
Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions

 ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sociodemographic Characteristics
2.3. General Health Status
2.4. Yale Physical Activity Survey
2.5. Perceived Barriers to the PA Questionnaire
2.6. Statistical Analysis
3. Results
4. Discussion
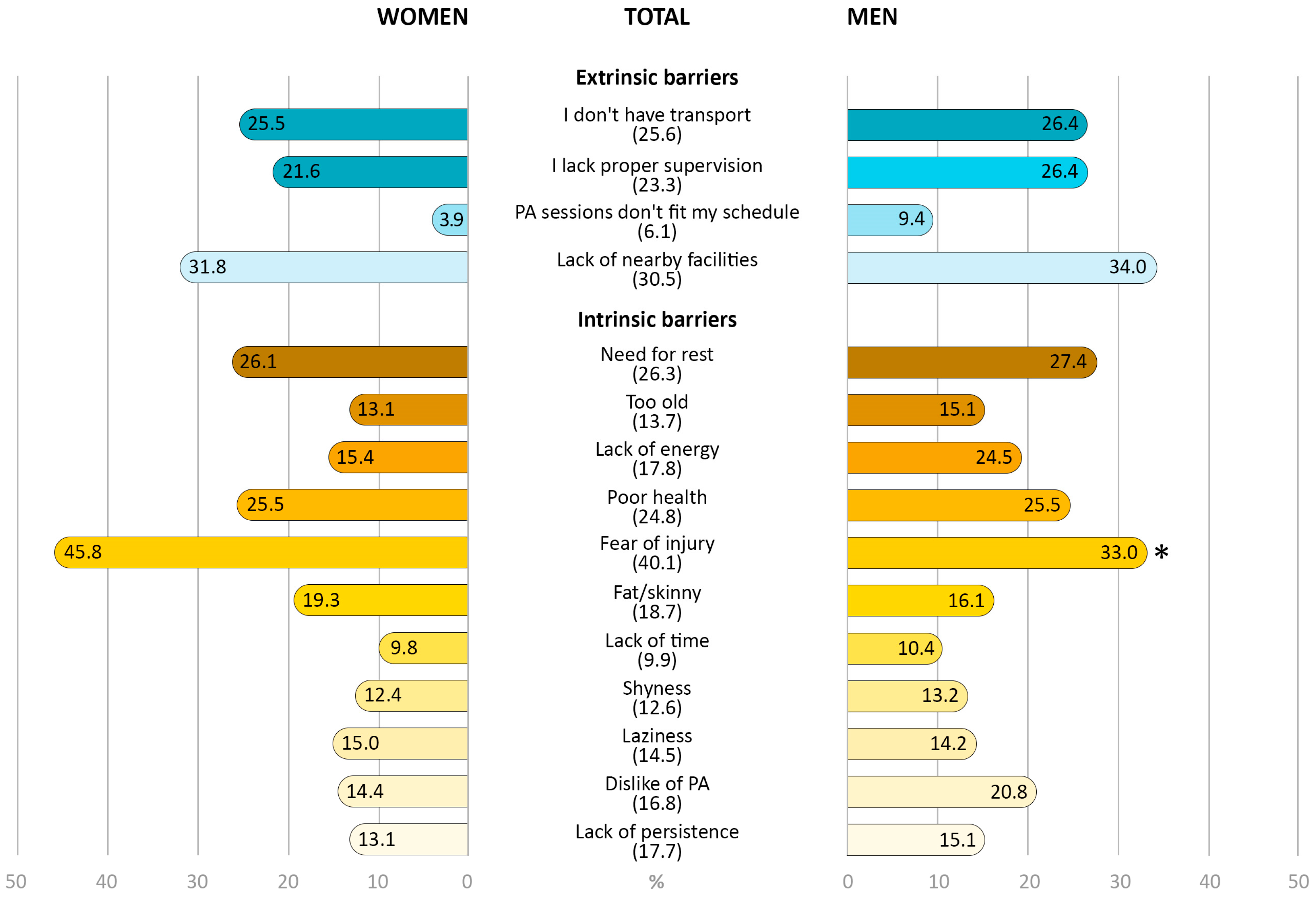
4.1. Prevalence and Gender Differences of Perceived Barriers to PA
4.2. Correlation between PA Barriers and PA Dimensions
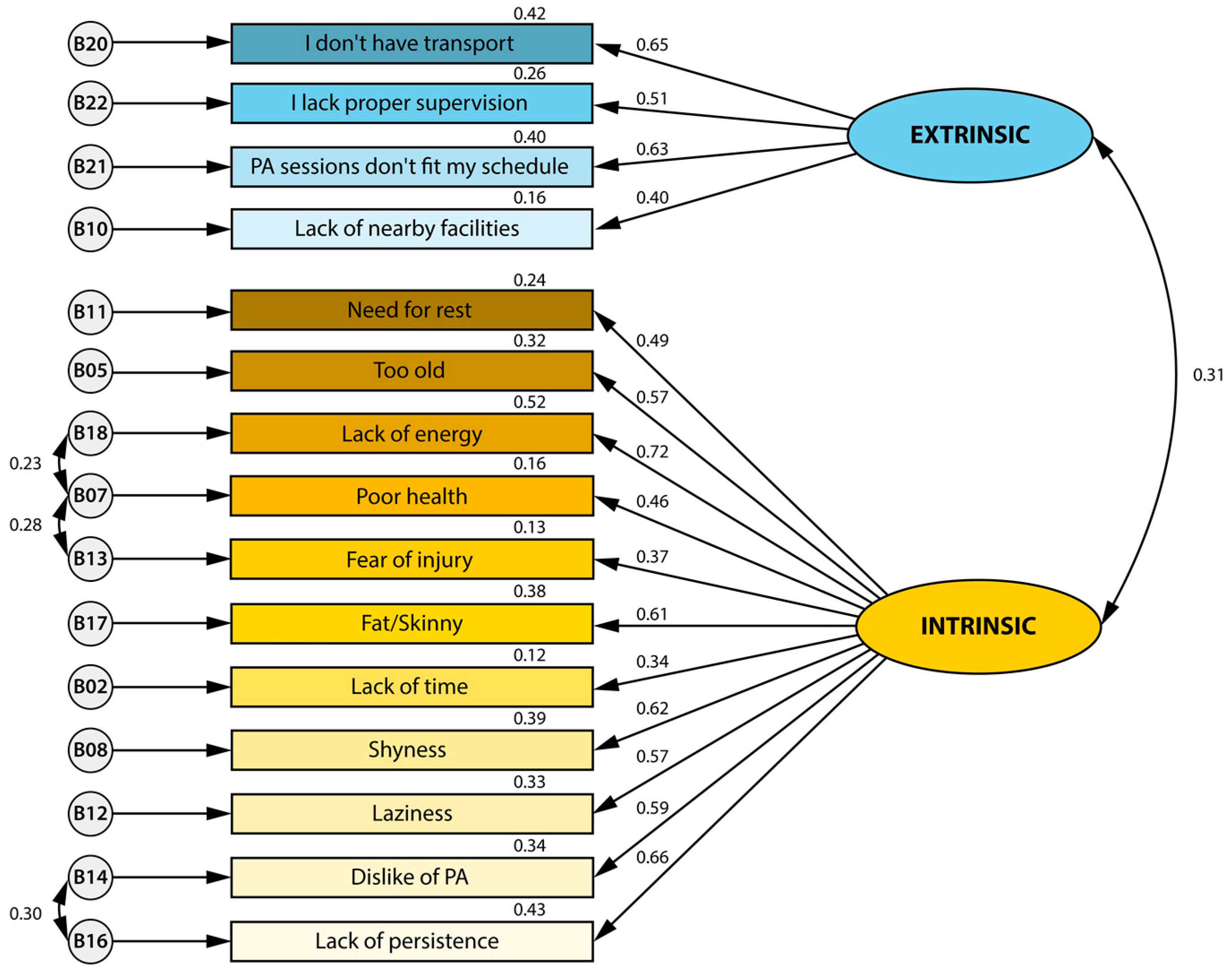
4.3. Confirmatory Factor Analysis Model
4.4. Limitations, Strengths, and Future Directions
4.5. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.-M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 2022, 56, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary behavior, exercise, and cardiovascular health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Stubbs, B.; Chen, L.J.; Chang, C.Y.; Sun, W.J.; Ku, P.W. Accelerometer-assessed light physical activity is protective of future cognitive ability: A longitudinal study among community dwelling older adults. Exp. Gerontol. 2017, 91, 104–109. [Google Scholar] [CrossRef]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Marquez, D.X.; Aguiñaga, S.; Vásquez, P.M.; Conroy, D.E.; Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Sheppard, B.B.; Petruzzello, S.J.; et al. A systematic review of physical activity and quality of life and well-being. Transl. Behav. Med. 2020, 10, 1098–1109. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet. Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Agostino, D.; Daskalopoulou, C.; Wu, Y.-T.; Koukounari, A.; Haro, J.M.; Tyrovolas, S.; Panagiotakos, D.B.; Prince, M.; Prina, A.M. The impact of physical activity on healthy ageing trajectories: Evidence from eight cohort studies. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, K.; Broom, D.; Bekhet, A.H.; De Caro, J.X.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-aged and Older-adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef]
- Baert, V.; Gorus, E.; Mets, T.; Geerts, C.; Bautmans, I. Motivators and barriers for physical activity in the oldest old: A systematic review. Ageing Res. Rev. 2011, 10, 464–474. [Google Scholar] [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Bethancourt, H.J.; Rosenberg, D.E.; Beatty, T.; Arterburn, D.E. Barriers to and facilitators of physical activity program use among older adults. Clin. Med. Res. 2014, 12, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Moschny, A.; Platen, P.; Klaaßen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to physical activity in older adults in Germany: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 121. [Google Scholar] [CrossRef]
- Omelan, A.; Podstawski, R.; Wziatek, B.; Merino-Marbán, R.; Romero-Ramos, O. Physical activity levels of rural and urban seniors in the region of Warmia and Mazury in Poland. Balt. J. Health Phys. Act. 2017, 2017, 74–88. [Google Scholar] [CrossRef]
- Rai, R.; Jongenelis, M.I.; Jackson, B.; Newton, R.U.; Pettigrew, S. Exploring Factors Associated with Physical Activity in Older Adults: An Ecological Approach. J. Aging Phys. Act. 2019, 27, 343–353. [Google Scholar] [CrossRef] [PubMed]
- van Uffelen, J.G.Z.; Khan, A.; Burton, N.W. Gender differences in physical activity motivators and context preferences: A population-based study in people in their sixties. BMC Public Health 2017, 17, 624. [Google Scholar] [CrossRef]
- Adjei, N.K.; Brand, T. Investigating the associations between productive housework activities, sleep hours and self-reported health among elderly men and women in western industrialised countries. BMC Public Health 2018, 18, 110. [Google Scholar] [CrossRef]
- Lee, Y.S. Gender differences in physical activity and walking among older adults. J. Women Aging 2005, 17, 55–70. [Google Scholar] [CrossRef]
- Cabanas-Sánchez, V.; Esteban-Cornejo, I.; Migueles, J.H.; Banegas, J.R.; Graciani, A.; Rodríguez-Artalejo, F.; Martínez-Gómez, D. Twenty four-hour activity cycle in older adults using wrist-worn accelerometers: The seniors-ENRICA-2 study. Scand. J. Med. Sci. Sports 2020, 30, 700–708. [Google Scholar] [CrossRef]
- Stalling, I.; Albrecht, B.M.; Doerwald, F.; Bammann, K. Time allocation to active domains, physical activity, and health indicators in older adults: Cross-sectional results from the OUTDOOR ACTIVE study. BMC Public Health 2020, 20, 1580. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Chaput, J.P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; Kho, M.E.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-Hour Movement Guidelines for Adults aged 18-64 years and Adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2020, 45, S57–S102. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Yang, P.S.; Park, B.E.; Kang, T.S.; Lim, S.H.; Cho, S.; Lee, S.Y.; Chung, Y.H.; Lee, M.Y.; Kim, D.; et al. Association of Light-Intensity Physical Activity with Mortality in the Older Population: A Nationwide Cohort Study. Front. Cardiovasc. Med. 2022, 9, 859277. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Qiang, F. Psychosocial Mediation of Light-Moderate Physical Activity and Cognitive Performance among Adults Aged 60+ in China. Behav. Sci. 2022, 12, 175. [Google Scholar] [CrossRef]
- McMullan, I.I.; Bunting, B.P.; McDonough, S.M.; Tully, M.A.; Casson, K. The association between light intensity physical activity with gait speed in older adults (≥ 50 years). A longitudinal analysis using the English Longitudinal Study of Ageing (ELSA). Aging Clin. Exp. Res. 2020, 32, 2279–2285. [Google Scholar] [CrossRef]
- Rees-Punia, E.; Deubler, E.; Campbell, P.; Gapstur, S.M.; Patel, A. Light-Intensity Physical Activity in a Large Prospective Cohort of Older US Adults: A 21-Year Follow-Up of Mortality. Gerontology 2020, 66, 259–265. [Google Scholar] [CrossRef]
- Welch, W.A.; Strath, S.J.; Brondino, M.; Walker, R.; Swartz, A.M. Duration-Response of Light-Intensity Physical Activity and Glucose Dynamics in Older Adults. J. Phys. Act. Health 2019, 16, 37–42. [Google Scholar] [CrossRef]
- Volders, E.; de Groot, R.H.M.; Bolman, C.A.W.; Lechner, L. The longitudinal associations between change in physical activity and cognitive functioning in older adults with chronic illness (es). BMC Geriatr. 2021, 21, 478. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Leslie, E.; Sugiyama, T.; Owen, N. Perceived barriers to leisure-time physical activity in adults: An ecological perspective. J. Phys. Act. Health 2010, 7, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry analysis of physical activity and sedentary behavior in older adults: A systematic review and data analysis. Eur. Rev. Aging Phys. Act. 2014, 11, 35–49. [Google Scholar] [CrossRef]
- Fernandes, D. A avaliação das aprendizagens no Sistema Educativo Português. Educ. Pesqui. 2007, 33, 581–600. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.L. Development of the Portuguese version of MOS SF-36. Part II--Validation tests. Acta Med. Port. 2000, 13, 119–127. [Google Scholar]
- Machado, M.; Tavares, C.; Moniz-Pereira, V.; André, H.; Ramalho, F.; Veloso, A.; Carnide, F. Validation of YPAS-PT—The Yale Physical Activity Survey for Portuguese Older People. Sci. J. Public Health 2016, 4, 72. [Google Scholar] [CrossRef][Green Version]
- Dipietro, L.; Caspersen, C.J.; Ostfeld, A.M.; Nadel, E.R. A survey for assessing physical activity among older adults. Med. Sci. Sports Exerc. 1993, 25, 628–642. [Google Scholar] [CrossRef]
- Young, D.R.; Jee, S.H.; Appel, L.J. A comparison of the Yale Physical Activity Survey with other physical activity measures. Med. Sci. Sports Exerc. 2001, 33, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Booth, M.L.; Bauman, A.; Owen, N. Perceived Barriers to Physical Activity among Older Australians. J. Aging Phys. Act. 2002, 10, 271–280. [Google Scholar] [CrossRef]
- Nascimento, C.M.C.; Gobbi, S.; Sussumu Hirayama, M.; Colim Brazão, M. Nível De Atividade Física E As Principais Barreiras Percebidas Por Idosos De Rio Claro. J. Phys. Educ. 2008, 19, 109–118. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef]
- Gjersing, L.; Caplehorn, J.R.; Clausen, T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Med. Res. Methodol. 2010, 10, 13. [Google Scholar] [CrossRef]
- Enders, C.K.; Bandalos, D.L. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Struct. Equ. Model. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016; Description: xvii; 534p. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS; Psychology Press: New York, NY, USA, 2000; ISBN 9781410600219. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- European Commission. European Commission Special Eurobarometer 525 for Sport and Physical Activity; European Union: Brussels, Belgium, 2022; ISBN 978-92-76-56432-4. [Google Scholar]
- Arazi, H.; Izadi, M.; Kabirian, H. Interactive effect of socio-eco-demographic characteristics and perceived physical activity barriers on physical activity level among older adults. Eur. Rev. Aging Phys. Act. 2022, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Guedes-Estevez, E.; Costa, A.R.; Moura-Ferreira, P.; Lunet, N.; Morais, S. Regular physical activity-related awareness and knowledge in Portugal: Results from a population-based survey. Porto Biomed. J. 2021, 6, e130. [Google Scholar] [CrossRef] [PubMed]
- Mathews, A.E.; Laditka, S.B.; Laditka, J.N.; Wilcox, S.; Corwin, S.J.; Liu, R.; Friedman, D.B.; Hunter, R.; Tseng, W.; Logsdon, R.G. Older adults’ perceived physical activity enablers and barriers: A multicultural perspective Mathews A.E. J. Aging Phys. Act. 2010, 18, 119–140. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, K.A.; Zhou, W.; Rojer, A.G.M.; Reijnierse, E.M.; Maier, A.B. Associations of objectively measured physical activity and sedentary behaviour with fall-related outcomes in older adults: A systematic review. Ann. Phys. Rehabil. Med. 2022, 65, 101571. [Google Scholar] [CrossRef]
- Wongsila, S.; Chernbumroong, S.; Sureephong, P. Systematic reviews of elderly exercise barriers. In Proceedings of the 2022 Joint International Conference on Digital Arts, Media and Technology with ECTI Northern Section Conference on Elec-trical, Electronics, Computer and Telecommunications Engineering (ECTI DAMT & NCON), Chiang Rai, Thailand, 26–28 January 2022; pp. 460–462. [Google Scholar]
- Harrison, E.A.; Lord, L.M.; Asongwed, E.; Jackson, P.; Johnson-Largent, T.; Jean Baptiste, A.M.; Harris, B.M.; Jeffery, T. Perceptions, Opinions, Beliefs, and Attitudes About Physical Activity and Exercise in Urban-Community-Residing Older Adults. J. Prim. Care Community Health 2020, 11, 2150132720924137. [Google Scholar] [CrossRef]
- Gray, P.M.; Murphy, M.H.; Gallagher, A.M.; Simpson, E.E.A. Motives and Barriers to Physical Activity Among Older Adults of Different Socioeconomic Status. J. Aging Phys. Act. 2016, 24, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, S.; Sebastiao, E.; Papini, C.B.; Nakamura, P.M.; Valdanha Netto, A.; Gobbi, L.T.B.; Kokubun, E. Physical inactivity and related barriers: A study in a community dwelling of older brazilians. J. Aging Res. 2012, 2012, 685190. [Google Scholar] [CrossRef]
- Sjöström, M.; Oja, P.; Hagströmer, M.; Smith, B.J.; Bauman, A. Health-enhancing physical activity across European Union countries: The Eurobarometer study. J. Public Health 2006, 14, 291–300. [Google Scholar] [CrossRef]
- Shinn, C.; Salgado, R.; Rodrigues, D. National programme for promotion of physical activity: The situation in Portugal. Cienc. Saude Coletiva 2020, 25, 1339–1348. [Google Scholar] [CrossRef]
- Rodrigues, V.; Mota-Pinto, A.; De Sousa, B.; Botelho, A.; Alves, C.; De Oliveira, C.R. The aging profile of the Portuguese population: A principal component analysis. J. Community Health 2014, 39, 747–752. [Google Scholar] [CrossRef][Green Version]
- Santos, R.; Nunes, A.; Ribeiro, J.C.; Santos, P.; Duarte, J.A.R.; Mota, J. Obesidade, síndrome metabólica e atividade física: Estudo exploratório realizado com adultos de ambos os sexos, da Ilha de S. Miguel, Região Autônoma dos Açores, Portugal. Rev. Bras. Educ. Física Esporte 2005, 19, 317–328. [Google Scholar] [CrossRef]
- Guerreiro, M.; Pereira, I. Women’s Occupational Patterns and Work-Family Arrangements: Do National and Organisational Policies Matter. In Women, Men, Work and Family in Europe; Springer: Berlin/Heidelberg, Germany, 2007; pp. 190–209. ISBN 978-1-349-54127-0. [Google Scholar]
- Cunha, M.; André, S.; Aparício, G.; Santos, E.; Nunes, C. Organization of housework in heterosexual couples: Systematic review of the literature. Procedia-Social Behav. Sci. 2016, 217, 459–468. [Google Scholar] [CrossRef][Green Version]
- Voicu, M.; Voicu, B.; Strapcova, K. Housework and gender inequality in European countries. Eur. Sociol. Rev. 2009, 25, 365–377. [Google Scholar] [CrossRef]
- Gross, S.M.; Gary, T.L.; Browne, D.C.; LaVeist, T.A. Gender differences in body image and health perceptions among graduating seniors from a historically black college. J. Natl. Med. Assoc. 2005, 97, 1608–1619. [Google Scholar]
- Rhodes, R.E.; Martin, A.D.; Taunton, J.E.; Rhodes, E.C.; Donnelly, M.; Elliot, J. Factors associated with exercise adherence among older adults. An individual perspective. Sport. Med. 1999, 28, 397–411. [Google Scholar] [CrossRef]
- McAuley, E.; Blissmer, B. Self-efficacy determinants and consequences of physical activity. Exerc. Sport Sci. Rev. 2000, 28, 85–88. [Google Scholar] [CrossRef]
- Bunn, F.; Dickinson, A.; Barnett-Page, E.; Mcinnes, E.; Horton, K. A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. 2008, 28, 449–472. [Google Scholar] [CrossRef]
- You, E.; Lautenschlager, N.T.; Wan, C.S.; Goh, A.M.Y.; Curran, E.; Chong, T.W.H.; Anstey, K.J.; Hanna, F.; Ellis, K.A. Ethnic Differences in Barriers and Enablers to Physical Activity Among Older Adults. Front. Public Health 2021, 9, 1309. [Google Scholar] [CrossRef]
- Guthold, R.; Ono, T.; Strong, K.L.; Chatterji, S.; Morabia, A. Worldwide Variability in Physical Inactivity. Am. J. Prev. Med. 2008, 34, 486–494. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Park, H.; Watanabe, E.; Park, S.; Shephard, R.J. Habitual physical activity and physical fitness in older Japanese adults: The nakanojo study. Gerontology 2009, 55, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Mcauley, E.; Szabo, A.; Gothe, N.; Olson, E.A. Self-Efficacy: Implications for Physical Activity, Function, and Functional Limitations in Older Adults. Am. J. Lifestyle Med. 2011, 5, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, B.J.; Parsons, T.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Papacosta, O.; Morris, R.W.; Wannamethee, S.G.; Lee, I.M.; Whincup, P.H. Objectively measured physical activity, sedentary behaviour and all-cause mortality in older men: Does volume of activity matter more than pattern of accumulation? Br. J. Sports Med. 2019, 53, 1013–1020. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Hawkins, K.; Greame, C. The Frequency and Health Benefits of Physical Activity for Older Adults. Popul. Health Manag. 2017, 20, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting time, physical activity, and risk of mortality in adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Compernolle, S.; De Cocker, K.; Cardon, G.; De Bourdeaudhuij, I.; Van Dyck, D. Older Adults’ Perceptions of Sedentary Behavior: A Systematic Review and Thematic Synthesis of Qualitative Studies. Gerontologist 2020, 60, e572–e582. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| χ2/df | SRMR | NFI | CFI | RMSEA | |
|---|---|---|---|---|---|
| Model | 192.84/0.86 | 0.072 | 0.810 | 0.882 | 0.070 |
| Characteristics | Total Sample (n = 259) | Women (n = 153) | Men (n = 106) |
|---|---|---|---|
| Sociodemographic | |||
| Age (years) ¥ | 75.17 ± 8.05 | 75.14 ± 7.96 | 75.22 ± 8.22 |
| 60–69 | 27.5 (72) | 26.8 (41) | 29.2 (31) |
| 70–79 | 43.1 (113) | 45.1 (69) | 41.5 (44) |
| ≥80 | 28.2 (74) | 28.1 (43) | 29.2 (31) |
| Education level ¥ | |||
| <4th Grade | 17.9 (47) | 19.6 (30) | 16.0 (17) |
| 4th Grade | 52.7 (138) | 53.6 (82) | 52.8 (56) |
| >4th Grade | 28.2 (74) | 26.8 (41) | 31.1 (33) |
| Income level ¥ | |||
| Low (<500€) | 38.2 (100) | 45.8 (70) | 28.3 (30) * |
| Average (500–750€) | 16.4 (43) | 15.0 (23) | 18.9 (20) |
| High (>750€) | 44.3 (116) | 39.8 (60) | 52.8 (56) |
| Living arrangement ¥ | |||
| Living with a partner | 56.9 (139) | 50.3 (77) | 67.9 (72) |
| Living alone | 43.1 (120) | 49.7 (76) | 32.1 (34) * |
| General health Status | |||
| Comorbidity index § | 3.33 (0.57) | 4.71 (1.37) | 4.47 (1.30) |
| Self-reported health status ¥ | |||
| Positive | 81.2 (211) | 92.7 (139) | 74.5 (79) |
| Negative | 18.8 (48) | 7.3 (14) | 25.5 (27) * |
| PA dimensions index | |||
| Vigorous index (u/m) | 16.66 ± 5.57 | 8.82 ± 9.64 | 8.82 ± 6.78 |
| Walking index (u/m) | 13.33 ± 4.61 | 13.91 ± 7.98 | 13.98 ± 9.07 |
| Moving index (h/d) | 11.11 ± 4.58 | 9.37 ± 3.28 | 8.39 ± 3.54 |
| Standing index (h/d) | 7.33 ± 3.05 | 6.06 ± 2.10 | 6.23 ± 2.24 |
| Sitting index (h/d) | 2.34 ± 1.86 | 2.22 ± 0.92 | 2.15 ± 0.81 |
| Physical Activity Dimension * | R2 | β | p |
|---|---|---|---|
| Vigorous index (units/month) | |||
| Model 2|comorbidities + self-reported health status | 0.07 | −0.122 | 0.002 |
| Leisure walking index (units/month) | |||
| Model 1|Intrinsic factors | 0.06 | −0.261 | 0.001 |
| Moving index (hours/day) | |||
| Model 3|Age + intrinsic factors + extrinsic factors | 0.08 | 0.182 | 0.001 |
| Standing index (hours/day) | |||
| Model 2|Age + extrinsic factors | 0.07 | −0.158 | 0.002 |
| Sitting index (hours/day) | |||
| Model 1|Age | 0.09 | 0.314 | <0.001 |
| Physical Activity Dimension * | R2 | β | p |
|---|---|---|---|
| Vigorous index (units/month) | |||
| Model 1|Self-reported health status | 0.03 | −0.205 | 0.039 |
| Leisure walking index (units/month) | |||
| Model 1|Self-reported health status | 0.12 | −0.353 | <0.001 |
| Moving index (hours/day) | |||
| Model 1|Extrinsic factors | 0.09 | −0.322 | 0.001 |
| Standing index (hours/day) | |||
| Model 1|Self-reported health status | 0.03 | −0.201 | 0.043 |
| Sitting index (hours/day) | |||
| Model 1|Self-reported health status | 0.03 | 0.209 | 0.035 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rúa-Alonso, M.; Bovolini, A.; Costa-Brito, A.R.; Vaz, C.; Marques, E.; Serra, N.; Lopes, V.P.; Vila-Chã, C. Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions. Healthcare 2023, 11, 2948. https://doi.org/10.3390/healthcare11222948
Rúa-Alonso M, Bovolini A, Costa-Brito AR, Vaz C, Marques E, Serra N, Lopes VP, Vila-Chã C. Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions. Healthcare. 2023; 11(22):2948. https://doi.org/10.3390/healthcare11222948
Chicago/Turabian StyleRúa-Alonso, María, Antonio Bovolini, Ana Raquel Costa-Brito, Cláudia Vaz, Ermelinda Marques, Nuno Serra, Vítor P. Lopes, and Carolina Vila-Chã. 2023. "Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions" Healthcare 11, no. 22: 2948. https://doi.org/10.3390/healthcare11222948
APA StyleRúa-Alonso, M., Bovolini, A., Costa-Brito, A. R., Vaz, C., Marques, E., Serra, N., Lopes, V. P., & Vila-Chã, C. (2023). Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions. Healthcare, 11(22), 2948. https://doi.org/10.3390/healthcare11222948