M.B.; Thompson, L.W. Helping Hispanic Dementia Caregivers Cope with Stress Using Technology-based Resources. Clin. Gerontol. 2018, 41, 209–216. [Google Scholar] [CrossRef]
- Madden, G.; Rose, T.; Crystal, L. Using video consultations to support family carers of people living with dementia. Nurs. Older People 2022, 34, 28–33. [Google Scholar] [CrossRef]
- Poole, M.; Davis, N.; Robinson, L. Massive Open Online Courses: Enhancing caregiver education and support about dementia care towards and at end of life. Age Ageing 2019, 49, 171–174. [Google Scholar] [CrossRef]
- Romero-Mas, M.; Ramon-Aribau, A.; Souza, D.L.B.D.; Cox, A.M.; Gómez-Zúñiga, B. Improving the Quality of Life of Family Caregivers of People with Alzheimer’s Disease through Virtual Communities of Practice: A Quasiexperimental Study. Int. J. Alzheimer’s Dis. 2021, 2021, 8817491. [Google Scholar] [CrossRef]
- Anderson, J.G.; Hundt, E.; Dean, M.; Keim-Malpass, J.; Lopez, R.P. “The Church of Online Support”: Examining the Use of Blogs among Family Caregivers of Persons with Dementia. J. Fam. Nurs. 2017, 23, 34–54. [Google Scholar] [CrossRef]
- Wilkerson, D.A.; Brady, E.; Yi, E.H.; Bateman, D.R. Friendsourcing Peer Support for Alzheimer’s Caregivers Using Facebook Social Media. J. Technol. Hum. Serv. 2018, 36, 105–124. [Google Scholar] [CrossRef]
- Valaitis, R.K.; Akhtar-Danesh, N.; Brooks, F.; Binks, S.; Semogas, D. Online communities of practice as a communication resource for community health nurses working with homeless persons. J. Adv. Nurs. 2011, 67, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Bolisani, E.; Fedeli, M.; De Marchi, V.; Bierema, L. Together we win: Communities of practice to face the COVID crisis in higher education. In Proceedings of the 17th International Conference on Intellectual Capital, Knowledge Management & Organisational Learning ICICKM, Toronto, ON, Canada, 15–16 October 2020. [Google Scholar]
- Jones, G.; Miesen, B. Care-Giving in Dementia: Volume 2; Routledge: London, UK, 2021. [Google Scholar]
- Mastel-Smith, B.; Kimzey, M.; Garner, J.; Shoair, O.A.; Stocks, E.; Wallace, T. Dementia care boot camp: Interprofessional education for healthcare students. J. Interprof. Care 2020, 34, 799–811. [Google Scholar] [CrossRef]
- Dhawan, S. Online Learning: A Panacea in the Time of COVID-19 Crisis. J. Educ. Technol. Syst. 2020, 49, 5–22. [Google Scholar] [CrossRef]
- Hassan, A.Y.I. Challenges and Recommendations for the Deployment of Information and Communication Technology Solutions for Informal Caregivers: Scoping Review. JMIR Aging 2020, 3, e20310. [Google Scholar] [CrossRef]
- Parkinson, M.; Carr, S.M.; Rushmer, R.; Abley, C. Investigating what works to support family carers of people with dementia: A rapid realist review. J. Public Health 2016, 39, e290–e301. [Google Scholar] [CrossRef] [PubMed]
- Hepburn, K.W.; Lewis, M.; Sherman, C.W.; Tornatore, J. The Savvy Caregiver Program: Developing and Testing a Transportable Dementia Family Caregiver Training Program. Gerontologist 2003, 43, 908–915. [Google Scholar] [CrossRef]
- United Nations, UN. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, USA, 2015; Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 5 February 2023).
- European Commission, EC. Horizon Europe Strategic Plan 2021–2024; Publications Office of the European Union: Luxembourg, 2021; p. 101. Available online: https://www.eeas.europa.eu/sites/default/files/horizon_europe_strategic_plan_2021-2024.pdf (accessed on 5 February 2023).
- Europe Parliament; European Commission; Council of Europe. European Pillar of Social Rights—Building a Fairer and More Inclusive European Union; European Commission: Brussels, Belgium; Available online: https://commission.europa.eu/strategy-and-policy/priorities-2019-2024/economy-works-people/jobs-growth-and-investment/european-pillar-social-rights/european-pillar-social-rights-20-principles_en (accessed on 5 February 2023).
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. JBI Evid. Implement. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed]

| Author, Year, Country | Aim(s), Design, Sample Population and Ethics | Study Context and Concept | Results |
|---|---|---|---|
| Anderson et al. (2017) [28], Utah, USA | Aim: The study explored how family caregivers of PwD use the social media platform (blogs) as part of the individual caregiving experience. Design: Qualitative descriptive content analysis Sample population: Family caregivers. Sample size: 10 blog sites Ethics: Yes | Context: Social media blog genre “the church of online support”. Concept: Social media blog genre on dementia caregiving experience. | The social media blog genre content analysis showed family caregivers used blogs as platform: for engaging and communicating with others: “…a place to update people…”; to seek and disseminate information; to record caregiving experience, decline of disease, etc.;“ …to document [for] whatever purpose...”; “…as a way of contributing to society…“; and “…to write notes so that later down the road I can write a manual or a book and donate the proceeds.” |
| Bachmann (2020) [29], USA, the UK and Canada | Aim: To examine the nature of the caregiver’s work, its mental and physical demands, experience and questions, and the relationship between the persons with Alzheimer’s dementia (AD), the caregiver, and family members. Design: A content analysis of longitudinal social media communication. Population: Persons with Alzheimer’s dementia, family caregivers, care professionals. Sample size: 28 Ethics: Yes | Context: Facebook social networking site. Concept: Facebook post on Basic Activity of Daily Living (BADLs) and Instrument Activity of Daily Living (IADLs) support information from persons with Alzheimer’s dementia, family caregivers, care professionals. | Discussion posts from patients included: self-feeding, healthcare and well-being, e.g., taking prescribed medication; positive effects of entertainment, e.g., watching movie, listening to music, etc.; transferring/moving in the community; managing money; shopping; preparing meal; getting help from family members; sleeping disorders; appointments, e.g., tests and surgeries; caregivers and facility selection; ageing, death, and dying. Others include engagements in interpersonal communication between caregivers and persons with Alzheimer’s dementia; religious observance, holiday, or birthday anniversary; social groups and other public events; care of pets; and safety procedures and emergency response. Discussion post from family caregivers and care professionals included: exhaustion and feeling of giving up; changes in health state of a patient caregivers success and positive feeling; violent behavior; financial issues. |
| Efthymiou et al. (2021) [30], Greece and Cyprus | Aim: Identify the levels of Health Literacy (HL) and eHealth Literacy (eHL) among carers of person with dementia in Greece and Cyprus, and to search for the associations with other caring concepts. Design: Descriptive correlational. Sample population: Informal carers of persons with dementia. Sample size: 241 Ethics: Yes. | Context: Face to face Internet survey platform. Concept: Care-giving self-efficacy, coping strategies, care-giving perceptions, and social support. | Higher score on eHeals-Carer “information seeking” was related with higher use of emotion-focused strategies, care-giving self-efficacy, and lower score of problematic/dysfunctional coping. Primary informal carers reported a high level of HL and eHL. Carers with higher HL were more likely to report higher score of eHL. |
| Fauth et al. (2021) [31], USA | Aim: To evaluate a pilot Acceptance Commitment Therapy (ACT) for caregivers program, a community-based, self-guided, online adaptation of ACT. Design: Pre/post-test and four week follow-up. Population: Family caregivers. Sample size: 160 Ethics: Yes | Context: An online dementia education library. Concept: Online ACT for family caregivers on evaluating depressive symptoms, burden, stressful reactions to Behavioral and Psychological Symptoms of Dementia (BPSD), positive aspects of caregiving, and quality of life. | Online ACT showed decreased depressive symptoms, burden, and stress reactions to behavioral symptoms, and increased positive aspects of caregiving and quality of life. ACT-specific measures improved, with decreases in cognitive function and psychological inflexibility, and improvements in living according to personal values, i.e., valuing progress increased; valuing obstruction decreased. |
| Griffiths et al. (2018) [32], USA | Aim: Assessment of caregiver burden, caregiver competency, and frequency of Behavioral and Psychological Symptoms of Dementia (BPSD). Design: Six weeks pre/post-test. Sample population: Dementia caregivers. Sample size: 22 Ethics: Yes. | Context: Online Tele-Savvy caregiver program. Concept: Psychoeducation program on caregiver burden, caregiver competency, and frequency BPSD. | Contributed significantly to reductions in caregiver burden and depressive symptoms, a significant increase in caregiver competence, and significant reductions in the average number of BPSD and the BPSD that occur daily or more. |
| Kajiyama et al. (2018) [33] South America | Aim: Develop and evaluate a culturally appropriate intervention for Hispanic/Latino caregivers of persons with dementia using a structured online program Design: Six weeks pre/post-test Sample population: Dementia caregivers. Sample size: 25 Ethics: Yes | Context: Webnovela Mirela, an online Spanish Telenovela program. Concept: Webnovela Mirela, an online Spanish Telenovela psychoeducation program to teach caregivers coping with dementia caregiving. | Significant decrease in levels of stress and symptoms of depression among dementia caregivers. Technology enables support programs to reach a broader audience in a cost-effective manner. |
| Madden et al. (2022) [34], the UK | Aim: To increase the accessibility and efficiency of care support for families affected by dementia. Design: Participatory action research Sample population: Family caregivers Sample size: 52 Ethics: Not applicable | Context: Online video consultations Concept: Video consultation to increase access and efficiency of care support for family caregivers | Video consultations enable carers to put face to voice, focus, and connected compared to using a telephone conversation, which made them felt disconnected and unfocused. Care professionals were anxious when discussing during video consultation, due to absence of physical contact, which often served as prompts, sustained their discussions, and encouraged disclosure. Lack of facial contact led to feeling helpless and disempowerment. Inability to use therapeutic touch. Challenges to change from one task to another with video consultation. The situation was described as firefighting and confusing; frequent changes occurred regarding personal and professional info and guidelines; expressed disappointment for the initiated video consultation not being offered routinely for its innovative nature. |
| Poole (2020) [35], the UK | Aim: To provide accessible sources of relevant and engaging information to family carers, and to enable carers to create a space in which they could engage in peer support. Design: Cross-sectional design. Sample population: Family caregivers, care pro-fessional. Sample size: 36 Ethics: Yes. | Context: Massive Open Online Courses Survey (MOOCs). Concept: Online resource for educational and support need for family caregivers and care professionals. | The MOOC survey showed that over 90% of learners reported acquiring new skills and knowledge. Over two-thirds and three-quarters applied knowledge acquired in their daily lives and shared what they have learned with others. The peer support element enhanced learner interactions, as well as the course content, e.g., comparing experiences; offering guidance; suggesting solutions; exchanging hints and tips; providing encouragement and condolences; and empathizing with each other. The ‘safe space’ section also provided encouragement for the sharing of personal feelings regarding sensitive matters, e.g., grieving process, however, posts from participants largely influence the course content managed by the course educator to control inappropriate posts. Although developed for family caregivers, it has seen the likes of persons with dementia and care professionals advancing their knowledge in dementia care and progression. |
| Romero-Mas et al. (2021) [36], Spain | Aim: Describe the relation between QoL of the family caregivers of a person with Alzheimer’s disease, and their participation in a virtual community of practice (vCoP). Design: Pre/post-test quasi-experimental. Sample population: Family caregivers and health professionals Sample size: 38 with 1 drop out. Ethics: Yes. | Context: The application “Estic amb tu - I’m with you” Concept: Online social support network to evaluate QoL of family caregiver’s participation in vCoP | The application “Estic amb tu - I’m with you” showed that caregivers improve their QoL while participating in a vCoP. There was no significant difference in QoL among male and female, except for their age demographic parameter. The authors noted a negative correlation between “length of caring” and psychological and social domain of QoL. There was a difference between the relationship with the person with Alzheimer’s (spouse, offspring, and others), and overall QoL was improved through vCoP, except for the spouse parameter. Family caregivers found meaning in providing care to a loved one, feeling more useful, gaining new skills, and experience. There was no correlation between the functional deterioration of the person with Alzheimer and caregivers’ QoL. eHealth literacy impacted positively on the physical domain of the caregivers’ QoL. |
| Wilkerson et al. (2018) [37] USA | Aim: The study introduced Friendsourcing Web application (FPS) and examines the effects on the psychological well-being of AD caregivers. Design: Pre/post test Sample population: AD caregivers Sample size: 12 Ethics: Yes | Context: Friendsourcing Web application Concept: AD caregivers discussion on emotional and informational support via Friendsourcing Web application | A Wilcoxon signed-rank test showed that caregiving burden and perceived stress while emotional and informational support significantly reduced and increased, respectively. Subjective interviews and discussions identified: caregiving belief experience, cognitive transformation, and new behaviors learned (seeking and trying new caregiving ways/roles and applying them) from Facebook social network described as ‘’FPS’’ to reduce burden and perceived stress. |
| Themes | Subthemes |
|---|---|
| Knowledge acquisition |
|
| Strengthening resilience capacity |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dedzoe, J.D.-S.; Malmgren Fänge, A.; Christensen, J.; Lethin, C. Collaborative Learning through a Virtual Community of Practice in Dementia Care Support: A Scoping Review. Healthcare 2023, 11, 692. https://doi.org/10.3390/healthcare11050692
Dedzoe JD-S, Malmgren Fänge A, Christensen J, Lethin C. Collaborative Learning through a Virtual Community of Practice in Dementia Care Support: A Scoping Review. Healthcare. 2023; 11(5):692. https://doi.org/10.3390/healthcare11050692
Chicago/Turabian StyleDedzoe, Justice Dey-Seshie, Agneta Malmgren Fänge, Jonas Christensen, and Connie Lethin. 2023. "Collaborative Learning through a Virtual Community of Practice in Dementia Care Support: A Scoping Review" Healthcare 11, no. 5: 692. https://doi.org/10.3390/healthcare11050692
APA StyleDedzoe, J. D.-S., Malmgren Fänge, A., Christensen, J., & Lethin, C. (2023). Collaborative Learning through a Virtual Community of Practice in Dementia Care Support: A Scoping Review. Healthcare, 11(5), 692. https://doi.org/10.3390/healthcare11050692