
Diabetes Pay-for-Performance Program Participation and Dialysis Risk in Relation to Educational Attainment: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
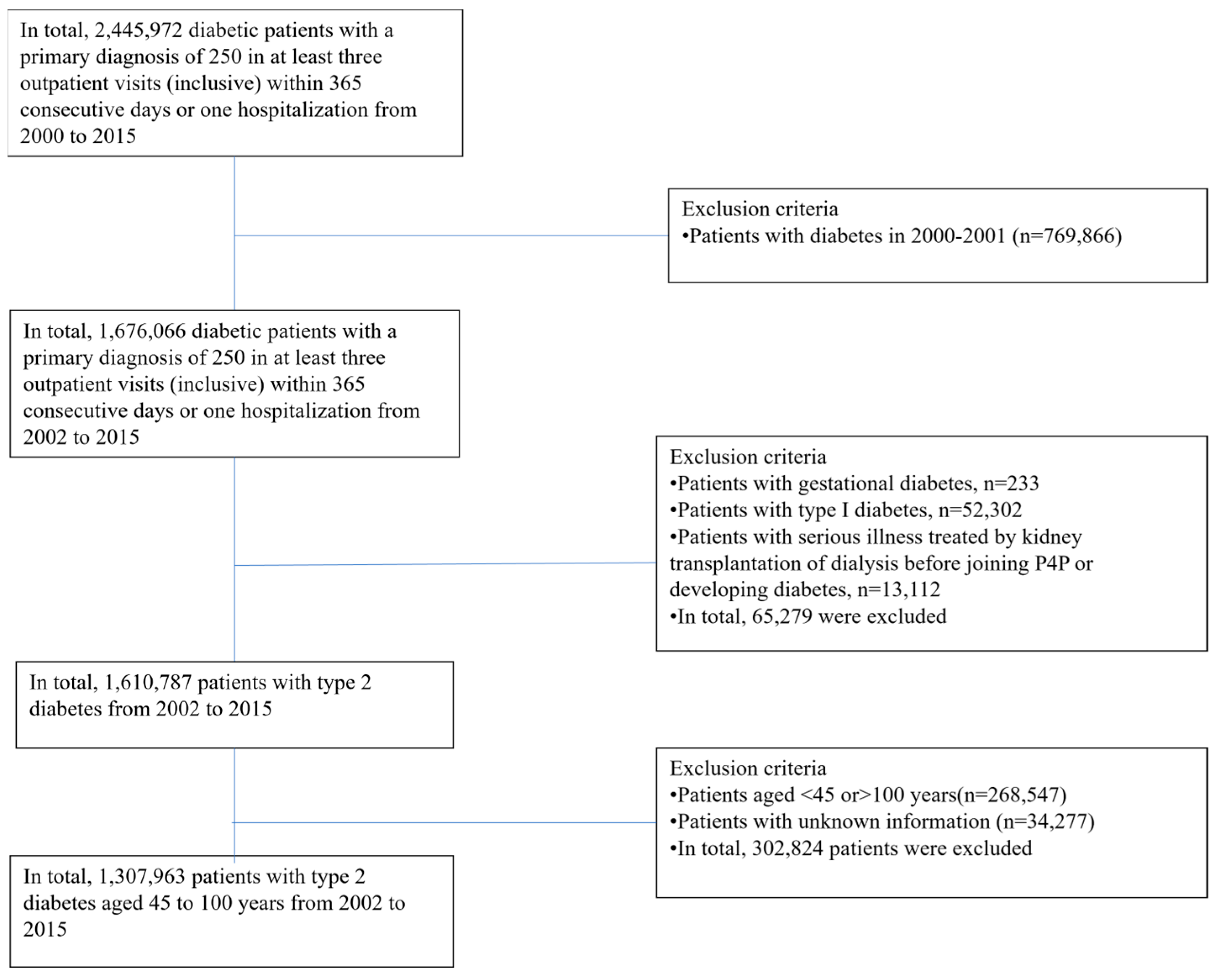
2.1. Study Subjects
2.2. Data Sources
2.3. Descriptions of Variables
2.4. Statistical Analysis
3. Results
3.1. Differences in Participation in the Pay-for-Performance Program among Diabetic Patients with Different Educational Levels
3.2. Educational Level Associated with the Dialysis Incidence Rate (Per Thousand Person-Years) of Diabetic Patients Participating and Not Participating in the Pay-for-Performance Program
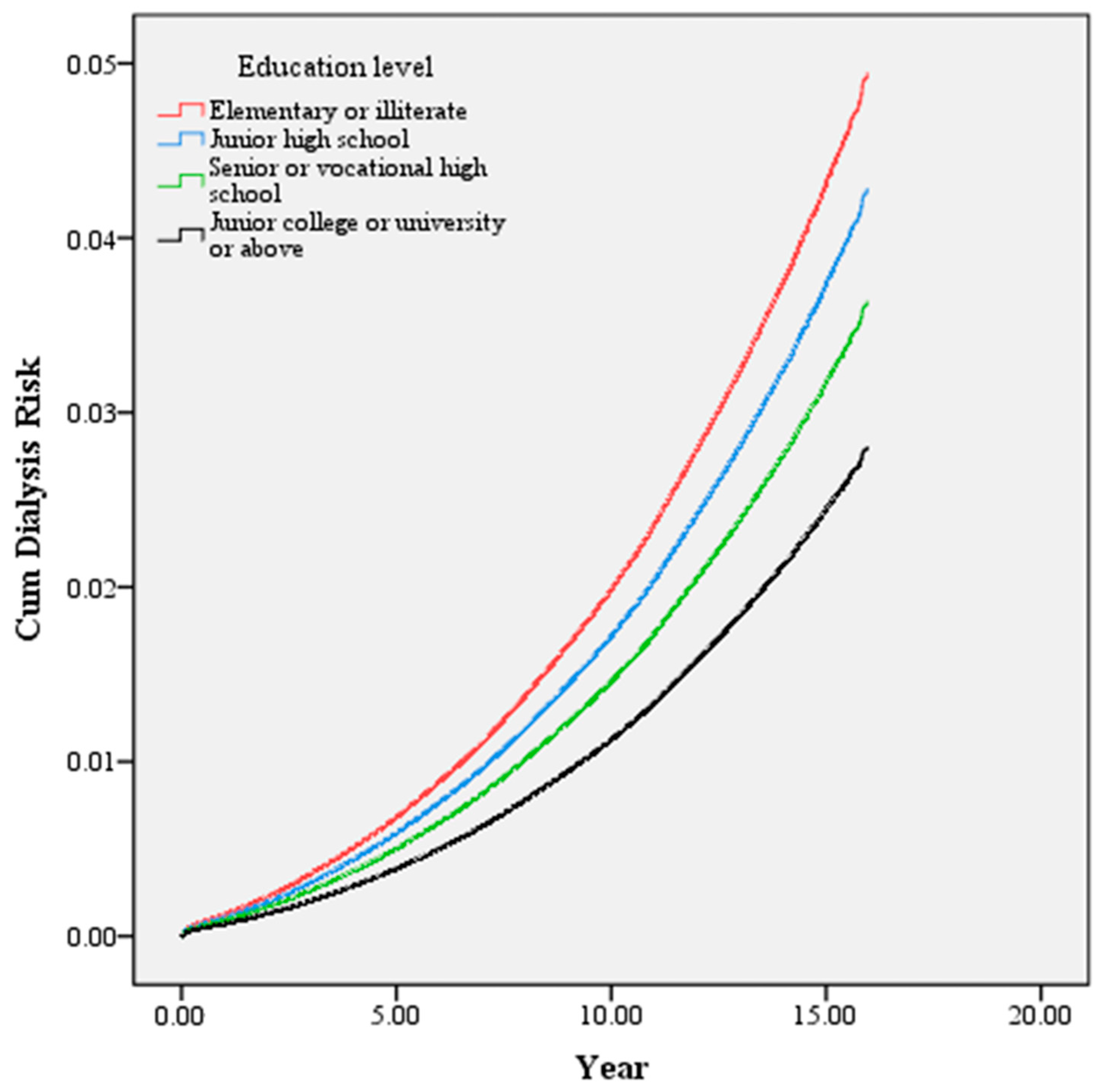
3.3. Educational Level Associated with the Risk of Dialysis in Diabetic Patients Participating and Not Participating in the Pay-for-Performance Program
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, R.; Karuranga, S.; Malanda, B.; Saeedi, P.; Basit, A.; Besançon, S.; Bommer, C.; Esteghamati, A.; Ogurtsova, K.; Colagiuri, S.; et al. Global and Regional Estimates and Projections of Diabetes-Related Health Expenditure: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2020, 162, 108072. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Katon, W.J.; et al. Diabetes Complications Severity Index and Risk of Mortality, Hospitalization, and Healthcare Utilization. Am. J. Manag. Care 2008, 14, 15–23. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3810070/ (accessed on 28 October 2013).
- Tien, K.-J.; Lin, Z.-Z.; Chio, C.-C.; Wang, J.-J.; Chu, C.-C.; Sun, Y.-M.; Kan, W.-C.; Chien, C.-C. Epidemiology and Mortality of New-Onset Diabetes after Dialysis: Taiwan National Cohort Study. Diabetes Care 2013, 36, 3027–3032. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020; pp. 12–15. Available online: https://www.cdc.gov/diabetes/data/statistics-report/coexisting-conditions-complications.html (accessed on 29 June 2022).
- Perkovic, V.; Heerspink, H.L.; Chalmers, J.; Woodward, M.; Jun, M.; Li, Q.; MacMahon, S.; Cooper, M.E.; Hamet, P.; Marre, M.; et al. Intensive Glucose Control Improves Kidney Outcomes in Patients with Type 2 Diabetes. Kidney Int. 2013, 83, 517–523. [Google Scholar] [CrossRef]
- Chang, P.-Y.; Chien, L.-N.; Lin, Y.-F.; Chiou, H.-Y.; Chiu, W.-T. Nonadherence of Oral Antihyperglycemic Medication Will Increase Risk of End-Stage Renal Disease. Medicine 2015, 94, e2051. [Google Scholar] [CrossRef]
- Hoogeveen, E.K. The Epidemiology of Diabetic Kidney Disease. Kidney Dial. 2022, 2, 433–442. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Bragg-Gresham, J.; Balkrishnan, R.; Bhave, N.; Dietrich, X.; Ding, Z.; Eggers, P.W.; et al. US Renal Data System 2018 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2019, 73, A7–A8. [Google Scholar] [CrossRef]
- Taiwan Society of Nephrology. 2021 Annual Report on Kidney Disease in Taiwan. Available online: https://www.tsn.org.tw/enVersion/TWRDS.aspx (accessed on 6 April 2021).
- Lai, T.-S.; Hsu, C.-C.; Lin, M.-H.; Wu, V.-C.; Chen, Y.-M. Trends in the Incidence and Prevalence of End-Stage Kidney Disease Requiring Dialysis in Taiwan: 2010–2018. J. Formos. Med. Assoc. 2022, 121, S5–S11. [Google Scholar] [CrossRef]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; De Boer, I.H. Kidney Disease and Increased Mortality Risk in Type 2 Diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef]
- Chiou, S.-T.; Lin, H.-D.; Yu, N.-C.; Hseuh, H.-K.; Lin, L.-H.; Lin, L.-T.; Chen, T.-J.; Lai, M.-S. An Initial Assessment of the Feasibility and Effectiveness of Implementing Diabetes Shared Care System in Taiwan—Some Experiences from I-Lan County. Diabetes Res. Clin. Pract. 2001, 54, 67–73. [Google Scholar] [CrossRef]
- Ryan, A.M.; Krinsky, S.; Kontopantelis, E.; Doran, T. Long-Term Evidence for the Effect of Pay-for-Performance in Primary Care on Mortality in the UK: A Population Study. Lancet 2016, 388, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Van Herck, P.; De Smedt, D.; Annemans, L.; Remmen, R.; Rosenthal, M.B.; Sermeus, W. Systematic Review: Effects, Design choices, and Context of Pay-for-Performance in Health Care. BMC Health Serv. Res. 2010, 10, 247. [Google Scholar] [CrossRef] [PubMed]
- Oluwatowoju, I.; Abu, E.; Wild, S.H.; Byrne, C.D. Improvements in Glycaemic Control and Cholesterol Concentrations Associated with the Quality and Outcomes Framework: A Regional 2-Year Audit of Diabetes Care in the UK. Diabet. Med. 2010, 27, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Alshamsan, R.; Millett, C.; Majeed, A.; Khunti, K. Has Pay for Performance Improved the Management of Diabetes in the United Kingdom? Prim. Care Diabetes 2010, 4, 73–78. [Google Scholar] [CrossRef]
- Cheng, S.H.; Lee, T.T.; Chen, C.C. A Longitudinal Examination of a Pay-for-Performance Program for Diabetes Care: Evidence from a Natural Experiment. Med. Care 2012, 50, 109–116. [Google Scholar] [CrossRef]
- Hsieh, H.-M.; Lin, T.-H.; Lee, I.-C.; Huang, C.-J.; Shin, S.-J.; Chiu, H.-C. The Association between Participation in a Pay-for-Performance Program and Macrovascular Complications in Patients with Type 2 Diabetes in Taiwan: A Nationwide Population-Based Cohort Study. Prev. Med. 2016, 85, 53–59. [Google Scholar] [CrossRef]
- Choi, A.I.; Weekley, C.C.; Chen, S.-C.; Li, S.; Tamura, M.K.; Norris, K.C.; Shlipak, M.G. Association of Educational Attainment with Chronic Disease and Mortality: The Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2011, 58, 228–234. [Google Scholar] [CrossRef]
- Hummer, R.A.; Lariscy, J.T. Educational Attainment and Adult Mortality. In International Handbook of Adult Mortality; Springer: Berlin/Heidelberg, Germany, 2011; pp. 241–261. [Google Scholar] [CrossRef]
- Ross, C.E.; Wu, C.-L. The Links between Education and Health. Am. Sociol. Rev. 1995, 60, 719. [Google Scholar] [CrossRef]
- Doshi, T.; Smalls, B.L.; Williams, J.S.; Wolfman, T.E.; Egede, L.E. Socioeconomic Status and Cardiovascular Risk Control in Adults with Diabetes. Am. J. Med. Sci. 2016, 352, 36–44. [Google Scholar] [CrossRef]
- Lai, Y.-J.; Hu, H.-Y.; Lee, Y.-L.; Ku, P.-W.; Yen, Y.-F.; Chu, D. A Retrospective Cohort Study on the Risk of Stroke in Relation to a Priori Health Knowledge Level among People with Type 2 Diabetes Mellitus in Taiwan. BMC Cardiovasc. Disord. 2017, 17, 130. [Google Scholar] [CrossRef]
- Saydah, S.H.; Imperatore, G.; Beckles, G.L. Socioeconomic Status and Mortality: Contribution of Health Care Access and Psychological Distress among Us Adults with Diagnosed Diabetes. Diabetes Care 2012, 36, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Saydah, S.; Lochner, K. Socioeconomic Status and Risk of Diabetes-Related Mortality in the U.S. Public Health Rep. 2010, 125, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-C.; Kung, P.-T.; Chiu, L.-T.; Liao, Y.P.; Tsai, W.-C. Patients with Diabetes in Pay-for-Performance Programs Have Better Physician Continuity of Care and Survival. Am. J. Manag. Care 2017, 23, e57–e66. [Google Scholar] [PubMed]
- Chang, C.H.; Shau, W.Y.; Jiang, Y.D.; Li, H.Y.; Chang, T.J.; Sheu, W.H.; Kwok, C.F.; Ho, L.T.; Chuang, L.M. Type 2 Diabetes Prevalence and Incidence among Adults in Taiwan during 1999–2004: A National Health Insurance Data Set Study. Diabet. Med. 2010, 27, 636–643. [Google Scholar] [CrossRef]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a Clinical Comorbidity Index for Use with ICD-9-cm Administrative Databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Berthoux, F.; Mohey, H.; Laurent, B.; Mariat, C.; Afiani, A.; Thibaudin, L. Predicting the Risk for Dialysis or Death in IgA Nephropathy. J. Am. Soc. Nephrol. 2011, 22, 752–761. [Google Scholar] [CrossRef]
- Bakris, G.L.; Weir, M.R.; Shanifar, S.; Zhang, Z.; Douglas, J.; van Dijk, D.J.; Brenner, B.M.; RENAAL Study Group. Effects of Blood Pressure Level on Progression of Diabetic Nephropathy: Results from the RENAAL Study. Arch. Intern. Med. 2003, 163, 1555–1565. [Google Scholar] [CrossRef]
- Sandhu, S.; Wiebe, N.; Fried, L.F.; Tonelli, M. Statins for Improving Renal Outcomes: A Meta-Analysis. J. Am. Soc. Nephrol. 2006, 17, 2006. [Google Scholar] [CrossRef]
- Mühlfeld, A.S.; Spencer, M.W.; Hudkins, K.L.; Kirk, E.; Leboeuf, R.C.; Alpers, C.E. Hyperlipidemia Aggravates Renal Disease in B6.ROP Os/+ mice. Kidney Int. 2004, 66, 1393–1402. [Google Scholar] [CrossRef]
- Fleischer, N.L.; Henderson, A.K.; Wu, Y.-H.; Liese, A.D.; McLain, A.C. Disparities in Diabetes by Education and Race/Ethnicity in the U.S., 1973–2012. Am. J. Prev. Med. 2016, 51, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration. Diabetes Prevalence. 2017. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1126&pid=1765 (accessed on 24 January 2017).
- Agardh, E.; Allebeck, P.; Hallqvist, J.; Moradi, T.; Sidorchuk, A. Type 2 Diabetes Incidence and Socio-Economic Position: A Systematic Review and Meta-Analysis. Leuk. Res. 2011, 40, 804–818. [Google Scholar] [CrossRef]
- Borrell, L.N.; Dallo, F.J.; White, K. Education and Diabetes in a Racially and Ethnically Diverse Population. Am. J. Public Health 2006, 96, 1637–1642. [Google Scholar] [CrossRef] [PubMed]
- Sacerdote, C.; Ricceri, F.; Rolandsson, O.; Baldi, I.; Chirlaque, M.-D.; Feskens, E.; Bendinelli, B.; Ardanaz, E.; Arriola, L.; Balkau, B.; et al. Lower Educational Level Is a Predictor of Incident Type 2 Diabetes in European Countries: The Epic-Interact Study. Int. J. Epidemiol. 2012, 41, 1162–1173. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.-E.; Lin, S.-P.; Aron, D.C. A Pay-for-Performance Program in Taiwan Improved Care for Some Diabetes Patients, but Doctors May Have Excluded Sicker Ones. Health Aff. 2012, 31, 93–102. [Google Scholar] [CrossRef]
- Do, Y.K.; Eggleston, K.N. Educational Disparities in Quality of Diabetes Care in a Universal Health Insurance System: Evidence from the 2005 Korea National Health and Nutrition Examination Survey. Int. J. Qual. Health Care 2011, 23, 397–404. [Google Scholar] [CrossRef]
- Duong, V.T.; Lin, I.-F.; Sorensen, K.; Pelikan, J.M.; Broucke, S.V.D.; Lin, Y.-C.; Chang, P.W. Health Literacy in Taiwan: A Population-Based Study. Asia Pac. J. Public Health 2015, 27, 871–880. [Google Scholar] [CrossRef]
- Huang, C.-H.; Talley, P.C.; Lin, C.-W.; Huang, R.-Y.; Liu, I.-T.; Chiang, I.-H.; Lu, I.-C.; Lai, Y.-C.; Kuo, K.-M. Factors Associated with Low Health Literacy among Community-Dwelling Women in Taiwan. Women Health 2020, 60, 487–501. [Google Scholar] [CrossRef]
- Wei, M.-H. The Associations between Health Literacy, Reasons for Seeking Health Information, and Information Sources Utilized by Taiwanese Adults. Health Educ. J. 2014, 73, 423–434. [Google Scholar] [CrossRef]
- Chen, T.; Chung, K.; Lin, I.; Lai, M. The Unintended Consequence of Diabetes Mellitus Pay-for-Performance (P4p) Program in Taiwan: Are Patients with More Comorbidities or More Severe Conditions Likely to Be Excluded from the P4p Program? Health Serv. Res. 2011, 46, 47–60. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Springate, D.A.; Ashcroft, D.M.; Valderas, J.M.; van der Veer, S.N.; Reeves, D.; Guthrie, B.; Doran, T. Associations between Exemption and Survival Outcomes in the UK’s Primary Care Pay-for-Performance Programme: A Retrospective Cohort Study. BMJ Qual. Saf. 2016, 25, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Shahbazian, H.; Rezaii, I. Diabetic Kidney Disease; Review of the Current Knowledge. J. Renal Inj. Prev. 2013, 2, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Selby, N.M.; Taal, M.W. An Updated Overview of Diabetic Nephropathy: Diagnosis, Prognosis, Treatment Goals and Latest Guidelines. Diabetes Obes. Metab. 2020, 22, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Roshan, B.; Stanton, R.C. A Story of Microalbuminuria and Diabetic Nephropathy. J. Nephropathol. 2013, 2, 234–240. [Google Scholar] [CrossRef]
- Samsu, N. Diabetic Nephropathy: Challenges in Pathogenesis, Diagnosis, and Treatment. BioMed Res. Int. 2021, 2021, 1–17. [Google Scholar] [CrossRef]
- Shih, H.-M.; Tsai, W.-C.; Wu, P.-Y.; Chiu, L.-T.; Kung, P.-T. Risk of Rapid Progression to Dialysis in Patients with Type 2 Diabetes Mellitus with and without Diabetes-Related Complications at Diagnosis. Sci. Rep. 2023, 13, 1–12. [Google Scholar] [CrossRef]
- So, W.Y.; Kong, A.P.; Ma, R.C.; Ozaki, R.; Szeto, C.C.; Chan, N.N.; Ng, V.; Ho, C.S.; Lam, C.W.; Chow, C.C.; et al. Glomerular Filtration Rate, Cardiorenal End Points, and All-Cause Mortality in Type 2 Diabetic Patients. Diabetes Care 2006, 29, 2046–2052. [Google Scholar] [CrossRef]
- Andrésdóttir, G.; Jensen, M.L.; Carstensen, B.; Parving, H.-H.; Rossing, K.; Hansen, T.W.; Rossing, P. Improved Survival and Renal Prognosis of Patients with Type 2 Diabetes and Nephropathy with Improved Control of Risk Factors. Diabetes Care 2014, 37, 1660–1667. [Google Scholar] [CrossRef]
- Poulimeneas, D.; Grammatikopoulou, M.G.; Bougioukli, V.; Iosifidou, P.; Vasiloglou, M.F.; Gerama, M.-A.; Mitsos, D.; Chrysanthakopoulou, I.; Tsigga, M.; Kazakos, K. Diabetes Knowledge among Greek Type 2 Diabetes Mellitus Patients. Endocrinol. Nutr.(Ed. Impr.) 2016, 63, 320–326. [Google Scholar] [CrossRef]
- Bains, S.S.; Egede, L.E.; Thurston, M.M.; Bourg, C.A.; Phillips, B.B.; Huston, S.A.; Osborn, C.Y.; Pereira, K.; Johnson, C.; Vorderstrasse, A.; et al. Associations Between Health Literacy, Diabetes Knowledge, Self-Care Behaviors, and Glycemic Control in a Low Income Population with Type 2 Diabetes. Diabetes Technol. Ther. 2011, 13, 335–341. [Google Scholar] [CrossRef]
- Brown, A.F.; Ettner, S.L.; Piette, J.; Weinberger, M.; Gregg, E.; Shapiro, M.F.; Karter, A.J.; Safford, M.; Waitzfelder, B.; Prata, P.A.; et al. Socioeconomic Position and Health among Persons with Diabetes Mellitus: A Conceptual Framework and Review of the Literature. Epidemiol. Rev. 2004, 26, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Liu, J.; Tao, S.; Hong, H.G.; Li, Y.; Fu, P. Associations between Socioeconomic Status and Chronic Kidney Disease: A Meta-Analysis. J. Epidemiol. Community Health 2018, 72, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, S.; Cai, X.; Adhikari, A.; Kershaw, K.; Peralta, C.A.; Kramer, H.; Jacobs, D.R.; Gutierrez, O.M.; Carnethon, M.R.; Isakova, T. Association of Educational Attainment with Incidence of Ckd in Young Adults. Kidney Int. Rep. 2020, 5, 2256–2263. [Google Scholar] [CrossRef] [PubMed]
- Duru, O.K.; Middleton, T.; Tewari, M.K.; Norris, K. The Landscape of Diabetic Kidney Disease in the United States. Curr. Diabetes Rep. 2018, 18, 14. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Tai, T.-Y. Long-Term Glycemic Control By a Diabetes Case-Management Program and the Challenges of Diabetes Care in Taiwan. Diabetes Res. Clin. Pract. 2014, 106, S328–S332. [Google Scholar] [CrossRef]
- Yuan, S.-P.; Huang, C.-N.; Liao, H.-C.; Lin, Y.-T.; Wang, Y.-H. Glycemic Control Outcomes by Gender in the Pay-for-Performance System: A Retrospective Database Analysis in Patients with Type 2 Diabetes Mellitus. Int. J. Endocrinol. 2014, 2014, 1–11. [Google Scholar] [CrossRef]
- Liao, P.-J.; Lin, T.-Y.; Wang, T.-C.; Ting, M.-K.; Wu, I.-W.; Huang, H.-T.; Wang, F.-C.; Chang, H.-C.; Hsu, K.-H. Long-Term and Interactive Effects of Pay-for-Performance Interventions among Diabetic Nephropathy Patients at the Early Chronic Kidney Disease Stage. Medicine 2016, 95, e3282. [Google Scholar] [CrossRef]
- Lin, M.-T.; Hsu, C.-N.; Lee, C.-T.; Cheng, S.-H. Effect of a Pay-for-Performance Program on Renal Outcomes among Patients with Early-Stage Chronic Kidney Disease in Taiwan. Int. J. Health Policy Manag. 2021, 11, 1307–1315. [Google Scholar] [CrossRef]
- Dubay, L.C.; Lebrun, L.A. Health, Behavior, and Health Care Disparities: Disentangling the Effects of Income and Race in the United States. Int. J. Health Serv. 2012, 42, 607–625. [Google Scholar] [CrossRef]
- McCall, D.T.; Sauaia, A.; Hamman, R.F.; Reusch, J.E.; Barton, P. Are Low-Income Elderly Patients at Risk for Poor Diabetes Care? Diabetes Care 2004, 27, 1060–1065. [Google Scholar] [CrossRef]
- Kim, S.H. Educational Attainment Moderates the Associations of Diabetes Education with Health Outcomes. Int. J. Nurs. Pract. 2016, 22, 444–450. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Non P4P | P4P | Adjusted Model | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | N | % | n | % | n | % | p-Value a | aHR | 95% CI | p-Value b | ||
| Total | 1,307,963 | 100 | 823,551 | 62.96 | 484,412 | 37.04 | ||||||
| Educational level | <0.001 | |||||||||||
| Illiteracy or elementary school (ref) | 667,419 | 51.03 | 435,690 | 65.28 | 231,729 | 34.72 | 1.00 | - | - | - | ||
| Junior high school | 255,585 | 19.54 | 154,835 | 60.58 | 100,750 | 39.42 | 1.13 | 1.12 | 1.14 | <0.001 | ||
| Senior high school | 266,363 | 20.36 | 159,181 | 59.76 | 107,182 | 40.24 | 1.13 | 1.13 | 1.14 | <0.001 | ||
| University or above | 118,596 | 9.07 | 73,845 | 62.27 | 44,751 | 37.73 | 1.05 | 1.03 | 1.06 | <0.001 | ||
| Gender | <0.001 | |||||||||||
| Male (ref) | 687,165 | 52.54 | 440,384 | 64.09 | 246,781 | 35.91 | 1.00 | - | - | - | ||
| Female | 620,798 | 47.46 | 383,167 | 61.72 | 237,631 | 38.28 | 1.01 | 1.00 | 1.02 | 0.001 | ||
| Age | <0.001 | |||||||||||
| 45–54 years (ref) | 411,343 | 31.45 | 229,382 | 55.76 | 181,961 | 44.24 | 1.00 | - | - | - | ||
| 55–64 years | 425,315 | 32.52 | 252,601 | 59.39 | 172,714 | 40.61 | 1.07 | 1.06 | 1.08 | <0.001 | ||
| 65–74 years | 285,080 | 21.80 | 189,580 | 66.50 | 95,500 | 33.50 | 1.01 | 1.01 | 1.02 | 0.003 | ||
| ≥75 years | 186,225 | 14.24 | 151,988 | 81.62 | 34,237 | 18.38 | 0.84 | 0.83 | 0.85 | <0.001 | ||
| Marital status | <0.001 | |||||||||||
| Unmarried (ref) | 59,175 | 4.52 | 40,158 | 67.86 | 19,017 | 32.14 | 1.00 | - | - | - | ||
| Married | 957,399 | 73.20 | 584,331 | 61.03 | 373,068 | 38.97 | 1.01 | 1.00 | 1.03 | 0.092 | ||
| Divorced and Widowed | 291,389 | 22.28 | 199,062 | 68.31 | 92,327 | 31.69 | 1.03 | 1.01 | 1.04 | 0.001 | ||
| Monthly salary | <0.001 | |||||||||||
| ≤17,280 (ref) | 304,806 | 23.3 | 201,897 | 66.24 | 102,909 | 33.76 | 1.00 | - | - | - | ||
| 17,281–22,800 | 537,788 | 41.12 | 340,255 | 63.27 | 197,533 | 36.73 | 1.00 | 1.00 | 1.01 | 0.294 | ||
| 22,801–28,800 | 99,931 | 7.64 | 59,083 | 59.12 | 40,848 | 40.88 | 1.04 | 1.03 | 1.05 | <0.001 | ||
| 28,801–36,300 | 106,987 | 8.18 | 63,945 | 59.77 | 43,042 | 40.23 | 1.06 | 1.05 | 1.07 | <0.001 | ||
| 36,301–45,800 | 131,401 | 10.05 | 78,828 | 59.99 | 52,573 | 40.01 | 1.06 | 1.05 | 1.07 | <0.001 | ||
| ≥45,801 | 127,050 | 9.71 | 79,543 | 62.61 | 47,507 | 37.39 | 0.95 | 0.94 | 0.96 | <0.001 | ||
| Urbanization degree of residential area | <0.001 | |||||||||||
| 1 (ref) | 270,269 | 20.66 | 172,987 | 64.01 | 97,282 | 35.99 | 1.00 | - | - | - | ||
| 2 | 349,453 | 26.72 | 216,380 | 61.92 | 133,073 | 38.08 | 1.09 | 1.08 | 1.10 | <0.001 | ||
| 3 | 256,815 | 19.63 | 164,298 | 63.98 | 92,517 | 36.02 | 1.08 | 1.07 | 1.09 | <0.001 | ||
| 4 | 228,152 | 17.44 | 138,592 | 60.75 | 89,560 | 39.25 | 1.27 | 1.26 | 1.29 | <0.001 | ||
| 5 | 46,174 | 3.53 | 30,723 | 66.54 | 15,451 | 33.46 | 1.12 | 1.10 | 1.14 | <0.001 | ||
| 6 | 80,358 | 6.14 | 52,256 | 65.03 | 28,102 | 34.97 | 1.15 | 1.14 | 1.17 | <0.001 | ||
| 7 | 76,742 | 5.87 | 48,315 | 62.96 | 28,427 | 37.04 | 1.23 | 1.22 | 1.25 | <0.001 | ||
| CCI | <0.001 | |||||||||||
| 0 point (ref) | 764,242 | 58.43 | 449,852 | 58.86 | 314,390 | 41.14 | 1.00 | - | - | - | ||
| 1 point | 297,542 | 22.75 | 193,415 | 65.00 | 104,127 | 35.00 | 0.93 | 0.92 | 0.94 | <0.001 | ||
| 2 points | 132,498 | 10.13 | 91,301 | 68.91 | 41,197 | 31.09 | 0.91 | 0.90 | 0.92 | <0.001 | ||
| ≥3 points | 113,681 | 8.69 | 88,983 | 78.27 | 24,698 | 21.73 | 0.83 | 0.82 | 0.85 | <0.001 | ||
| DCSI | <0.001 | |||||||||||
| 0 point (ref) | 924,481 | 70.68 | 577,929 | 62.51 | 346,552 | 37.49 | 1.00 | - | - | - | ||
| 1 point | 183,817 | 14.05 | 102,490 | 55.76 | 81,327 | 44.24 | 1.27 | 1.26 | 1.28 | <0.001 | ||
| ≥2 points | 199,665 | 15.27 | 143,132 | 71.69 | 56,533 | 28.31 | 1.16 | 1.15 | 1.17 | <0.001 | ||
| Service volume of primary treatment physician | <0.001 | |||||||||||
| Low (ref) | 327,528 | 25.04 | 304,892 | 93.09 | 22,636 | 6.91 | 1.00 | - | - | - | ||
| Medium | 653,521 | 49.96 | 441,950 | 67.63 | 211,571 | 32.37 | 4.65 | 4.59 | 4.72 | <0.001 | ||
| High | 326,914 | 24.99 | 76,709 | 23.46 | 250,205 | 76.54 | 8.50 | 8.37 | 8.63 | <0.001 | ||
| Department of primary treatment physician | <0.001 | |||||||||||
| Endocrinology | 314,182 | 24.02 | 71,164 | 22.65 | 243,018 | 77.35 | 3.70 | 3.66 | 3.75 | <0.001 | ||
| Family medicine | 261,953 | 20.03 | 169,829 | 64.83 | 92,124 | 35.17 | 2.40 | 2.38 | 2.43 | <0.001 | ||
| Internal medicine | 256,494 | 19.61 | 167,565 | 65.33 | 88,929 | 34.67 | 2.18 | 2.15 | 2.20 | <0.001 | ||
| Other departments (ref) | 475,334 | 36.34 | 414,993 | 87.31 | 60,341 | 12.69 | 1.00 | - | - | - | ||
| Level of primary treatment medical institution | <0.001 | |||||||||||
| Medical center (ref) | 249,709 | 19.09 | 172,770 | 69.19 | 76,939 | 30.81 | 1.00 | - | - | - | ||
| Regional hospital | 320,825 | 24.53 | 205,177 | 63.95 | 115,648 | 36.05 | 1.20 | 1.19 | 1.21 | <0.001 | ||
| Local hospital | 207,602 | 15.87 | 129,958 | 62.60 | 77,644 | 37.40 | 1.43 | 1.42 | 1.45 | <0.001 | ||
| Primary clinic | 529,827 | 40.51 | 315,646 | 59.58 | 214,181 | 40.42 | 1.65 | 1.63 | 1.66 | <0.001 | ||
| Ownership of primary treatment medical institution | <0.001 | |||||||||||
| Public (ref) | 294,221 | 22.49 | 173,873 | 59.10 | 120,348 | 40.90 | 1.00 | - | - | - | ||
| Non-public | 1,013,742 | 77.51 | 649,678 | 64.09 | 364,064 | 35.91 | 0.88 | 0.87 | 0.88 | <0.001 | ||
| No Dialysis | Dialysis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | N | % | n | % | n | % | p-Value a | Observed Person-Years | Dialysis Rate Per Thousand Person-Years | p-Value b | |
| Total | 1,307,963 | 100 | 1,283,509 | 98.13 | 24,454 | 1.87 | 9,926,679 | 2.46 | |||
| Educational level | <0.001 | ||||||||||
| Illiteracy or elementary school (ref) | 667,419 | 51.03 | 652,890 | 97.82 | 14,529 | 2.18 | 5,216,353 | 2.79 | - | ||
| Junior high school | 255,585 | 19.54 | 250,975 | 98.20 | 4610 | 1.80 | 1,880,218 | 2.45 | <0.001 | ||
| Senior high school | 266,363 | 20.36 | 262,399 | 98.51 | 3964 | 1.49 | 1,957,429 | 2.03 | <0.001 | ||
| University or above | 118,596 | 9.07 | 117,245 | 98.86 | 1351 | 1.14 | 872,679 | 1.55 | <0.001 | ||
| P4P | <0.001 | ||||||||||
| Not participating (ref) | 823,551 | 62.96 | 806,537 | 97.93 | 17,014 | 2.07 | 5,672,503 | 3.00 | - | ||
| Participating | 484,412 | 37.04 | 476,972 | 98.46 | 7440 | 1.54 | 4,254,176 | 1.75 | <0.001 | ||
| Gender | <0.001 | ||||||||||
| Male | 687,165 | 52.54 | 672,880 | 97.92 | 14,285 | 2.08 | 5,068,670 | 2.82 | - | ||
| Female | 620,798 | 47.46 | 610,629 | 98.36 | 10,169 | 1.64 | 4,858,010 | 2.09 | <0.001 | ||
| Age | <0.001 | ||||||||||
| 45–54 years | 411,343 | 31.45 | 402,659 | 97.89 | 8684 | 2.11 | 3,472,436 | 2.50 | - | ||
| 55–64 years | 425,315 | 32.52 | 418,103 | 98.30 | 7212 | 1.70 | 3,320,146 | 2.17 | <0.001 | ||
| 65–74 years | 285,080 | 21.80 | 279,536 | 98.06 | 5544 | 1.94 | 2,147,769 | 2.58 | 0.066 | ||
| ≥75 years | 186,225 | 14.24 | 183,211 | 98.38 | 3014 | 1.62 | 986,327.3 | 3.06 | <0.001 | ||
| Marital status | <0.001 | ||||||||||
| Unmarried | 59,175 | 4.52 | 57,784 | 97.65 | 1391 | 2.35 | 386,415.6 | 3.60 | - | ||
| Married | 957,399 | 73.20 | 939,706 | 98.15 | 17,693 | 1.85 | 7,559,209 | 2.34 | <0.001 | ||
| Divorced and widowed | 291,389 | 22.28 | 286,019 | 98.16 | 5370 | 1.84 | 1,981,055 | 2.71 | <0.001 | ||
| Monthly salary | <0.001 | ||||||||||
| ≤17,280 | 304,806 | 23.3 | 297,759 | 97.69 | 7047 | 2.31 | 2,256,063 | 3.12 | - | ||
| 17,281–22,800 | 537,788 | 41.12 | 527,327 | 98.05 | 10,461 | 1.95 | 4,121,267 | 2.54 | <0.001 | ||
| 22,801–28,800 | 99,931 | 7.64 | 98,194 | 98.26 | 1737 | 1.74 | 798,308.7 | 2.18 | <0.001 | ||
| 28,801–36,300 | 106,987 | 8.18 | 105,350 | 98.47 | 1637 | 1.53 | 796,703.4 | 2.05 | <0.001 | ||
| 36,301–45,800 | 131,401 | 10.05 | 129,524 | 98.57 | 1877 | 1.43 | 973,800.3 | 1.93 | <0.001 | ||
| ≥45,801 | 127,050 | 9.71 | 125,355 | 98.67 | 1695 | 1.33 | 980,537.1 | 1.73 | <0.001 | ||
| Urbanization degree of residential area | <0.001 | ||||||||||
| 1 | 270,269 | 20.66 | 265,215 | 98.13 | 5054 | 1.87 | 2,119,262 | 2.38 | - | ||
| 2 | 349,453 | 26.72 | 342,999 | 98.15 | 6454 | 1.85 | 2,681,828 | 2.41 | 0.629 | ||
| 3 | 256,815 | 19.63 | 251,831 | 98.06 | 4984 | 1.94 | 1,931,752 | 2.58 | <0.001 | ||
| 4 | 228,152 | 17.44 | 223,900 | 98.14 | 4252 | 1.86 | 1,700,622 | 2.50 | 0.023 | ||
| 5 | 46,174 | 3.53 | 45,376 | 98.27 | 798 | 1.73 | 340,588.6 | 2.34 | 0.643 | ||
| 6 | 80,358 | 6.14 | 78,864 | 98.14 | 1494 | 1.86 | 590,833.1 | 2.53 | 0.047 | ||
| 7 | 76,742 | 5.87 | 75,324 | 98.15 | 1418 | 1.85 | 561,793.4 | 2.52 | 0.073 | ||
| CCI | <0.001 | ||||||||||
| 0 point | 764,242 | 58.43 | 750,564 | 98.21 | 13,678 | 1.79 | 6,106,230 | 2.24 | - | ||
| 1 point | 297,542 | 22.75 | 293,653 | 98.69 | 3889 | 1.31 | 2,297,878 | 1.69 | <0.001 | ||
| 2 points | 132,498 | 10.13 | 129,274 | 97.57 | 3224 | 2.43 | 917,316.6 | 3.51 | <0.001 | ||
| ≥3 points | 113,681 | 8.69 | 110,018 | 96.78 | 3663 | 3.22 | 605,254.8 | 6.05 | <0.001 | ||
| DCSI | <0.001 | ||||||||||
| 0 point | 924,481 | 70.68 | 914,023 | 98.87 | 10,458 | 1.13 | 7,309,283 | 1.43 | - | ||
| 1 point | 183,817 | 14.05 | 180,906 | 98.42 | 2911 | 1.58 | 1,423,628 | 2.04 | <0.001 | ||
| ≥2 points | 199,665 | 15.27 | 188,580 | 94.45 | 11,085 | 5.55 | 1,193,769 | 9.29 | <0.001 | ||
| Hypertension | |||||||||||
| No | 634,640 | 48.52 | 622,741 | 98.13 | 11,899 | 1.87 | 5,035,531 | 2.36 | - | ||
| Yes | 673,323 | 51.48 | 660,768 | 98.14 | 12,555 | 1.86 | 4,891,149 | 2.57 | <0.001 | ||
| Hyperlipemia | <0.001 | ||||||||||
| No | 1,242,365 | 94.98 | 1,218,719 | 98.10 | 23,646 | 1.90 | 9,440,726 | 2.50 | - | ||
| Yes | 65,598 | 5.02 | 64,790 | 98.77 | 808 | 1.23 | 485,952.9 | 1.66 | <0.001 | ||
| Service volume of primary treatment physician | <0.001 | ||||||||||
| Low | 327,528 | 25.04 | 320,713 | 97.92 | 6815 | 2.08 | 2,227,758 | 3.06 | - | ||
| Medium | 653,521 | 49.96 | 640,841 | 98.06 | 12,680 | 1.94 | 4,927,195 | 2.57 | <0.001 | ||
| High | 326,914 | 24.99 | 321,955 | 98.48 | 4959 | 1.52 | 2,771,726 | 1.79 | <0.001 | ||
| Level of primary treatment medical institution | <0.001 | ||||||||||
| Medical center | 249,709 | 19.09 | 243,274 | 97.42 | 6435 | 2.58 | 1,880,848 | 3.42 | - | ||
| Regional hospital | 320,825 | 24.53 | 313,008 | 97.56 | 7817 | 2.44 | 2,454,255 | 3.19 | <0.001 | ||
| Local hospital | 207,602 | 15.87 | 203,346 | 97.95 | 4256 | 2.05 | 1,571,450 | 2.71 | <0.001 | ||
| Primary clinic | 529,827 | 40.51 | 523,881 | 98.88 | 5946 | 1.12 | 4,020,127 | 1.48 | <0.001 | ||
| Ownership of primary treatment medical institution | <0.001 | ||||||||||
| Public | 294,221 | 22.49 | 288,375 | 98.01 | 5846 | 1.99 | 2,282,277 | 2.56 | - | ||
| Non-public | 1,013,742 | 77.51 | 995,134 | 98.16 | 18,608 | 1.84 | 7,644,402 | 2.43 | 0.001 | ||
| Adjusted Model A | Adjusted Model B | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | aHR | 95% CI | p-Value | aHR | 95% CI | p-Value | |||
| Educational level | |||||||||
| Illiteracy or elementary school (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Junior high school | 0.87 | 0.84 | 0.90 | <0.001 | 0.87 | 0.83 | 0.91 | <0.001 | |
| Senior high school | 0.74 | 0.71 | 0.77 | <0.001 | 0.75 | 0.72 | 0.78 | <0.001 | |
| University or above | 0.57 | 0.54 | 0.60 | <0.001 | 0.59 | 0.55 | 0.63 | <0.001 | |
| P4P | |||||||||
| Not participating (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Participating | 0.71 | 0.69 | 0.73 | <0.001 | 0.72 | 0.69 | 0.75 | <0.001 | |
| Interaction | |||||||||
| P4P × Illiteracy or elementary school (ref) | 1.00 | - | - | - | |||||
| P4P × Junior high school | 1.00 | 0.93 | 1.07 | 0.979 | |||||
| P4P × Senior high school | 0.96 | 0.89 | 1.03 | 0.246 | |||||
| P4P × University or above | 0.88 | 0.78 | 1.00 | 0.054 | |||||
| Gender | |||||||||
| Male (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Female | 0.75 | 0.73 | 0.77 | <0.001 | 0.75 | 0.73 | 0.77 | <0.001 | |
| Age | |||||||||
| 45–54 years (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| 55–64 years | 0.77 | 0.75 | 0.80 | <0.001 | 0.77 | 0.75 | 0.80 | <0.001 | |
| 65–74 years | 0.73 | 0.70 | 0.76 | <0.001 | 0.73 | 0.71 | 0.76 | <0.001 | |
| ≥75 years | 0.69 | 0.66 | 0.72 | <0.001 | 0.69 | 0.66 | 0.72 | <0.001 | |
| Marital status | |||||||||
| Unmarried (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Married | 0.78 | 0.74 | 0.82 | <0.001 | 0.78 | 0.74 | 0.82 | <0.001 | |
| Divorce and widowed | 0.89 | 0.84 | 0.94 | <0.001 | 0.89 | 0.84 | 0.94 | <0.001 | |
| Monthly salary | |||||||||
| ≤17,280 (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| 17,281–22,800 | 0.86 | 0.83 | 0.89 | <0.001 | 0.86 | 0.83 | 0.89 | <0.001 | |
| 22,801–28,800 | 0.82 | 0.77 | 0.86 | <0.001 | 0.82 | 0.77 | 0.86 | <0.001 | |
| 28,801–36,300 | 0.80 | 0.76 | 0.85 | <0.001 | 0.80 | 0.76 | 0.85 | <0.001 | |
| 36,301–45,800 | 0.75 | 0.71 | 0.79 | <0.001 | 0.75 | 0.71 | 0.79 | <0.001 | |
| ≥45,801 | 0.71 | 0.67 | 0.75 | <0.001 | 0.71 | 0.67 | 0.75 | <0.001 | |
| Urbanization degree of residential area | |||||||||
| 1 (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| 2 | 1.04 | 1.00 | 1.08 | 0.041 | 1.04 | 1.00 | 1.08 | 0.038 | |
| 3 | 1.08 | 1.04 | 1.12 | <0.001 | 1.08 | 1.04 | 1.12 | <0.001 | |
| 4 | 1.05 | 1.01 | 1.10 | 0.021 | 1.05 | 1.01 | 1.10 | 0.019 | |
| 5 | 0.92 | 0.85 | 1.00 | 0.036 | 0.92 | 0.85 | 1.00 | 0.037 | |
| 6 | 1.02 | 0.96 | 1.08 | 0.587 | 1.02 | 0.96 | 1.08 | 0.573 | |
| 7 | 1.02 | 0.96 | 1.08 | 0.603 | 1.02 | 0.96 | 1.08 | 0.590 | |
| CCI | |||||||||
| 0 point (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| 1 point | 0.54 | 0.52 | 0.56 | <0.001 | 0.54 | 0.52 | 0.56 | <0.001 | |
| 2 points | 1.02 | 0.98 | 1.06 | 0.354 | 1.02 | 0.98 | 1.06 | 0.352 | |
| ≥3 points | 1.33 | 1.27 | 1.38 | <0.001 | 1.33 | 1.27 | 1.38 | <0.001 | |
| DCSI | |||||||||
| 0 point (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| 1 point | 1.48 | 1.42 | 1.54 | <0.001 | 1.48 | 1.42 | 1.54 | <0.001 | |
| ≥2 points | 6.24 | 6.06 | 6.42 | <0.001 | 6.24 | 6.06 | 6.43 | <0.001 | |
| Hypertension | |||||||||
| No (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Yes | 0.93 | 0.91 | 0.96 | <0.001 | 0.93 | 0.91 | 0.96 | <0.001 | |
| Hyperlipemia | |||||||||
| No (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Yes | 0.67 | 0.62 | 0.72 | <0.001 | 0.67 | 0.62 | 0.72 | <0.001 | |
| Service volume of primary treatment physician | |||||||||
| Low (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Medium | 0.88 | 0.85 | 0.90 | <0.001 | 0.88 | 0.85 | 0.90 | <0.001 | |
| High | 0.64 | 0.61 | 0.67 | <0.001 | 0.64 | 0.61 | 0.67 | <0.001 | |
| Level of primary treatment medical institution | |||||||||
| Medical center | 1.00 | - | - | - | 1.00 | - | - | - | |
| Regional hospital | 0.95 | 0.92 | 0.99 | 0.005 | 0.95 | 0.92 | 0.99 | 0.005 | |
| Local hospital | 0.79 | 0.76 | 0.82 | <0.001 | 0.79 | 0.76 | 0.82 | <0.001 | |
| Primary clinic | 0.49 | 0.47 | 0.50 | <0.001 | 0.49 | 0.47 | 0.50 | <0.001 | |
| Ownership of primary treatment medical institution | |||||||||
| Public (ref) | 1.00 | - | - | - | 1.00 | - | - | - | |
| Non-public | 1.05 | 1.02 | 1.08 | 0.001 | 1.05 | 1.02 | 1.08 | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-S.; Tsai, W.-C.; Chiu, L.-T.; Kung, P.-T. Diabetes Pay-for-Performance Program Participation and Dialysis Risk in Relation to Educational Attainment: A Retrospective Cohort Study. Healthcare 2023, 11, 2913. https://doi.org/10.3390/healthcare11222913
Tsai Y-S, Tsai W-C, Chiu L-T, Kung P-T. Diabetes Pay-for-Performance Program Participation and Dialysis Risk in Relation to Educational Attainment: A Retrospective Cohort Study. Healthcare. 2023; 11(22):2913. https://doi.org/10.3390/healthcare11222913
Chicago/Turabian StyleTsai, Yi-Shiun, Wen-Chen Tsai, Li-Ting Chiu, and Pei-Tseng Kung. 2023. "Diabetes Pay-for-Performance Program Participation and Dialysis Risk in Relation to Educational Attainment: A Retrospective Cohort Study" Healthcare 11, no. 22: 2913. https://doi.org/10.3390/healthcare11222913
APA StyleTsai, Y.-S., Tsai, W.-C., Chiu, L.-T., & Kung, P.-T. (2023). Diabetes Pay-for-Performance Program Participation and Dialysis Risk in Relation to Educational Attainment: A Retrospective Cohort Study. Healthcare, 11(22), 2913. https://doi.org/10.3390/healthcare11222913