
Health, Stress and Technologies: Integrating Technology Acceptance and Health Belief Models for Smartphone-Based Stress Intervention

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
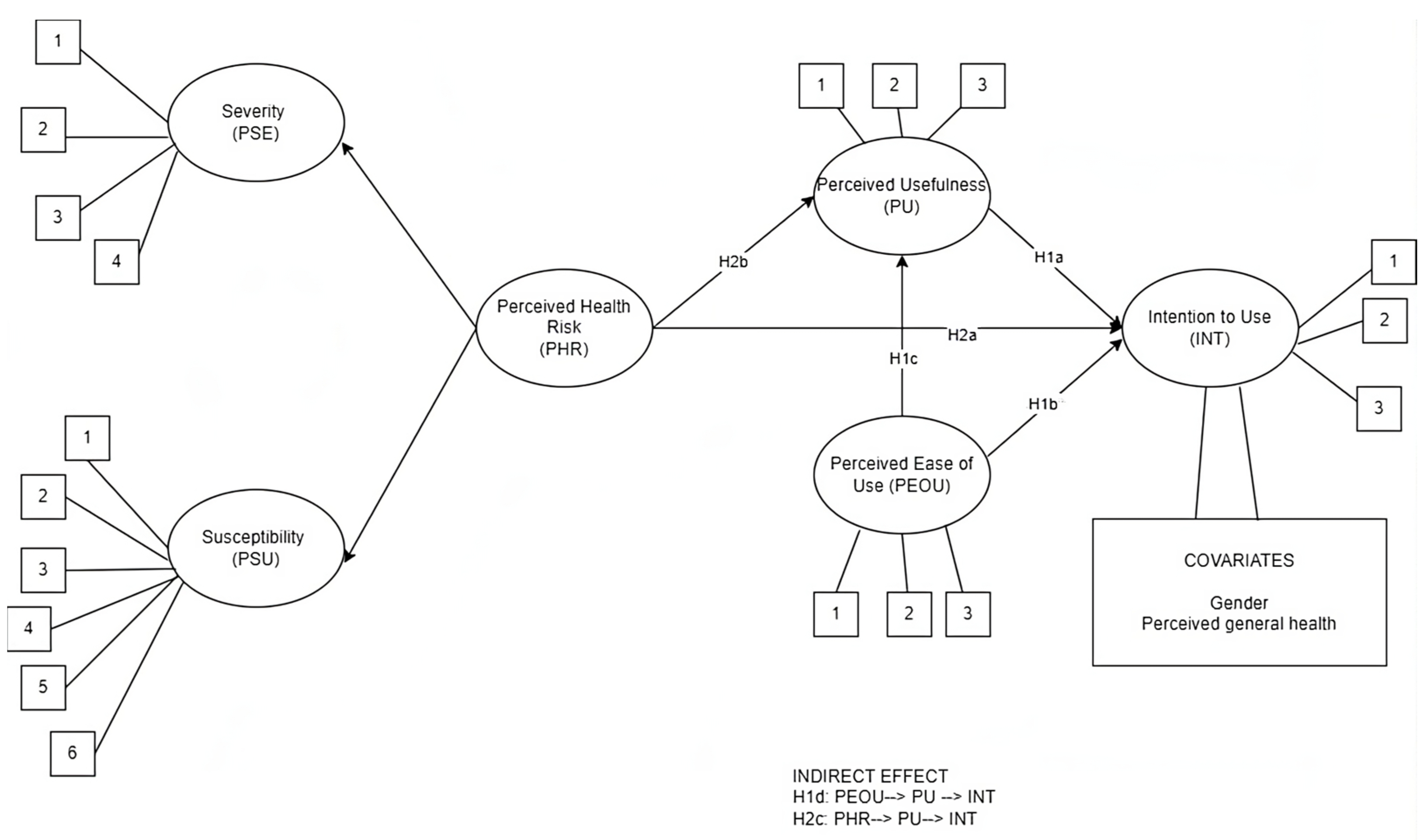
2. Theoretical Background and Hypothesis Development
2.1. Smartphone-Based Interventions for Stress Management
2.2. Technology Acceptance
2.3. Integrating TAM and HBM
3. Materials and Methods
3.1. Context and Participants
3.2. Measures
3.3. Data Analysis
4. Results
4.1. Descriptive Statistics
4.2. Confirmatory Factor Analysis (CFA)
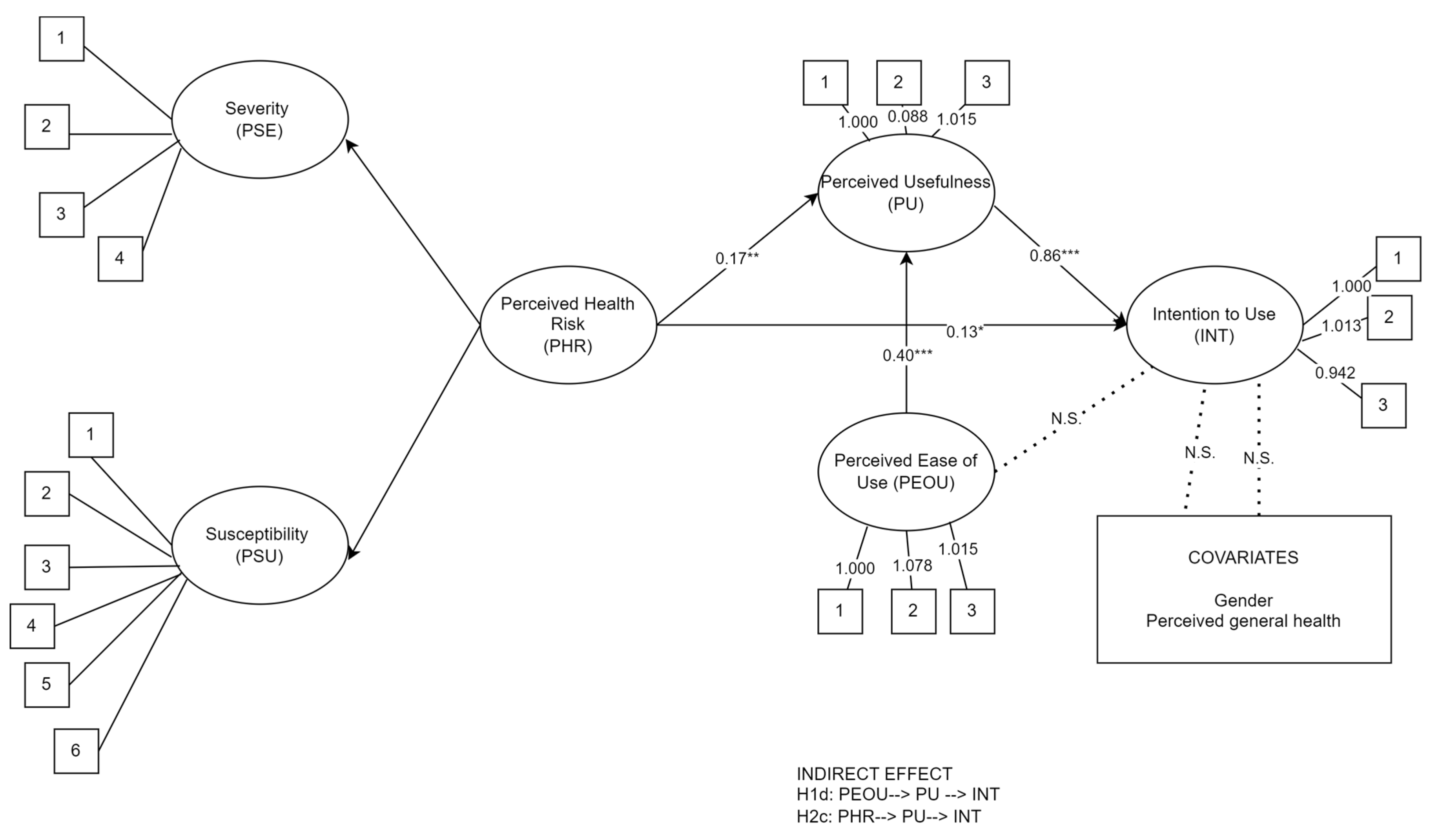
4.3. Direct Effects
4.4. Mediation Analysis
5. Discussion
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hassard, J.; Teoh, K.R.H.; Visockaite, G.; Dewe, P.; Cox, T. The Cost of Work-Related Stress to Society: A Systematic Review. J. Occup. Health Psychol. 2018, 23, 1–17. [Google Scholar] [CrossRef] [PubMed]
- de Neve, J.; Diener, E.; Tay, L.; Xuereb, C. The Objective Benefits of Subjective Well-Being. In CEP Discussion Paper No 1236; Centre for Economic Performance: London, UK, 2013. [Google Scholar]
- Holman, D.; Johnson, S.; O’ Connor, E. Stress Management Interventions: Improving Subjective Psychological Well-Being in the Workplace; The University of Manchester: Manchester, UK, 2018. [Google Scholar]
- Sucharitha, M.M.; Basha, S.A. A Study on Impact of Stress on Employee’s Productivity and Job Performance: Implications for Stress Measurement and Management. İlköğretim Online 2020, 19, 823–831. [Google Scholar]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of EHealth Interventions for Reducing Mental Health Conditions in Employees: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef]
- Apraiz, A.; Lasa, G.; Montagna, F.; Blandino, G.; Triviño-Tonato, E.; Dacal-Nieto, A. An Experimental Protocol for Human Stress Investigation in Manufacturing Contexts: Its Application in the NO-STRESS Project. Systems 2023, 11, 448. [Google Scholar] [CrossRef]
- de Korte, E.; Wiezer, N.; Roozeboom, M.B.; Vink, P.; Kraaij, W. Behavior Change Techniques in Mhealth Apps for the Mental and Physical Health of Employees: Systematic Assessment. JMIR mHealth uHealth 2018, 6, e167. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Bergin, M.; Chalder, T.; Wells, J.S.G. Web-Based Interventions for the Management of Stress in the Workplace: Focus, Form, and Efficacy. J. Occup. Health 2017, 59, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Taherdoost, H. A Review of Technology Acceptance and Adoption Models and Theories. Procedia Manuf. 2019, 22, 960–967. [Google Scholar] [CrossRef]
- Tong, X. A Cross-National Investigation of an Extended Technology Acceptance Model in the Online Shopping Context. Int. J. Retail. Distrib. Manag. 2010, 38, 742–759. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–339. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Behav. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Dederichs, M.; Weber, J.; Pischke, C.R.; Angerer, P.; Apolinário-Hagen, J. Exploring Medical Students’ Views on Digital Mental Health Interventions: A Qualitative Study. Internet Interv. 2021, 25, 100398. [Google Scholar] [CrossRef] [PubMed]
- Bakhuys Roozeboom, M.; Schelvis, R.; Houtman, I.; Wiezer, N.; Bongers, P. Decreasing Employees’ Work Stress by a Participatory, Organizational Level Work Stress Prevention Approach: A Multiple-Case Study in Primary Education. BMC Public Health 2020, 20, 676. [Google Scholar] [CrossRef] [PubMed]
- Toh, S.Y.; Ng, S.A.; Phoon, S.T. Accentuating Technology Acceptance among Academicians: A Conservation of Resource Perspective in the Malaysian Context. Educ. Inf. Technol. 2023, 28, 2529–2545. [Google Scholar] [CrossRef] [PubMed]
- De Korte, E.M.; Wiezer, N.; Janssen, J.H.; Vink, P.; Kraaij, W. Evaluating an MHealth App for Health and Well-Being at Work: Mixed-Method Qualitative Study. J. Med. Internet Res. 2018, 20, e6335. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, P.; Bregenzer, A. Integration of EHealth Tools in the Process of Workplace Health Promotion: Proposal for Design and Implementation. J. Med. Internet Res. 2018, 20, e65. [Google Scholar] [CrossRef] [PubMed]
- Carissoli, C.; Villani, D.; Riva, G. Does a Meditation Protocol Supported by a Mobile Application Help People Reduce Stress? Suggestions from a Controlled Pragmatic Trial. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Deady, M.; Johnston, D.; Milne, D.; Glozier, N.; Peters, D.; Calvo, R.; Harvey, S. Preliminary Effectiveness of a Smartphone App to Reduce Depressive Symptoms in the Workplace: Feasibility and Acceptability Study. JMIR mHealth uHealth 2018, 6, e11661. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.; Jayawardana, M.W.; Muir, S.D.; Ho, D.Y.T.; Sackett, O. Promoting Psychological Well-Being at Work by Reducing Stress and Improving Sleep: Mixed-Methods Analysis. J. Med. Internet Res. 2018, 20, e267. [Google Scholar] [CrossRef]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and Promoting Effective Engagement With Digital Behavior Change Interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef]
- Bidargaddi, N.; Almirall, D.; Murphy, S.; Nahum-Shani, I.; Kovalcik, M.; Pituch, T.; Maaieh, H.; Strecher, V. To Prompt or Not to Prompt? A Microrandomized Trial of Time-Varying Push Notifications to Increase Proximal Engagement with a Mobile Health App. JMIR mHealth uHealth 2018, 6, e10123. [Google Scholar] [CrossRef]
- Venkatesh, V. Determinants of Perceived Ease of Use: Integrating Control, Intrinsic Motivation, and Emotion into the Technology Acceptance Model. Inf. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef]
- Marangunić, N.; Granić, A. Technology Acceptance Model: A Literature Review from 1986 to 2013. Univers. Access Inf. Soc. 2015, 14, 81–95. [Google Scholar] [CrossRef]
- Taherdoost, H. Importance of Technology Acceptance Assessment for Successful Implementation and Development of New Technologies. Glob. J. Eng. Sci. 2019, 1. [Google Scholar] [CrossRef]
- Svendsen, G.B.; Johnsen, J.A.K.; Almås-Sørensen, L.; Vittersø, J. Personality and Technology Acceptance: The Influence of Personality Factors on the Core Constructs of the Technology Acceptance Model. Behav. Inf. Technol. 2013, 32, 323–334. [Google Scholar] [CrossRef]
- Champion, V.; Skinner, C. The Health Belief Model. In Health Behavior and Health Education; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 45–65. [Google Scholar]
- Ross, T.P.; Ross, L.T.; Rahman, A.; Cataldo, S. The Bicycle Helmet Attitudes Scale: Using the Health Belief Model to Predict Helmet Use among Undergraduates. J. Am. Coll. Health 2010, 59, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Ploubidis, G.B.; George, L.A. Climate Change and Climate Variability: Personal Motivation for Adaptation and Mitigation. Env. Health 2011, 10, 46. [Google Scholar] [CrossRef] [PubMed]
- Ahadzadeh, A.S.; Pahlevan Sharif, S.; Ong, F.S.; Khong, K.W. Integrating Health Belief Model and Technology Acceptance Model: An Investigation of Health-Related Internet Use. J. Med. Internet Res. 2015, 17, e45. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H.; Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, T.; Barnoy, S. Assessment of the Intention to Use Mobile Health Applications Using a Technology Acceptance Model in an Israeli Adult Population. Telemed. e-Health 2020, 26, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Purwanto, E.; Budiman, V. Applying the Technology Acceptance Model to Investigate the Intention to Use E-Health: A Conceptual Framework. Technol. Rep. Kansai Univ. 2020, 62, 2569–2580. [Google Scholar]
- Walrave, M.; Waeterloos, C.; Ponnet, K. Adoption of a Contact Tracing App for Containing COVID-19: A Health Belief Model Approach. JMIR Public Health Surveill. 2020, 6, e20572. [Google Scholar] [CrossRef] [PubMed]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an Effective Health Interventions Design: An Extension of the Health Belief Model. Online J. Public Health Inf. 2012, 4, e9. [Google Scholar] [CrossRef] [PubMed]
- Mathieson, K. Predicting User Intentions: Comparing the Technology Acceptance Model with the Theory of Planned Behavior. Inf. Syst. Res. 1991, 2, 173–191. [Google Scholar] [CrossRef]
- Chuttur, M. Overview of the Technology Acceptance Model: Origins, Developments and Future Directions. Sprouts Work. Pap. Inf. Syst. 2009, 9, 3169–3177. [Google Scholar] [CrossRef]
- Yun, E.K. Development and Testing of a Model of Consumer’s Health Information Seeking Behavior on the Internet. Ph.D. Thesis, Seoul National University, Seoul, Republic of Korea, 2008. [Google Scholar]
- Fishbein, M. Attitude and the Prediction of Behaviour. In Readings in Attitude Theory and Measurement; Wiley: Hoboken, NJ, USA, 1967. [Google Scholar]
- Ajzen, I.; Cote, N.G. Attitudes and the Prediction of Behavior. In Attitudes and Attitude Change; Psychology Press: London, UK, 2011. [Google Scholar]
- Kim, J.; Park, H.A. Development of a Health Information Technology Acceptance Model Using Consumers’ Health Behavior Intention. J. Med. Internet Res. 2012, 14, e133. [Google Scholar] [CrossRef] [PubMed]
- Melzner, J.; Heinze, J.; Fritsch, T. Mobile Health Applications in Workplace Health Promotion: An Integrated Conceptual Adoption Framework. Procedia Technol. 2014, 16, 1374–1382. [Google Scholar] [CrossRef]
- Paganin, G.; Simbula, S. New Technologies in the Workplace: Can Personal and Organizational Variables Affect the Employees’ Intention to Use a Work-Stress Management App? Int. J. Env. Res. Public Health 2021, 18, 9366. [Google Scholar] [CrossRef] [PubMed]
- Gabbiadini, A.; Paganin, G.; Simbula, S. Teaching after the Pandemic: The Role of Technostress and Organizational Support on Intentions to Adopt Remote Teaching Technologies. Acta Psychol. 2023, 236, 103936. [Google Scholar] [CrossRef]
- Paganin, G.; Apolinário-Hagen, J.; Simbula, S. Introducing Mobile Apps to Promote the Well-Being of German and Italian University Students. A Cross-National Application of the Technology Acceptance Model. Curr. Psychol. 2022. [Google Scholar] [CrossRef]
- Bryan, A.D.; Aiken, L.S.; West, S.G. Young Women’s Condom Use: The Influence of Acceptance of Sexuality, Control over the Sexual Encounter, and Perceived Susceptibility to Common STDs. Health Psychol. 1997, 16, 468–479. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. Answers to Selected Exercises. In SPSS for Windows Step by Step: A Simple Guide and Reference, 4th ed.; 11.0 Update; Allyn & Bacon: Boston, MA, USA, 2003; p. 63. [Google Scholar]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: Thousands Oaks, CA, USA, 2016. [Google Scholar]
- Carolan, S.; De Visser, R.O. Employees’ Perspectives on the Facilitators and Barriers to Engaging with Digital Mental Health Interventions in the Workplace: Qualitative Study. J. Med. Internet Res. 2018, 5, e9146. [Google Scholar] [CrossRef] [PubMed]
- Egger, S.M.; Frey, S.; Sauerzopf, L.; Meidert, U. A Literature Review to Identify Effective Web- and App-Based MHealth Interventions for Stress Management at Work. Work. Health Saf. 2023, 71, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Rick, V.B.; Rasche, P.; Mertens, A.; Nitsch, V. Workplace Health Promotion: MHealth as a Preventive Mediator between Psychosocial Workplace Characteristics and Well-Being at Work. In Proceedings of the Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Health, Operations Management, and Design, Virtual, 26 June–1 July 2022. [Google Scholar]
- Paganin, G.; Simbula, S. Smartphone-Based Interventions for Employees’ Well-Being Promotion: A Systematic Review. Electron. J. Appl. Stat. Anal. 2020, 13, 682–712. [Google Scholar] [CrossRef]
- Deng, Z. Understanding Public Users’ Adoption of Mobile Health Service. Int. J. Mob. Commun. 2013, 11, 351. [Google Scholar] [CrossRef]
- Tsai, C.H. The Adoption of a Telehealth System: The Integration of Extended Technology Acceptance Model and Health Belief Model. J. Med. Imaging Health Inf. 2014, 4, 448–455. [Google Scholar] [CrossRef]
- Abd-alrazaq, A.A.; Bewick, B.M.; Farragher, T.; Gardner, P. Factors That Affect the Use of Electronic Personal Health Records among Patients: A Systematic Review. Int. J. Med. Inform. 2019, 126, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Askari, M.; Klaver, N.S.; van Gestel, T.J.; van de Klundert, J. Intention to Use Medical Apps among Older Adults in the Netherlands: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e18080. [Google Scholar] [CrossRef]
- Beldad, A.D.; Hegner, S.M. Expanding the Technology Acceptance Model with the Inclusion of Trust, Social Influence, and Health Valuation to Determine the Predictors of German Users’ Willingness to Continue Using a Fitness App: A Structural Equation Modeling Approach. Int. J. Hum. Comput. Interact. 2018, 34, 882–893. [Google Scholar] [CrossRef]
- Palos-Sanchez, P.R.; Saura, J.R.; Martin, M.Á.R.; Aguayo-Camacho, M. Toward a Better Understanding of the Intention to Use Mhealth Apps: Exploratory Study. JMIR mHealth uHealth 2021, 9, e27021. [Google Scholar] [CrossRef]
- Jung, M.-L.; Loria, K. Acceptance of Swedish E-Health Services. J. Multidiscip. Health 2010, 3, 55–63. [Google Scholar] [CrossRef]
- Junker, M.; Böhm, M.; Franz, M.; Fritsch, T.; Krcmar, H. Value of Normative Belief in Intention to Use Workplace Health Promotion Apps. BMC Med. Inf. Decis. Mak. 2022, 22, 30. [Google Scholar] [CrossRef] [PubMed]
- Champion, V.L. Instrument Development for Health Belief Model Constructs. ANS Adv. Nurs. Sci. 1984, 6, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Hassard, J.; Cox, T.; Murawski, S.; De Meyer, S.; Muylaert, K. Mental Health Promotion in the Workplace—A Good Practice Report. In Working Environment Information Working Paper; European Agency for Safety & Health at Work: Bilbao, Spain, 2011; ISBN 9789291914890. [Google Scholar]
- Wahyuni, R. Nurbojatmiko Explaining Acceptance of E-Health Services: An Extension of TAM and Health Belief Model Approach. In Proceedings of the 2017 5th International Conference on Cyber and IT Service Management (CITSM), Denpasar, Indonesia, 8–10 August 2017. [Google Scholar]
- Fraboni, F.; Paganin, G.; Mazzetti, G.; Guglielmi, D.; Pietrantoni, L. The Intricate Pathways From Empowering Leadership to Burnout: A Deep Dive Into Interpersonal Conflicts, Work-Home Interactions, and Supportive Colleagues. Informing Sci. Int. J. Emerg. Transdiscipl. 2023, 26, 149–172. [Google Scholar] [CrossRef] [PubMed]
- Alsswey, A.; Al-Samarraie, H. Elderly Users’ Acceptance of MHealth User Interface (UI) Design-Based Culture: The Moderator Role of Age. J. Multimodal. User Interfaces 2020, 14, 49–59. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| r | ||||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | |
| 2.96 | 0.77 | 0.89 | |||||
| 3.67 | 0.73 | 0.46 *** | 0.94 | ||||
| 3.05 | 0.85 | 0.72 *** | 0.44 *** | 0.93 | |||
| 2.60 | 0.99 | 0.17 ** | 0.15 ** | 0.28 *** | 0.91 | ||
| 3.02 | 1.03 | 0.16 ** | 0.16 ** | 0.28 *** | 0.62 *** | 0.89 | |
| 0.14 * | 0.09 | 0.09 | 0.10 | 0.06 | |||
| −0.07 | −0.07 | 0.02 | 0.23 *** | 0.18 ** | 0.07 | ||
| Model | χ2 | df | p | RMSEA | SRMR | CFI | TLI | AIC | Comp. | Δ χ2 |
|---|---|---|---|---|---|---|---|---|---|---|
| One-factor model a | 3872.22 | 170 | 0.000 | 0.23 | 0.23 | 0.37 | 0.30 | 20,762.74 | ||
| Five-factor model b | 345.12 | 160 | 0.000 | 0.05 | 0.05 | 0.97 | 0.96 | 17,254.64 | M1–M2 | 3527.10 *** |
| Second-order model c | 101.52 | 48 | 0.000 | 0.05 | 0.03 | 0.98 | 0.97 | 10,193.67 | M2–M3 | 243.59 *** |
| Standardized Indirect Effects | Estimates | SE | 95% CI |
|---|---|---|---|
| PEOU → PU → INT | 0.30 *** | 0.05 | [0.23; 0.43] |
| PHR → PU → INT | 0.14 * | 0.05 | [0.04; 0.22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paganin, G.; Margheritti, S.; Farhane-Medina, N.Z.; Simbula, S.; Mazzetti, G. Health, Stress and Technologies: Integrating Technology Acceptance and Health Belief Models for Smartphone-Based Stress Intervention. Healthcare 2023, 11, 3030. https://doi.org/10.3390/healthcare11233030
Paganin G, Margheritti S, Farhane-Medina NZ, Simbula S, Mazzetti G. Health, Stress and Technologies: Integrating Technology Acceptance and Health Belief Models for Smartphone-Based Stress Intervention. Healthcare. 2023; 11(23):3030. https://doi.org/10.3390/healthcare11233030
Chicago/Turabian StylePaganin, Giulia, Simona Margheritti, Naima Z. Farhane-Medina, Silvia Simbula, and Greta Mazzetti. 2023. "Health, Stress and Technologies: Integrating Technology Acceptance and Health Belief Models for Smartphone-Based Stress Intervention" Healthcare 11, no. 23: 3030. https://doi.org/10.3390/healthcare11233030
APA StylePaganin, G., Margheritti, S., Farhane-Medina, N. Z., Simbula, S., & Mazzetti, G. (2023). Health, Stress and Technologies: Integrating Technology Acceptance and Health Belief Models for Smartphone-Based Stress Intervention. Healthcare, 11(23), 3030. https://doi.org/10.3390/healthcare11233030