


Technologies for Managing the Health of Older Adults with Multiple Chronic Conditions: A Systematic Literature Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Systematic Literature Review Methodology
2.1. Question Formulation
2.2. Locating Studies
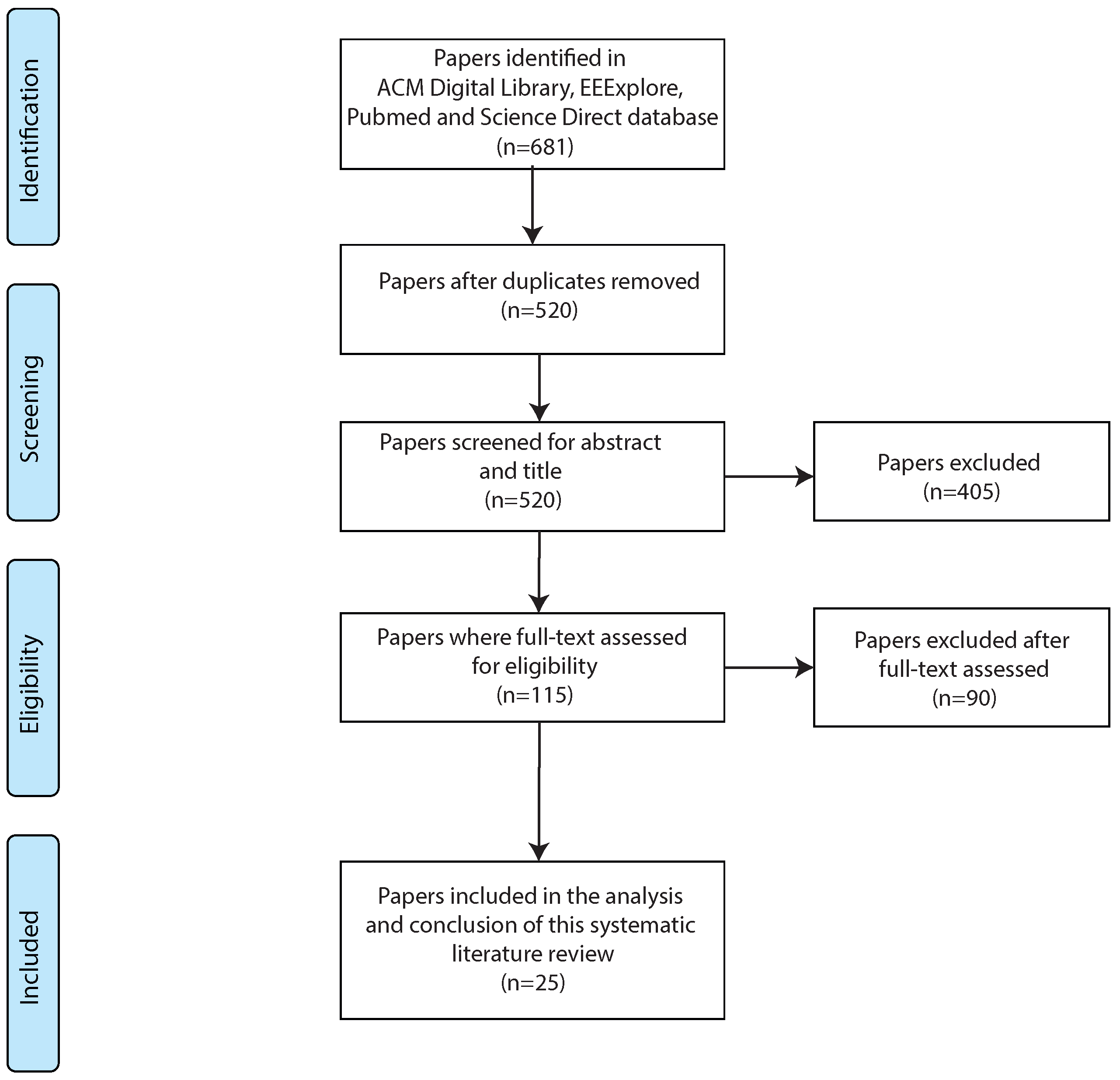
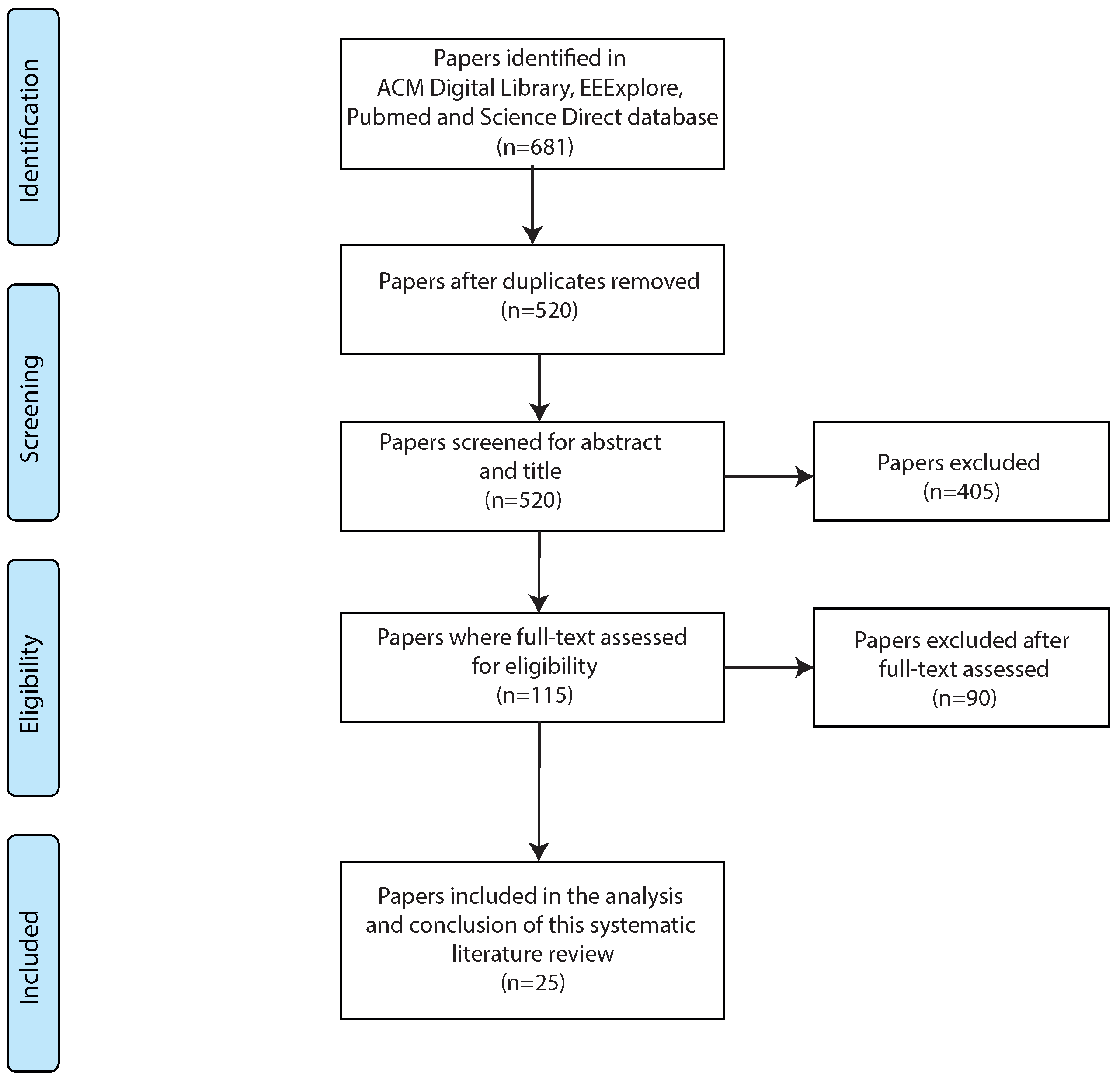
2.3. Study Selection and Evaluation
2.4. Analysis and Synthesis
2.5. Reporting and Using Results
3. Results
3.1. RQ1: Which Types of Technologies Have Been Developed to Support the Health Management of Older Adults with Multiple Health Conditions?
3.2. RQ2: What Are the Expected Health-Related Outcomes of Technological Interventions for Older Adults with Multimorbidity?
3.3. RQ3: How Are Technologies for Older Adults with Multiple Health Conditions Evaluated?
4. Discussion
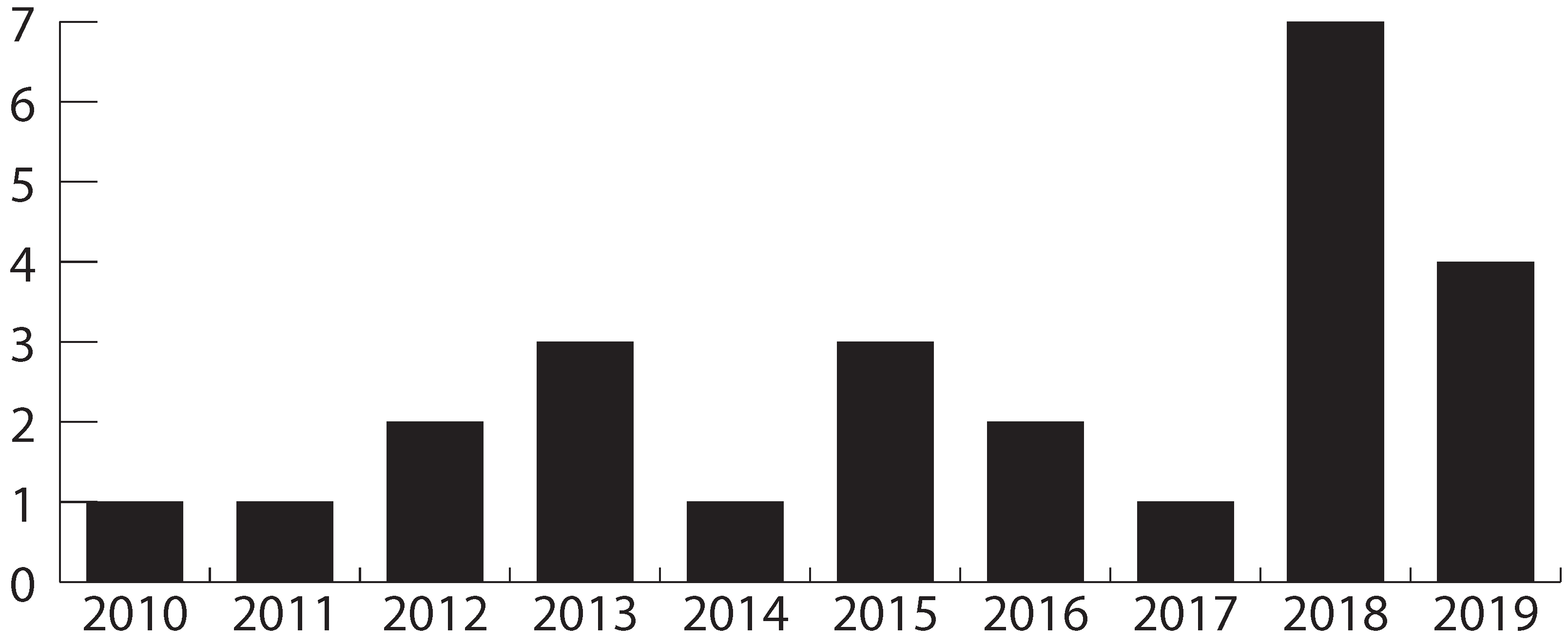
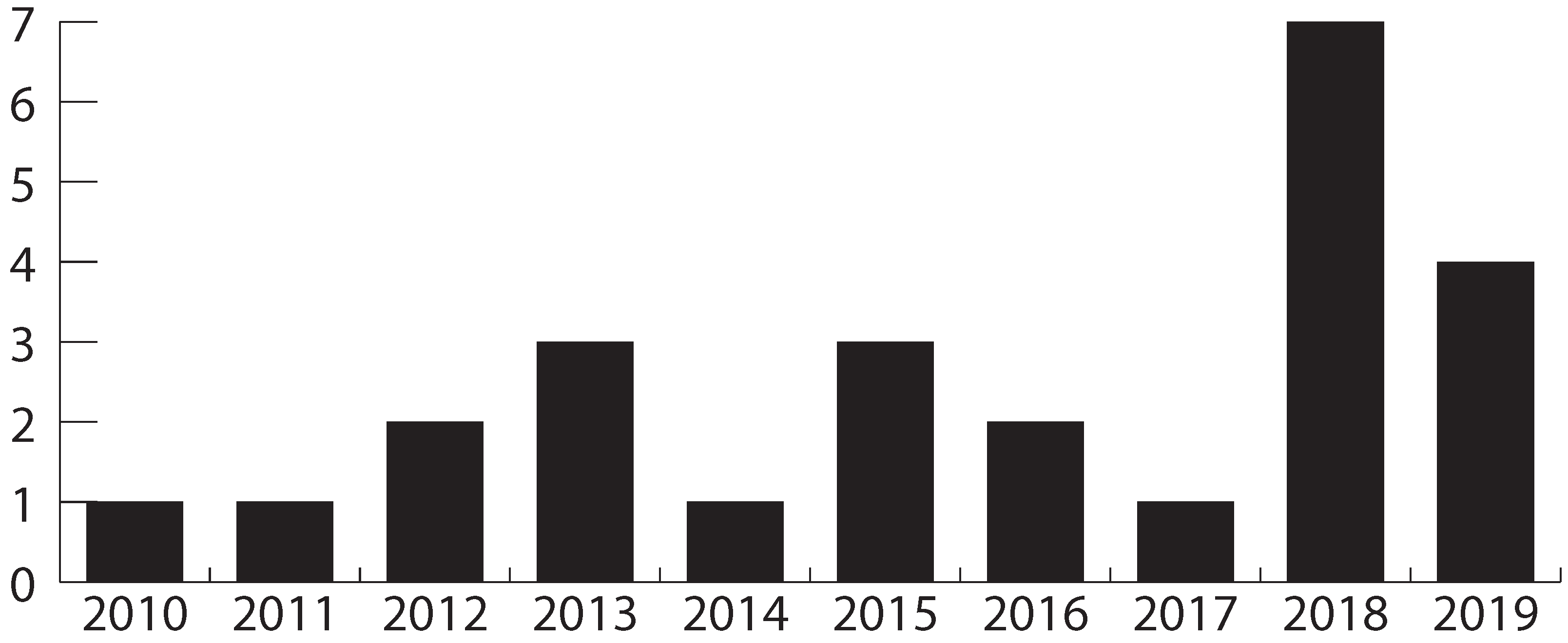
4.1. Literature Review Overview
4.2. Limitations
4.3. Requirements and Challenges for Interactive Health Technologies for Multimorbidity
4.3.1. Increasing Integration
4.3.2. Improving Ubiquity
4.3.3. Personalization
4.3.4. Older Adult-Centered Design
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SLR | Systematic Literature Review |
| RQ | Research Question |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PICOC | Population, Intervention, Comparisons, Results, Context |
| CDS | Clinical Decision Support |
References
- Sanderson, W.C.; Scherbov, S.; Gerland, P. Probabilistic population aging. PLoS ONE 2017, 12, e0179171. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Soubhi, H.; Hudon, C.; Bayliss, E.A.; Van den Akker, M. Multimorbidity’s many challenges. BMJ 2007, 334, 1016–1017. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Bravo, G.; Hudon, C.; Vanasse, A.; Lapointe, L. Prevalence of multimorbidity among adults seen in family practice. Ann. Fam. Med. 2005, 3, 223–228. [Google Scholar] [CrossRef]
- Lochner, K.A.; Goodman, R.A.; Posner, S.; Parekh, A. Multiple chronic conditions among Medicare beneficiaries: State-level variations in prevalence, utilization, and cost, 2011. Medicare Medicaid Res. Rev. 2013, 3, mmrr.003.03.b02. [Google Scholar] [CrossRef]
- Williams, J.S.; Egede, L.E. The association between multimorbidity and quality of life, health status and functional disability. Am. J. Med. Sci. 2016, 352, 45–52. [Google Scholar] [CrossRef]
- Ryan, A.; Wallace, E.; O’Hara, P.; Smith, S.M. Multimorbidity and functional decline in community-dwelling adults: A systematic review. Health Qual. Life Outcomes 2015, 13, 168. [Google Scholar] [PubMed]
- Wei, M.Y.; Mukamal, K.J. Multimorbidity, mortality, and long-term physical functioning in 3 prospective cohorts of community-dwelling adults. Am. J. Epidemiol. 2018, 187, 103–112. [Google Scholar]
- Townsend, A.; Hunt, K.; Wyke, S. Managing multiple morbidity in mid-life: A qualitative study of attitudes to drug use. BMJ 2003, 327, 837. [Google Scholar] [CrossRef]
- Ploeg, J.; Matthew-Maich, N.; Fraser, K.; Dufour, S.; McAiney, C.; Kaasalainen, S.; Markle-Reid, M.; Upshur, R.; Cleghorn, L.; Emili, A. Managing multiple chronic conditions in the community: A Canadian qualitative study of the experiences of older adults, family caregivers and healthcare providers. BMC Geriatr. 2017, 17, 40. [Google Scholar]
- Consorti, F.; Borcea, M.C.; Laca, A.; Melcarne, R.; Scorziello, C.; Ventrone, L.; Giacomelli, L. Education of clinical reasoning in patients with multimorbidity: A scoping review and perspectives for technology-enhanced learning. Front. Educ. 2023, 8, 1202360. [Google Scholar] [CrossRef]
- Gallacher, K.; May, C.R.; Montori, V.M.; Mair, F.S. Understanding patients’ experiences of treatment burden in chronic heart failure using normalization process theory. Ann. Fam. Med. 2011, 9, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Morrison, R.S. Research priorities in geriatric palliative care: An introduction to a new series. J. Palliat. Med. 2013, 16, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Zulman, D.M.; Jenchura, E.C.; Cohen, D.M.; Lewis, E.T.; Houston, T.K.; Asch, S.M. How can eHealth technology address challenges related to multimorbidity? Perspectives from patients with multiple chronic conditions. J. Gen. Intern. Med. 2015, 30, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Moran, O.; Doyle, J.; Smith, S.; Giggins, O.; Dinsmore, J. Investigating the needs and concerns of older adults with multimorbidity and their healthcare professionals for conceivable digital psychotherapeutic interventions. Digit. Health 2022, 8, 20552076221089097. [Google Scholar] [CrossRef]
- Dabbs, A.D.V.; Myers, B.A.; Mc Curry, K.R.; Dunbar-Jacob, J.; Hawkins, R.P.; Begey, A.; Dew, M.A. User-centered design and interactive health technologies for patients. Comput. Inform. Nurs. CIN 2009, 27, 175. [Google Scholar] [CrossRef]
- Tam, L.T.; Valera, A.C.; Tan, H.P.; Koh, C. Online detection of behavioral change using unobtrusive eldercare monitoring system. In Proceedings of the 11th International Conference on Queueing Theory and Network Applications, Wellington, New Zealand, 13–15 December 2016; pp. 1–8. [Google Scholar]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. Can Mobile Health Technologies Transform Health Care? JAMA 2013, 310, 2395–2396. [Google Scholar] [CrossRef]
- Stellefson, M.; Chaney, B.; Barry, A.E.; Chavarria, E.; Tennant, B.; Walsh-Childers, K.; Sriram, P.; Zagora, J. Web 2.0 chronic disease self-management for older adults: A systematic review. J. Med. Internet Res. 2013, 15, e35. [Google Scholar] [CrossRef]
- Whitlock, L.A.; McLaughlin, A.C.; Harris, M.; Bradshaw, J. The design of mobile technology to support diabetes self-management in older adults. In Human Aspects of IT for the Aged Population; Design for Everyday Life; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2015; Volume 9194, pp. 211–221. [Google Scholar]
- Searcy, R.P.; Summapund, J.; Estrin, D.; Pollak, J.P.; Schoenthaler, A.; Troxel, A.B.; Dodson, J.A. Mobile health technologies for older adults with cardiovascular disease: Current evidence and future directions. Curr. Geriatr. Rep. 2019, 8, 31–42. [Google Scholar] [CrossRef]
- Manning, S.E.; Wang, H.; Dwibedi, N.; Shen, C.; Wiener, R.C.; Findley, P.A.; Mitra, S.; Sambamoorthi, U. Association of multimorbidity with the use of health information technology. Digit. Health 2023, 9, 20552076231163797. [Google Scholar] [CrossRef]
- Matthew-Maich, N.; Harris, L.; Ploeg, J.; Markle-Reid, M.; Valaitis, R.; Ibrahim, S.; Gafni, A.; Isaacs, S. Designing, implementing, and evaluating mobile health technologies for managing chronic conditions in older adults: A scoping review. JMIR mHealth uHealth 2016, 4, e29. [Google Scholar] [CrossRef]
- Kim, B.Y.; Lee, J. Smart devices for older adults managing chronic disease: A scoping review. JMIR mHealth uHealth 2017, 5, e69. [Google Scholar] [CrossRef] [PubMed]
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef]
- Kitchenham, B.; Charters, S. Guidelines for Performing Systematic Literature Reviews in Software Engineering. Technical Report EBSE 2007-001, Keele University and Durham University Joint Report. 2007. Available online: https://www.elsevier.com/__data/promis_misc/525444systematicreviewsguide.pdf (accessed on 1 September 2023).
- Denyer, D.; Tranfield, D. Producing a systematic review. In The Sage Handbook of Organizational Research Methods; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.C.; Chiang, I.J.; Xiao, F.; Liao, C.C.; Liu, C.C.H.; Wong, J.M. PICO element detection in medical text without metadata: Are first sentences enough? J. Biomed. Inform. 2013, 46, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Kot, S.; Kurkiewicz, J. The new measures of the population ageing. Stud. Demogr. 2004, 2, 17–29. [Google Scholar]
- World Health Organization. Definition of an Older or Elderly Person; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Burnette, R.; Simmons, L.A.; Snyderman, R. Personalized health care as a pathway for the adoption of genomic medicine. J. Pers. Med. 2012, 2, 232–240. [Google Scholar] [CrossRef]
- Fortuna, K.L.; DiMilia, P.R.; Lohman, M.C.; Bruce, M.L.; Zubritsky, C.D.; Halaby, M.R.; Walker, R.M.; Brooks, J.M.; Bartels, S.J. Feasibility, acceptability, and preliminary effectiveness of a peer-delivered and technology supported self-management intervention for older adults with serious mental illness. Psychiatr. Q. 2018, 89, 293–305. [Google Scholar] [CrossRef]
- Vos, J.; Gerling, K.; Linehan, C.; Siriwardena, A.N.; Windle, K. Understanding care navigation by older adults with multimorbidity: Mixed-methods study using social network and framework analyses. JMIR Aging 2018, 1, e11054. [Google Scholar] [CrossRef]
- Schmidt, S.; Behrens, J.; Lautenschlaeger, C.; Gaertner, B.; Luderer, C. Experiences with combined personal-online case management and the self-reliance of older people with multimorbidity living alone in private households: Results of an interpretative-hermeneutical analysis. Scand. J. Caring Sci. 2019, 33, 931–939. [Google Scholar] [CrossRef]
- Martínez-García, A.; Moreno-Conde, A.; Jódar-Sánchez, F.; Leal, S.; Parra, C. Sharing clinical decisions for multimorbidity case management using social network and open-source tools. J. Biomed. Inform. 2013, 46, 977–984. [Google Scholar] [CrossRef]
- Portz, J.D.; Bayliss, E.A.; Bull, S.; Boxer, R.S.; Bekelman, D.B.; Gleason, K.; Czaja, S. Using the technology acceptance model to explore user experience, intent to use, and use behavior of a patient portal among older adults with multiple chronic conditions: Descriptive qualitative study. J. Med. Internet Res. 2019, 21, e11604. [Google Scholar] [CrossRef] [PubMed]
- Berner, J.; Anderberg, P.; Rennemark, M.; Berglund, J. Case management for frail older adults through tablet computers and Skype. Inform. Health Soc. Care 2016, 41, 405–416. [Google Scholar] [CrossRef] [PubMed]
- de Jong, C.C.; Ros, W.J.; van Leeuwen, M.; Schrijvers, G. How professionals share an E-care plan for the elderly in primary care: Evaluating the use of an E-communication tool by different combinations of professionals. J. Med. Internet Res. 2016, 18, e304. [Google Scholar] [CrossRef]
- Siek, K.A.; Ross, S.E.; Khan, D.U.; Haverhals, L.M.; Cali, S.R.; Meyers, J. Colorado Care Tablet: The design of an interoperable Personal Health Application to help older adults with multimorbidity manage their medications. J. Biomed. Inform. 2010, 43, S22–S26. [Google Scholar] [CrossRef]
- Haverhals, L.M.; Lee, C.A.; Siek, K.A.; Darr, C.A.; Linnebur, S.A.; Ruscin, J.M.; Ross, S.E. Older adults with multi-morbidity: Medication management processes and design implications for personal health applications. J. Med. Internet Res. 2011, 13, e44. [Google Scholar] [CrossRef] [PubMed]
- Reeder, B.; Demiris, G.; Marek, K.D. Older adults’ satisfaction with a medication dispensing device in home care. Inform. Health Soc. Care 2013, 38, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Mertens, M.; Raepsaet, J.; Mondelaers, M.; Vanrumste, B.; Davis, J. Use of wearable technology to quantify fall risk in psychogeriatric environments: A feasability study. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 3187–3190. [Google Scholar]
- Tchalla, A.E.; Lachal, F.; Cardinaud, N.; Saulnier, I.; Bhalla, D.; Roquejoffre, A.; Rialle, V.; Preux, P.M.; Dantoine, T. Efficacy of simple home-based technologies combined with a monitoring assistive center in decreasing falls in a frail elderly population (results of the Esoppe study). Arch. Gerontol. Geriatr. 2012, 55, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Pires, G.; Correia, P.; Jorge, D.; Mendes, D.; Gomes, N.; Dias, P.; Ferreira, P.; Lopes, A.; Manso, A.; Almeida, L.; et al. VITASENIOR-MT: A telehealth solution for the elderly focused on the interaction with TV. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018; pp. 1–6. [Google Scholar]
- Murphy, E.; Doyle, J.; Hannigan, C.; Smith, S.; Kuiper, J.; Jacobs, A.; Hoogerwerf, E.J.; Desideri, L.; Fiordelmondo, V.; Maluccelli, L.; et al. Perceptions and Use of Technology to Support Older Adults with Multimorbidity. In Proceedings of the AAATE Conference, Sheffield, UK, 11–15 September 2017; pp. 160–167. [Google Scholar]
- Mangin, D.; Parascandalo, J.; Khudoyarova, O.; Agarwal, G.; Bismah, V.; Orr, S. Multimorbidity, eHealth and implications for equity: A cross-sectional survey of patient perspectives on eHealth. BMJ Open 2019, 9, e023731. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Agache, I.; Aliberti, M.; Angles, R.; Annesi-Maesano, I.; Anto, J.; Arnavielhe, S.; Asayag, E.; Bacci, E.; Bedbrook, A.; et al. Transfer of innovation on allergic rhinitis and asthma multimorbidity in the elderly (MACVIA-ARIA)-EIP on AHA Twinning Reference Site (GARD research demonstration project). Allergy 2018, 73, 77–92. [Google Scholar] [CrossRef]
- Levine, D.M.; Lipsitz, S.R.; Linder, J.A. Changes in everyday and digital health technology use among seniors in declining health. J. Gerontol. Ser. A 2018, 73, 552–559. [Google Scholar] [CrossRef]
- Doyle, J.; Murphy, E.; Hannigan, C.; Smith, S.; Bettencourt-Silva, J.; Dinsmore, J. Designing Digital Goal Support Systems for Multimorbidity Self-Management: Insights from Older Adults and their Care Network. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare, New York, NY, USA, 21–24 May 2018; pp. 168–177. [Google Scholar]
- Barron, J.S.; Finkelstein, J. Feasibility of providing personalized health information to older adults and their caregivers. In Proceedings of the 2013 IEEE Point-of-Care Healthcare Technologies (PHT), Bangalore, India, 16–18 January 2013; pp. 232–235. [Google Scholar]
- Greenhalgh, T.; Procter, R.; Wherton, J.; Sugarhood, P.; Hinder, S.; Rouncefield, M. What is quality in assisted living technology? The ARCHIE framework for effective telehealth and telecare services. BMC Med. 2015, 13, 91. [Google Scholar] [CrossRef] [PubMed]
- Valdivieso, B.; García-Sempere, A.; Sanfélix-Gimeno, G.; Faubel, R.; Librero, J.; Soriano, E.; Peiró, S.; GeChronic Group. The effect of telehealth, telephone support or usual care on quality of life, mortality and healthcare utilization in elderly high-risk patients with multiple chronic conditions. A prospective study. Med. Clin. 2018, 151, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Ancker, J.S.; Witteman, H.O.; Hafeez, B.; Provencher, T.; Van de Graaf, M.; Wei, E. “You get reminded you’re a sick person”: Personal data tracking and patients with multiple chronic conditions. J. Med. Internet Res. 2015, 17, e202. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.H.; Wu, H.C. A cloud medication safety support system using QR code and Web services for elderly outpatients. Technol. Health Care 2014, 22, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, J.T.; Fernandes-Taylor, S.; Barnes, M.L.; Tomsejova, A.; Saunders, R.S.; Kent, K.C. Conceptualizing smartphone use in outpatient wound assessment: Patients’ and caregivers’ willingness to use technology. J. Surg. Res. 2015, 198, 245–251. [Google Scholar] [CrossRef]
- Schulz, R.; Beach, S.R.; Ives, D.G.; Martire, L.M.; Ariyo, A.A.; Kop, W.J. Association between depression and mortality in older adults: The Cardiovascular Health Study. Arch. Intern. Med. 2000, 160, 1761–1768. [Google Scholar] [CrossRef]
- Bayliss, E.A.; Bonds, D.E.; Boyd, C.M.; Davis, M.M.; Finke, B.; Fox, M.H.; Glasgow, R.E.; Goodman, R.A.; Heurtin-Roberts, S.; Lachenmayr, S.; et al. Understanding the context of health for persons with multiple chronic conditions: Moving from what is the matter to what matters. Ann. Fam. Med. 2014, 12, 260–269. [Google Scholar] [CrossRef]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rios Rincon, A. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Bayliss, E.A.; Steiner, J.F.; Fernald, D.H.; Crane, L.A.; Main, D.S. Descriptions of barriers to self-care by persons with comorbid chronic diseases. Ann. Fam. Med. 2003, 1, 15–21. [Google Scholar] [CrossRef]
- Muth, C.; Blom, J.; Smith, S.; Johnell, K.; Gonzalez-Gonzalez, A.I.; Nguyen, T.S.; Brueckle, M.S.; Cesari, M.; Tinetti, M.; Valderas, J. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. J. Intern. Med. 2019, 285, 272–288. [Google Scholar] [CrossRef]
- Caldeira, C.; Gui, X.; Reynolds, T.L.; Bietz, M.; Chen, Y. Managing healthcare conflicts when living with multiple chronic conditions. Int. J. Hum.-Comput. Stud. 2021, 145, 102494. [Google Scholar] [CrossRef]
- Mitzner, T.L.; Boron, J.B.; Fausset, C.B.; Adams, A.E.; Charness, N.; Czaja, S.J.; Dijkstra, K.; Fisk, A.D.; Rogers, W.A.; Sharit, J. Older adults talk technology: Technology usage and attitudes. Comput. Hum. Behav. 2010, 26, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Hargittai, E.; Piper, A.M.; Morris, M.R. From internet access to internet skills: Digital inequality among older adults. Univers. Access Inf. Soc. 2019, 18, 881–890. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Criterion | Description | Keywords |
|---|---|---|
| Population | Older adults | Older, senior, elderly |
| Intervention | Health Management Technologies | Technology |
| Comparison | — | — |
| Outcomes | Effects on health | — |
| Context | Multiple health conditions | Multimorbidity, multiple chronic conditions, multiple diseases, comorbidity |
| Paper ID | Type of Technology | Multimorbidity Support | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mobile Application | Website | Wearable Sensors | Device | Medical Records | Communication | Treatment | Information Access | Medication Management | |
| [42] | Y | Y | |||||||
| [33] | Y | Y | Y | ||||||
| [34] | Y | Y | |||||||
| [46] | Y | Y | |||||||
| [45] | Y | ||||||||
| [35] | Y | Y | Y | ||||||
| [39] | Y | Y | |||||||
| [40] | Y | Y | |||||||
| [36] | Y | Y | Y | ||||||
| [37] | Y | Y | |||||||
| [41] | Y | Y | |||||||
| [31] | Y | Y | |||||||
| [32] | Y | Y | |||||||
| [47] | Y | Y | |||||||
| [48] | Y | Y | Y | ||||||
| [38] | Y | Y | Y | ||||||
| [49] | Y | ||||||||
| [50] | Y | Y | |||||||
| [44] | Y | Y | |||||||
| [51] | Y | ||||||||
| [52] | Y | Y | |||||||
| [53] | |||||||||
| [54] | Y | ||||||||
| [43] | Y | ||||||||
| [55] | Y | ||||||||
| Study | How Does Technology Support Multimorbidity? |
|---|---|
| [33] | Healthcare and social care systems integrated navigation and communication support |
| [34] | Care and case management (CCM) using video conferencing |
| [35] | The care system integrated the social network component, called the Clinical Wall, and the Clinical Decision Support system. |
| [39] | Medication management application provides medication information retrieval, doctor visit preparation, and information on when to seek assistance. |
| [40] | System to provide links to medication information, facilitate communication between patients and physicians and pharmacists, and facility to selectively disclose medication information to different physicians. |
| [36] | Health portal that integrates e-mail, pharmacy and lab results. |
| [41] | Drug-handling device includes cognitive and sensory assistance |
| [31] | Personalized health care integrates appropriate personalized health technologies, standards of care and health planning |
| [32] | System with integrated medical and psychiatric self-management intervention. |
| [47] | Improved diagnosis by transferring clinical information (allergic rhinitis and asthma) from MACVIA-France’s EIP on AHA (Allergy Diary) to other sites. |
| [38] | System with care plan and a communication channel (in the registries the professionals interacted on the patients’ data). |
| [49] | System integrates goal setting, combined with progress feedback. |
| [44] | A television that records biometric parameters and displays health-related alerts and recommendations and environmental sensor logs. |
| [52] | Structured telephone support, with reminders and follow-up that allows remote self-management and transmission of clinical information. |
| [54] | System with medication reminders, pill dispensing assistance, medication log, medication position and forgotten medication alerts. |
| [43] | Fall arrest system included a light path along with the telecare service (the telecare service consisted of a remote intercom, an electronic bracelet). |
| [55] | System that allows taking photos, asking health-related questions and coordinating with caregivers. |
| Health Dimensions | Studies | Count |
|---|---|---|
| Social | [31,33,34,35,36,38,39,45,46,50,51], | 11 |
| Mental | [32,37,39,40,41,45,48,49,52,53,54] | 11 |
| Physical | [42,43,44,47,48,49,52,53,55] | 9 |
| Emotional | [31,36,51] | 3 |
| Environmental | [44] | 1 |
| Study | Methodology | Sample Size | Average Participant Age | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Quantitative | Qualitative | Mixed | 0–9 | 10–49 | 50–99 | >100 | 60–69 | 70–79 | 80–90 | |
| [42] | Y | Y | ||||||||
| [33] | Y | Y | ||||||||
| [34] | Y | Y | Y | |||||||
| [46] | Y | Y | ||||||||
| [45] | Y | Y | Y | |||||||
| [35] | Y | |||||||||
| [39] | Y | Y | Y | |||||||
| [40] | Y | Y | Y | |||||||
| [36] | Y | Y | Y | |||||||
| [37] | Y | Y | Y | |||||||
| [41] | Y | Y | ||||||||
| [32] | Y | Y | Y | |||||||
| [48] | Y | Y | ||||||||
| [38] | Y | |||||||||
| [49] | Y | Y | Y | |||||||
| [50] | Y | Y | Y | |||||||
| [51] | Y | Y | ||||||||
| [52] | Y | Y | Y | |||||||
| [53] | Y | Y | Y | |||||||
| [54] | Y | Y | Y | |||||||
| [43] | Y | Y | Y | |||||||
| [55] | Y | Y | Y | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cajamarca, G.; Proust, V.; Herskovic, V.; Cádiz, R.F.; Verdezoto, N.; Fernández, F.J. Technologies for Managing the Health of Older Adults with Multiple Chronic Conditions: A Systematic Literature Review. Healthcare 2023, 11, 2897. https://doi.org/10.3390/healthcare11212897
Cajamarca G, Proust V, Herskovic V, Cádiz RF, Verdezoto N, Fernández FJ. Technologies for Managing the Health of Older Adults with Multiple Chronic Conditions: A Systematic Literature Review. Healthcare. 2023; 11(21):2897. https://doi.org/10.3390/healthcare11212897
Chicago/Turabian StyleCajamarca, Gabriela, Valentina Proust, Valeria Herskovic, Rodrigo F. Cádiz, Nervo Verdezoto, and Francisco J. Fernández. 2023. "Technologies for Managing the Health of Older Adults with Multiple Chronic Conditions: A Systematic Literature Review" Healthcare 11, no. 21: 2897. https://doi.org/10.3390/healthcare11212897
APA StyleCajamarca, G., Proust, V., Herskovic, V., Cádiz, R. F., Verdezoto, N., & Fernández, F. J. (2023). Technologies for Managing the Health of Older Adults with Multiple Chronic Conditions: A Systematic Literature Review. Healthcare, 11(21), 2897. https://doi.org/10.3390/healthcare11212897