
Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Cardio-Pulmonary Exercise Test (CPET)
2.3. Measuring Device (modiCARE-MC100, MC-100)
2.4. Developing a Machine Learning Algorithm to Predict VO2max
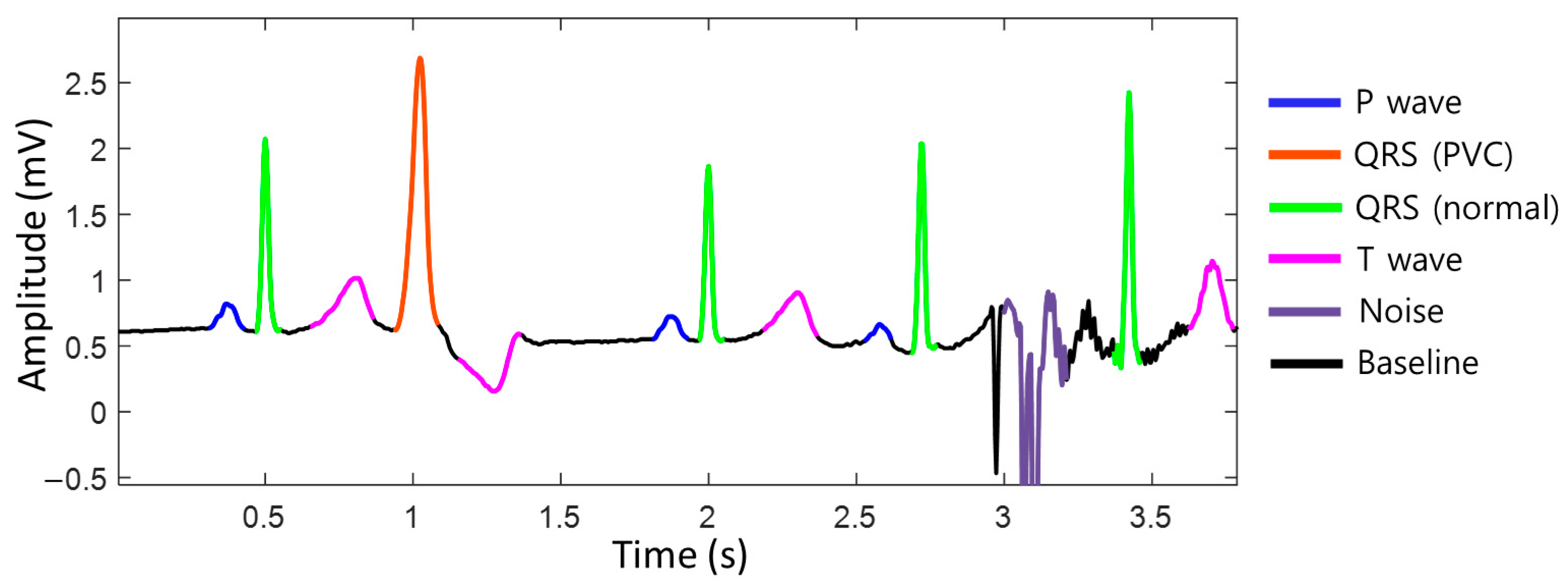
2.4.1. Measurement Variables by MC-100: Heart Rate, Acceleration, and Gyroscope
2.4.2. Feature Selection
2.4.3. Model Development
2.4.4. Comparison between the Machine-Learning Model and Clinical Equation
- ACSM equationVO2max = [speed (m/min) × (0.1 + fractional grade × 1.8) + 3.5];
- FRIEND equationVO2max = [speed (m/min) × (0.17 + fractional grade × 0.79) + 3.5];
- HF-FRIEND equationVO2max = [speed (m/min) × (0.17 + fractional grade × 0.32) + 3.5].
- The “speed” and “fractional grade” represent the values corresponding to the stage at which the patient achieved their maximum during a CPET conducted according to the modified Bruce protocol.
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Pulmonary Function Test (PFT) and CPET
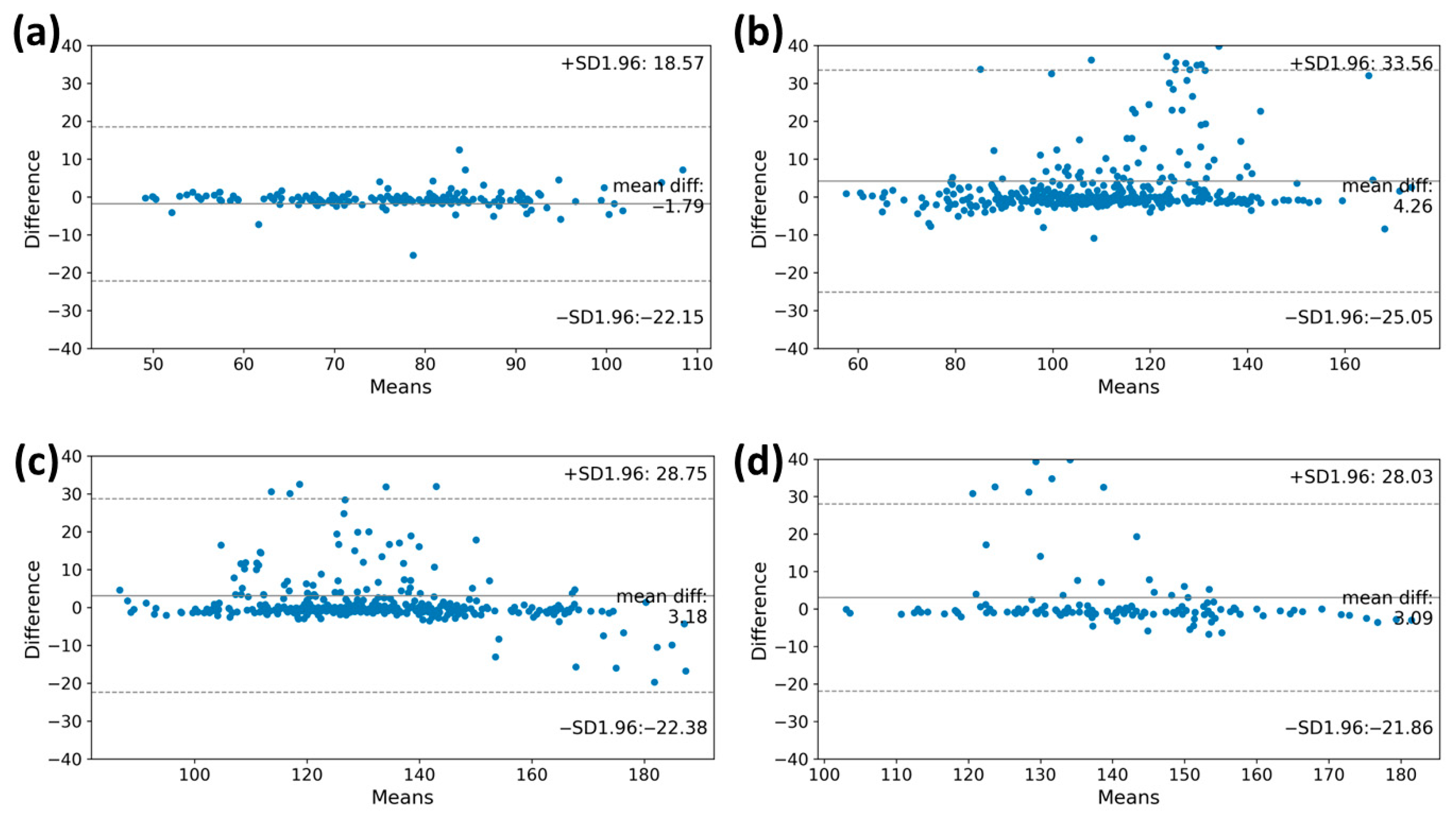
3.3. Heart Rate Accuracy during Graded Exercise Testing
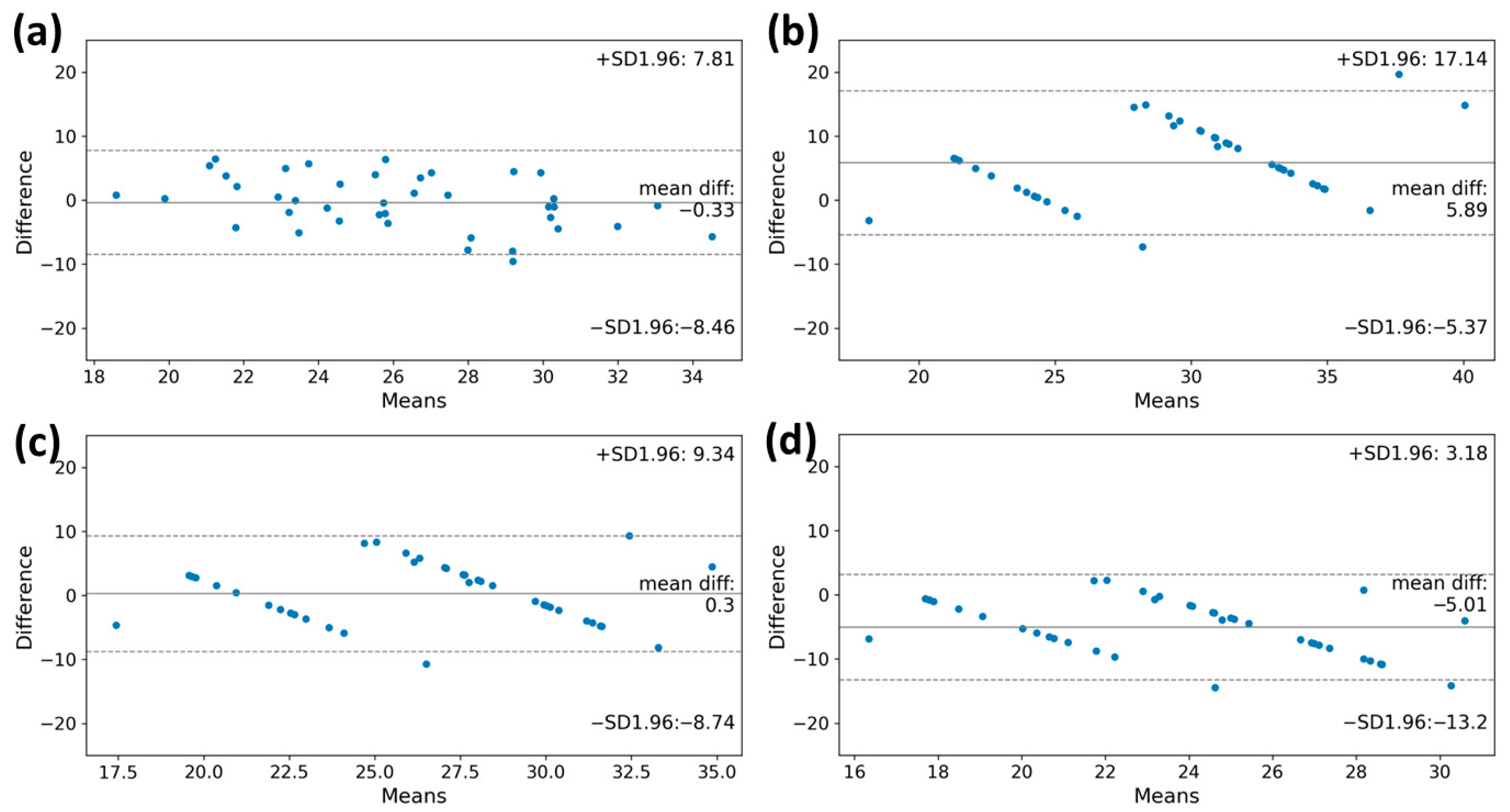
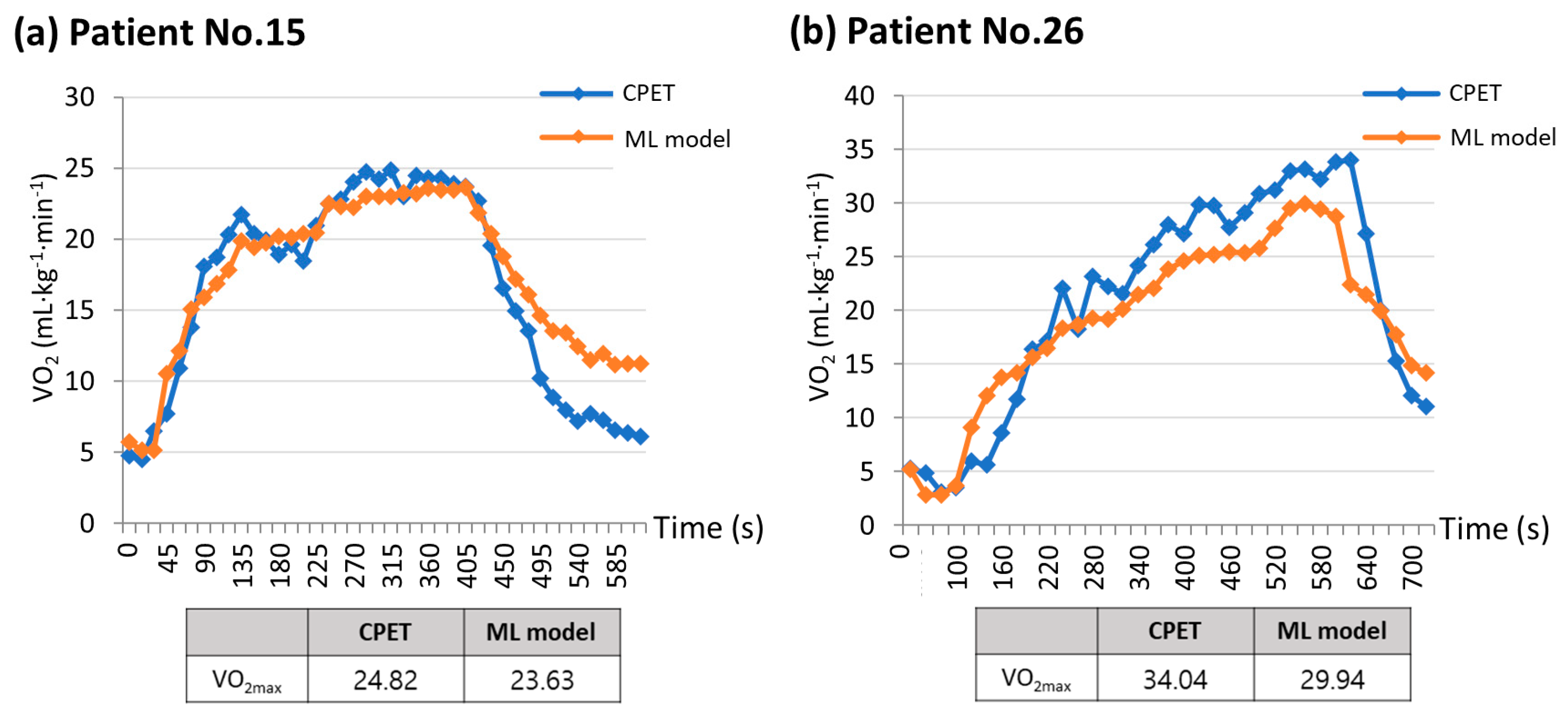
3.4. VO2max Estimation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Hoy, H.; Lynch, T.; Beck, M. Surgical Treatment of Lung Cancer. Crit. Care Nurs. Clin. N. Am. 2019, 31, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Cassivi, S.D.; Fibla, J.; Halgren, L.A.; Wigle, D.A.; Allen, M.S.; Nichols, F.C.; Shen, K.R.; Deschamps, C. External validation of the recalibrated thoracic revised cardiac risk index for predicting the risk of major cardiac complications after lung resection. Ann. Thorac. Surg. 2011, 92, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Deshpand, R.; Chandra, M.; Rauthan, A. Evolving trends in lung cancer: Epidemiology, diagnosis, and management. Indian J. Cancer 2022, 59, S90–S105. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K. Video-Assisted Thoracic Surgery Lobectomy. J. Chest Surg. 2021, 54, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Beckles, M.A.; Spiro, S.G.; Colice, G.L.; Rudd, R.M.; American College of Chest Physicians. The physiologic evaluation of patients with lung cancer being considered for resectional surgery. Chest 2003, 123, 105S–114S. [Google Scholar] [CrossRef] [PubMed]
- British Thoracic Society; Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. BTS guidelines: Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001, 56, 89–108. [Google Scholar] [CrossRef]
- Colice, G.L.; Shafazand, S.; Griffin, J.P.; Keenan, R.; Bolliger, C.T.; American College of Chest Physicians. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidenced-based clinical practice guidelines (2nd edition). Chest 2007, 132, 161S–177S. [Google Scholar] [CrossRef]
- Brunelli, A.; Charloux, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur. Respir. J. 2009, 34, 17–41. [Google Scholar] [CrossRef]
- Kallianos, A.; Rapti, A.; Tsimpoukis, S.; Charpidou, A.; Dannos, I.; Kainis, E.; Syrigos, K. Cardiopulmonary exercise testing (CPET) as preoperative test before lung resection. Vivo 2014, 28, 1013–1020. [Google Scholar]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- Kokkinos, P.; Kaminsky, L.A.; Arena, R.; Zhang, J.; Myers, J. New Generalized Equation for Predicting Maximal Oxygen Uptake (from the Fitness Registry and the Importance of Exercise National Database). Am. J. Cardiol. 2017, 120, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Kokkinos, P.; Kaminsky, L.A.; Arena, R.; Zhang, J.; Franklin, B.; Kraus, W.; Triantafyllidi, H.; Benas, D.; Whellan, D.J.; Myers, J. New Equations for Predicting Maximum Oxygen Uptake in Patients with Heart Failure. Am. J. Cardiol. 2020, 128, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.M.; Zabor, E.C.; Schwitzer, E.; Koelwyn, G.J.; Adams, S.C.; Nilsen, T.S.; Moskowitz, C.S.; Matsoukas, K.; Iyengar, N.M.; Dang, C.T.; et al. Efficacy of Exercise Therapy on Cardiorespiratory Fitness in Patients With Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2018, 36, 2297–2305. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Eves, N.D.; Haykowsky, M.; Joy, A.A.; Douglas, P.S. Cardiorespiratory exercise testing in clinical oncology research: Systematic review and practice recommendations. Lancet Oncol. 2008, 9, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Brickwood, K.J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-Based Wearable Activity Trackers Increase Physical Activity Participation: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]
- Datta, D.; Normandin, E.; ZuWallack, R. Cardiopulmonary exercise testing in the assessment of exertional dyspnea. Ann. Thorac. Med. 2015, 10, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Pina, I.L.; Rodney, R.; et al. Exercise standards for testing and training: A statement for healthcare professionals from the American Heart Association. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef]
- Zhu, H.; Pan, Y.; Wu, F.; Huan, R. Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules based on the LANS Method. Sensors 2019, 19, 4458. [Google Scholar] [CrossRef]
- Hong, Y.; Pan, H.; Sun, W.; Jia, Y. Deep dual-resolution networks for real-time and accurate semantic segmentation of road scenes. arXiv 2021, arXiv:2101.06085 2021. [Google Scholar]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Fokkema, T.; Kooiman, T.J.; Krijnen, W.P.; van der Schans, C.P.; de Groot, M. Reliability and Validity of Ten Consumer Activity Trackers Depend on Walking Speed. Med. Sci. Sports Exerc. 2017, 49, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Leboeuf, S.F.; Aumer, M.E.; Kraus, W.E.; Johnson, J.L.; Duscha, B. Earbud-based sensor for the assessment of energy expenditure, HR, and VO2max. Med. Sci. Sports Exerc. 2014, 46, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Kraft, G.L.; Roberts, R.A. Validation of the garmin forerunner 920xt fitness watch vo2peak test. Int. J. Innov. Educ. Res. 2017, 5, 63. [Google Scholar] [CrossRef]
- Cooper, K.D.; Shafer, A.B. Validity and reliability of the polar A300’s fitness test feature to predict VO2max. Int. J. Exerc. Sci. 2019, 12, 393. [Google Scholar]
- Greco, M.; Angelucci, A.; Avidano, G.; Marelli, G.; Canali, S.; Aceto, R.; Lubian, M.; Oliva, P.; Piccioni, F.; Aliverti, A.; et al. Wearable Health Technology for Preoperative Risk Assessment in Elderly Patients: The WELCOME Study. Diagnostics 2023, 13, 630. [Google Scholar] [CrossRef]
- Jones, L.; Tan, L.; Carey-Jones, S.; Riddell, N.; Davies, R.; Brownsdon, A.; Kelson, M.; Williams-Thomas, R.; Busse, M.; Davies, M.M.; et al. Can wearable technology be used to approximate cardiopulmonary exercise testing metrics? Perioper. Med. 2021, 10, 9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Feature | R2 | MAE | MSE | RMSE |
|---|---|---|---|---|---|
| 5 | HR, ACC, AGE, HEIGHT, BW | 0.702 | 2.883 | 13.698 | 3.686 |
| 4 | HR, ACC, AGE, HEIGHT | 0.592 | 3.212 | 18.644 | 4.274 |
| HR, ACC, AGE, BW | 0.717 | 2.770 | 13.084 | 3.605 | |
| HR, ACC, HEIGHT, BW | 0.662 | 3.048 | 15.391 | 3.888 | |
| HR, AGE, HEIGHT, BW | 0.603 | 3.381 | 18.735 | 4.288 | |
| 3 | HR, ACC, AGE | 0.688 | 3.112 | 17.452 | 4.131 |
| HR, ACC, HEIGHT | 0.754 | 2.828 | 14.103 | 3.744 | |
| HR, ACC, BW | 0.794 | 2.622 | 11.773 | 3.416 | |
| HR, AGE, HEIGHT | 0.630 | 3.424 | 21.224 | 4.564 | |
| HR, AGE, BW | 0.674 | 3.189 | 18.553 | 4.255 | |
| HR, HEIGHT, BW | 0.682 | 3.259 | 18.385 | 4.244 | |
| 2 | HR, ACC | 0.770 | 2.697 | 13.105 | 3.607 |
| HR, AGE | 0.678 | 3.163 | 18.329 | 4.224 | |
| HR, HEIGHT | 0.717 | 3.041 | 16.396 | 4.038 | |
| HR, BW | 0.727 | 2.960 | 15.690 | 3.942 | |
| 1 | HR | 0.735 | 2.882 | 15.183 | 3.881 |
| Linear | Quadratic | Cubic | Ridge | Lasso | Elastic | Random Forest | |
|---|---|---|---|---|---|---|---|
| R2 | 0.670 | 0.794 | 0.714 | 0.670 | 0.636 | 0.644 | 0.679 |
| MAE | 3.329 | 2.622 | 2.901 | 3.328 | 3.443 | 3.396 | 3.098 |
| MSE | 18.654 | 11.773 | 16.383 | 18.652 | 20.615 | 20.121 | 18.345 |
| RMSE | 4.270 | 3.416 | 3.925 | 4.269 | 4.44 | 4.396 | 4.241 |
| Variables | Patients (N = 40) |
|---|---|
| Age, yr | 66.7 ± 8.8 |
| Male | 24 (60) |
| Height, cm | 161.4 ± 7.1 |
| Weight, kg | 64.4 ± 10.7 |
| Smoking | |
| Never | 21 (52.5) |
| Ex-smoker | 8 (20) |
| Current smoker | 11 (27.5) |
| Comorbidity | |
| Coronary artery disease | 6 (15) |
| Heart failure | 2 (5) |
| Arrhythmia | 1 (2.5) * |
| COPD | 10 (25) |
| CCI score | 4.6 ± 2.6 |
| PFT | |
| FVC, L | 3.0 ± 0.7 |
| FVC, % predicted | 90.7 ± 13.0 |
| FEV1, L | 2.2 ± 0.6 |
| FEV1, % predicted | 88.0 ± 18.8 |
| DLco, % predicted | 77.7 ± 17.6 |
| 6 MWT, m | 442.3 ± 57.0 |
| CPET | |
| Maximal stage | |
| 1 | 1 (2.5) |
| 2 | 15 (37.5) |
| 3 | 22 (55) |
| 4 | 2 (5) |
| 5–7 | 0 (0) |
| Peak heart rate, bpm | 133.9 ± 19.0 |
| % predicted maximal HR | 87.4 ± 12.4 ** |
| VO2max, mL/kg/min | 26.3 ± 5.0 |
| ECOG performance status | |
| 0 | 37 (92.5) |
| 1 | 3 (7.5) |
| ≥2 | 0 (0) |
| CPET | ML Model | ACSM | FRIEND | HF-FRIEND | ||
|---|---|---|---|---|---|---|
| Total (n = 40) | VO2max * [mL·kg−1·min−1] | 26.01 (22.82–30.77) | 25.37 (23.49–28.95) | 35.77 (24.57–35.77) | 29.22 (21.15–29.22) | 23.19 (17.39–23.19) |
| VO2max Difference ** [mL·kg−1·min−1] | - | −0.33 | 5.89 | 0.30 | −5.01 | |
| ICC *** | - | 0.693 (0.417–0.838) | 0.517 (−0.126–0.780) | 0.708 (0.445–0.846) | 0.466 (−0.197–0.759) | |
| Maximal Stage 1–2 (n = 14) | VO2max [mL·kg−1·min−1] | 22.99 (19.30–25.16) | 23.31 (21.71–24.21) | 24.57 (24.57–24.57) | 21.15 (21.15–21.15) | 17.39 (17.39–17.39) |
| VO2max Difference [mL·kg−1·min−1] | - | 0.32 | 1.24 | −2.03 | −5.68 | |
| ICC | - | 0.499 (−0.677–0.843) | 0.301 (−1.072–0.772) | 0.229 (−0.858–0.727) | 0.081 (−0.242–0.493) | |
| Maximal stage 3–4 (n = 26) | VO2max [mL·kg−1·min−1] | 27.32 (24.93–31.81) | 27.84 (25.03–29.82) | 35.77 (35.77–35.77) | 29.22 (29.22–29.22) | 23.19 (23.19–23.19) |
| VO2max Difference [mL·kg−1·min−1] | - | −0.68 | 8.39 | 1.56 | −4.65 | |
| ICC | - | 0.488 (−0.145–0.771) | 0.085 (−0.150–0.372) | 0.209 (−0.637–0.633) | 0.094 (−0.288–0.455) | |
| Male (n = 24) | VO2max [mL·kg−1·min−1] | 26.90 (24.15–31.41) | 25.41 (23.73–28.77) | 35.77 (24.57–35.77) | 29.22 (21.15–2922) | 23.19 (17.39–23.19) |
| VO2max Difference [mL·kg−1·min−1] | - | −0.99 | 6.19 | 0.25 | −5.32 | |
| ICC | - | 0.545 (−0.034–0.802) | 0.365 (−0.220–0.701) | 0.562 (−0.037–0.812) | 0.325 (−0.231–0.678) | |
| Female (n = 16) | VO2max [mL·kg−1·min−1] | 23.84 (20.47–26.94) | 25.14 (22.50–29.58) | 35.48 (24.57–35.77) | 28.99 (21.15–29.22) | 23.01 (17.39–23.19) |
| VO2max Difference [mL·kg−1·min−1] | - | 0.66 | 5.43 | 0.38 | −4.55 | |
| ICC | - | 0.808 (0.453–0.933) | 0.660 (−0.176–0.895) | 0.818 (0.473–0.937) | 0.593 (−0.218–0.867) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.A.; Yu, W.; Choi, J.D.; Lee, Y.-s.; Park, J.W.; Jung, Y.J.; Sheen, S.S.; Jung, J.; Haam, S.; Kim, S.H.; et al. Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates. Healthcare 2023, 11, 2863. https://doi.org/10.3390/healthcare11212863
Lee HA, Yu W, Choi JD, Lee Y-s, Park JW, Jung YJ, Sheen SS, Jung J, Haam S, Kim SH, et al. Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates. Healthcare. 2023; 11(21):2863. https://doi.org/10.3390/healthcare11212863
Chicago/Turabian StyleLee, Hyun Ah, Woosik Yu, Jong Doo Choi, Young-sin Lee, Ji Won Park, Yun Jung Jung, Seung Soo Sheen, Junho Jung, Seokjin Haam, Sang Hun Kim, and et al. 2023. "Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates" Healthcare 11, no. 21: 2863. https://doi.org/10.3390/healthcare11212863
APA StyleLee, H. A., Yu, W., Choi, J. D., Lee, Y.-s., Park, J. W., Jung, Y. J., Sheen, S. S., Jung, J., Haam, S., Kim, S. H., & Park, J. E. (2023). Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates. Healthcare, 11(21), 2863. https://doi.org/10.3390/healthcare11212863