Cytokine Levels and Severity of Illness Scoring Systems to Predict Mortality in COVID-19 Infection

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Patient Groups
2.4. Statistical Analysis
3. Results
4. Discussion
5. Strength and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://covid19.who.int/ (accessed on 8 October 2022).
- Bottle, A.; Faitna, P.; Brett, S.; Aylin, P. Factors associated with, and variations in, COVID-19 hospital death rates in England’s first two waves: Observational study. BMJ Open 2022, 12, e060251. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://covid19.saglik.gov.tr/ (accessed on 8 October 2022).
- Capalbo, C.; Aceti, A.; Simmaco, M.; Bonfini, R.; Rocco, M.; Ricci, A.; Napoli, C.; Rocco, M.; Alfonsi, V.; Teggi, A.; et al. The Exponential Phase of the COVID-19 Pandemic in Central Italy: An Integrated Care Pathway. Int. J. Environ. Res. Public Health 2020, 17, 3792. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, S.; Sharma, K.; Silakari, O. The interplay between inflammatory pathways and COVID-19: A critical review on pathogenesis and therapeutic options. Microb. Pathog. 2020, 150, 104673. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhao, T.; Zhou, X.; Xiang, Y.; Gutierrez-Castrellon, P.; Ma, X. Inflammatory pathways in COVID-19: Mechanism and therapeutic interventions. MedComm 2022, 3, e154. [Google Scholar] [CrossRef]
- Presti, E.L.; Nuzzo, D.; Al Mahmeed, W.; Al-Rasadi, K.; Al-Alawi, K.; Banach, M.; Banerjee, Y.; Ceriello, A.; Cesur, M.; Cosentino, F.; et al. Molecular and pro-inflammatory aspects of COVID-19: The impact on cardiometabolic health. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2022, 1868, 166559. [Google Scholar] [CrossRef]
- Tanveer, A.; Akhtar, B.; Sharif, A.; Saleem, U.; Rasul, A.; Ahmad, A.; Jilani, K. Pathogenic role of cytokines in COVID-19, its association with contributing co-morbidities and possible therapeutic regimens. Inflammopharmacology 2022, 30, 1503–1516. [Google Scholar] [CrossRef]
- Furci, F.; Murdaca, G.; Allegra, A.; Gammeri, L.; Senna, G.; Gangemi, S. IL-33 and the Cytokine Storm in COVID-19: From a Potential Immunological Relationship towards Precision Medicine. Int. J. Mol. Sci. 2022, 23, 14532. [Google Scholar] [CrossRef]
- El Kazafy, S.A.; Fouad, Y.M.; Said, A.F.; Assal, H.H.; Ahmed, A.E.; El Askary, A.; Ali, T.M.; Ahmed, O.M. Relation between Cytokine Levels and Pulmonary Dysfunction in COVID-19 Patients: A Case-Control Study. J. Pers. Med. 2023, 13, 34. [Google Scholar] [CrossRef]
- Casas-Aparicio, G.; Alvarado-de la Barrera, C.; Escamilla-Illescas, D.; León-Rodríguez, I.; Del Río-Estrada, P.M.; González-Navarro, M.; Calderón-Dávila, N.; Olmedo-Ocampo, R.; Castillejos-López, M.; Figueroa-Hernández, L.; et al. Longitudinal Analysis of Urinary Cytokines and Biomarkers in COVID-19 Patients with Subclinical Acute Kidney Injury. Int. J. Mol. Sci. 2022, 23, 15419. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Available online: https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci#use-cases (accessed on 8 October 2022).
- Suidan, R.S.; Leitao, M.M.; Zivanovic, O.; Gardner, G.J.; Roche, K.C.L.; Sonoda, Y.; Levine, D.A.; Jewell, E.L.; Brown, C.L.; Abu-Rustum, N.R.; et al. Predictive value of the Age-Adjusted Charlson Comorbidity Index on perioperative complications and survival in patients undergoing primary debulking surgery for advanced epithelial ovarian cancer. Gynecol. Oncol. 2015, 138, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-C.; Chen, P.-C.; Hsu, C.-W.; Chang, S.-L.; Lee, C.-C. Validity of the age-adjusted charlson comorbidity index on clinical outcomes for patients with nasopharyngeal cancer post radiation treatment: A 5-year nationwide cohort study. PLoS ONE 2015, 10, e0117323. [Google Scholar] [CrossRef]
- Robbins, J.R.; Gayar, O.H.; Zaki, M.; Mahan, M.; Buekers, T.; Elshaikh, M.A. Impact of Age-Adjusted Charlson Comorbidity score on outcomes for patients with early-stage endometrial cancer. Gynecol. Oncol. 2013, 131, 593–597. [Google Scholar] [CrossRef]
- Bhatti, K.M.; Hamzah, B.; Rehman, S.; Birkett, E.; Langford, W.; Aung, M.; Canelo, R. Novel Use Of Age-Adjusted Charlson Comorbidity Index (ACCI) As A Risk Stratification Tool For Development Of Postoperative SARS-CoV-2 Infection In Surgical Patients. J. Ayub. Med. Coll. Abbottabad. 2021, 33, 622–627. [Google Scholar] [PubMed]
- Nuevo-Ortega, P.; Reina-Artacho, C.; Dominguez-Moreno, F.; Becerra-Muñoz, V.M.; Ruiz-Del-Fresno, L.; Estecha-Foncea, M.A.; Aguilar-Galvez, A.M.; Barrera-Serrano, R.; Cabrera-Cesar, E.; Castillo-Caballero, J.M.; et al. Prognosis of COVID-19 pneumonia can be early predicted combining Age-adjusted Charlson Comorbidity Index, CRB score and baseline oxygen saturation. Sci. Rep. 2022, 12, 2367. [Google Scholar] [CrossRef] [PubMed]
- Baris, S.A.; Boyaci, H.; Akhan, S.; Mutlu, B.; Deniz, M.; Basyigit, I. Charlson Comorbidity Index in Predicting Poor Clinical Outcomes and Mortality in Patients with COVID-19. Turk. Thorac. J. 2022, 23, 145–153. [Google Scholar] [CrossRef]
- Akman, C.; Bardakçı, O.; Daş, M.; Akdur, G. The Effectiveness of National Early Warning Score, Quick Sequential Organ Failure Assessment, Charlson Comorbidity Index, and Elixhauser Comorbidity Index Scores in Predicting Mortality Due to COVID-19 in Elderly Patients. Cureus 2022, 14, e23012. [Google Scholar] [CrossRef]
- Comoglu, S. Does the Charlson comorbidity index help predict the risk of death in COVID-19 patients? North. Clin. Istanb. 2022, 9, 117–121. [Google Scholar] [CrossRef]
- Ayvat, P.; Omeroglu, S.K. Mortality estimation using APACHE and CT scores with stepwise linear regression method in COVID-19 intensive care unit: A retrospective study. Clin. Imaging 2022, 88, 4–8. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Amoozadeh, L.; Motlagh, F.R.; Rahimi, M.; Maghsoudloo, M.; Jafarnejad, B.; Eslami, B.; Salehi, M.R.; Zendehdel, K. Mortality Predictive Value of APACHE II and SOFA Scores in COVID-19 Patients in the Intensive Care Unit. Can. Respir. J. 2022, 2022, 5129314. [Google Scholar] [CrossRef]
- Ejaz, T.; Rehman, F.; Ahmed, A.; Akhlaq, S.; Saadia, S.; Aziz, A.; Hussain, E. Clinical Characteristics and Outcomes of COVID-19 Acute Respiratory Distress Syndrome Patients Requiring Invasive Mechanical Ventilation in a Lower Middle-Income Country. J. Crit. Care Med. 2022, 8, 23–32. [Google Scholar] [CrossRef]
- Shang, Y.; Liu, T.; Wei, Y.; Li, J.; Shao, L.; Liu, M.; Zhang, Y.; Zhao, Z.; Xu, H.; Peng, Z.; et al. Scoring systems for predicting mortality for severe patients with COVID-19. EClinicalMedicine 2020, 24, 100426. [Google Scholar] [CrossRef]
- Cho, S.Y.; Park, S.S.; Song, M.K.; Bae, Y.Y.; Lee, D.G.; Kim, D.W. Prognosis Score System to Predict Survival for COVID-19 Cases: A Korean Nationwide Cohort Study. J. Med. Internet Res. 2021, 23, e26257. [Google Scholar] [CrossRef] [PubMed]
- Mureșan, A.V.; Hălmaciu, I.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Budișcă, O.A.; Melinte, R.M.; Vunvulea, V.; Filep, R.C.; Mărginean, L.; et al. Prognostic Nutritional Index, Controlling Nutritional Status (CONUT) Score, and Inflammatory Biomarkers as Predictors of Deep Vein Thrombosis, Acute Pulmonary Embolism, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2757. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, D.; Hou, J.; Li, H.; Cao, D.; Guo, M.; Ling, Y.; Gao, M.; Zhou, Y.; Wan, Y.; et al. An inter-correlated cytokine network identified at the center of cytokine storm predicted COVID-19 prognosis. Cytokine 2020, 138, 155365. [Google Scholar] [CrossRef]
- Cabaro, S.; D’Esposito, V.; Di Matola, T.; Sale, S.; Cennamo, M.; Terracciano, D.; Parisi, V.; Oriente, F.; Portella, G.; Beguinot, F.; et al. Cytokine signature and COVID-19 prediction models in the two waves of pandemics. Sci. Rep. 2021, 11, 20793. [Google Scholar] [CrossRef]
- Jafrin, S.; Aziz, M.A.; Islam, M.S. Elevated Levels of Pleiotropic Interleukin-6 (IL-6) and Interleukin-10 (IL-10) Are Critically Involved With the Severity and Mortality of COVID-19: An Updated Longitudinal Meta-Analysis and Systematic Review on 147 Studies. Biomark. Insights 2022, 17, 11772719221106600. [Google Scholar] [CrossRef]
- Guo, J.; Wang, S.; Xia, H.; Shi, D.; Chen, Y.; Zheng, S.; Chen, Y.; Gao, H.; Guo, F.; Ji, Z.; et al. Cytokine Signature Associated with Disease Severity in COVID-19. Front. Immunol. 2021, 12, 681516. [Google Scholar] [CrossRef]
- Pons, M.J.; Ymaña, B.; Mayanga-Herrera, A.; Sáenz, Y.; Alvarez-Erviti, L.; Tapia-Rojas, S.; Gamarra, R.; Blanco, A.B.; Moncunill, G.; Ugarte-Gil, M.F. Cytokine Profiles Associated with Worse Prognosis in a Hospitalized Peruvian COVID-19 Cohort. Front. Immunol. 2021, 12, 700921. [Google Scholar] [CrossRef]
- Tang, Y.; Sun, J.; Pan, H.; Yao, F.; Yuan, Y.; Zeng, M.; Ye, G.; Yang, G.; Zheng, B.; Fan, J.; et al. Aberrant cytokine expression in COVID-19 patients: Associations between cytokines and disease severity. Cytokine 2021, 143, 155523. [Google Scholar] [CrossRef]
- Ozsurekci, Y.; Aykac, K.; Er, A.G.; Halacli, B.; Arasli, M.; Oygar, P.D.; Gürlevik, S.; Yayla, B.C.C.; Karakaya, J.; Alp, A.; et al. Predictive value of cytokine/chemokine responses for the disease severity and management in children and adult cases with COVID-19. J. Med. Virol. 2021, 93, 2828–2837. [Google Scholar] [CrossRef]
- Liu, Y.; Tan, W.; Chen, H.; Zhu, Y.; Wan, L.; Jiang, K.; Guo, Y.; Tang, K.; Xie, C.; Yi, H.; et al. Dynamic changes in lymphocyte subsets and parallel cytokine levels in patients with severe and critical COVID-19. BMC Infect. Dis. 2021, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Fara, A.; Mitrev, Z.; Rosalia, R.A.; Assas, B.M. Cytokine storm and COVID-19: A chronicle of pro-inflammatory cytokines. Open Biol. 2020, 10, 200160. [Google Scholar] [CrossRef]
- Milenkovic, M.; Hadzibegovic, A.; Kovac, M.; Jovanovic, B.; Stanisavljevic, J.; Djikic, M.; Sijan, D.; Ladjevic, N.; Palibrk, I.; Djukanovic, M.; et al. D-dimer, CRP, PCT, and IL-6 levels at admission to ICU can predict in-hospital mortality in patients with COVID-19 pneumonia. Oxid. Med. Cell. Longev. 2022, 2022, 8997709. [Google Scholar] [CrossRef] [PubMed]
- Ozger, H.S.; Karakus, R.; Kuscu, E.N.; Bagriacik, U.E.; Oruklu, N.; Yaman, M.; Turkoglu, M.; Erbas, G.; Atak, A.Y.; Senol, E. Serial measurement of cytokines strongly predict COVID-19 outcome. PLoS ONE 2021, 16, e0260623. [Google Scholar] [CrossRef] [PubMed]
- Gou, X.; Ying, J.; Yue, Y.; Qiu, X.; Hu, P.; Qu, Y.; Li, J.; Mu, D. The Roles of High Mobility Group Box 1 in Cerebral Ischemic Injury. Front. Cell. Neurosci. 2020, 14, 600280. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Alkazmi, L.; Habotta, O.A.; Batiha, G.E.-S. High-mobility group box 1 (HMGB1) in COVID-19: Extrapolation of dangerous liaisons. Inflammopharmacology 2022, 30, 811–820. [Google Scholar] [CrossRef]
- Chen, L.; Long, X.; Xu, Q.; Tan, J.; Wang, G.; Cao, Y.; Wei, J.; Luo, H.; Zhu, H.; Huang, L.; et al. Elevated serum levels of S100A8/A9 and HMGB1 at hospital admission are correlated with inferior clinical outcomes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 992–994. [Google Scholar] [CrossRef]
- Sivakorn, C.; Dechsanga, J.; Jamjumrus, L.; Boonnak, K.; Schultz, M.J.; Dorndorp, A.M.; Phumratanaprapin, W.; Ratanarat, R.; Naorungroj, T.; Wattanawinitchai, P.; et al. High Mobility Group Box 1 and Interleukin 6 at Intensive Care Unit Admission as Biomarkers in Critically Ill COVID-19 Patients. Am. J. Trop. Med. Hyg. 2021, 105, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Topcu, H.; Arik, Y. The Importance of D-Dimer, Ferritin, CRP and Lymphocyte Values in Determining Mortality in COVID-19 Disease in Turkey. Clin. Lab. 2022, 68, 2274–2280. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.; Pranata, R.; Lim, M.A.; Oehadian, A.; Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: A meta-analysis. Ther. Adv. Respir. Dis. 2020, 14, 1753466620937175. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Marte, M.; Massetti, A.P.; Carli, S.M.; Romano, F.; Mastroianni, C.M.; Minorenti, M.; Alessandri, F.; Ajassa, C.; Fusconi, M.; et al. COVID-Collaborative group. The neutrophil/lymphocyte ratio as a prognostic factor in COVID-19 patients: A case-control study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1056–1064. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Halmaciu, I.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Suciu, B.A.; Coșarcă, C.M.; Cojocaru, I.I.; Melinte, R.M.; Russu, E. Systemic Inflammatory Biomarkers and Chest CT Findings as Predictors of Acute Limb Ischemia Risk, Intensive Care Unit Admission, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2379. [Google Scholar] [CrossRef]
- Rehatta, N.M.; Chandra, S.; Sari, D.; Lestari, M.I.; Senapathi, T.G.A.; Nurdin, H.; Wirabuana, B.; Pramodana, B.; Pradhana, A.P.; Isngadi, I.; et al. Comorbidities and COVID-19 status influence the survival rate of geriatric patients in intensive care units: A prospective cohort study from the Indonesian Society of Anaesthesiology and Intensive Therapy. BMC Geriatr. 2022, 22, 523. [Google Scholar] [CrossRef]
- Yıldız, B.; Erden, S.; Öz, A.; Karabağ, T. The Relationship of Comorbidities with Intensive Care Unit Admission and Mortality in Patients with COVID-19. Turk. J. Anaesthesiol. Reanim. 2022, 50, 187–193. [Google Scholar] [CrossRef]
- Türker, B.C.; Türker, F.; Ahbab, S.; Hoca, E.; Urvasızoğlu, A.O.; Cetin, S.I.; Ataoğlu, H.E. Evaluation of the Charlson Comorbidity Index and Laboratory Parameters as Independent Early Mortality Predictors in COVID-19 Patients. Int. J. Gen. Med. 2022, 15, 6301–6307. [Google Scholar] [CrossRef]
- Kumar, M.; Behera, A.; Singh, P.; Shaji, A.; Ghosh, A.; Bhatia, M.; Singla, N.; Singh, M.P. Severe Acute Respiratory Infection Surveillance during the Initial Phase of the COVID-19 Outbreak in North India: A Comparison of COVID-19 to Other SARI Causes. Indian J. Crit. Care Med. 2021, 25, 761–767. [Google Scholar] [CrossRef]
- Vandenbrande, J.; Verbrugge, L.; Bruckers, L.; Geebelen, L.; Geerts, E.; Callebaut, I.; Gruyters, I.; Heremans, L.; Dubois, J.; Stessel, B. Validation of the Acute Physiology and Chronic Health Evaluation (APACHE) II and IV Score in COVID-19 Patients. Crit. Care Res. Pract. 2021, 2021, 5443083. [Google Scholar] [CrossRef]
- Taleb, S.; Yassine, H.M.; Benslimane, F.M.; Smatti, M.K.; Schuchardt, S.; Albagha, O.; Al-Thani, A.A.; Hssain, A.A.; Diboun, I.; Elrayess, M.A. Predictive Biomarkers of Intensive Care Unit and Mechanical Ventilation Duration in Critically-Ill Coronavirus Disease 2019 Patients. Front. Med. 2021, 8, 733657. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Wu, H.; Yang, J.; Song, X.; Xu, M.; Li, B.; Zhang, J.; Qin, M.; Zhou, C.; Zhou, X. Pneumonia scoring systems for severe COVID-19: Which one is better. Virol. J. 2021, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Xu, W.; Li, W.-X.; Huang, C.-L.; Chen, L. Dynamics of cytokines and lymphocyte subsets associated with the poor prognosis of severe COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12536–12544. [Google Scholar] [CrossRef] [PubMed]
- Nagant, C.; Ponthieux, F.; Smet, J.; Dauby, N.; Doyen, V.; Besse-Hammer, T.; De Bels, D.; Maillart, E.; Corazza, F. A score combining early detection of cytokines accurately predicts COVID-19 severity and intensive care unit transfer. Int. J. Infect. Dis. 2020, 101, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Jin, H.; Wen, Y.F.; Yin, G. Efficacy of COVID-19 Treatments: A Bayesian Network Meta-Analysis of Randomized Controlled Trials. Front. Public Health 2021, 9, 729559. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Groups | Test Statistics | |||
|---|---|---|---|---|
| Group A (Survived) n = 36 | Group B (Died) n = 27 | Test Value | p Value | |
| Age ± sd M (min–max) | 65.69 ± 13.56 64.5 (45.0–43.0) | 70.85 ± 10.06 73.0 (35.0–53.0) | t = 1.661 | 0.102 |
| Sex n (%) Female Male | 17 (73.9) 19 (47.5) | 6 (26.1) 21 (52.5) | χ2 = 4.160 | 0.064 |
| BMI ± sd | 26.94 ±4.50 | 28.12 ± 3.81 | t = 1.097 | 0.277 |
| Type 2 diabetes mellitus Absent Present | 22 (59.5) 14 (53.8) | 15 (40.5) 12 (46.2) | χ2 = 0.196 | 0.797 |
| Hypertension Absent Present | 18 (62.1) 18 (52.9) | 11 (37.9) 16 (47.1) | χ2 = 0.532 | 0.610 |
| Coronary artery disease Absent Present | 26 (55.3) 10 (62.5) | 21 (44.7) 6 (37.5) | χ2 = 0.251 | 0.772 |
| Cerebrovascular accident Absent Present | 32 (56.1) 4 (66.7) | 25 (43.9) 2 (33.3) | χ2 = 0.246 | 0.693 |
| Chronic pulmonary disease Absent Present | 29 (58.0) 7 (53.8) | 21 (42.0) 6 (46.2) | χ2 = 0.073 | >0.999 |
| Liver disease Absent Present | 36 (58.1) 0 (0.0) | 26 (41.9) 1 (100.0) | χ2 = 1.355 | 0.429 |
| APACHE II score M (IQR) | 10.0 (4.75) | 11.0 (9.0) | z = 1.689 | 0.091 |
| SOFA score M (IQR) | 4.0 (1.0) | 5.0 (3.0) | z = 1.217 | 0.224 |
| GCS score M (IQR) | 15.0 (2.0) | 15.0 (1.0) | z = 1.064 | 0.287 |
| Charlson comorbidity index score M (IQR) | 4.0 (2.75) | 4.0 (4.0) | z = 1.073 | 0.283 |
| AKI Absent Present | 31 (68.9) 5 (27.8) | 14 (31.1) 13 (72.2) | χ2 = 8.873 | 0.005 |
| Duration of hospitalization M (IQR) | 19.5 (16.75) | 15.0 (18.0) | z = 1.237 | 0.216 |
| Duration of ICU admission M (IQR) | 10.50 (8.0) | 11.0 (12.0) | z = 1.351 | 0.177 |
| Tocilizumab therapy Absent Present | 31 (58.5) 5 (50.0) | 22 (41.5) 5 (50.0) | χ2 = 0.248 | 0.733 |
| Dexamethasone therapy M (IQR) | 16.0 (8.0) | 16.0 (8.0) | z = 0.612 | 0.594 |
| Methylprednisolone therapy M (IQR) | 40.0 (40.0) | 60.0 (129) | z = 0.055 | >0.999 |
| Groups | Test Statistics | |||
|---|---|---|---|---|
| Group A (Survived) n = 36 M (IQR) | Group B (Died) n = 27 M (IQR) | z Value | p Value | |
| Lymphocyte | 0.77 (1.13) | 0.66 (0.52) | 0.896 | 0.370 |
| PMNL | 9.74 (8.31) | 8.79 (9.05) | 0.451 | 0.652 |
| NLR | 10.67 (14.50) | 15.50 (15.09) | 1.278 | 0.201 |
| Platelet | 242.50 (114.0) | 220.0 (105.0) | 1.111 | 0.266 |
| D-dimer | 1650.0 (2844.50) | 2230.0 (2716.0) | 0.354 | 0.723 |
| Fibrinogen | 5830.0 (3495.0) | 6650.0 (1560.0) | 1.375 | 0.169 |
| Ferritin | 459.50 (790.25) | 863.0 (1463.0) | 2.833 | 0.005 |
| LDH | 370.50 (305.5) | 553.0 (314.0) | 2.834 | 0.005 |
| GGT | 29.0 (30.32) | 39.0 (28.0) | 1.362 | 0.173 |
| CRP | 117.0 (156.02) | 96.0 (149.0) | 0.361 | 0.718 |
| Procalcitonin | 0.18 (0.86) | 0.55 (1.25) | 1.459 | 0.145 |
| Lactate | 1.45 (1.25) | 1.60 (1.0) | 0.612 | 0.540 |
| PaO2/FiO2 | 82.42 (139.50) | 71.42 (27.78) | 2.709 | 0.007 |
| IL-1β | 1093.50 (611.64) | 1312.70 (1114.86) | 2.236 | 0.025 |
| IL-6 | 94.15 (37.08) | 133.54 (120.94) | 2.479 | 0.013 |
| IL-8 | 198.39 (68.89) | 263.68 (272.36) | 2.660 | 0.008 |
| IL-10 | 212.36 (133.75) | 263.25 (364.76) | 2.222 | 0.026 |
| TNF-α | 154.43 (69.52) | 193.85 (182.10) | 2.868 | 0.004 |
| HMGB-1 | 20.99 (9.68) | 26.0 (20.65) | 2.201 | 0.028 |
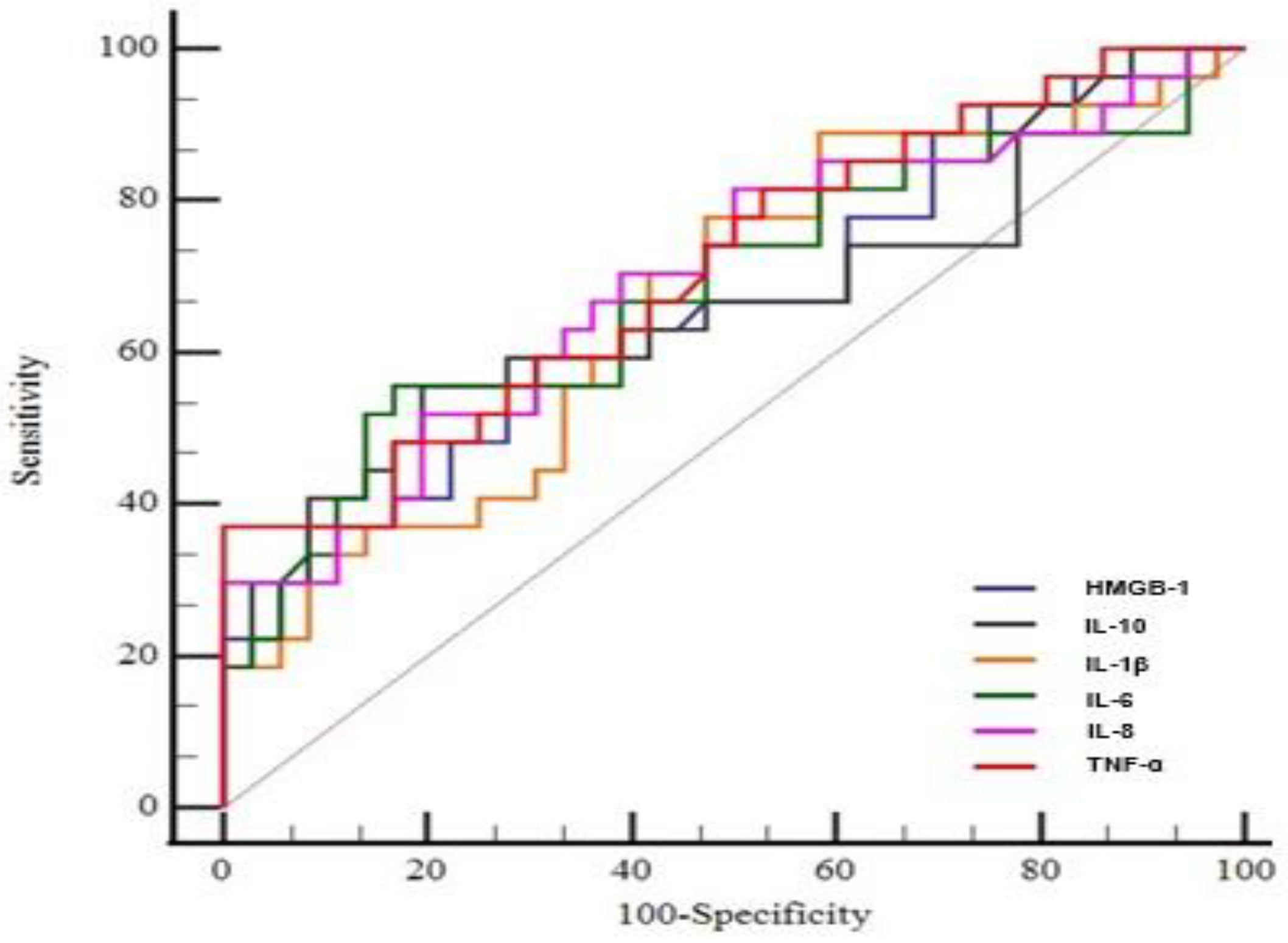
| AUC (%95 CI) | p Value | Cut-Off | Sensitivity (%95 CI) | Specificity (%95 CI) | |
|---|---|---|---|---|---|
| TNF-α | 0.712 (0.585–0.820) | 0.001 | >280.7 | 37.0 (19.4–57.4) | 100.0 (90.3–100.0) |
| IL-8 | 0.697 (0.568–0.807) | 0.004 | >258.4 | 51.8 (31.9–71.4) | 80.5 (64.0–91.8) |
| IL-6 | 0.684 (0.554–0.795) | 0.010 | >116.7 | 55.5 (35.3–74.5) | 83.3 (67.2–93.6) |
| IL-1β | 0.666 (0.536–0.780) | 0.018 | >1015.7 | 88.8 (70.8–97.6) | 41.6 (25.5–59.2) |
| IL-10 | 0.665 (0.534–0.779) | 0.024 | >247.5 | 55.5 (35.3–74.5) | 80.5 (64.0–91.8) |
| HMGB-1 | 0.663 (0.533–0.777) | 0.021 | >23.5 | 59.2 (38.8–77.6) | 69.4 (51.9–83.7) |
| Regression Coefficients | ||||
|---|---|---|---|---|
| p | Odds Ratio | 95% CI | ||
| Lower | Upper | |||
| Constant | 0.001 | 0.016 | ||
| AKI | 0.014 | 7.081 | 1.482 | 33.834 |
| IL-1β | 0.016 | 1.005 | 1.001 | 1.009 |
| TNF-α | 0.004 | 1.047 | 1.015 | 1.080 |
| Ferritin | 0.016 | 1.001 | 1.000 | 1.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onuk, S.; Sipahioğlu, H.; Karahan, S.; Yeşiltepe, A.; Kuzugüden, S.; Karabulut, A.; Beştepe Dursun, Z.; Akın, A. Cytokine Levels and Severity of Illness Scoring Systems to Predict Mortality in COVID-19 Infection. Healthcare 2023, 11, 387. https://doi.org/10.3390/healthcare11030387
Onuk S, Sipahioğlu H, Karahan S, Yeşiltepe A, Kuzugüden S, Karabulut A, Beştepe Dursun Z, Akın A. Cytokine Levels and Severity of Illness Scoring Systems to Predict Mortality in COVID-19 Infection. Healthcare. 2023; 11(3):387. https://doi.org/10.3390/healthcare11030387
Chicago/Turabian StyleOnuk, Sevda, Hilal Sipahioğlu, Samet Karahan, Ali Yeşiltepe, Sibel Kuzugüden, Aycan Karabulut, Zehra Beştepe Dursun, and Aynur Akın. 2023. "Cytokine Levels and Severity of Illness Scoring Systems to Predict Mortality in COVID-19 Infection" Healthcare 11, no. 3: 387. https://doi.org/10.3390/healthcare11030387
APA StyleOnuk, S., Sipahioğlu, H., Karahan, S., Yeşiltepe, A., Kuzugüden, S., Karabulut, A., Beştepe Dursun, Z., & Akın, A. (2023). Cytokine Levels and Severity of Illness Scoring Systems to Predict Mortality in COVID-19 Infection. Healthcare, 11(3), 387. https://doi.org/10.3390/healthcare11030387