
Incidence and Risk Factors for Wound Revision after Surgical Treatment of Spinal Metastasis: A National Population-Based Study in South Korea

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population and Sample
2.3. Inclusion Criteria
2.4. Group Allocation
2.5. Covariates
2.6. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Incidence and Risk Factors of Wound Revision
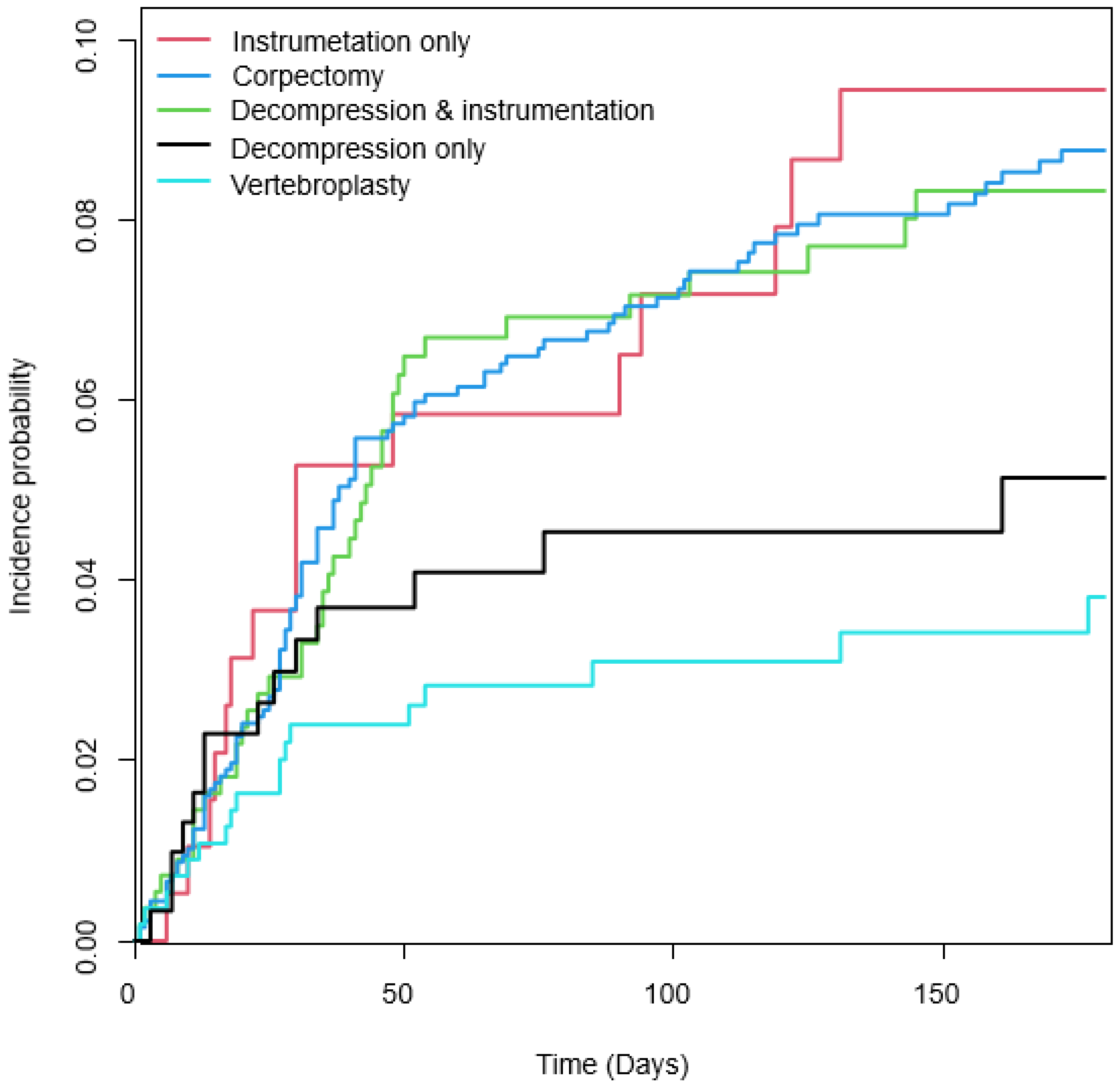
3.3. Wound Revision Risk Factors According to the Surgical Method
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tarawneh, A.M.; Pasku, D.; Quraishi, N.A. Surgical complications and re-operation rates in spinal metastases surgery: A systematic review. Eur. Spine J. 2021, 30, 2791–2799. [Google Scholar] [CrossRef]
- Carl, H.M.; Ahmed, A.K.; Abu-Bonsrah, N.; De la Garza Ramos, R.; Sankey, E.W.; Pennington, Z.; Bydon, A.; Witham, T.F.; Wolinsky, J.-P.; Gokaslan, Z.L. Risk factors for wound-related reoperations in patients with metastatic spine tumor. J. Neurosurg. Spine 2018, 28, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Schilling, A.T.; Ehresman, J.; Huq, S.; Ahmed, A.K.; Lubelski, D.; Cottrill, E.; Pennington, Z.; Shin, J.H.; Sciubba, D.M. Risk factors for wound-related complications after surgery for primary and metastatic spine tumors: A systematic review and meta-analysis. World Neurosurg. 2020, 141, 467–478.e3. [Google Scholar] [CrossRef] [PubMed]
- Jarvers, J.-S.; Lange, M.; Schiemann, S.; Pfränger, J.; Heyde, C.-E.; Osterhoff, G. Risk factors for wound-related complications after surgical stabilization of spinal metastases with a special focus on the effect of postoperative radiation therapy. BMC Surg. 2021, 21, 423. [Google Scholar] [CrossRef] [PubMed]
- White, A.J.; Fiani, B.; Jarrah, R.; Momin, A.A.; Rasouli, J. Surgical site infection prophylaxis and wound management in spine surgery. Asian Spine J. 2022, 16, 451. [Google Scholar] [CrossRef] [PubMed]
- Tavares-Júnior, M.C.M.; Cabrera, G.E.D.; Teixeira, W.G.J.; Narazaki, D.K.; Ghilardi, C.S.; Marcon, R.M.; Cristante, A.F.; de Barros-Filho, T.E.P. Risk Factors Associated with Postoperative Infection in Cancer Patients Undergoing Spine Surgery. Clinics 2021, 76, e2741. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Mansfield, F.L.; Borges, L.F. Spinal radiation before surgical decompression adversely affects outcomes of surgery for symptomatic metastatic spinal cord compression. Spine 2001, 26, 818–824. [Google Scholar] [CrossRef]
- Farrokhi, M.; Nouraei, H.; Kiani, A. The efficacy of percutaneous vertebroplasty in pain relief in patients with pathological vertebral fractures due to metastatic spinal tumors. Iran. Red Crescent Med. J. 2012, 14, 523–530. [Google Scholar]
- Lee, B.; Franklin, I.; Lewis, J.S.; Coombes, R.C.; Leonard, R.; Gishen, P.; Stebbing, J. The efficacy of percutaneous vertebroplasty for vertebral metastases associated with solid malignancies. Eur. J. Cancer 2009, 45, 1597–1602. [Google Scholar] [CrossRef]
- Abdelrahman, H.; Siam, A.E.; Shawky, A.; Ezzati, A.; Boehm, H. Infection after vertebroplasty or kyphoplasty. A series of nine cases and review of literature. Spine J. 2013, 13, 1809–1817. [Google Scholar] [CrossRef]
- Olmos, M.A.; González, A.S.; Clemente, J.D.; Tomé, C.V. Infected vertebroplasty due to uncommon bacteria solved surgically: A rare and threatening life complication of a common procedure: Report of a case and a review of the literature. Spine 2006, 31, E770–E773. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Madhu, S.; Bohra, H.; Pandita, N.; Wang, S.S.Y.; Lopez, K.G.; Tan, J.H.; Vellayappan, B.A. Is there an optimal timing between radiotherapy and surgery to reduce wound complications in metastatic spine disease? A systematic review. Eur. Spine J. 2020, 29, 3080–3115. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Griffin, R.J.; Hui, S.; Levitt, S.H.; Song, C.W. Radiation-induced vascular damage in tumors: Implications of vascular damage in ablative hypofractionated radiotherapy (SBRT and SRS). Radiat. Res. 2012, 177, 311–327. [Google Scholar] [CrossRef] [PubMed]
- Haubner, F.; Ohmann, E.; Pohl, F.; Strutz, J.; Gassner, H.G. Wound healing after radiation therapy: Review of the literature. Radiat. Oncol. 2012, 7, 162. [Google Scholar] [CrossRef] [PubMed]
- Vargas, E.; Mummaneni, P.V.; Rivera, J.; Huang, J.; Berven, S.H.; Braunstein, S.E.; Chou, D. Wound complications in metastatic spine tumor patients with and without preoperative radiation. J. Neurosurg. Spine 2022, 1, 265–270. [Google Scholar] [CrossRef]
- Kelly, C.M.; Shahrokni, A. Moving beyond Karnofsky and ECOG performance status assessments with new technologies. J. Oncol. 2016, 2016, 6186543. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems, 2nd ed.; Tenth Revision; World Health Organization: Geneva, Switzerland, 2004. Available online: https://iris.who.int/handle/10665/42980?&locale-attribute=en (accessed on 23 June 2021).
- Korea Informative Classification of Diseases. Korea Classification Disease (KCD8). Daejeon: Korea Informative Classification of Diseases. 2020. Available online: https://koicd.kr/main.do (accessed on 23 June 2021).
- Choi, H.; Kim, M.; Kim, H.; Pyo Lee, J.; Lee, J.; Tak Park, J.; Hoon Kim, K.; Sik Ahn, H.; Jae Hann, H.; Ryu, D.-R. Excess mortality among patients on dialysis: Comparison with the general population in Korea. Kidney Res. Clin. Pract. 2014, 33, 89–94. [Google Scholar] [CrossRef]
- Barrie, U.; Montgomery, E.Y.; Ogwumike, E.; Pernik, M.N.; Luu, I.Y.; Adeyemo, E.A.; Christian, Z.K.; Edukugho, D.; Johnson, Z.D.; Hoes, K. Household income as a predictor for surgical outcomes and opioid use after spine surgery in the United States. Glob. Spine J. 2023, 13, 2124–2134. [Google Scholar] [CrossRef]
- Omeis, I.A.; Dhir, M.; Sciubba, D.M.; Gottfried, O.N.; McGirt, M.J.; Attenello, F.J.; Wolinsky, J.-P.; Gokaslan, Z.L. Postoperative Surgical Site Infections in Patients Undergoing Spinal Tumor Surgery: Incidence and Risk Factors. Spine 2011, 36, 1410–1419. [Google Scholar] [CrossRef]
- Choi, S.H.; Koo, J.W.; Choe, D.; Kang, C.-N. The incidence and management trends of metastatic spinal tumors in South Korea: A nationwide population-based study. Spine 2020, 45, E856–E863. [Google Scholar] [CrossRef] [PubMed]
- Sohn, S.; Chung, C.K.; Do Han, K.; Jung, J.H.; Hyeun, J.H.; Kim, J.; Chang, U.-K.; Sohn, M.J.; Kim, S.H. A nationwide study of surgery in a newly diagnosed spine metastasis population. J. Korean Neurosurg. Soc. 2019, 62, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef] [PubMed]
- Lakomkin, N.; Zuckerman, S.L.; Stannard, B.; Montejo, J.; Sussman, E.S.; Virojanapa, J.; Kuzmik, G.; Goz, V.; Hadjipanayis, C.G.; Cheng, J.S. Preoperative Risk Stratification in Spine Tumor Surgery: A Comparison of the Modified Charlson Index, Frailty Index, and ASA Score. Spine 2019, 44, E782–E787. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Rooh-ul-Muqim, Z.M.; Khalil, J.; Salman, M. Influence of ASA score and Charlson Comorbidity Index on the surgical site infection rates. J. Coll. Physicians Surg. Pak. 2010, 20, 506–509. [Google Scholar] [PubMed]


{kind=link}
| Total (n = 3001) | Wound Revision Group (n = 197) | Control (n = 2804) | p | |
|---|---|---|---|---|
| Age | 0.1076 | |||
| –39 | 105 (3.5) | 11 (5.58) | 94 (3.35) | |
| 40–64 | 1420 (47.32) | 100 (50.76) | 1320 (47.08) | |
| 65– | 1476 (49.18) | 86 (43.65) | 1390 (49.57) | |
| Sex, male | 1948 (64.91) | 126 (63.96) | 1822 (64.98) | 0.772 |
| Income, low 25% | 757 (25.22) | 56 (28.43) | 701 (25) | 0.2845 |
| Surgery | 0.0018 * | |||
| 307 (10.23) | 14 (7.11) | 293 (10.45) | |
| 194 (6.46) | 16 (8.12) | 178 (6.35) | |
| 555 (18.49) | 41 (20.81) | 514 (18.33) | |
| 1385 (46.15) | 108 (54.82) | 1277 (45.54) | |
| 560 (18.66) | 18 (9.14) | 542 (19.33) | |
| Preoperative radiation | 1025 (34.16) | 74 (37.56) | 951 (33.92) | 0.2967 |
| Early postoperative radiation | 869 (28.96) | 52 (26.4) | 817 (29.14) | 0.4123 |
| Late postoperative radiation | 1346 (44.85) | 83 (42.13) | 1263 (45.04) | 0.4272 |
| Preoperative Chemotherapy | 1184 (39.45) | 87 (44.16) | 1097 (39.12) | 0.1618 |
| Early postoperative chemotherapy | 345 (11.5) | 23 (11.68) | 322 (11.48) | 0.9351 |
| Late postoperative chemotherapy | 1034 (34.46) | 70 (35.53) | 964 (34.38) | 0.7419 |
| Cord compression | 648 (21.59) | 42 (21.32) | 606 (21.61) | 0.9232 |
| CCI | 7.65 ± 2.13 | 7.94 ± 1.95 | 7.63 ± 2.15 | 0.0467 * |
| Decompression Only (n = 307) | Instrumentation Only (n = 194) | Decompression and Instrumentation (n = 555) | Corpectomy (n = 1385) | Vertebroplasty (n = 560) | p | |
|---|---|---|---|---|---|---|
| Age | 11 (3.58) | 8 (4.12) | 17 (3.06) | 61 (4.4) | 8 (1.43) | <0.0001 * |
| –39 | 143 (46.58) | 98 (50.52) | 267 (48.11) | 741 (53.5) | 171 (30.54) | |
| 40–64 | 153 (49.84) | 88 (45.36) | 271 (48.83) | 583 (42.09) | 381 (68.04) | |
| 65– | 226 (73.62) | 116 (59.79) | 373 (67.21) | 895 (64.62) | 338 (60.36) | |
| Sex, male | 89 (28.99) | 53 (27.32) | 149 (26.85) | 346 (24.98) | 120 (21.43) | 0.0008 * |
| Income, low 25% | 11 (3.58) | 8 (4.12) | 17 (3.06) | 61 (4.4) | 8 (1.43) | 0.097 |
| Preoperative radiation | 87 (28.34) | 66 (34.02) | 199 (35.86) | 461 (33.29) | 212 (37.86) | 0.056 |
| Early postoperative radiation | 95 (30.94) | 55 (28.35) | 171 (30.81) | 425 (30.69) | 123 (21.96) | 0.002 * |
| Late postoperative radiation | 122 (39.74) | 103 (53.09) | 240 (43.24) | 738 (53.29) | 143 (25.54) | <0.0001 |
| Preoperative | 99 (32.25) | 69 (35.57) | 208 (37.48) | 548 (39.57) | 260 (46.43) | 0.0005 * |
| Chemotherapy | 33 (10.75) | 21 (10.82) | 65 (11.71) | 142 (10.25) | 84 (15) | 0.0577 |
| Early postoperative chemotherapy | 94 (30.62) | 80 (41.24) | 200 (36.04) | 509 (36.75) | 151 (26.96) | <0.0001 * |
| Late postoperative chemotherapy | 54 (17.59) | 35 (18.04) | 131 (23.6) | 292 (21.08) | 136 (24.29) | 0.0816 |
| Cord compression | 7.74 ± 2.23 | 7.43 ± 1.94 | 7.64 ± 2.06 | 7.58 ± 2.1 | 7.85 ± 2.28 | 0.0616 |
| CCI | 87 (28.34) | 66 (34.02) | 199 (35.86) | 461 (33.29) | 212 (37.86) | 0.056 |
| Surgery | Event (n) | HR for Model 1 | p- Value | HR for Model 2 | p-Value | HR for Model 3 | p-Value |
|---|---|---|---|---|---|---|---|
| Decompression only (n = 307) | 14 | 1.421 (0.707, 2.858) | 0.0076 * | 1.354 (0.67, 2.734) | 0.0188 * | 1.347 (0.667, 2.721) | 0.0171 * |
| Instrumentation only (n = 194) | 16 | 2.481 (1.265, 4.866) | 2.332 (1.184, 4.592) | 2.379 (1.207, 4.687) | |||
| Decompression and instrumentation (n = 555) | 41 | 2.255 (1.296, 3.925) | 2.154 (1.233, 3.762) | 2.159 (1.235, 3.774) | |||
| Corpectomy (n = 1385) | 108 | 2.336 (1.418, 3.847) | 2.175 (1.31, 3.609) | 2.181 (1.313, 3.621) | |||
| Vertebroplasty (n = 560) | 18 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-D.; Jang, H.-D.; Park, J.-S.; Chung, N.-S.; Chung, H.-W.; Jun, J.-Y.; Han, K.; Hong, J.-Y. Incidence and Risk Factors for Wound Revision after Surgical Treatment of Spinal Metastasis: A National Population-Based Study in South Korea. Healthcare 2023, 11, 2962. https://doi.org/10.3390/healthcare11222962
Lee H-D, Jang H-D, Park J-S, Chung N-S, Chung H-W, Jun J-Y, Han K, Hong J-Y. Incidence and Risk Factors for Wound Revision after Surgical Treatment of Spinal Metastasis: A National Population-Based Study in South Korea. Healthcare. 2023; 11(22):2962. https://doi.org/10.3390/healthcare11222962
Chicago/Turabian StyleLee, Han-Dong, Hae-Dong Jang, Jin-Sung Park, Nam-Su Chung, Hee-Woong Chung, Jin-Young Jun, Kyungdo Han, and Jae-Young Hong. 2023. "Incidence and Risk Factors for Wound Revision after Surgical Treatment of Spinal Metastasis: A National Population-Based Study in South Korea" Healthcare 11, no. 22: 2962. https://doi.org/10.3390/healthcare11222962
APA StyleLee, H.-D., Jang, H.-D., Park, J.-S., Chung, N.-S., Chung, H.-W., Jun, J.-Y., Han, K., & Hong, J.-Y. (2023). Incidence and Risk Factors for Wound Revision after Surgical Treatment of Spinal Metastasis: A National Population-Based Study in South Korea. Healthcare, 11(22), 2962. https://doi.org/10.3390/healthcare11222962