
Factors of Capital on Depression in Older Adulthood: A Comparison of Urban and Rural Regions in Korea

Abstract
:1. Introduction
2. Theoretical Background
2.1. Capital and Depression
2.2. Capital and Depression in Older Adulthood and Regions
3. Materials and Methods
3.1. Data
3.2. Study Parameters and Instruments: Geriatric Depression
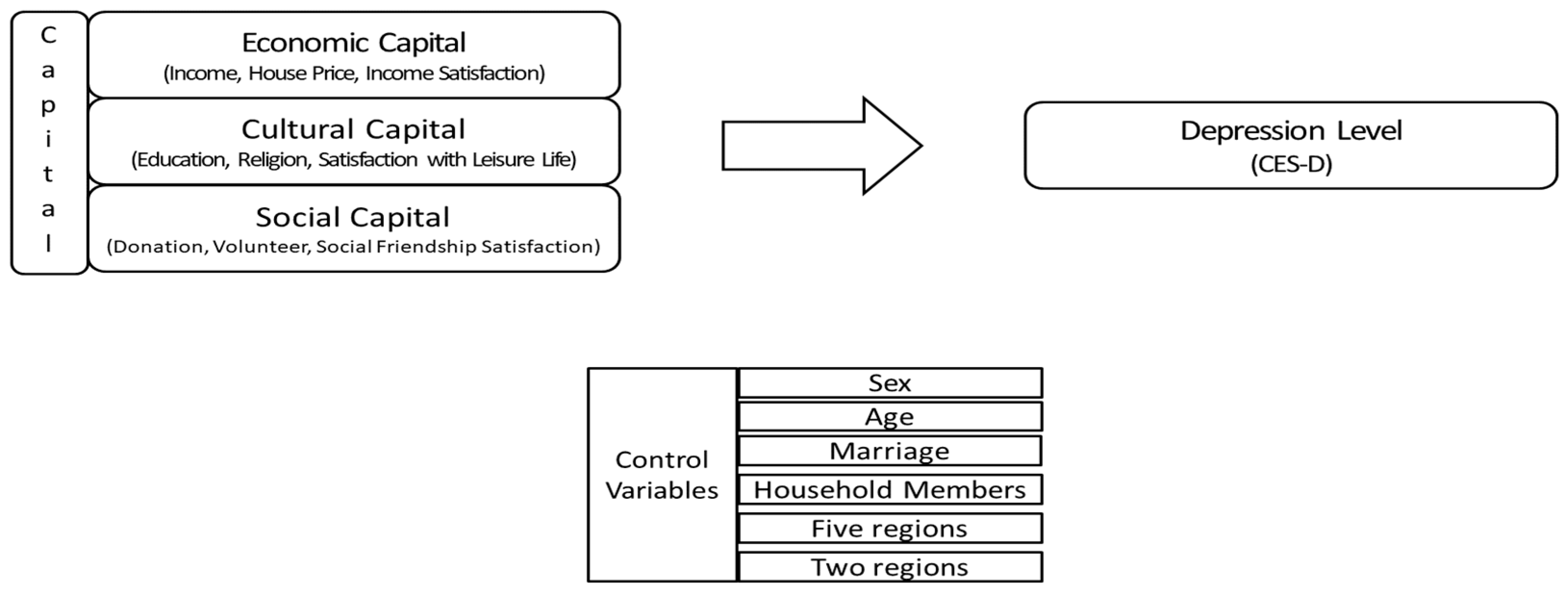
3.3. Capital
3.3.1. Economic Capital
3.3.2. Cultural Capital
3.3.3. Social Capital

{kind=link}
{kind=link}
| Type of Capital | Authors (Year) | Variable Composition |
|---|---|---|
| Economic capital | Caro et al. (2014) [56] | Income and assets, parents’ education level, parents’ employment status |
| Lissitsa (2015) [57] | Individual income, social benefits at work | |
| Cultural capital | Holt (1998) [39] | Parents’ education level and occupation, individual’s education level and occupation |
| Tang (2006) [58] | Religion, frequency of participation in religious activities, pleasure reading, quality of life | |
| Social capital | Inouye (2007) [63] | Network, reciprocity norms, trust, participation opportunity, formal and informal interaction, life as a member of a community |
| SCCBS | Trust (social trust, interracial trust), diversity of friendship, political participation (electoral political participation, participation in protest politics), civil leadership and associational involvement, donation and volunteering, faith-based engagement, equality of civic engagement | |
| HQS | Social participation, social network and social support, reciprocity and trust, civic engagement, views about community | |
| Social capital-related indices in the WVS | Social participation, reciprocity, political interest, trust |
3.3.4. Other Variables
3.3.5. Panel Analysis
4. Analysis Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for Sociology of Education; Richardson, J.G., Ed.; Greenwood: Westport, CT, USA, 1986; pp. 241–258. [Google Scholar]
- Fung, H.H.; Stoeber, F.S.; Yeung, D.Y.L.; Lang, F.R. Cultural specificity of socioemotional selectivity: Age differences in social network composition among Germans and Hong Kong Chinese. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2008, 63, 156–164. [Google Scholar] [CrossRef]
- Wilkinson, R.G. Unhealthy Societies: The Afflictions of Inequality; Routledge: Oxfordshire, UK, 1996. [Google Scholar]
- Bonnewyn, A.; Shah, A.; Demyttenaere, K. Suicidality and suicide in older people. Rev. Clin. Gerontol. 2009, 19, 271–294. [Google Scholar] [CrossRef]
- Goldney, R.D.; Dal Grande, E.; Fisher, L.J.; Wilson, D. Population attributable risk of major depression for suicidal ideation in a random and representative community sample. J. Affect. Disord. 2003, 74, 267–272. [Google Scholar] [CrossRef]
- Joiner, T.E.; Van Orden, K.A. The interpersonal psychological theory of suicidal behavior indicates specific and crucial psychotherapeutic targets. Int. J. Cogn. Ther. 2008, 1, 80–89. [Google Scholar] [CrossRef]
- Billings, A.G.; Moos, R.H. Psychosocial theory and research on depression: An integrative framework and review. Clin. Psychol. Rev. 1982, 2, 213–237. [Google Scholar] [CrossRef]
- Lin, N. Social Capital: A Theory of Social Structure and Action; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Abel, T. Cultural capital and social inequality in health. J. Epidemiol. Community Health 2008, 62, e13. [Google Scholar] [CrossRef] [PubMed]
- Statistics Korea. Results of the 2022 Agricultural and Fisheries Survey; Statistics Korea: Daejeon, Republic of Korea, 2023. [Google Scholar]
- Burholt, V.; Windle, G.; Morgan, D.J. A social model of loneliness: The roles of disability, social resources, and cognitive impairment. Gerontologist 2017, 57, 1020–1030. [Google Scholar] [CrossRef]
- Dare, J.; Wilkinson, C.; Marquis, R.; Donovan, R.J. The people make it fun, the activities we do just make sure we turn up on time. Factors influencing older adults’ participation in community-based group programmes in Perth, Western Australia. Health Soc. Care Community 2018, 26, 871–881. [Google Scholar] [CrossRef]
- Rudman, L.; Gold, D.D.; McGrath, C.; Zuvela, B.; Spafford, M.M.; Renwick, R. Why would I want to go out?: Age-related Vision Loss and Social Participation. Can. J. Aging 2016, 35, 465–478. [Google Scholar] [CrossRef]
- Torres, S.; Warren-Findlow, J. Aging Alone, Gossiping Together: Older Adults’ Talk as Social Glue. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2019, 74, 1474–1482. [Google Scholar] [CrossRef]
- Kim, Y.Y.; Jeon, Y.H.; Kim, B.Y. Deprivation index, suicidal ideation, depression, and social service innovative measures for older adults in the COVID-19 era. In Proceedings of the 2021 Social Welfare Conference, Seoul, Republic of Korea, 25 October 2021. [Google Scholar]
- Cottam, H. Relational welfare. Soundings 2011, 48, 134–144. [Google Scholar] [CrossRef]
- Cottam, H. Radical Help: How We Can Remake the Relationships between Us and Revolutionize the Welfare State; Virago: London, UK, 2008. [Google Scholar]
- Von Heimburg, D.; Ness, O. Relational welfare: A socially just response to co-creating health and wellbeing for all. Scand. J. Public Health 2021, 49, 639–652. [Google Scholar] [CrossRef] [PubMed]
- KoWePS. Korean Welfare Panel Study. Available online: https://www.koweps.re.kr:442/main.do;jsessionid=71381BDC4B427E6842ED7BBB93A35FD5 (accessed on 1 August 2021).
- Marx, K. Capital: An Abridged Edition; McLellan, D., Ed.; Oxford University Press: Oxford, UK, 1867. [Google Scholar]
- DiMaggio, P.; Hargittai, E.; Neuman, W.R.; Robinson, J.P. Social implications of the internet. Annu. Rev. Sociol. 2001, 27, 307–336. [Google Scholar] [CrossRef]
- UNESCO. Chair of Human Rights, Peace and Democracy; The International Bill of Human Rights, Volume I, Part I, World Documents Tehran; Shahid Beheshti University Press: Tehran, Iran, 2002. [Google Scholar]
- World Health Organization. Depression; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int (accessed on 1 July 2021).
- Abel, T.; Frohlich, K.L. Capital and capabilities: Linking structure and agency to reduce health inequalities. Soc. Sci. Med. 2012, 74, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Pinxten, W.; Lievens, J. The importance of economic, social and cultural capital in understanding health inequalities: Using a Bourdieu-based approach in research on physical and mental health perceptions. Sociol. Health Illn. 2014, 36, 1095–1110. [Google Scholar] [CrossRef] [PubMed]
- Hanklang, S.; Ratanasiripong, P.; Naksranoi, S.; Sathira-Anant, S.; Patanasri, K. Quality of life and mental health among Thai older workers in community enterprises. J. Health Res. 2018, 32, 237–250. [Google Scholar] [CrossRef]
- Morrow-Howell, N.; Hinterlong, J.; Rozario, P.A.; Tang, F. Effects of volunteering on the well-being of older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S137–S145. [Google Scholar] [CrossRef] [PubMed]
- Thoits, P.A.; Hewitt, L.N. Volunteer work and well-being. J. Health Soc. Behav. 2001, 42, 115–131. [Google Scholar] [CrossRef]
- Witherspoon, K.; Bindman, J. Economic capital and mental health in later life: A review of the literature. J. Aging Health 2018, 30, 597–622. [Google Scholar]
- Koyanagi, A.; Carvalho, J.; Koyanagi, C. The relationship between social, economic, and cultural capital and mental health in old age: A systematic review. Aging Ment. Health 2018, 22, 937–947. [Google Scholar]
- Sato, K.; Kondo, N.; Kondo, K. Pre-pandemic individual-and community-level social capital and depressive symptoms during COVID-19: A longitudinal study of Japanese older adults in 2019–2021. Health Place 2022, 74, 102772. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Wu, X.; Zeng, D. Promoting ageing in place in Hong Kong: Neighbourhood social environment and depression among older adults. J. Asian Public Policy 2022, 1–18. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, L.; Wu, H.; Zhu, Y.; Shi, X. Targeted poverty reduction under new structure: A perspective from mental health of older adults in rural China. China Agric. Econ. Rev. 2019, 11, 555–566. [Google Scholar] [CrossRef]
- Scott, A.; Storper, M. Regions, globalization, development. Reg. Stud. 2003, 37, 579–593. [Google Scholar] [CrossRef]
- Storper, M. Keys to the City: How Economics, Institutions, Social Interaction, and Politics Shape Development; Princeton University Press: Princeton, NJ, USA, 2013. [Google Scholar]
- Castells-Quintana, D.; Royuela, V.; Veneri, P. Inequality and city size: An analysis for OECD functional urban areas. Pap. Reg. Sci. 2020, 99, 1045–1064. [Google Scholar] [CrossRef]
- Glaeser, E.; Resseger, M.; Tobio, K. Inequality in cities. J. Reg. Sci. 2015, 49, 617–646. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R.G. Psychosocial and material pathways in the relation between income and health: A response to Lynch et al. Br. Med. J. 2001, 322, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.B. Does cultural capital structure American consumption? J. Consum. Res. 1998, 25, 1–25. [Google Scholar] [CrossRef]
- De Graaf, N.D.; De Graaf, P.M.; Kraaykamp, G. Parental cultural capital and educational attainment in the Netherlands: A refinement of the cultural capital perspective. Sociol. Educ. 2000, 7, 92–111. [Google Scholar] [CrossRef]
- Havighurst, R.J.; Albrecht, R. Older People; Longmans, Green: London, UK, 1953. [Google Scholar]
- World Health Organization. Active Ageing: A Policy Framework; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Almedon, A. Social capital and mental health: An interdisciplinary review of primary evidence. Soc. Sci. Med. 2005, 61, 943–964. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Williams, K.L.; Galliher, R.V. Predicting depression and self-esteem from social connectedness, support, and competence. J. Soc. Clin. Psychol. 2006, 25, 855–874. [Google Scholar] [CrossRef]
- Kobayashi, T.; Suzuki, E.; Noguchi, M.; Kawachi, I.; Takao, S. Community-level social capital and psychological distress among the elderly in Japan: A population-based study. PLoS ONE 2015, 10, e0142629. [Google Scholar]
- Cornwell, B. Social disadvantage and network turnover. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 70, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and analysis of definitions of social participation found in the aging literature: Toward a taxonomy of social participation. Soc. Sci. Med. 2020, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Richard, L.; Gauvin, L.; Gosselin, C.; Laforest, S. Staying connected: Neighbourhood correlates of social participation among older adults living in an urban environment in Montreal, Quebec. Health Promot. Int. 2009, 24, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.W.; Loo, B.P.; Mahendran, R. Neighbourhood environment and depressive symptoms among the elderly in Hong Kong and Singapore. Int. J. Health Geogr. 2020, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.L. Important elements and features of neighborhood landscape for aging in place: A study in Hong Kong. Front. Public Health 2020, 8, 316. [Google Scholar] [CrossRef]
- Zhang, Z. The Impact of Children’s Migrant Work on the Physical and Mental Health of Left-Behind Parents; Capital University of Economics and Business: Beijing, China, 2018. (In Chinese) [Google Scholar]
- Li, Q. The Impact of Family Care on the Health of the Disabled Elderly and Caregivers in Urban and Rural Areas; Department of Population and Labor Economics, University of Chinese Academy of Social Sciences: Beijing, China, 2021; pp. 110–121. (In Chinese) [Google Scholar]
- Guo, A.; Da Nan, G. The impact of medical service accessibility on elderly health from the perspective of health inequality: An empirical analysis based on CLHLS data. Popul. Dev. 2002, 26, 60–69. (In Chinese) [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Caro, D.H.; Sandoval-Hernández, A.; Lüdtke, O. Cultural, social, and economic capital constructs in international assessments: An evaluation using exploratory structural equation modeling. Sch. Eff. Sch. Improv. 2014, 25, 433–450. [Google Scholar] [CrossRef]
- Lissitsa, S. Digital use as a mechanism to accrue economic capital: A Bourdieusian perspective. Innov. Eur. J. Soc. Sci. Res. 2015, 28, 464–482. [Google Scholar] [CrossRef]
- Tang, F. What resources are needed for volunteerism? A life course perspective. J. Appl. Gerontol. 2006, 25, 375–390. [Google Scholar] [CrossRef]
- Hong, D.S.; Lee, M.S.; Hwang, I.S. A study on the factors influencing the elderly’s choice of sharing behavior: Analysis of the influence of various types of capital. Korean Soc. Welf. Adm. 2020, 22, 73–102. [Google Scholar]
- SCCBS. US Social Capital Community Benchmark Survey. Available online: https://www.thearda.com/Archive/Files/Descriptions/SCCBS.asp (accessed on 19 March 2021).
- HQS. UK Social Capital Harmonised Question Set. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/bulletins/socialcapitalintheuk/2020 (accessed on 11 February 2021).
- WVS. World Values Survey. Available online: http://www.worldvaluessurvey.org/wvs.jsp (accessed on 10 January 2021).
- Inouye, J.E. Effect of institutional trust on formal and informal volunteering. In Proceedings of the 102nd Annual Meeting of American Sociological Association, New York, NY, USA, 11–14 August 2007. [Google Scholar]
- Kim, Y.; Park, H. Factors influencing suicidal ideation according to the deprivation indices of different regions in Korea. J. Prev. Med. Public Health 2023, 56, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Goswami, S.; Deshmukh, P.R.; Pawar, R.; Raut, A.V.; Bhagat, M.; Mehendale, A.M. Magnitude of depression and its correlates among elderly population in a rural area of Maharashtra: A cross-section study. J. Fam. Med. Prim. Care 2018, 6, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Kinston, J.P. Ian Rankin: The Accidental Crime Writer; January Interview. January Magazine, 1999. [Google Scholar]
- Fengler, A.P. Life satisfaction of subpopulations of elderly: The comparative effects of volunteerism, employment, and meal site participation. Res. Aging 1984, 6, 189–212. [Google Scholar] [CrossRef] [PubMed]
- Musick, M.A.; Herzog, A.R.; House, J.S. Volunteering and mortality among older adults: Findings from a national sample. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1999, 54, S173–S180. [Google Scholar] [CrossRef] [PubMed]
- Statistical Office. KOSIS. Available online: www.kostat.go.kr (accessed on 1 August 2021).
- Zhang, F.; Loo, R.P.Y.; Wang, B. Aging in place: From the neighborhood environment, sense of community, to life satisfaction. Ann. Am. Assoc. Geogr. 2022, 112, 1484–1499. [Google Scholar] [CrossRef]
- Hwang, M.J.; Kim, H.S. Establishment of community security council linked with community organization: Focusing on community network utilization strategy. J. Northeast Asian Stud. 2019, 24, 207–227. [Google Scholar] [CrossRef]
- Coleman, J.S. Social capital in the creation of human capital. In Knowledge and Social Capital; Butterworth-Heinemann: Oxford, UK, 2000. [Google Scholar]
- Lim, H.N. The effects of social capital on life satisfaction of the elderly participating in social activities: The mediating effect of community spirit. Humanit. Soc. Sci. 21 2020, 11, 979–994. [Google Scholar]
- Fougeyrollas, P.; Noreau, L.; Bergeron, H.; Cloutier, R.; Dion, S.A.; St. Michel, G. Social consequences of long term impairments and disabilities: Conceptual approach and assessment of handicap. Int. J. Rehabil. Res. 1998, 21, 127–142. [Google Scholar] [CrossRef]
- Demers, L.; Robichaud, L.; Gélinas, I.; Noreau, L.; Desrosiers, L. Coping strategies and social participation in older adults. Gerontology 2009, 55, 233–239. [Google Scholar] [CrossRef]


| Variable | Categories | Explanation |
| Dependent variables | Depression level (CES-D) | |
Questions:
| Rarely or none of the time (less than 1 day) = 0, some or a little of the time (1–2 days) = 1, occasionally or a moderate amount of time (3–4 days) = 2, most or all of the time (5–7 days) = 3 | |
| Independent variables | Economic capital | |
| Income | Disposable income (Log function) | |
| House price | House price (Log function) | |
| Income satisfaction | Very Dissatisfied = 0, Dissatisfied = 1, Moderate = 2, Satisfied = 3, Very Satisfied = 4 | |
| Cultural capital | ||
| Education | Less than high school graduate = 1, High school graduate or higher = 2 | |
| Religion | Religious = 1, No Religion = 2 | |
| Satisfaction with leisure life | Very Dissatisfied = 0, Dissatisfied = 1, Moderate = 2, Satisfied = 3, Very Satisfied = 4 | |
| Social capital | ||
| Donation Volunteer | no = 1, yes = 2 | |
| Social Friendship Satisfaction | Very Dissatisfied = 0, Dissatisfied = 1, Moderate = 2, Satisfied = 3, Very Satisfied = 4 | |
| Control variables | ||
| Sex | Man = 0, Woman = 1 | |
| Age | 65–69 = 0, 70–74 = 1, 75–79 = 2, Oer 80 years old = 3 | |
| Marriage | No = 0, Yes = 1 | |
| Household members | persons | |
| Five regions | Seoul = 1, area near Seoul = 2, City = 3, rural county = 4, complex county = 5 | |
| Two regions | City = 1 (Add 1–3 above), rural = 2 (Add 4–5 above) |
| 2012–2020 | 2012 | 2020 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Obs | Mean | S.D | Obs | Mean | S.D | Obs | Mean | S.D |
| Depression | 42,332 | 9.54 | 9.69 | 4945 | 9.51 | 9.22 | 4356 | 9.24 | 9.32 |
| lncome | 45,013 | 7.47 | 0.74 | 5295 | 7.33 | 0.74 | 4644 | 7.62 | 0.71 |
| House | 38,006 | 8.76 | 1.43 | 4473 | 8.58 | 1.40 | 3924 | 9.01 | 1.44 |
| Satisfaction of income | 42,333 | 2.79 | 0.87 | 4946 | 2.57 | 0.86 | 4356 | 2.99 | 0.81 |
| Religion | 40,481 | 0.58 | 0.49 | 5308 | 0.61 | 0.49 | 4817 | 0.565 | 0.49 |
| Education | 45,144 | 1.18 | 0.39 | 5308 | 1.17 | 0.37 | 4663 | 1.22 | 0.41 |
| Satisfaction with leisure life | 42,331 | 3.25 | 0.77 | 4945 | 30.11 | 0.78 | 4356 | 3.22 | 0.74 |
| Volunteer | 43,429 | 0.033 | 0.18 | 5103 | 0.028 | 0.17 | 4476 | 0.034 | 0.18 |
| Donation | 45,144 | 1.98 | 0.14 | 5308 | 1.99 | 0.12 | 4663 | 1.98 | 0.15 |
| Social Friendship satisfaction | 42,333 | 3.63 | 0.66 | 4946 | 3.62 | 0.67 | 4356 | 3.57 | 0.65 |
| Sex | 45,144 | 1.62 | 0.49 | 5308 | 1.60 | 0.49 | 4663 | 1.62 | 0.49 |
| Age | 45,144 | 75.67 | 6.66 | 5308 | 74.33 | 6.28 | 4663 | 76.86 | 7.04 |
| Marriage | 45,144 | 1.42 | 0.49 | 5308 | 1.40 | 0.49 | 4663 | 1.43 | 0.50 |
| Household members | 45,129 | 2.02 | 1.03 | 5308 | 2.11 | 1.12 | 4662 | 1.91 | 0.90 |
| No Region Variables | Urban/Rural Dummy Variables | Five Regional Dummy Variables Variables | |
|---|---|---|---|
| Variables | Depression | Depression | Depression |
| Income | −0.863 *** | −0.862 *** | −0.872 *** |
| (0.11) | (0.11) | (0.11) | |
| House prices | −8.74 × 106 ** | −9.27 × 106 ** | −1.23 × 105 *** |
| (0.00) | (0.00) | (0.00) | |
| Income satisfaction | −1.531 *** | −1.529 *** | −1.525 *** |
| (0.06) | (0.06) | (0.06) | |
| Religion | −0.109 | −0.111 | −0.0944 |
| (0.11) | (0.11) | (0.11) | |
| Education | −0.265 | −0.282 | −0.285 |
| (0.20) | (0.20) | (0.20) | |
| Satisfaction with leisure life | −1.822 *** | −1.822 *** | −1.819 *** |
| (0.07) | (0.07) | (0.07) | |
| Volunteering | −0.385 | −0.381 | −0.395 |
| (0.41) | (0.41) | (0.41) | |
| Donations | −0.143 | −0.140 | −0.164 |
| (0.51) | (0.51) | (0.51) | |
| Social friendship satisfaction | −1.520 *** | −1.516 *** | −1.523 *** |
| (0.08) | (0.08) | (0.08) | |
| Sex | 2.189 *** | 2.187 *** | 2.182 *** |
| (0.16) | (0.16) | (0.16) | |
| Age | 0.176 *** | 0.177 *** | 0.175 *** |
| (0.01) | (0.01) | (0.01) | |
| Marriage | 1.371 *** | 1.362 *** | 1.351 *** |
| (0.16) | (0.16) | (0.16) | |
| Household members | −0.218 *** (0.08) | −0.220 *** (0.08) | −0.223 *** (0.08) |
D_Areas near Seoul D_City D_Rural county D_Urban−rural complex | 0.144 (0.16) | −1.009 *** (0.24) −0.475 ** (0.23) −0.739 *** (0.25) −0.750 * (0.43) | |
| Constant | 17.35 *** | 17.20 *** | 18.18 *** |
| (1.27) | (1.28) | (1.29) | |
| Observations | 31,852 | 31,852 | 31,852 |
| Number of pid | 5962 | 5962 | 5962 |
| Urban | Rural | |
|---|---|---|
| Variables | Depression | Depression |
| Income | −0.889 *** | −0.711 *** |
| (0.13) | (0.20) | |
| House prices | −7.16 × 106 * | −2.94 × 105 ** |
| (0.00) | (0.00) | |
| Income satisfaction | −1.603 *** | −1.313 *** |
| (0.07) | (0.11) | |
| Religion | −0.182 | −0.0152 |
| (0.13) | (0.21) | |
| Education | −0.145 | −0.742 * |
| (0.22) | (0.45) | |
| Satisfaction with leisure life | −1.958 *** | −1.457 *** |
| (0.08) | (0.13) | |
| Volunteering | 0.0933 | −1.555 ** |
| (0.49) | (0.77) | |
| Donations | 0.448 | −1.850 ** |
| (0.59) | (1.03) | |
| Social friendship satisfaction | −1.535 *** | −1.405 *** |
| (0.09) | (0.16) | |
| Sex | 2.257 *** | 2.101 *** |
| (0.19) | (0.30) | |
| Age | 0.193 *** | 0.135 *** |
| (0.01) | (0.02) | |
| Marriage | 1.419 *** | 1.230 *** |
| (0.19) | (0.30) | |
| Household members | −0.232 ** | −0.150 |
| (0.09) | (0.15) | |
| Constant | 16.42 *** | 18.85 *** |
| (1.49) | (2.48) | |
| Observations | 23,145 | 8707 |
| Number of pid | 4359 | 1769 |
| Region | 2015 | 2016 | 2017 | 2018 | 2019 |
| All | 0.314 | 0.308 | 0.303 | 0.294 | 0.297 |
| Seoul/metropolis | 0.298 | 0.291 | 0.310 | 0.300 | 0.302 |
| Rural areas | 0.280 | 0.257 | 0.298 | 0.276 | 0.278 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, M.; Kim, Y.; Hong, I. Factors of Capital on Depression in Older Adulthood: A Comparison of Urban and Rural Regions in Korea. Healthcare 2023, 11, 2850. https://doi.org/10.3390/healthcare11212850
Bae M, Kim Y, Hong I. Factors of Capital on Depression in Older Adulthood: A Comparison of Urban and Rural Regions in Korea. Healthcare. 2023; 11(21):2850. https://doi.org/10.3390/healthcare11212850
Chicago/Turabian StyleBae, MinYoung, YunYoung Kim, and Ijin Hong. 2023. "Factors of Capital on Depression in Older Adulthood: A Comparison of Urban and Rural Regions in Korea" Healthcare 11, no. 21: 2850. https://doi.org/10.3390/healthcare11212850
APA StyleBae, M., Kim, Y., & Hong, I. (2023). Factors of Capital on Depression in Older Adulthood: A Comparison of Urban and Rural Regions in Korea. Healthcare, 11(21), 2850. https://doi.org/10.3390/healthcare11212850