
Psychological Symptoms in Parents Who Experience Child-to-Parent Violence: The Role of Self-Efficacy Beliefs



Abstract
:1. Introduction
1.1. CPV and Psychological Symptoms in Parents
1.2. Victimization and Self-Efficacy Beliefs in Parents
1.3. The Present Study
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Measures
2.4. Data Analysis
3. Results
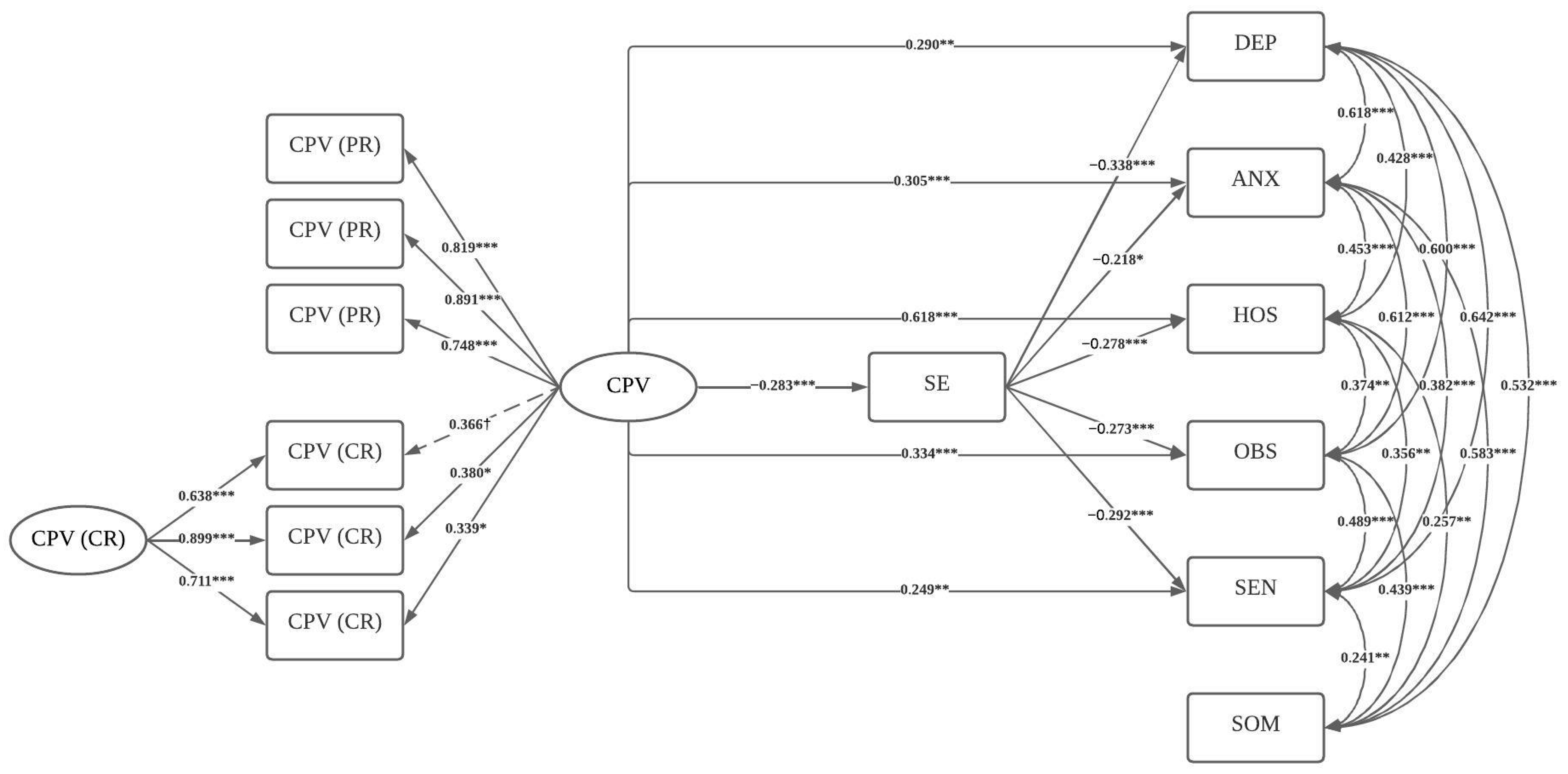
Associations between CPV, Self-Efficacy, and Psychological Symptoms
4. Discussion
Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simmons, M.; McEwan, T.E.; Purcell, R.; Ogloff, J.R.P. Sixty years of child-to-parent abuse research: What we know and where to go. Aggress. Violent Behav. 2018, 38, 31–52. [Google Scholar] [CrossRef]
- Arias-Rivera, S.; Hidalgo-Garcia, V. Theoretical framework and explanatory factors for child-to-parent violence. A scoping review. Anales de Psicología 2020, 36, 220–231. [Google Scholar] [CrossRef]
- Cottrell, B. Parent Abuse: The Abuse of Parents by Their Teenage Children; Family Violence Prevention Unit, Health Canada: Toronto, OR, Canada, 2001; p. 49. [Google Scholar]
- Paterson, R.; Luntz, H.; Perlesz, A.; Cotton, S. Adolescent violence towards parents: Maintaining family connections when the going gets tough. Aust. N. Z. J. Fam. 2002, 23, 90–100. [Google Scholar] [CrossRef]
- Calvete, E.; Jimenez-Granado, A.; Orue, I. The Revised Child-to-Parent Aggressions Questionnaire: An examination during the Covid-19 Pandemic. J. Fam. Violence 2023, 38, 1563–1576. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Loinaz, I.; Del Hoyo-Bilbao, J.; Arrospide, J.; Bertino, L.; Calvo, A.; Montes, Y.; Gutierrez, M.M. Proposal for a definition of filio-parental violence: Consensus of the Spanish Society for the Study of child-to-parent violence (SEVIFIP). Papeles del Psicólogo 2017, 38, 216–223. [Google Scholar] [CrossRef]
- Kennair, N.; Mellor, D. Parent abuse: A review. Child Psychiatry Hum. Dev. 2007, 38, 203–219. [Google Scholar] [CrossRef]
- Morán-Rodríguez, N.; González-Álvarez, M.; Gesteira-Santos, C.; García-Vera, M.P. Menores que agreden a sus padres: Análisis de los datos de prevalencia a nivel nacional e internacional. Psicopatol. Clin. Leg. Forense 2012, 12, 101–120. [Google Scholar]
- Beckmann, L.; Bergmann, M.C.; Fischer, F.; Mossle, T. Risk and protective factors of child-to-parent violence: A comparison between physical and verbal aggression. J. Interpers. Violence 2021, 36, NP1309–NP1334. [Google Scholar] [CrossRef]
- Ilabaca-Baeza, P.A.; Gaete-Fiscella, J.M. Adolescents who are violent toward their parents: An approach to the situation in Chile. J. Interpers. Violence 2021, 36, NP5678–NP5698. [Google Scholar] [CrossRef]
- Ibabe, I. A systematic review of youth-to-parent aggression: Conceptualization, typologies, and instruments. Front. Psychol. 2020, 11, 577757. [Google Scholar] [CrossRef]
- Calvete, E.; Orue, I.; Gonzalez-Cabrera, J. Child-to-parent violence: Comparing adolescent-reports with parent-reports. Revista De Psicologia Clinica Con Ninos Y Adolescentes 2017, 4, 9–15. [Google Scholar]
- Pagani, L.S.; Tremblay, R.E.; Nagin, D.; Zoccolillo, M.; Vitaro, F.; McDuff, P. Risk factor models for adolescent verbal and physical aggression toward mothers. Int. J. Behav. Dev. 2004, 28, 528–537. [Google Scholar] [CrossRef]
- Pagani, L.; Tremblay, R.E.; Nagin, D.; Zoccolillo, M.; Vitaro, F.; McDuff, P. Risk factor models for adolescent verbal and physical aggression toward fathers. J. Fam. Violence 2009, 24, 173–182. [Google Scholar] [CrossRef]
- Agnew, R.; Huguley, S. Adolescent violence toward parents. J. Marriage Fam. 1989, 51, 699–711. [Google Scholar] [CrossRef]
- Hong, J.S.; Kral, M.J.; Espelage, D.L.; Allen-Meares, P. The social ecology of adolescent-initiated parent abuse: A review of the literature. Child Psychiatry Hum. Dev. 2012, 43, 431–454. [Google Scholar] [CrossRef]
- Brule, N.J.; Eckstein, J.J. Am I really a bad parent?: Adolescent-to-Parent Abuse (AtPA) identity and the Stigma Management Communication (SMC) Model. J. Fam. Commun. 2016, 16, 198–215. [Google Scholar] [CrossRef]
- Gardner, M.J.; Thomas, H.J.; Erskine, H.E. The association between five forms of child maltreatment and depressive and anxiety disorders: A systematic review and meta-analysis. Child Abuse Negl. 2019, 96, 104082. [Google Scholar] [CrossRef]
- Chan, C.H.; Tiwari, A.; Fong, D.Y.T.; Ho, P.C. Post-traumatic stress disorder among chinese women survivors of intimate partner violence: A review of the literature. Int. J. Nurs. Stud. 2010, 47, 918–925. [Google Scholar] [CrossRef]
- Dillon, G.; Hussain, R.; Loxton, D.; Rahman, S. Mental and physical health and intimate partner violence against women: A review of the literature. Int. J. Fam. Med. 2013, 2013, 313909. [Google Scholar] [CrossRef]
- Giovagnoli, G.; Postorino, V.; Fatta, L.M.; Sanges, V.; De Peppo, L.; Vassena, L.; De Rose, P.; Vicari, S.; Mazzone, L. Behavioral and emotional profile and parental stress in preschool children with autism spectrum disorder. Res. Dev. Disabil. 2015, 45–46, 411–421. [Google Scholar] [CrossRef]
- Portnoy, J.; Bedoya, A.; Wong, K.K.-Y. Child externalising and internalising behaviour and parental wellbeing during the Covid-19 pandemic. UCL Open Environ. 2022, 4, e040. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.K.; Seltzer, M.M.; Greenberg, J.S. Longitudinal effects of adaptability on behavior problems and maternal depression in families of adolescents with autism. J. Fam. Psychol. 2011, 25, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Falk, N.H.; Norris, K.; Quinn, M.G. The factors predicting stress, anxiety and depression in the parents of children with autism. J. Autism Dev. Disord. 2014, 44, 3185–3203. [Google Scholar] [CrossRef]
- Edenborough, M.; Jackson, D.; Mannix, J.; Wilkes, L.M. Living in the red zone: The experience of child-to-mother violence. Child Fam. Soc. Work 2008, 13, 464–473. [Google Scholar] [CrossRef]
- Holt, A.; Birchall, J. Their mum messed up and gran can’t afford to: Violence towards grandparent kinship carers and the implications for social work. Br. J. Soc. Work 2022, 52, 1231–1248. [Google Scholar] [CrossRef]
- Arias-Rivera, S.; Lorence, B.; Hidalgo-García, V. Parenting skills, family functioning and social support in situations of child-to-parent violence: A scoping review of the literature. J. Fam. Violence 2022, 37, 1147–1160. [Google Scholar] [CrossRef]
- Rutter, N. I’m meant to be his comfort blanket, not a punching bag—Ethnomimesis as an exploration of maternal child to parent violence in pre-adolescents. Qual. Soc. Work 2021, 20, 1317–1338. [Google Scholar] [CrossRef]
- Ulman, A.; Straus, M.A. Violence by children against mothers in relation to violence between parents and corporal punishment by parents. J. Comp. Fam. Stud. 2003, 34, 41–60. [Google Scholar] [CrossRef]
- Turner, H.A.; Finkelhor, D.; Ormrod, R. The effects of adolescent victimization on self-concept and depressive symptoms. Child Maltreat. 2010, 15, 76–90. [Google Scholar] [CrossRef]
- Alba, J.; Calvete, E.; Wante, L.; Van Beveren, M.L.; Braet, C. Early maladaptive schemas as moderators of the association between bullying victimization and depressive symptoms in adolescents. Cogn. Ther. Res. 2018, 42, 24–35. [Google Scholar] [CrossRef]
- Calvete, E.; Estevez, A.; Corral, S. Intimate partner violence and depressive symptoms in women: Cognitive schemas as moderators and mediators. Behav. Res. Ther. 2007, 45, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Trompeter, N.; Bussey, K.; Fitzpatrick, S. Cyber victimization and internalizing difficulties: The mediating roles of coping self-efficacy and emotion dysregulation. J. Abnorm. Child Psychol. 2018, 46, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, C.T.; Lynch, S.M.; Benight, C.C. The indirect effect of coping self-efficacy on the relation between sexual violence and PTSD symptoms. J. Interpers. Violence 2021, 36, 9996–10012. [Google Scholar] [CrossRef] [PubMed]
- Webermann, A.R.; Dardis, C.M.; Iverson, K.M. The role of general self-efficacy in intimate partner violence and symptoms of posttraumatic stress disorder among women veterans. J. Traum. Stress 2022, 35, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy—Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Glatz, T.; Buchanan, C.M. Change and predictors of change in parental self-efficacy from early to middle adolescence. Dev. Psychol. 2015, 51, 1367–1379. [Google Scholar] [CrossRef]
- Sevigny, P.R.; Loutzenhiser, L. Predictors of parenting self-efficacy in mothers and fathers of toddlers. Child Care Health Dev. 2010, 36, 179–189. [Google Scholar] [CrossRef]
- Glatz, T.; Buchanan, C.M. Exploring how adolescent boys’ and girls’ internalizing and externalizing behaviors impact parental self-efficacy: A vignette study. Fam. Relat. 2023, 72, 347–360. [Google Scholar] [CrossRef]
- Troutman, B.; Moran, T.E.; Arndt, S.; Johnson, R.F.; Chmielewski, M. Development of parenting self-efficacy in mothers of infants with high negative emotionality. Infant Ment. Health J. 2012, 33, 45–54. [Google Scholar] [CrossRef]
- Ardelt, M.; Eccles, J.S. Effects of mothers’ parental efficacy beliefs and promotive parenting strategies on inner-city youth. J. Fam. Issues 2001, 22, 944–972. [Google Scholar] [CrossRef]
- Albanese, A.M.; Russo, G.R.; Geller, P.A. The role of parental self-efficacy in parent and child well-being: A systematic review of associated outcomes. Child Care Health Dev. 2019, 45, 333–363. [Google Scholar] [CrossRef] [PubMed]
- Hamovitch, E.K.; Acri, M.C.; Bornheimer, L.A. An analysis of the relationship between parenting self-efficacy, the quality of parenting, and parental and child emotional health. J. Fam. Soc. Work 2019, 22, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Hastings, R.P.; Brown, T. Behavior problems of children with autism, parental self-efficacy, and mental health. Am. J. Ment. Retard. 2002, 107, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chang, C.; Lin, C.; Wang, L. An investigation of longitudinal associations between psychological distress and student victimization by teachers. J. Interpers. Violence 2023, 38, 3279–3297. [Google Scholar] [CrossRef]
- Anacona, C.; Gómez, J.A.M. Variables associated with dating violence victimization in Colombian adolescents. Pensamiento Psicológico 2021, 19, 1–12. [Google Scholar]
- Toro Tobar, R.A.; Alfaro Medina, D.M.; Juyó Mosuca, E.V.; Sandino Serrano, V. Rumiación cognitiva y afecto negativo como predictores diferenciales de los síntomas psicopatológicos internalizantes. [Cognitive rumination and negative affect as differential predictors of internalizing psychopathological symptoms]. Psychologia 2020, 14, 27–36. [Google Scholar] [CrossRef]
- Calvete, E.; Gamez-Guadix, M.; Orue, I.; Gonzalez-Diez, Z.; López de Arroyabe, L.; Sampedro, R.; Pereira, R.; Zubizarreta, A.; Borrajo, E. Brief report: The adolescent Child-to-Parent Aggression Questionnaire: An examination of aggressions against parents in Spanish adolescents. J. Adolesc. 2013, 36, 1077–1081. [Google Scholar] [CrossRef]
- Calvete, E.; Orue, I.; Gamez-Guadix, M.; Bushman, B.J. Predictors of child-to-parent aggression: A 3-year longitudinal study. Dev. Psychol. 2015, 51, 663–676. [Google Scholar] [CrossRef]
- Sandín, B.; Valiente, R.M.; Chorot, P.; Santed, M.A.; Lostao, L. SA-45: Forma abreviada del SCL-90. Psicothema 2008, 20, 290–296. [Google Scholar]
- Davison, M.L.; Bershadsky, B.; Bieber, J.; Silversmith, D.; Maruish, M.E.; Kane, R.L. Development of a brief, multidimensional, self-report instrument for treatment outcomes assessment in psychiatric settings: Preliminary findings. Assessment 1997, 4, 259–276. [Google Scholar] [CrossRef]
- Derogatis, L.R. SCL-90-R: Administration, Scoring and Procedures. Manual II for the Revised Version and Other Instruments of the Psychopathology Rating Scale Series, 2nd ed.; Clinical Psychometric Research: Towson, MD, USA, 1983. [Google Scholar]
- Alvarado, B.G.; Bonifacio, S.; Valdez-Medina, J.L.; González-Arratia, N. Analisis factorial confirmatorio del Cuestionario SA-45 en una muestra mexicana. Anales de Psicología 2012, 28, 426–433. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. Measurement of Perceived Self-Efficacy. Psychometric Scales for Cross-Cultural Research; Freie Universität Berlin: Berlin, Germany, 1993. [Google Scholar]
- Baessler, J.; Schwarzer, R. Evaluación de la autoeficacia: Adaptación española de la Escala de Autoeficacia general. Ansiedad y Estrés 1996, 2, 1–8. [Google Scholar]
- Sanjuán-Suarez, P.; Pérez-García, A.M.; Bermúdez-Moreno, J. The general self-efficacy scale: Psychometric data from the Spanish adaptation. Psicothema 2000, 12, 509–513. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2021. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Eid, M. A multitrait-multimethod model with minimal assumptions. Psychometrika 2000, 65, 241–261. [Google Scholar] [CrossRef]
- Geiser, C.; Simmons, T.G. Do method effects generalize across traits (and what if they don’t)? J. Pers. 2021, 89, 382–401. [Google Scholar] [CrossRef]
- Shrout, P.E.; Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef]
- Harbin, H.T.; Madden, D.J. Battered parents: A new syndrome. Am. J. Psychiatry 1979, 136, 1288–1291. [Google Scholar] [CrossRef]
- Williams, M.; Tuffin, K.; Niland, P. It’s like he just goes off, BOOM!: Mothers and grandmothers make sense of child-to-parent violence. Child Fam. Soc. Work 2017, 22, 597–606. [Google Scholar] [CrossRef]
- Gleeson, J.; Lederman, R.; Koval, P.; Wadley, G.; Bendall, S.; Cotton, S.; Herrman, H.; Crisp, K.; Alvarez-Jimenez, M. Moderated online social therapy: A model for reducing stress in carers of young people diagnosed with mental health disorders. Front. Psychol. 2017, 8, 485. [Google Scholar] [CrossRef]
- Toole-Anstey, C.; Townsend, M.L.; Keevers, L. He’s out of control, I’m out of control, it’s just—I’ve got to do something: A narrative inquiry of child to parent violence. Child Adolesc. Soc. Work J. 2022, 1–12, Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Zacarias, A.E.; Macassa, G.; Soares, J.J.F.; Svanstrom, L.; Antai, D. Symptoms of depression, anxiety, and somatization in female victims and perpetrators of intimate partner violence in Maputo City, Mozambique. Int. J. Womens Health 2012, 4, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Kokoulina-Cherevach, E.; Fernandez-Martinez, R. Parental care in childhood and borderline personality disorder. Behav. Psychol. 2016, 24, 237–252. [Google Scholar]

{kind=link}
| Mean | SD | Range | Asymmetry | Skewness | |
|---|---|---|---|---|---|
| 1 CPV (CR) | 0.18 | 0.31 | 0–3 | 4.03 | 24.14 |
| 2 CPV (PR) | 0.16 | 0.26 | 0–3 | 3.23 | 15.25 |
| 3 Self-efficacy | 2.96 | 0.41 | 0–3 | −0.47 | 1.77 |
| 4 Depression | 0.57 | 0.59 | 1–4 | 1.65 | 3.27 |
| 5 Anxiety | 0.56 | 0.52 | 0–4 | 1.38 | 2.29 |
| 6 Hostility | 0.29 | 0.29 | 0–4 | 2.59 | 7.84 |
| 7 Obsessive–compulsive | 0.60 | 0.60 | 0–4 | 1.38 | 2.44 |
| 8 Interpersonal sensitivity | 0.48 | 0.48 | 0–4 | 1.90 | 4.73 |
| 9 Somatization | 0.63 | 0.63 | 0–4 | 1.59 | 2.14 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1 CPV (CR) | 1 | ||||||||
| 2 CPV (PR) | 0.27 *** | 1 | |||||||
| 3 Self-efficacy | −0.16 * | −0.21 ** | 1 | ||||||
| 4 Depression | 0.06 | 0.26 *** | −0.32 *** | 1 | |||||
| 5 Anxiety | −0.03 | 0.24 ** | −0.24 ** | 0.61 *** | 1 | ||||
| 6 Hostility | 0.18 * | 0.36 *** | −0.32 *** | 0.46 *** | 0.52 *** | 1 | |||
| 7 Obsessive–compulsive | 0.14 | 0.27 *** | −0.28 *** | 0.49 *** | 0.61 *** | 0.43 *** | 1 | ||
| 8 Interpersonal sensitivity | 0.10 | 0.34 *** | −0.27 *** | 0.66 *** | 0.51 *** | 0.45 *** | 0.63 *** | 1 | |
| 9 Somatization | −0.02 | 0.17 * | −0.06 | 0.63 *** | 0.52 *** | 30 *** | 0.59 *** | 29 *** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Granado, A.; Fernández-González, L.; del Hoyo-Bilbao, J.; Calvete, E. Psychological Symptoms in Parents Who Experience Child-to-Parent Violence: The Role of Self-Efficacy Beliefs. Healthcare 2023, 11, 2894. https://doi.org/10.3390/healthcare11212894
Jiménez-Granado A, Fernández-González L, del Hoyo-Bilbao J, Calvete E. Psychological Symptoms in Parents Who Experience Child-to-Parent Violence: The Role of Self-Efficacy Beliefs. Healthcare. 2023; 11(21):2894. https://doi.org/10.3390/healthcare11212894
Chicago/Turabian StyleJiménez-Granado, Aitor, Liria Fernández-González, Joana del Hoyo-Bilbao, and Esther Calvete. 2023. "Psychological Symptoms in Parents Who Experience Child-to-Parent Violence: The Role of Self-Efficacy Beliefs" Healthcare 11, no. 21: 2894. https://doi.org/10.3390/healthcare11212894
APA StyleJiménez-Granado, A., Fernández-González, L., del Hoyo-Bilbao, J., & Calvete, E. (2023). Psychological Symptoms in Parents Who Experience Child-to-Parent Violence: The Role of Self-Efficacy Beliefs. Healthcare, 11(21), 2894. https://doi.org/10.3390/healthcare11212894