
Factors, Barriers, and Recommendations Related to Mobile Health Acceptance among the Elderly in Saudi Arabia: A Qualitative Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Healthcare Technology Acceptance Model
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Participant Description
3.2. Thematic Analysis
3.2.1. Theme 1: Factors Affecting Intention to Use mHealth
- Sub-theme 1: role of demographics and health status
- Sub-theme 2: perceived usefulness
- Sub-theme 3: ease of use
- Sub-theme 4: role of social factors
- Sub-theme 5: facilitating conditions
- Sub-theme 6: attitude
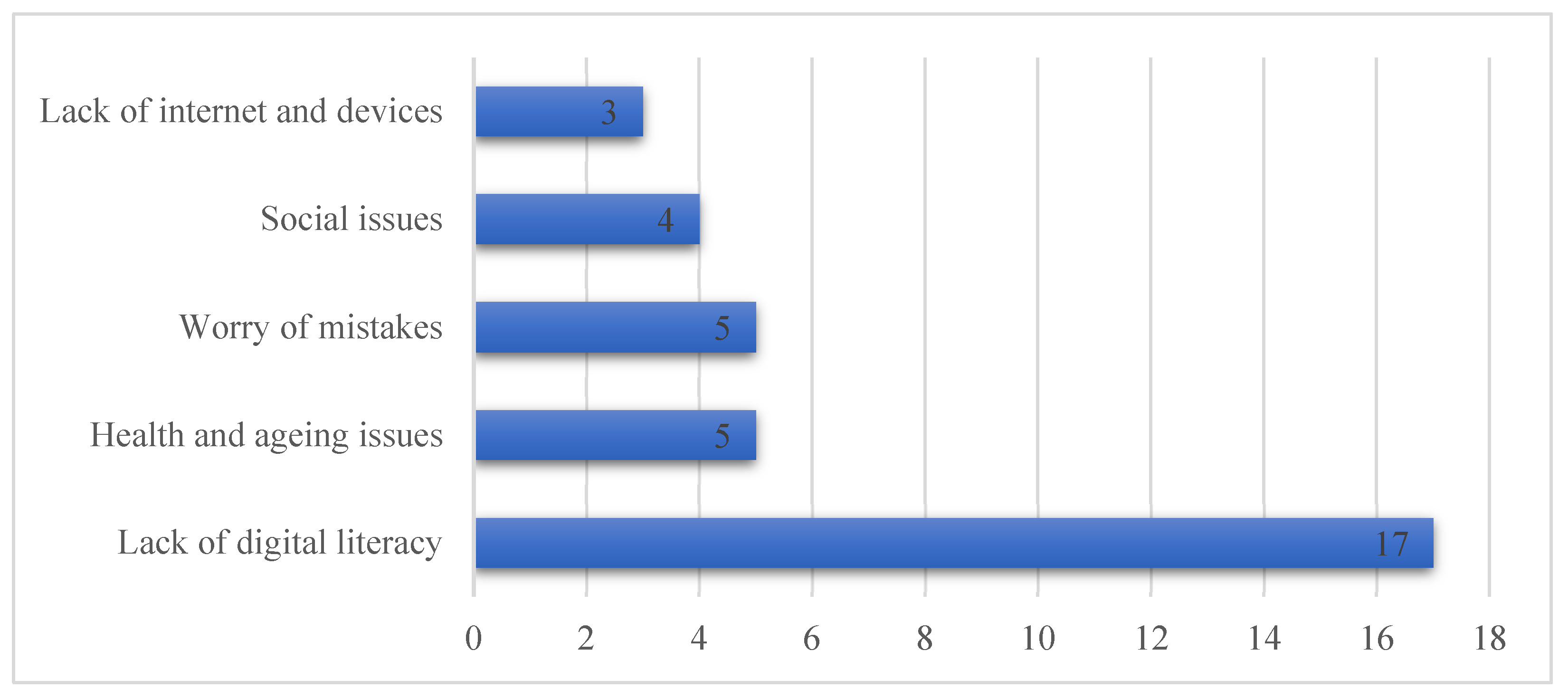
3.2.2. Theme 2: Concerns and Barriers
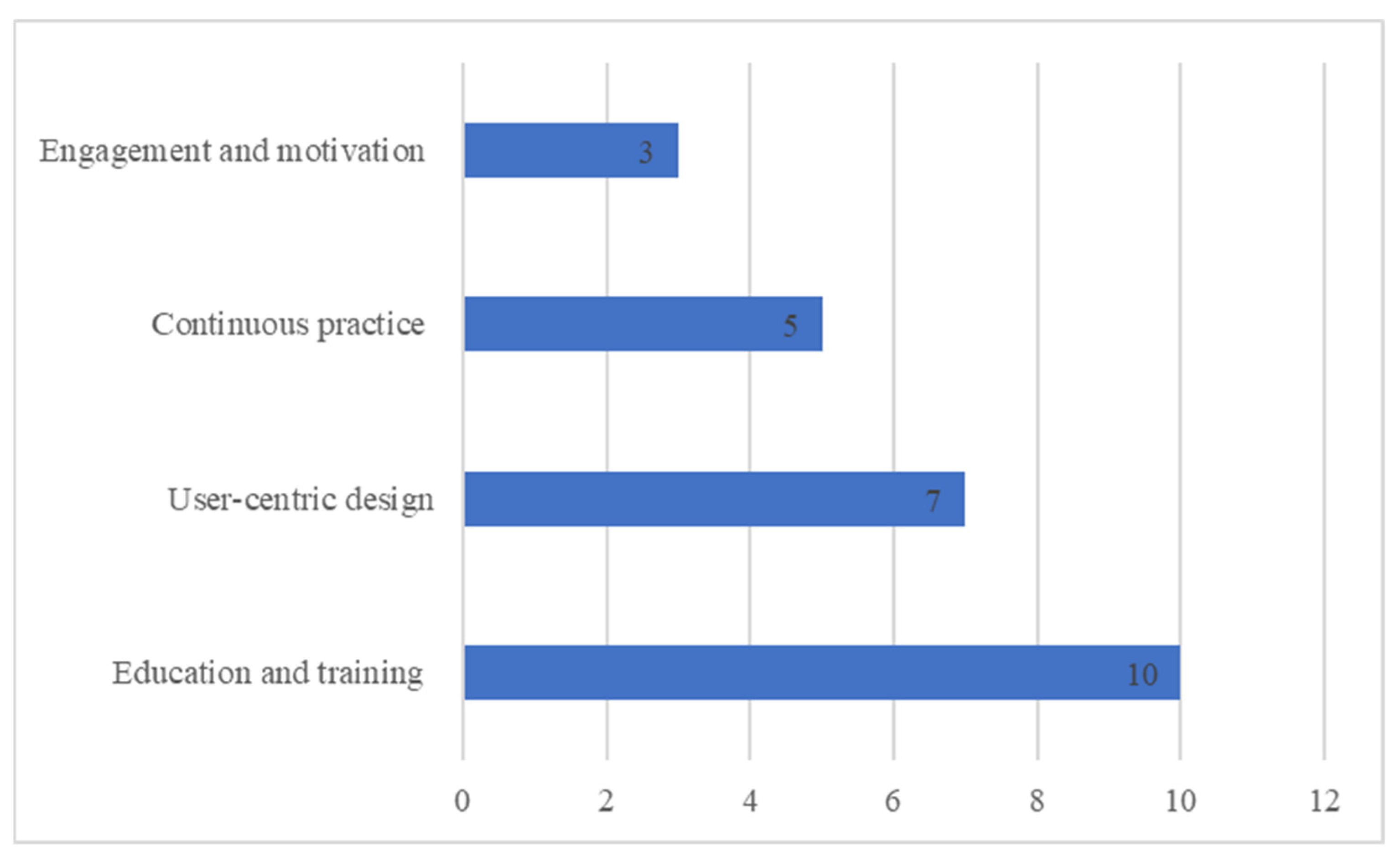
3.2.3. Theme 3: Solutions and Recommendations
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
Appendix A
References
- Wolrd Health Organization. Ageing and Health. WHO. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 3 August 2023).
- Ministry of Health. Health Days 2023—International Day of Older Persons. Available online: https://www.moh.gov.sa/en/HealthAwareness/healthDay/2023/Pages/HealthDay-2023-10-01-001.aspx (accessed on 17 May 2023).
- Al-Amoud, M.M.; Omar, D.I.; Almashjary, E.N.; Alomary, S.A. Morbidity profile among older people at primary health care centers in Saudi Arabia during the period 2012–2020. Saudi Med. J. 2023, 44, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.N. Population aging and health. BMJ 1997, 315, 1082–1084. [Google Scholar] [CrossRef] [PubMed]
- Pahlevanynejad, S.; Niakan Kalhori, S.R.; Katigari, M.R.; Eshpala, R.H. Personalized Mobile Health for Elderly Home Care: A Systematic Review of Benefits and Challenges. Int. J. Telemed. Appl. 2023, 2023, 5390712. [Google Scholar] [CrossRef]
- Chan, J. Exploring digital health care: eHealth, mHealth, and librarian opportunities. J. Med Libr. Assoc. 2021, 109, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Boren, S.A.; Khan, U.; Simoes, E.J.; Kim, M.S. Experience of diabetes self-management with mobile applications: A focus group study among older people with diabetes. Eur. J. Pers. Centered Healthc. 2018, 6, 262–273. [Google Scholar] [CrossRef]
- Frishammar, J.; Essén, A.; Bergström, F.; Ekman, T. Digital health platforms for the elderly? Key adoption and usage barriers and ways to address them. Technol. Forecast. Soc. Chang. 2023, 189, 122319. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. Manag. Inf. Syst. 1989, 13, 319–339. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.; Xu, X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. SSRN. MIS Q. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2002388 (accessed on 5 August 2023).
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Chen, K.; Chan, A.H.S. Gerontechnology acceptance by elderly Hong Kong Chinese: A senior technology acceptance model (STAM). Ergonomics 2014, 57, 635–652. [Google Scholar] [CrossRef]
- Harris, M.T.; Rogers, W.A. Developing a Healthcare Technology Acceptance Model (H-TAM) for Older Adults with Hypertension. Ageing Soc. 2023, 43, 814–834. [Google Scholar] [CrossRef]
- van Elburg, F.R.T.; Klaver, N.S.; Nieboer, A.P.; Askari, M. Gender differences regarding intention to use mHealth applications in the Dutch elderly population: A cross-sectional study. BMC Geriatr. 2022, 22, 449. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Q. The willingness to use mobile health and its influencing factors among elderly patients with chronic heart failure in Shanghai, China. Int. J. Med. Inform. 2022, 158, 104656. [Google Scholar] [CrossRef]
- Palas, J.U.; Sorwar, G.; Hoque, R.; Sivabalan, A. Factors influencing the elderly’s adoption of mHealth: An empirical study using extended UTAUT2 model. BMC Med. Inform. Decis. Mak. 2022, 22, 191. [Google Scholar] [CrossRef]
- Hassounah, M.; Raheel, H.; Alhefzi, M. Digital Response during the COVID-19 Pandemic in Saudi Arabia. J. Med. Internet Res. 2020, 22, e19338. [Google Scholar] [CrossRef]
- Health Sector Transformation Program—Vision 2030. Available online: https://www.vision2030.gov.sa/v2030/vrps/hstp/ (accessed on 17 May 2023).
- Alsahafi, Y.A.; Gay, V.; Khwaji, A.A. Factors affecting the acceptance of integrated electronic personal health records in Saudi Arabia: The impact of e-health literacy. Health Inf. Manag. J. 2020, 51, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Thapa, S.; Nielsen, J.B.; Aldahmash, A.M.; Qadri, F.R.; Leppin, A. Willingness to Use Digital Health Tools in Patient Care Among Health Care Professionals and Students at a University Hospital in Saudi Arabia: Quantitative Cross-sectional Survey. JMIR Med. Educ. 2021, 7, e18590. [Google Scholar] [CrossRef] [PubMed]
- Suri, H. Purposeful Sampling in Qualitative Research Synthesis Harsh Suri. Qual. Res. J. 2011, 11, 63–75. [Google Scholar] [CrossRef]
- Harris, M.T. Developing the Healthcare Technology Acceptance Model (H-TAM) for Older Adults; University of Illinois at Urbana-Champaign: Champaign, IL, USA, 2019. [Google Scholar]
- Kallio, H.; Pietilä, A.-M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016, 72, 2954–2965. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Sehhaty Platform. Available online: https://www.moh.gov.sa/en/eServices/Sehhaty/Pages/default.aspx (accessed on 6 August 2023).
- Johnson, J.L.; Adkins, D.; Chauvin, S. A Review of the Quality Indicators of Rigor in Qualitative Research. Am. J. Pharm. Educ. 2020, 84, 7120. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Dedoose. Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data. Available online: https://www.dedoose.com/ (accessed on 25 October 2023).
- Peek, S.T.M.; Luijkx, K.G.; Vrijhoef, H.J.M.; Nieboer, M.E.; Aarts, S.; van der Voort, C.S.; Rijnaard, M.D.; Wouters, E.J.M. Origins and consequences of technology acquirement by independent-living seniors: Towards an integrative model. BMC Geriatr. 2017, 17, 189. [Google Scholar] [CrossRef] [PubMed]
- The Communications, Space and TC. Saudi Internet Report 2022. Available online: https://www.cst.gov.sa/en/mediacenter/pressreleases/Pages/2023030802.aspx (accessed on 25 October 2023).
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Raja, M.; Bjerkan, J.; Kymre, I.G.; Galvin, K.T.; Uhrenfeldt, L. Telehealth and digital developments in society that persons 75 years and older in European countries have been part of: A scoping review. BMC Health Serv. Res. 2021, 21, 1157. [Google Scholar] [CrossRef]
- Maswadi, K.; Ghani, N.A.; Hamid, S. Factors influencing the elderly’s behavioural intention to use smart home technologies in Saudi Arabia. PLoS ONE 2022, 17, e0272525. [Google Scholar] [CrossRef]
- Calegari, L.P.; Tortorella, G.L.; Fettermann, D.C. Getting Connected to M-Health Technologies through a Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 4369. [Google Scholar] [CrossRef]
- van Hoof, J.; Demiris, G.; Wouters, E.J.M. (Eds.) Handbook of Smart Homes, Health Care and Well-Being; Springer International Publishing: Cham, Germany, 2017. [Google Scholar] [CrossRef]
- Alsswey, A.; Al-Samarraie, H. Elderly users’ acceptance of mHealth user interface (UI) design-based culture: The moderator role of age. J. Multimodal. User Interfaces 2020, 14, 49–59. [Google Scholar] [CrossRef]
- Khan, T.; Khan, K.D.; Azhar, M.S.; Shah, S.N.A.; Uddin, M.M.; Khan, T.H. Mobile health services and the elderly: Assessing the determinants of technology adoption readiness in Pakistan. J. Public Aff. 2021, 22, e2685. [Google Scholar] [CrossRef]
- General Authority for Statistics. The Elderly in the Kingdom of Saudi Arabia in 2019. Available online: https://www.stats.gov.sa/sites/default/files/repport_compressed_1_0.pdf (accessed on 25 October 2023).
- Saudi Census. Population by Age Group. Available online: https://portal.saudicensus.sa/portal/public/1/17/44 (accessed on 15 November 2023).
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | N | (%) | Mean (SD) |
|---|---|---|---|
| Age | 62.6 (5.9) | ||
| Gender | |||
| Male | 8 | 57.2 | |
| Female | 6 | 42.8 | |
| Education | |||
| Middle school graduate | 3 | 21.43 | |
| High school graduate | 3 | 21.43 | |
| Bachelor’s Degree | 4 | 28.57 | |
| Master’s Degree | 1 | 7.14 | |
| Ph.D. Degree | 3 | 21.42 | |
| Marital status | |||
| Married | 12 | 85.71 | |
| Widowed | 2 | 14.29 | |
| Income per month | |||
| 0–10,000 | 6 | 42.86 | |
| >10,000–20,000 | 5 | 35.71 | |
| >20,000 and more | 3 | 21.43 | |
| Self-Rated Health | |||
| Fair | 1 | 7.143 | |
| Good | 6 | 42.86 | |
| Very good | 4 | 28.57 | |
| Excellent | 3 | 21.43 | |
| Chronic Diseases | |||
| Yes | 10 | 71.43 | |
| No | 4 | 28.57 | |
| Factor | Type | Count | Quotes from Participants |
|---|---|---|---|
| Sub-theme 1 | |||
| Role of demographics and health status | Age | 12 | “Especially those over 80 years old, they will not use it”. |
| Education | 16 | “The more educated an older person is, the easier the technology will be for him”. | |
| Health status | 13 | “It depends on the extent to which the person cares about his health. There is a difference between a person who is concerned about his health, and exercise, and a person who is not concerned”. | |
| Gender | 14 | “I prefer to go to the hospital and book appointments. As for the app, I don’t like to use it”. | |
| Sub-theme 2 | |||
| Perceived Usefulness | Useful | 12 | “Yes, it is very useful because health awareness has become widespread among the elderly”. |
| Not useful | 5 | “I prefer to go to the hospital and book appointments. As for the technology, I don’t like to use it…” | |
| Perceived Benefit | 30 | “It saves time instead of going to the hospital to make appointments. Also, if I need medical information, I can contact the virtual consultation service and ask them instead of going to the doctor”. | |
| Perceived Need | For oneself | 12 | “Yes, I need it. For example, book appointment” |
| For others | 11 | “Most people are using mobile phones”. | |
| Relative Advantage | Not using similar technology | 5 | “No, I don’t have any similar technology”. |
| Using similar technology | 4 | “Yes, there is a special technology [app] for the university hospital, but it is difficult to book appointments because they are only available within 3 months”. | |
| Sub-theme 3 | |||
| Perceived Ease of Use | Easy | 9 | “It’s easy, just click on the link”. |
| Not easy | 6 | “But if he is uneducated, uncultured, and does not care about his health, it will be difficult for him”. | |
| Convenience | Convenience | 8 | “There is no effort or fatigue”. |
| Inconvenience | 6 | “Make a greater effort to learn it and use it correctly” | |
| Familiarity | Yes | 9 | “Yes, I know about this technology”. |
| No | 2 | “I don’t know it” | |
| Privacy | Invades privacy | 8 | “The topic is sensitive. No one wants to reveal that he has such-and-such a disease because they do not want anyone to know about the disease, or their medical history, as it is confidential information”. |
| Lack of privacy concern/not an issue | 11 | “There is no concern because there is no financial or cognitive return from hacking it”. | |
| Trust | In technology | 11 | “I definitely trust it”. |
| In person | 2 | “Because those responsible for it are trustworthy people”. | |
| Lack of trust | 1 | “I’d rather go to the hospital”. | |
| Sub-theme 4 | |||
| Subjective Norm Health care provider | Positive | 4 | “He’ll see that I’m a advanced person with the ability to use mHealth technology”. |
| Not care | 6 | “I don’t know” | |
| Subjective Norm Family | Positive | 5 | “My family is also happy that I use these technologies and rely on myself”. |
| Not care | 3 | “This is up to me. There is no one who encouraged me or discouraged me from using mHealth technology”. | |
| Subjective Norm Friends | Positive | 5 | “…I expect that they will be happy…” |
| Not care | 1 | “I don’t know” | |
| Advice Acceptance Healthcare provider | Positive | 11 | “…if I do not have it, I should ask the doctor for information about the technology and how to use it…” |
| Negative | 2 | “No, because I have many mHealth applications…” | |
| Advice Acceptance Family | Positive | 10 | “Yes, it excites me”. |
| Negative | 3 | “No, I am satisfied with the mHealth applications on my phone”. | |
| Advice Acceptance Friends | Positive | 6 | “Of course, if I know its benefits, I will help and spread it”. |
| Negative | 2 | “I do not trust people from outside my family”. | |
| Sub-theme 5 | |||
| Compatibility | Compatible | 8 | “Yes, it is easy to integrate”. |
| Incompatible | 4 | “No, on a daily basis, it will be difficult, because it takes time”. | |
| Price Value | Pay | 8 | “If I am used to it and comfortable using it, I will pay”. |
| Not pay | 7 | “No, I will not pay”. | |
| Support availability | Family support | 19 | “First I need someone from my family to teach me and then I will be able to use it”. |
| No support | 8 | “I rely on myself and am not intruding on others…” | |
| Sub-theme 6 | |||
| Attitudes | Positive | 9 | “I feel it is a safety valve for those who understand, and those who learn begin to benefit from them after”. |
| Negative | 5 | “But I want to go to the hospital, it is better for me. Because I don’t like using the mobile phone a lot, only messages or calls”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almulhem, J.A. Factors, Barriers, and Recommendations Related to Mobile Health Acceptance among the Elderly in Saudi Arabia: A Qualitative Study. Healthcare 2023, 11, 3024. https://doi.org/10.3390/healthcare11233024
Almulhem JA. Factors, Barriers, and Recommendations Related to Mobile Health Acceptance among the Elderly in Saudi Arabia: A Qualitative Study. Healthcare. 2023; 11(23):3024. https://doi.org/10.3390/healthcare11233024
Chicago/Turabian StyleAlmulhem, Jwaher A. 2023. "Factors, Barriers, and Recommendations Related to Mobile Health Acceptance among the Elderly in Saudi Arabia: A Qualitative Study" Healthcare 11, no. 23: 3024. https://doi.org/10.3390/healthcare11233024
APA StyleAlmulhem, J. A. (2023). Factors, Barriers, and Recommendations Related to Mobile Health Acceptance among the Elderly in Saudi Arabia: A Qualitative Study. Healthcare, 11(23), 3024. https://doi.org/10.3390/healthcare11233024