
A Study of the Relationship between Men Who Have Sex with Men Stigma and Depression: A Moderated Mediation Model

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Predictor Variable
2.3. Mediator/Moderator Variables
2.4. Outcome Variable
2.5. Control Variables
2.6. Statistical Analysis
3. Results
3.1. Sample Characteristic
3.2. Correlation Analysis
3.3. Confirmatory Factor Analysis
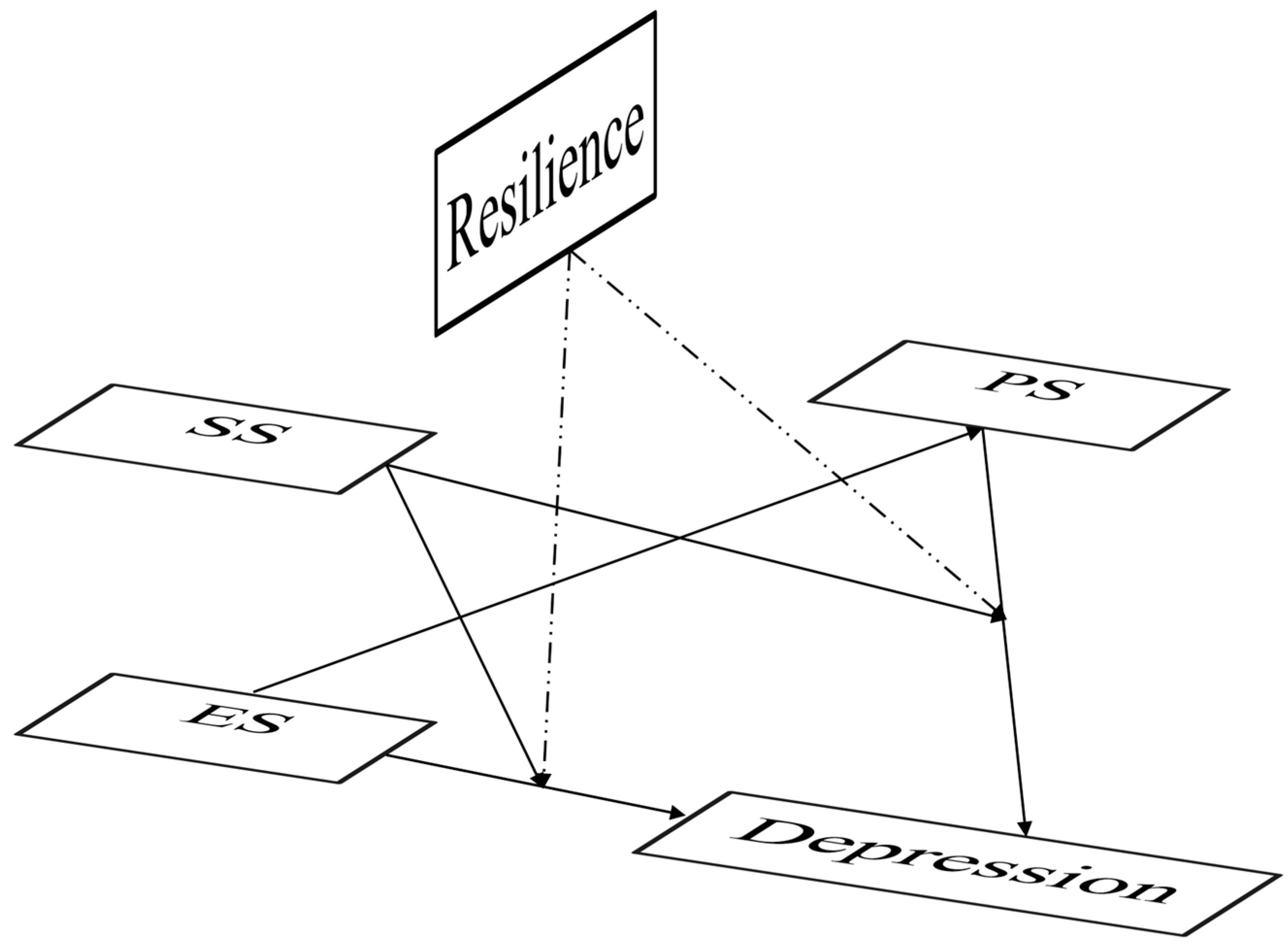
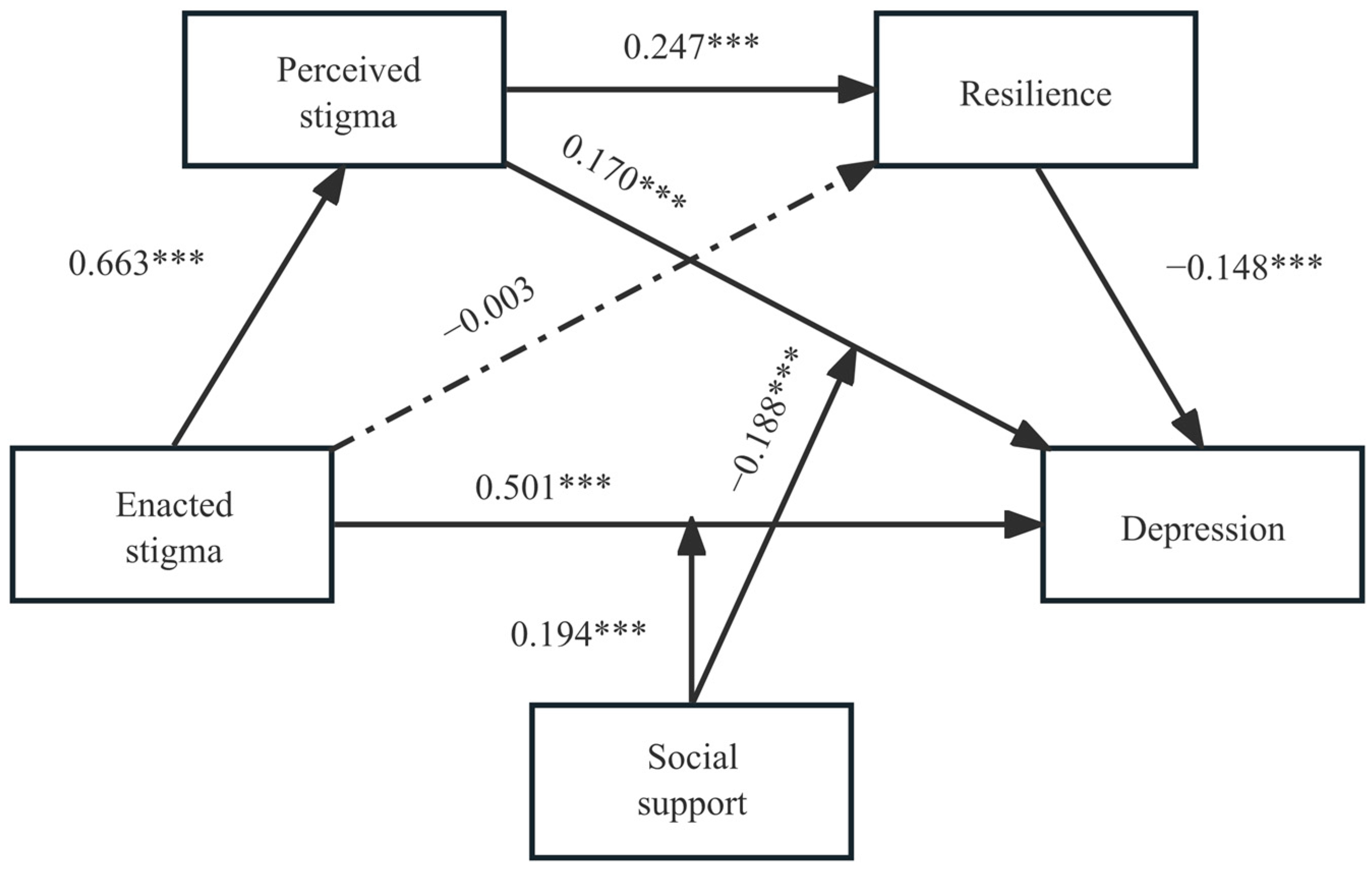
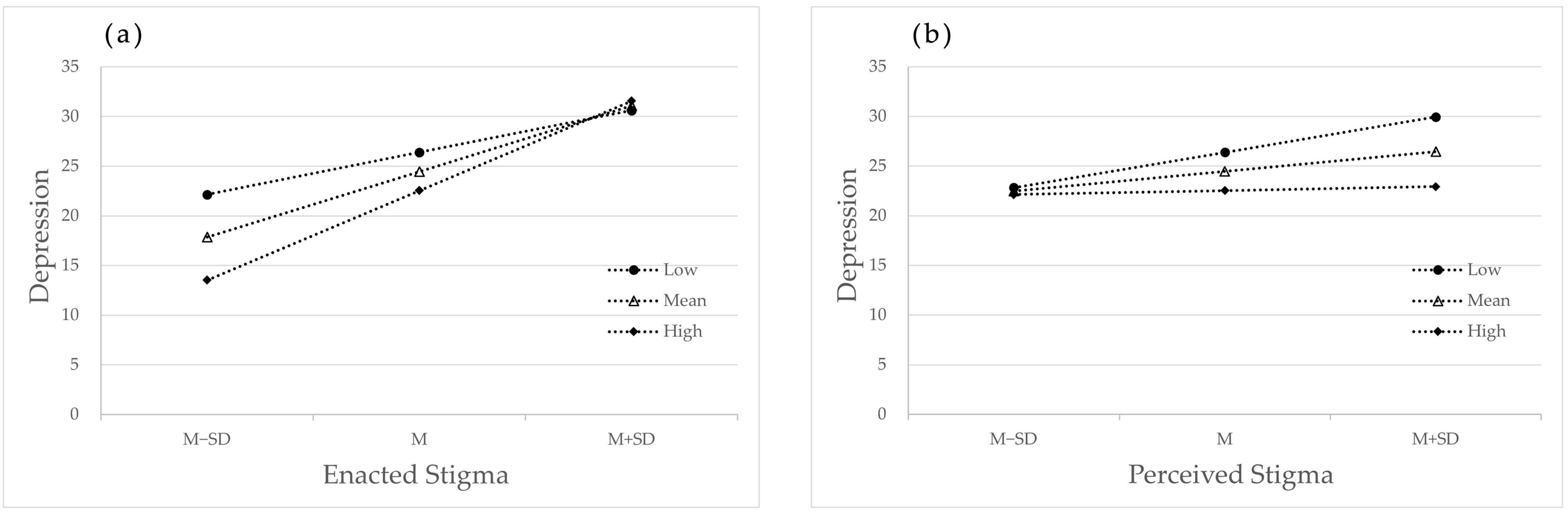
3.4. Moderated Mediation Effect Analysis
4. Discussion
5. Limitations
6. Implications for Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nouri, E.; Moradi, Y.; Moradi, G. What is the global prevalence of depression among men who have sex with men? A systematic review and meta-analysis. Ann. Gen. Psychiatry 2022, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Feng, T.; Wang, T.; Wu, X.; Cai, Y.; Yang, T. Reported prevalence of depression or depressive symptoms among men who have sex with men in China, 2004–2018: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Sandfort, T.G.; Bakker, F.; Schellevis, F.G.; Vanwesenbeeck, I. Sexual orientation and mental and physical health status: Findings from a Dutch population survey. Am. J. Public Health 2006, 96, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Sivasubramanian, M.; Mimiaga, M.J.; Mayer, K.H.; Anand, V.R.; Johnson, C.V.; Prabhugate, P.; Safren, S.A. Suicidality, clinical depression, and anxiety disorders are highly prevalent in men who have sex with men in Mumbai, India: Findings from a community-recruited sample. Psychol. Health Med. 2011, 16, 450–462. [Google Scholar] [CrossRef]
- Wei, D.; Wang, X.; You, X.; Luo, X.; Hao, C.; Gu, J.; Peng, S.; Yang, X.; Hao, Y.; Silenzio, V.M.B.; et al. Prevalence of depression, anxiety and suicide among men who have sex with men in China: A systematic review and meta-analysis. J. Epidemiol. Psychiatr. Sci. 2020, 29, e136. [Google Scholar] [CrossRef]
- Don, O.; Shufang, S.; Nazer, B.A.; Rainier, M.; Sylvia, S.; Elise, v.d.E.; Eduard, S. Integrating HIV and mental health interventions to address a global syndemic among men who have sex with men. J. Lancet HIV 2022, 9, e574–e584. [Google Scholar]
- Di Ciaccio, M.; Villes, V.; Michels, D.; Morel, S.; Delabre, R.M.; Rojas Castro, D.; Velter, A. Impact of the early 2020 COVID-19 crisis and lockdown on PrEP use among men who have sex with men (MSM) in France. Sex Transm. Infect. 2022, 98, 510–517. [Google Scholar] [CrossRef]
- Stefan, B.; Darrin, A.; Judith, L.; Bafokeng, K.; Puleng, L.; Relebohile, T.; Andrea, W.; Chris, B. A cross-sectional assessment of population demographics, HIV risks and human rights contexts among men who have sex with men in Lesotho. J. Int. AIDS Soc. 2011, 14, 36. [Google Scholar]
- Storm, S.; Deuba, K.; Shrestha, R.; Pandey, L.R.; Dahal, D.; Shrestha, M.K.; Pokhrel, T.N.; Marrone, G. Social and structural factors associated with depression and suicidality among men who have sex with men and transgender women in Nepal. BMC Psychiatry 2021, 21, 476. [Google Scholar] [CrossRef]
- Pan, X.H.; Li, R.H.; Ma, Q.Q.; Wang, H.; Jiang, T.T.; He, L.; Zeng, S.D.; Wang, D.Y.; Ye, Z.M.; Zhu, H.S.; et al. Sexual risk behaviour, sexual victimisation, substance use and other factors related to depression in men who have sex with men in Wenzhou, China: A cross-sectional study. BMJ Open 2018, 8, e013512. [Google Scholar] [CrossRef]
- Shi, X.; Xu, W.; Zheng, Y. Heterosexual Marital Intention: Effects of Internalized Homophobia, Homosexual Identity, Perceived Family Support, and Disclosure Among Chinese Gay and Bisexual Men. J. Homosex. 2020, 67, 452–467. [Google Scholar] [CrossRef]
- Wen, G.; Zheng, L. Relationship Status and Marital Intention Among Chinese Gay Men and Lesbians: The Influences of Minority Stress and Culture-Specific Stress. Arch. Sex. Behav. 2020, 49, 681–692. [Google Scholar] [CrossRef]
- Steward, W.T.; Miège, P.; Choi, K.H. Charting a moral life: The influence of stigma and filial duties on marital decisions among Chinese men who have sex with men. PLoS ONE 2013, 8, e71778. [Google Scholar] [CrossRef]
- Zhang, B.C.; Chu, Q.S. MSM and HIV/AIDS in China. Cell Res. 2005, 15, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, M.D.C.; McKinnon, K.; Dourado, I.; Veras, M.A.; Magno, L.; Almeida, M.; Wainberg, M.; Kendall, C.; Kerr, L.; Cournos, F. A potential syndemic effect associated with symptoms of depression among men who have sex with men. Braz. J. Psychiatry 2022, 44, 517–521. [Google Scholar] [CrossRef]
- Okonkwo, N.; Rwema, J.O.T.; Lyons, C.; Liestman, B.; Nyombayire, J.; Olawore, O.; Nsanzimana, S.; Mugwaneza, P.; Kagaba, A.; Sullivan, P.; et al. The Relationship Between Sexual Behavior Stigma and Depression Among Men Who have Sex with Men and Transgender Women in Kigali, Rwanda: A Cross-sectional Study. Int. J. Ment. Health Addict. 2022, 20, 3228–3243. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H.; Yang, Y.T.; Fu, C.W.; Lin, H.J.; Wang, T.T.; Wang, S.L.; Kuang, J.W.; Chen, X.X.; Wang, J.Y. Loneliness and depressive symptoms among men who have sex with men in China: A cross-sectional study. Front. Psychiatry 2023, 14, 1179703. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Li, X.; Li, J.; Wang, W.; Yang, Y.; Yao, X.; Yang, N.; Li, S. Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing, China. AIDS Care 2019, 31, 1069–1076. [Google Scholar] [CrossRef]
- Hu, Y.; Zhong, X.N.; Peng, B.; Zhang, Y.; Liang, H.; Dai, J.H.; Zhang, J.; Zhong, X.H.; Huang, A.L. Comparison of depression and anxiety between HIV-negative men who have sex with men and women (MSMW) and men who have sex with men only (MSMO): A cross-sectional study in Western China. J. BMJ Open 2019, 9, e023498. [Google Scholar] [CrossRef]
- Luo, R.; Silenzio, V.M.B.; Huang, Y.; Chen, X.; Luo, D. The Disparities in Mental Health Between Gay and Bisexual Men Following Positive HIV Diagnosis in China: A One-Year Follow-Up Study. Int. J. Environ. Res. Public Health 2020, 17, 3414. [Google Scholar] [CrossRef]
- Skakoon-Sparling, S.; Berlin, G.; Lachowsky, N.J.; Moore, D.M.; Lambert, G.; Cox, J.; Grace, D.; Apelian, H.; Sang, J.R.M.; Hart, T.A. Social Support and HIV Prevention Behaviors Among Urban HIV-Negative Gay, Bisexual, and Other Men Who Have Sex with Men. Health Psychol. 2022, 41, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.F.; Budge, S.; Shen, W.X.; Xu, G.; Liu, M.Q.; Feng, S.Q. Minority stress and health: A grounded theory exploration among men who have sex with men in China and implications for health research and interventions. Soc. Sci. Med. 2020, 252, 112917. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. J. Psychol. Sex. Orientat. Gend. Divers. 2013, 1, 3–26. [Google Scholar] [CrossRef]
- Bruce, D.; Harper, G.W.; Bauermeister, J.A. Minority Stress, Positive Identity Development, And Depressive Symptoms: Implications For Resilience Among Sexual Minority Male Youth. J. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 287. [Google Scholar] [CrossRef]
- Li, X.; Yan, H.; Wang, W.; Yang, H.; Li, S. Association between enacted stigma, internalized stigma, resilience, and depressive symptoms among young men who have sex with men in China: A moderated mediation model analysis. Ann. Epidemiol. 2021, 56, 1–8. [Google Scholar] [CrossRef]
- Tan, S.; Cen, P.; Fang, T.; Yang, X.; Zhang, Y.; Zhu, J.; Huang, H.; Wang, M.; Jiang, L.; Mo, J.; et al. Chained multimediator model of sexual orientation disclosure, sexual minority stigma, sexual minority identity, social support, and resilience among ymsms. BMC Public. Health 2022, 22, 797. [Google Scholar] [CrossRef]
- Pflum, R.S.; Testa, J.R.; Balsam, F.K.; Goldblum, B.P.; Bongar, B. Social support, trans community connectedness, and mental health symptoms among transgender and gender nonconforming adults. J. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 281. [Google Scholar] [CrossRef]
- Gerke, D.R.; Glotfelty, J.; Freshman, M.; Schlueter, J.; Ochs, A.; Plax, K. Help Is Available: Supporting Mental Wellness Through Peer Health Navigation with Young Black Men Who Have Sex with Men with HIV. Aids Patient Care Stds 2022, 36, S54–S64. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, H.; O’Connor, C.; Leyritana, K.; Salvana, E.; Cox, S.E. Depression, Nutrition, and Adherence to Antiretroviral Therapy in Men Who Have Sex With Men in Manila, Philippines. Front. Public Health 2021, 9, 644438. [Google Scholar] [CrossRef]
- De Jesus, M.; Ware, D.; Brown, A.L.; Egan, J.E.; Haberlen, S.A.; Palella, F.J., Jr.; Detels, R.; Friedman, M.R.; Plankey, M.W. Social-environmental resiliencies protect against loneliness among HIV-Positive and HIV-negative older men who have sex with men: Results from the Multicenter AIDS Cohort Study (MACS). Soc. Sci. Med. 2021, 272, 113711. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Song, B.; Feng, S.Y.; Lin, Y.L.; Du, J.; Shao, H.; Chi, Z.; Yang, Y.Z.; Wang, F.X. The relationship of social support, mental health, and health-related quality of life in human immunodeficiency virus-positive men who have sex with men: From the analysis of canonical correlation and structural equation model: A cross-sectional study. Medicine 2018, 97, e11652. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Qu, B.; Zhu, Y.X.; Hu, B.X. The Influence of Social Support on Quality of Life of Men Who Have Sex with Men in China: A Preliminary Study. PLoS ONE 2015, 10, e0127644. [Google Scholar] [CrossRef] [PubMed]
- Chakrapani, V.; Vijin, P.P.; Logie, C.H.; Newman, P.A.; Shunmugam, M.; Sivasubramanian, M.; Samuel, M. Understanding How Sexual and Gender Minority Stigmas Influence Depression Among Trans Women and Men Who Have Sex with Men in India. LGBT Health 2017, 4, 217–226. [Google Scholar] [CrossRef]
- Brown, C.A.; Sullivan, P.S.; Stephenson, R.; Baral, S.D.; Bekker, L.G.; Phaswana-Mafuya, N.R.; Simbayi, L.C.; Sanchez, T.; Valencia, R.K.; Zahn, R.J.; et al. Developing and validating the Multidimensional Sexual Identity Stigma Scale among men who have sex with men in South Africa. Stigma Health 2021, 6, 277–286. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress. 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Tonsing, K.; Zimet, G.D.; Tse, S. Assessing social support among South Asians: The multidimensional scale of perceived social support. Asian J. Psychiatr. 2012, 5, 164–168. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. J. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Dai, Z.; Fu, J.; Qu, Y.; Wu, Y.; Si, M.; Chen, X.; Wang, H.; Xiao, W.; Huang, Y.; Yu, F.; et al. Depressive symptoms, perceived social support, and anticipated HIV stigma among HIV-negative/unknown men who have sex with men in China during the COVID-19 pandemic: A multicenter online cross-sectional study. Brain Behav. 2023, 13, e2946. [Google Scholar] [CrossRef]
- Liu, Y.Y.; Jiang, C.; Li, S.Y.; Gu, Y.; Zhou, Y.; An, X.X.; Zhao, L.; Pan, G.W. Association of recent gay-related stressful events with depressive symptoms in Chinese men who have sex with men. BMC Psychiatry 2018, 18, 217. [Google Scholar] [CrossRef]
- Kitsuse, J.I. Societal Reaction to Deviant Behavior: Problems of Theory and Method. J. Soc. Probl. 1962, 9, 247. [Google Scholar] [CrossRef]
- Koolhaas, J.M.; Bartolomucci, A.; Buwalda, B.; Boer, S.F.d.; Flügge, G.; Korte, S.M.; Meerlo, P.; Murison, R.; Olivier, B.; Palanza, P.; et al. Stress revisited: A critical evaluation of the stress concept. J. Neurosci. Biobehav. Rev. 2011, 35, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.C.; DeBlaere, C.; Moradi, B. Approaches to Research on Intersectionality: Perspectives on Gender, LGBT, and Racial/Ethnic Identities. J. Sex Roles 2013, 68, 639–645. [Google Scholar] [CrossRef]
- Safren, S.A.; Thomas, B.; Biello, K.B.; Mayer, K.H.; Rawat, S.; Dange, A.; Bedoya, C.A.; Menon, S.; Anand, V.; Balu, V.; et al. Strengthening resilience to reduce HIV risk in Indian MSM: A multicity, randomised, clinical efficacy trial. Lancet Glob. Health 2021, 9, e446–e455. [Google Scholar] [CrossRef]
- Trang, K.; Ly, A.T.; Lam, L.X.; Brown, C.A.; To, M.Q.; Sullivan, P.S.; Worthman, C.M.; Giang, L.M.; Jovanovic, T. Mental health in HIV prevention and care: A qualitative study of challenges and facilitators to integration in Vietnam. Social. Sci. Med. 2021, 279, 113978. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Classification | n | % |
|---|---|---|---|
| Age | 18–26 | 680 | 62.3 |
| 27–35 | 320 | 29.3 | |
| >35 | 91 | 8.4 | |
| Household registration | Urban | 757 | 69.4 |
| Rural | 334 | 30.6 | |
| Education level | Illiteracy and semi-illiteracy | 8 | 0.7 |
| Grade school | 16 | 1.5 | |
| Junior high school | 60 | 5.5 | |
| Senior high school | 179 | 16.4 | |
| Junior college | 291 | 26.7 | |
| University degree or above | 537 | 49.2 | |
| Employment status | Employed | 728 | 66.7 |
| Retired | 28 | 2.6 | |
| Students | 269 | 24.7 | |
| Unemployed | 66 | 6.0 | |
| Marital status | Unmarried | 761 | 69.8 |
| Married | 293 | 26.8 | |
| Divorced | 32 | 2.9 | |
| Widowed | 5 | 0.5 | |
| Monthly disposable income (RMB) | <1000 | 49 | 4.5 |
| 1001–3000 | 234 | 21.5 | |
| 3001–5000 | 344 | 31.5 | |
| 5001–10,000 | 346 | 31.7 | |
| >10,000 | 118 | 10.8 |
| Variables | Mean | S.D. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 26.34 | 6.324 | 1 | |||||||
| 2. Education | 5.14 | 1.051 | −0.094 *** | 1 | ||||||
| 3. Income | 3.23 | 1.045 | 0.322 *** | 0.192 *** | 1 | |||||
| 4. Enacted stigma | 15.13 | 5.717 | 0.024 | −0.182 *** | 0.063 ** | 1 | ||||
| 5. Perceived stigma | 18.62 | 6.230 | 0.035 | −0.026 | 0.029 | 0.642 *** | 1 | |||
| 6. Resilience | 36.38 | 8.545 | 0.550 | 0.082 *** | 0.118 *** | 0.148 *** | 0.247 *** | 1 | ||
| 7. Social support | 44.85 | 10.331 | 0.09 *** | 0.059 | 0.102 *** | 0.021 | 0.051 | 0.663 *** | 1 | |
| 8. Depression | 24.00 | 13.320 | −0.017 | −0.240 *** | −0.061 ** | 0.621 *** | 0.475 *** | −0.107 *** | −0.210 *** | 1 |
| Models | X2/df | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|
| Five factors (ES, PS, SS, R, D) | 3.567 | 0.928 | 0.924 | 0.049 | 0.043 |
| Four factors (ES + PS, SS, R, D) | 4.898 | 0.890 | 0.885 | 0.060 | 0.051 |
| Four factors (ES, PS, SS + R, D) | 5.981 | 0.860 | 0.853 | 0.068 | 0.064 |
| Three factors (ES + PS, SS + R, D) | 7.294 | 0.822 | 0.815 | 0.076 | 0.069 |
| Two factors (ES + PS + SS + R, D) | 13.620 | 0.643 | 0.628 | 0.108 | 0.206 |
| Single factor (ES + PS + SS + R + D) | 20.896 | 0.437 | 0.414 | 0.135 | 0.233 |
| Outcome Variable | Predictive Variable | R2 | F | β | b | S.E. | t | LLCL | ULCL |
|---|---|---|---|---|---|---|---|---|---|
| Model 1 | |||||||||
| Perceived stigma | Enacted stigma | 0.423 | 199.159 *** | 0.663 *** | 0.723 | 0.025 | 28.144 | 0.672 | 0.773 |
| Model 2 | |||||||||
| Resilience | Enacted stigma | 0.078 | 18.490 *** | −0.03 | −0.005 | 0.05 | −0.088 | −0.120 | 0.109 |
| Perceived stigma | 0.247 *** | 0.339 | 0.052 | 6.454 | 0.236 | 0.443 | |||
| Model 3 | |||||||||
| Depression | Enacted stigma | 0.464 | 156.734 *** | 0.503 *** | 1.173 | 0.069 | 16.846 | 1.036 | 1.310 |
| Perceived stigma | 0.204 *** | 0.437 | 0.063 | 6.854 | 0.311 | 0.562 | |||
| Resilience | −0.215 *** | −0.336 | 0.036 | −9.323 | −0.407 | −0.265 | |||
| Model 4 | |||||||||
| Depression | Enacted stigma | 0.408 | 105.339 *** | 0.604 *** | 1.408 | 0.055 | 25.323 | 1.299 | 1.513 |
| Outcome Variable | Predictive Variable | R2 | F | β | b | S.E. | t | LLCL | ULCL |
|---|---|---|---|---|---|---|---|---|---|
| Model 1 | |||||||||
| Perceived stigma | Enacted stigma | 0.423 | 199.159 *** | 0.663 *** | 0.723 | 0.025 | 28.177 | 0.675 | 0.776 |
| Model 2 | |||||||||
| Resilience | Enacted stigma | 0.078 | 18.490 *** | −0.003 | −0.005 | 0.059 | −0.080 | −0.120 | 0.111 |
| Perceived stigma | 0.247 *** | 0.339 | 0.052 | 6.399 | 0.234 | 0.442 | |||
| Model 3 | |||||||||
| Depression | Enacted stigma | 0.495 | 117.537 *** | 0.501 *** | 1.168 | 0.069 | 17.016 | 1.010 | 1.279 |
| Perceived stigma | 0.170 *** | 0.364 | 0.630 | 5.796 | 0.202 | 0.459 | |||
| Resilience | −0.148 *** | −0.230 | 0.048 | −4.771 | −0.308 | −0.118 | |||
| Social support | −0.124 *** | −0.160 | 0.038 | −4.204 | −0.266 | −0.110 | |||
| Enacted stigma × Social support | 0.194 *** | 0.039 | 0.006 | 6.194 | 0.027 | 0.052 | |||
| Perceived stigma × Social support | −0.188 *** | −0.030 | 0.005 | −4.582 | −0.035 | −0.014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, T.; Chen, Q.; Zhong, X. A Study of the Relationship between Men Who Have Sex with Men Stigma and Depression: A Moderated Mediation Model. Healthcare 2023, 11, 2849. https://doi.org/10.3390/healthcare11212849
Zhou T, Chen Q, Zhong X. A Study of the Relationship between Men Who Have Sex with Men Stigma and Depression: A Moderated Mediation Model. Healthcare. 2023; 11(21):2849. https://doi.org/10.3390/healthcare11212849
Chicago/Turabian StyleZhou, Tianyi, Qiao Chen, and Xiaoni Zhong. 2023. "A Study of the Relationship between Men Who Have Sex with Men Stigma and Depression: A Moderated Mediation Model" Healthcare 11, no. 21: 2849. https://doi.org/10.3390/healthcare11212849
APA StyleZhou, T., Chen, Q., & Zhong, X. (2023). A Study of the Relationship between Men Who Have Sex with Men Stigma and Depression: A Moderated Mediation Model. Healthcare, 11(21), 2849. https://doi.org/10.3390/healthcare11212849