
Changes in Reaction Time, Balance and Neuroplasticity after Exercise with a Face Mask in Male Adults with Mild COVID-19 Symptoms

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
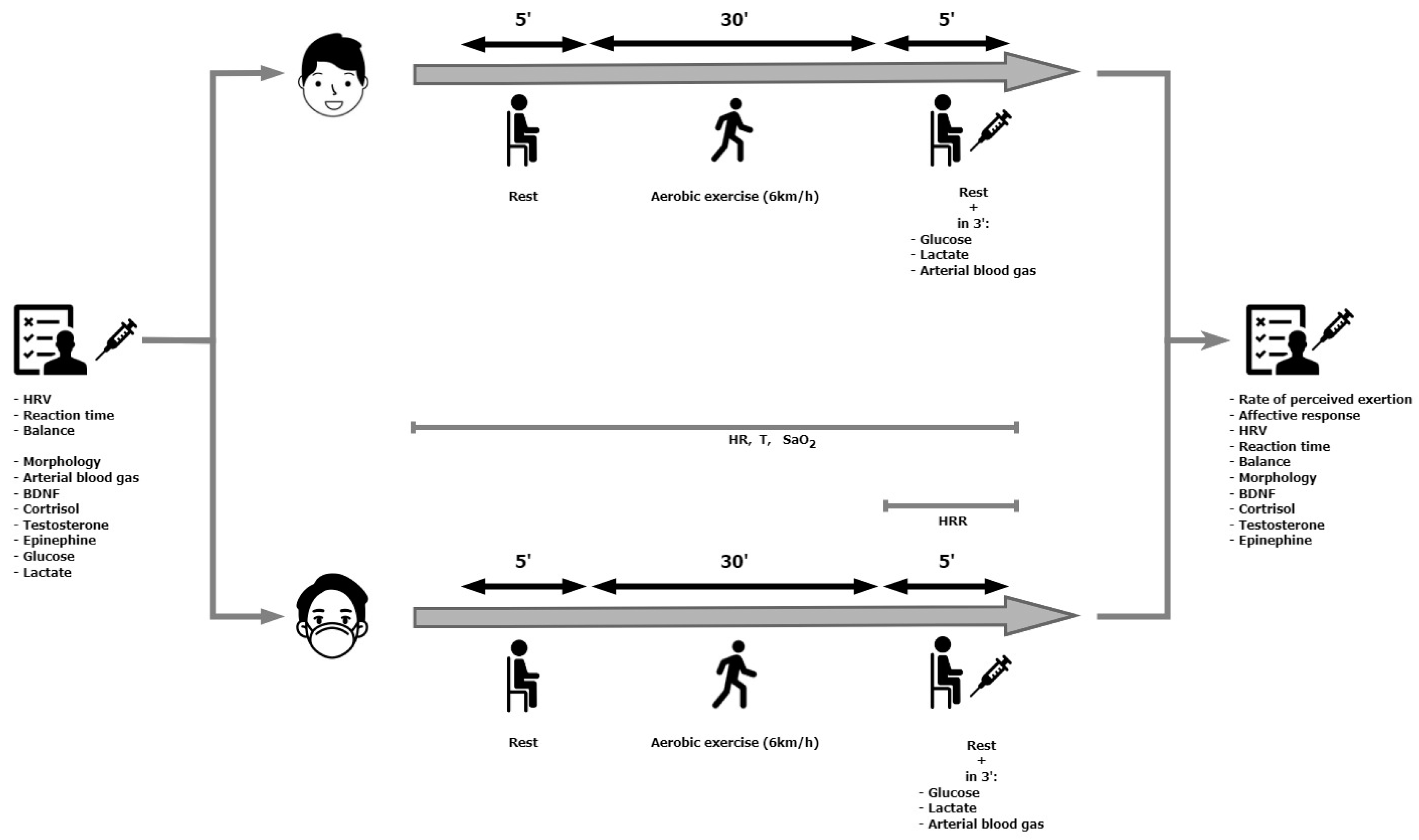
2.2. Study Design
2.3. Body Composition Analysis
2.4. Measurement of Choice Reaction Time
2.5. Balance Assessment
2.6. Biochemical Measurements
2.7. Prolonged Exercise with and without a Surgical Face Mask
2.8. Physiological Measurements
2.9. Psychological Responses
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cossarizza, A.; De Biasi, S.; Guaraldi, G.; Girardis, M.; Mussini, C. SARS-CoV-2, the Virus that Causes COVID-19: Cytometry and the New Challenge for Global Health. Cytometry A 2020, 97, 340–343. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 weekly epidemiological update, edition 159. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1-september-2023 (accessed on 11 September 2023).
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.M.; Wang, Y.P. Response to Char’s comment: Comment on Li et al.: COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 1433. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the Nervous System. Cell 2020, 183, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Hanif, M.; Ali, M.J.; Haider, M.A.; Kherani, D.; Memon, G.M.; Karim, A.H.; Sattar, A. Neurological Manifestations of COVID-19 (SARS-CoV-2): A Review. Front. Neurol. 2020, 11, 518. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. Preprint. medRxiv 2021, 11, 16144. [Google Scholar] [CrossRef]
- Costa, Í.F.; Bonifácio, L.P.; Bellissimo-Rodrigues, F.; Rocha, E.M.; Jorge, R.; Bollela, V.R.; Antunes-Foschini, R. Ocular Findings among Patients Surviving COVID-19. Sci. Rep. 2021, 11, 11085. [Google Scholar] [CrossRef] [PubMed]
- Lechner-Scott, J.; Levy, M.; Hawkes, C.; Yeh, A.; Giovannoni, G. Long COVID or post COVID-19 syndrome. Mult. Scler. Relat. Disord. 2021, 55, 103268. [Google Scholar] [CrossRef]
- Hugon, J.; Msika, E.F.; Queneau, M.; Farid, K.; Paquet, C. Long COVID: Cognitive complaints (brain fog) and dysfunction of the cingulate cortex. J. Neurol. 2022, 269, 44–46. [Google Scholar] [CrossRef]
- Ferrucci, R.; Dini, M.; Groppo, E.; Rosci, C.; Reitano, M.R.; Bai, F.; Poletti, B.; Brugnera, A.; Silani, V.; Monforte, A.D.; et al. Long-Lasting Cognitive Abnormalities after COVID-19. Brain Sci. 2021, 11, 235. [Google Scholar] [CrossRef]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef]
- Klein, R.; Soung, A.; Sissoko, C.; Nordvig, A.; Canoll, P.; Mariani, M.; Jiang, X.; Bricker, T.; Goldman, J.; Rosoklija, G. COVID-19 induces neuroinflammation and loss of hip-pocampal neurogenesis. Res. Sq. 2021, 3, rs-1031824. [Google Scholar] [CrossRef]
- Ramos-Campo, D.J.; Pérez-Piñero, S.; Muñoz-Carrillo, J.C.; López-Román, F.J.; García-Sánchez, E.; Ávila-Gandía, V. Acute Effects of Surgical and FFP2 Face Masks on Physiological Responses and Strength Performance in Persons with Sarcopenia. Biology 2021, 10, 213. [Google Scholar] [CrossRef] [PubMed]
- Brüssow, H.; Zuber, S. Can a combination of vaccination and face mask wearing contain the COVID-19 pandemic? Microb. Biotechnol. 2022, 15, 721–737. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Yang, H.; Zhang, M.; Liu, Q.; Alotaibi, G.; Irfan, M.; He, H.; Chang, J.; Liang, X.J.; Weng, Y.; et al. mRNA vaccines for COVID-19 and diverse diseases. J. Control. Release 2022, 345, 314–333. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain. Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Alomari, M.A.; Khabour, O.F.; Alzoubi, K.H. Changes in physical activity and sedentary behavior amid confinement: The BKSQ-COVID-19 project. Risk Manag. Healthc. Policy 2020, 13, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Rodulfo, J.I.A. Sedentarism, a disease from xxi century. Clin. Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef]
- Smith, J.D.; MacDougall, C.C.; Johnstone, J.; Copes, R.A.; Schwartz, B.; Garber, G.E. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: A systematic review and meta-analysis. CMAJ 2016, 188, 567–574. [Google Scholar] [CrossRef]
- Shaw, K.; Butcher, S.; Ko, J.; Zello, G.A.; Chilibeck, P.D. Wearing of Cloth or Disposable Surgical Face Masks has no Effect on Vigorous Exercise Performance in Healthy Individuals. Int. J. Environ. Res. Public Health 2020, 17, 8110. [Google Scholar] [CrossRef]
- Driver, S.; Reynolds, M.; Brown, K. Effects of wearing a cloth face mask on performance, physiological and perceptual responses during a graded treadmill running exercise test. Br. J. Sports Med. 2022, 56, 107–113. [Google Scholar] [CrossRef]
- Hopkins, S.R.; Dominelli, P.B.; Davis, C.K. Face Masks and the Cardiorespiratory Response to Physical Activity in Health and Disease. Ann. Am. Thorac. Soc. 2021, 18, 399–407. [Google Scholar] [CrossRef]
- Ogawa, T.; Koike, J.; Hirano, Y. The effects of cloth face masks on cardiorespiratory responses and VO2 during maximal incremental running protocol among apparently healthy men. Sci. Rep. 2022, 12, 22292. [Google Scholar] [CrossRef] [PubMed]
- Fikenzer, S.; Uhe, T.; Lavall, D. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin. Res. Cardiol. 2020, 109, 1522–1530. [Google Scholar] [CrossRef] [PubMed]
- Lässing, J.; Falz, R.; Pökel, C. Effects of surgical face masks on cardiopulmonary parameters during steady state exercise. Sci. Rep. 2020, 10, 22363. [Google Scholar] [CrossRef]
- Doherty, C.J.; Mann, L.M.; Angus, S.A.; Chan, J.S.; Molgat-Seon, Y.; Dominelli, P.B. Impact of wearing a surgical and cloth mask during cycle exercise. Appl. Physiol. Nutr. Metab. 2021, 46, 753–762. [Google Scholar] [CrossRef]
- Epstein, D.; Korytny, A.; Isenberg, Y. Return to training in the COVID-19 era: The physiological effects of face masks during exercise. Scand. J. Med. Sci. Sports 2021, 31, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, B.; Fernandes, S. “Exercise with facemask; Are we handling a devil’s sword?”—A physiological hypothesis. Med. Hypotheses 2020, 144, 110002. [Google Scholar] [CrossRef]
- An, N.; Chuo, J. Walking and Activeness: The First Step toward the Prevention of Strokes and Mental Illness. Comput. Intell. Neurosci. 2022, 2022, 3440437. [Google Scholar] [CrossRef]
- Vuillerme, N.; Sporbert, C.; Pinsault, N. Postural adaptation to unilateral hip muscle fatigue during human bipedal standing. Gait Posture 2009, 30, 122–125. [Google Scholar] [CrossRef]
- Paillard, T. Effects of general and local fatigue on postural control: A review. Neurosci. Biobehavi. Rev. 2012, 36, 162–176. [Google Scholar] [CrossRef]
- Taylor, J.L.; Butler, J.E.; Gandevia, S.C. Changes in muscle afferents, motoneurons and motor drive during muscle fatigue. Eur. J. Appl. Physiol. 2000, 83, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Yaggie, J.A.; McGregor, S.J. Effects of isokinetic ankle fatigue on the maintenance of balance and postural limits. Arch. Phys. Med. Rehabil. 2002, 83, 224–228. [Google Scholar] [CrossRef]
- Pavelka, R.; Třebický, V.; Třebická Fialová, J.; Zdobinský, A.; Coufalová, K.; Havlíček, J.; Tufano, J.J. Acute fatigue affects reaction times and reaction consistency in Mixed Martial Arts fighters. PLoS ONE 2020, 15, e0227675. [Google Scholar] [CrossRef] [PubMed]
- Lepers, R.; Bigard, A.X.; Diard, J.P.; Gouteyron, J.F.; Guezennec, C.Y. Posture control after prolonged exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 76, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Dzięcioł-Anikiej, Z.; Dakowicz, A.; Dzięcioł, J. Balance Disorders in People with History of COVID-19 in Light of Posturographic Tests. J. Clin. Med. 2023, 12, 4461. [Google Scholar] [CrossRef]
- Joli, J.; Buck, P.; Zipfel, S.; Stengel, A. Post-COVID-19 fatigue: A systematic review. Front. Psychiatry 2022, 13, 947973. [Google Scholar] [CrossRef]
- Vollrath, S.; Matits, L.; Schellenberg, J.; Kirsten, J.; Steinacker, J.M.; Bizjak, D.A. Decreased physical performance despite objective and subjective maximal exhaustion in post-COVID-19 individuals with fatigue. Eur. J. Med. Res. 2023, 28, 298. [Google Scholar] [CrossRef] [PubMed]
- Żychowska, M.; Jaworecka, K.; Mazur, E. COVID-19 and Postural Control-A Stabilographic Study Using Rambling-Trembling Decomposition Method. Med. Kaunas 2022, 58, 305. [Google Scholar] [CrossRef]
- Guzik, A.; Wolan-Nieroda, A.; Kochman, M.; Perenc, L.; Drużbicki, M. Impact of mild COVID-19 on balance function in young adults, a prospective observational study. Sci. Rep. 2022, 12, 12181. [Google Scholar] [CrossRef]
- Santoyo-Mora, M.; Villaseñor-Mora, C.; Cardona-Torres, L.M. COVID-19 Long-Term Effects: Is There an Impact on the Simple Reaction Time and Alternative-Forced Choice on Recovered Patients? Brain Sci. 2022, 12, 1258. [Google Scholar] [CrossRef] [PubMed]
- Maiorana, N.V.; Aiello, E.N.; Poletti, B. Relationship between Reaction Times and Post-COVID-19 Symptoms Assessed by a Web-Based Visual Detection Task. Healthcare 2023, 11, 284. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-%20room/factsheets/%20detail/physical-activity (accessed on 11 September 2023).
- van Praag, H. Exercise and the brain: Something to chew on. Trends Neurosci. 2009, 32, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Di Liegro, C.M.; Schiera, G.; Proia, P.; Di Liegro, I. Physical Activity and Brain Health. Genes 2019, 10, 720. [Google Scholar] [CrossRef]
- Hassanlouei, H.; Falla, D.; Arendt-Nielsen, L.; Kersting, U.G. The effect of six weeks endurance training on dynamic muscular control of the knee following fatiguing exercise. J. Electromyogr. Kines. 2014, 5, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Leckie, R.L.; Oberlin, L.E.; Voss, M.W.; Prakash, R.S.; Szabo-Reed, A.; Chaddock-Heyman, L.; Phillips, S.M.; Gothe, N.P.; Mailey, E.; Vieira-Potter, V.J.; et al. BDNF mediates improvements in executive function following a 1-year exercise intervention. Front. Hum. Neurosci. 2014, 8, 985. [Google Scholar] [CrossRef]
- Cai, M.; Wang, H.; Song, H.; Yang, R.; Wang, L.; Xue, X.; Sun, W.; Hu, J. Lactate Is Answerable for Brain Function and Treating Brain Diseases: Energy Substrates and Signal Molecule. Front. Nutr. 2022, 28, 9:800901. [Google Scholar] [CrossRef]
- Levy, B. Bench-to-bedside review: Is there a place for epinephrine in septic shock? Crit. Care 2005, 9, 561–565. [Google Scholar] [CrossRef][Green Version]
- Spritzer, M.D.; Roy, E.A. Testosterone and Adult Neurogenesis. Biomolecules 2020, 3, 225. [Google Scholar] [CrossRef] [PubMed]
- Issa, G.; Wilson, C.; Terry, A.V., Jr.; Pillai, A. An inverse relationship between cortisol and BDNF levels in schizophrenia: Data from human postmortem and animal studies. Neurobiol. Dis. 2010, 39, 327–333. [Google Scholar] [CrossRef]
- Ida, M.; Ida, I.; Wada, N.; Sohmiya, M.; Tazawa, M.; Shirakura, K. A clinical study of the efficacy of a single session of individual exercise for depressive patients, assessed by the change in saliva free cortisol level. Biopsychosoc. Med. 2013, 7, 18. [Google Scholar] [CrossRef]
- Groti Antonic, K.; Antonic, B.; Caliber, M.; Dhindsa, S. Men, testosterone and Covid-19. Clin. Endocrinol. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Toscano-Guerra, E.; Martínez-Gallo, M.; Arrese-Muñoz, I.; Giné, A.; Díaz-Troyano, N.; Gabriel-Medina, P.; Riveiro-Barciela, M.; Labrador-Horrillo, M.; Martinez-Valle, F.; Montalvá, A.S.; et al. Recovery of serum testosterone levels is an accurate predictor of survival from COVID-19 in male patients. BMC Med. 2022, 20, 129. [Google Scholar] [CrossRef]
- Salonia, A.; Pontillo, M.; Capogrosso, P.; Gregori, S.; Carenzi, C.; Ferrara, A.M.; Rowe, I.; Boeri, L.; Larcher, A.; Ramirez, G.A.; et al. Testosterone in males with COVID-19: A 7-month cohort study. Andrology 2022, 10, 34–41. [Google Scholar] [CrossRef]
- Dhindsa, S.; Zhang, N.; McPhaul, M.J.; Wu, Z.; Ghoshal, A.K.; Erlich, E.C.; Mani, K.; Randolph, G.J.; Edwards, J.R.; Mudd, P.A.; et al. Association of Circulating Sex Hormones with Inflammation and Disease Severity in Patients with COVID-19. JAMA Netw. Open 2021, 4, e2111398. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 11 September 2023).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Urbaniak, G.C.; Plous, S. Research Randomizer. 2013. Available online: https://www.randomizer.org/ (accessed on 11 September 2023).
- Jeacocke, N.A.; Burke, L.M. Methods to standardize dietary intake before performance testing. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 87–103. [Google Scholar] [CrossRef]
- Hebisz, P.; Cortis, C.; Hebisz, R. Acute Effects of Sprint Interval Training and Chronic Effects of Polarized Training (Sprint Interval Training, High Intensity Interval Training, and Endurance Training) on Choice Reaction Time in Mountain Bike Cyclists. Int. J. Environ. Res. Public Health 2022, 19, 14954. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Hardy, C.J.; Rejeski, W.J. Not what, but how one feels: The measurement of affect during exercise. J. Sport. Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Richardson, J.T. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Rutkowski, Ł.; Zatoń, M.; Michalik, K. Maximum oxygen uptake and post-exercise recovery in professional road cyclists. Hum. Mov. 2016, 17, 185–189. [Google Scholar] [CrossRef]
- Poon, E.T.; Zheng, C.; Wong, S.H. Effect of Wearing Surgical Face Masks During Exercise: Does Intensity Matter? Front. Physiol. 2021, 26, 775750. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, S.; Sattler, S.M.; Miskowiak, K.W.; Kunalan, K.; Victor, A.; Pedersen, L.; Andreassen, H.F.; Jørgensen, B.J.; Heebøll, H.; Andersen, M.B.; et al. Descriptive analysis of long COVID sequelae identified in a multidisciplinary clinic serving hospitalised and non-hospitalised patients. ERJ Open Res. 2021, 2, 00205–2021. [Google Scholar] [CrossRef] [PubMed]
- Blackmon, K.; Day, G.S.; Powers, H.R.; Bosch, W.; Prabhakaran, D.; Woolston, D.; Pedraza, O. Neurocognitive screening in patients following SARS-CoV-2 infection: Tools for triage. BMC Neurol. 2022, 30, 285. [Google Scholar] [CrossRef] [PubMed]
- Batty, G.D.; Deary, I.J.; Gale, C.R. Pre-pandemic cognitive function and COVID-19 mortality: Prospective cohort study. Eur. J. Epidemiol. 2021, 36, 559–564. [Google Scholar] [CrossRef]
- Deary, I.; Der, G.; Ford, G. Reaction Times and Intelligence Differences a Population-Based Cohort Study. Intelligence 2001, 29, 389–399. [Google Scholar] [CrossRef]
- Rosiak, O.; Szczepanik, M.; Woszczak, M.; Lucas-Grzelczyk, W.; Józefowicz-Korczyńska, M. Ocena skuteczności rehabilitacji przedsionkowej u pacjentów z dysfunkcją błędnika (Effectiveness of vestibular rehabilitation in patients with vestibular dysfunction). Med. Pr. 2019, 18, 545–553. (In Polish) [Google Scholar] [CrossRef]
- Heneka, M.T.; Carson, M.J.; El Khoury, J.; Landreth, G.E.; Brosseron, F.; Feinstein, D.L.; Jacobs, A.H.; Wyss-Coray, T.; Vitorica, J.; Ransohoff, R.M.; et al. Neuroinflammation in Alzheimer’s disease. Lancet Neurol. 2015, 14, 388–405. [Google Scholar] [CrossRef] [PubMed]
- Zanin, L.; Saraceno, G.; Panciani, P.P.; Renisi, G.; Signorini, L.; Migliorati, K.; Fontanella, M.M. SARS-CoV-2 can induce brain and spine demyelinating lesions. Acta Neurochir. 2020, 162, 1491–1494. [Google Scholar] [CrossRef]
- Palao, M.; Fernández-Díaz, E.; Gracia-Gil, J.; Romero-Sánchez, C.M.; Díaz-Maroto, I.; Segura, T. Multiple sclerosis following SARS-CoV-2 infection. Mult. Scler. Relat. Disord. 2020, 45, 102377. [Google Scholar] [CrossRef] [PubMed]
- Bathina, S.; Das, U.N. Brain-derived neurotrophic factor and its clinical implications. Arch. Med. Sci. 2015, 11, 1164–1178. [Google Scholar] [CrossRef] [PubMed]
- Minuzzi, L.G.; Seelaender, M.; Silva, B.S.A.; Cunha, E.D.B.B.; Deus, M.C.; Vasconcellos, F.T.F.; Marqueze, L.F.B.; Gadotti, A.C.; Baena, C.P.; Pereira, T.; et al. COVID-19 Outcome Relates with Circulating BDNF, According to Patient Adiposity and Age. Front. Nutr. 2021, 8, 784429. [Google Scholar] [CrossRef] [PubMed]
- Motaghinejad, M.; Gholami, M. Possible Neurological and Mental Outcomes of COVID-19 Infection: A Hypothetical Role of ACE-2\Mas\BDNF Signaling Pathway. Int. J. Prev. Med. 2020, 11, 84. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Martínez-Ortega, I.A.; Martínez-Vizcaíno, V.; Mesas, A.E.; Notario-Pacheco, B. Immediate effect of high-intensity exercise on brain-derived neurotrophic factor in healthy young adults: A systematic review and meta-analysis. J. Sport. Health Sci. 2022, 11, 367–375. [Google Scholar] [CrossRef]
- Budde, H.; Machado, S.; Ribeiro, P.; Wegner, M. The cortisol response to exercise in young adults. Front. Behav. Neurosci. 2015, 3, 13. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Faidah, H.; Alexiou, A.; Batiha, G.E. Testosterone in COVID-19: An Adversary Bane or Comrade Boon. Front. Cell Infect. Microbiol. 2021, 11, 666987. [Google Scholar] [CrossRef]
- De Nys, L.; Anderson, K.; Ofosu, E.F.; Ryde, G.C.; Connelly, J.; Whittaker, A.C. The effects of physical activity on cortisol and sleep: A systematic review and meta-analysis. Psychoneuroendocrinology 2022, 143, 105843. [Google Scholar] [CrossRef]
- Roviello, V.; Gilhen-Baker, M.; Vicidomini, C.; Roviello, G.N. Forest-bathing and physical activity as weapons against COVID-19: A review. Environ. Chem. Lett. 2022, 20, 131–140. [Google Scholar] [CrossRef]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Overall (n = 40) | Declared (n = 20) | Non-Declared (n = 20) | |||
|---|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | |
| Age (years) | 27.6 ± 6.1 | 26.2–29.0 | 27.8 ± 5.5 | 26.0–29.6 | 27.4 ± 6.8 | 25.2–29.6 |
| Height (cm) | 181.1 ± 5.3 | 179.9–182.3 | 182.2 ± 4.1 | 180.9–183.5 | 180.0 ± 6.1 | 178.1–182.0 |
| Weight (kg) | 81.4 ± 13.0 | 78.6–84.3 | 83.9 ± 14.8 | 79.2–88.7 | 78.9 ± 10.4 | 75.6–82.3 |
| BMI (kg∙m−2) | 24.8 ± 3.9 | 24.0–25.7 | 25.3 ± 4.1 | 23.9–26.6 | 24.4 ± 3.7 | 23.3–25.6 |
| FM (%) | 15.3 ± 6.9 | 13.8–16.9 | 16.9 ± 6.6 * | 14.8–19.0 | 13.8 ± 6.9 | 11.6–16.0 |
| HRmax pred (bpm) | 189 ± 5 | 188–190 | 189 ± 5 | 187–190 | 189 ± 5 | 187–190 |
| SBP (mmHg) | 117.2 ± 15.0 | 113.9–120.5 | 117.6 ± 15.5 | 112.7–122.5 | 116.8 ± 14.6 | 112.1–121.5 |
| DBP (mmHg) | 69.0 ± 9.0 | 67.0–71.0 | 71.0 ± 9.3 * | 68.0–73.9 | 67.0 ± 8.4 | 64.3–69.6 |
| Hb (g∙dL−1) | 14.4 ± 1.0 | 14.2–14.7 | 14.4 ± 0.8 | 14.1–14.7 | 14.5 ± 1.1 | 14.2–14.8 |
| Ht (%) | 43.8 ± 3.7 | 43.0–44.6 | 43.3 ± 4.4 | 41.9–44.7 | 44.3 ± 2.7 | 43.4–45.1 |
| RBC (106∙mm−3) | 4.8 ± 0.3 | 4.8–4.9 | 4.8 ± 0.3 | 4.7–4.9 | 4.9 ± 0.3 | 4.8–5.0 |
| WBC (103∙mm−3) | 5.3 ± 1.1 | 5.1–5.5 | 5.2 ± 1.1 | 4.8–5.5 | 5.4 ± 1.1 | 5.1–5.8 |
| Variable | Declared | Non-Declared | ||||||
|---|---|---|---|---|---|---|---|---|
| Masked | Unmasked | Masked | Unmasked | |||||
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | |
| Physiological | ||||||||
| HRav [bpm] | 103 ± 9 | 98–107 | 99 ± 8 | 96–103 | 102 ± 14 | 96–109 | 104 ± 14 | 97–110 |
| %HRPRED [%] | 53.9 ± 4.7 | 51.7–56.2 | 52.4 ± 4.4 | 50.4–54.8 | 54.2 ± 7.5 | 50.7–57.7 | 55.0 ± 7.4 | 51.6–58.5 |
| HRpeak [bpm] | 113 ± 11 | 108–119 | 110 ± 9 | 105–114 | 113 ± 14 | 107–120 | 114 ± 14 | 108–121 |
| HRR [bpm] | 81 ± 11 | 76–86 | 79 ± 12 | 73–84 | 82 ± 18 | 74–91 | 81 ± 16 | 74–89 |
| rMSSD pre [ms] | 53.9 ± 42.6 | 34.0–73.8 | 71.0 ± 58.2 | 43.8–98.3 | 66.7 ± 48.1 | 44.2–89.2 | 71.9 ± 38.5 | 53.9–89.9 |
| rMSSD post [ms] | 54.0 ± 27.3 | 41.2–66.7 | 66.4 ± 54.6 | 40.9–92.0 | 64.5 ± 59.5 | 36.7–92.4 | 61.5 ± 39.1 | 43.2–79.7 |
| LF/HF pre | 2.4 ± 2.3 | 1.3–3.4 | 2.5 ± 3.5 | 0.9–4.2 | 3.1 ± 4.9 | 0.8–5.4 | 2.5 ± 4.5 | 0.4–4.7 |
| LF/HF post | 2.5 ± 3.0 | 1.1–3.9 | 3.0 ± 4.3 | 1.0–5.0 | 3.2 ± 5.3 | 0.7–5.7 | 2.6 ± 4.0 | 0.7–4.5 |
| SaO2av [%] | 97.3 ± 0.8 | 96.9–97.7 | 97.5 ± 0.9 | 97.1–97.9 | 97.1 ± 1.0 | 96.7–97.5 | 97.2 ± 0.8 | 96.8–97.5 |
| Psychological | ||||||||
| RPE [6–20] | 9.1 ± 1.9 | 8.2–10.0 | 8.7 ± 2.2 | 7.6–9.7 | 8.9 ± 2.2 | 7.9–9.9 | 8.1 ± 2.2 | 7.0–9.1 |
| AR [−5 to +5] | 2.4 ± 2.1 | 1.4–3.3 | 3.1 ± 1.9 | 2.2–4.0 | 2.5–2.0 | 1.5–3.4 | 3.2 ± 1.8 | 2.3–4.1 |
| Variable | Declared | Non-Declared | ||||||
|---|---|---|---|---|---|---|---|---|
| Masked | Unmasked | Masked | Unmasked | |||||
| Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | |
| RTav pre [s] | 0.34 ± 0.04 | 0.32–0.36 | 0.35 ± 0.04 | 0.33–0.36 | 0.34 ± 0.03 | 0.32–0.35 | 0.34 ± 0.03 | 0.32–0.35 |
| RTav post [s] | 0.34 ± 0.04 | 0.33–0.36 | 0.35 ± 0.04 | 0.33–0.37 | 0.34 ± 0.03 | 0.32–0.36 | 0.34 ± 0.04 | 0.32–0.36 |
| RTmin pre [s] | 0.24 ± 0.03 | 0.22–0.26 | 0.25 ± 0.02 | 0.24–0.26 | 0.24 ± 0.03 | 0.22–0.25 | 0.24 ± 0.03 | 0.23–0.25 |
| RTmin post [s] | 0.25 ± 0.02 | 0.24–0.26 | 0.25 ± 0.03 | 0.23–0.26 | 0.23 ± 0.02 | 0.22–0.24 | 0.24 ± 0.04 | 0.22–0.26 |
| RTmax pre [s] | 0.51 ± 0.10 | 0.47–0.56 | 0.53 ± 0.12 | 0.47–0.58 | 0.51 ± 0.08 | 0.47–0.54 | 0.48 ± 0.08 | 0.44–0.52 |
| RTmax post [s] | 0.49 ± 0.09 | 0.45–0.53 | 0.53 ± 0.10 | 0.48–0.58 | 0.48 ± 0.08 | 0.44–0.52 | 0.53 ± 0.12 | 0.48–0.59 |
| NCR pre [n] | 16.3 ± 0.7 | 15.9–16.6 | 16.5 ± 0.8 | 16.1–16.9 | 16.2 ± 0.9 | 15.8–16.6 | 16.4 ± 1.2 | 15.8–17.0 |
| NCR post [n] | 16.9 ± 0.4 | 16.7–17.0 | 16.8 ± 0.4 | 16.6–17.0 | 16.7 ± 0.7 | 16.4–17.0 | 16.7 ± 0.5 | 16.5–16.9 |
| Variable | Declared | Non-Declared | ||||||
|---|---|---|---|---|---|---|---|---|
| Masked | Unmasked | Masked | Unmasked | |||||
| Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | |
| EO COPL pre [cm] | 22.5 ± 4.9 | 20.2–24.8 | 22.3 ± 6.9 | 19.1–25.6 | 23.9 ± 9.7 | 19.4–28.4 | 20.9 ± 7.0 | 17.6–24.1 |
| EO COPL post [cm] | 23.5 ± 7.5 | 20.0–27.0 | 22.9 ± 5.6 | 20.3–25.6 | 22.2 ± 5.1 | 19.8–24.6 | 20.4 ± 5.3 | 18.0–22.9 |
| EC COPL pre [cm] | 29.0 ± 10.1 | 24.2–33.7 | 33.5 ± 18.6 | 24.8–42.3 | 31.0 ± 12.5 | 25.1–36.9 | 31. ± 15.4 | 24.2–38.6 |
| EC COPL post [cm] | 17.5 ± 10.8 | 22.4–32.6 | 28.1 ± 10.0 | 23.4–32.8 | 27.8 ± 9.6 | 23.2–32.3 | 19.6 ± 14.4 | 22.8–36.4 |
| EO COPA pre [cm2] | 2.5 ± 1.8 | 1.6–3.3 | 2.0 ± 1.3 | 1.4–2.6 | 1.5 ± 0.9 | 1.1–1.9 | 1.6 ± 1.0 | 1.2–2.1 |
| EO COPA post [cm2] | 2.8 ± 1.8 | 1.9–3.6 | 3.0 ± 2.3 | 1.9–4.1 | 1.9 ± 0.9 | 1.5–2.4 | 2.1 ± 1.5 | 1.4–2.8 |
| EC COPA pre [cm2] | 2.1 ± 0.9 | 1.6–2.5 | 2.9 ± 2.4 | 1.8–4.0 | 1.6 ± 0.7 | 1.2–1.9 | 1.9 ± 1.0 | 1.4–2.3 |
| EC COPA post [cm2] | 2.5 ± 2.0 | 1.5–3.4 | 2.4 ± 1.6 | 1.7–3.2 | 1.7 ± 1.1 | 1.2–2.2 | 1.8 ± 1.2 | 1.3–2.4 |
| Variable | Declared | Non-Declared | ||||||
|---|---|---|---|---|---|---|---|---|
| Masked | Unmasked | Masked | Unmasked | |||||
| Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | Mean ± SD | 95%CI | |
| Metabolic | ||||||||
| Glu pre [mg∙dL−1] | 99.7 ± 7.9 | 96.0–103.3 | 95.2 ± 5.9 | 92.4–97.9 | 97.5 ± 7.8 | 93.8–101.2 | 97.0 ± 9.5 | 92.5–101.5 |
| Glu post [mg∙dL−1] | 96.4 ± 8.1 | 92.6–100.1 | 94.0 ± 8.8 | 89.8–98.1 | 93.4 ± 9.1 | 89.1–97.6 | 91.3 ± 8.3 | 87.4–95.1 |
| [La−] pre [mmol∙L−1] | 1.3 ± 0.4 | 1.1–1.5 | 1.1 ± 0.5 | 0.9–1.4 | 1.0 ± 0.4 | 0.8–1.2 | 1.0 ± 0.6 | 0.8–1.3 |
| [La−] post [mmol∙L−1] | 1.2 ± 0.3 | 1.0–1.3 | 0.8 ± 0.5 | 0.6–1.1 | 1.0 ± 0.5 | 0.8–1.2 | 1.0 ± 0.7 | 0.8–1.4 |
| [H+] pre [nmol∙L−1] | 41.0 ± 1.9 | 40.1–41.8 | 40.4 ± 1.7 | 39.6–41.1 | 40.9 ± 1.9 | 40.0–41.7 | 40.6 ± 1.1 | 40.1–41.1 |
| [H+] post [nmol∙L−1] | 38.9 ± 1.3 * | 38.2–39.5 | 38.4 ± 1.6 * | 37.6–39.1 | 39.1 ± 1.4 * | 38.4–39.8 | 39.2 ± 1.4 * | 38.6–39.9 |
| pCO2 pre [mm Hg] | 42.6 ± 3.3 | 41.0–44.1 | 42.7 ± 3.3 | 41.1–44.2 | 41.4 ± 2.2 | 40.4–42.5 | 41.4 ± 2.3 | 40.4–42.5 |
| pCO2 post [mm Hg] | 40.9 ± 2.2 | 39.8–41.9 | 41.1 ± 2.1 | 40.1–42.0 | 40.3 ± 2.1 | 39.3–41.3 | 40.4 ± 3.6 | 38.7–42.1 |
| [HCO3−] pre [mmol∙L−1] | 25.1 ± 1.6 | 24.3–25.8 | 25.5 ± 1.6 | 24.8–26.2 | 24.5 ± 1.3 | 23.9–25.1 | 24.6 ± 1.2 | 24.1–25.1 |
| [HCO3−] post [mmol∙L−1] | 25.3 ± 1.1 | 24.8–25.8 | 25.8 ± 1.2 | 25.3–26.4 | 24.9 ± 1.3 | 24.3–25.5 | 25.1 ± 1.0 | 24.7–25.6 |
| Hormonal | ||||||||
| BDNF pre [ng∙mL−1] | 277.7 ± 105.9 | 228.1–327.2 | 256.0 ± 95.4 | 211.3–300.6 | 270.9 ± 98.7 | 224.7–317.0 | 266.2 ± 116.2 | 211.8–320.6 |
| BDNF post [ng∙mL−1] | 270.1 ± 116.9 | 215.4–324.8 | 254.5 ± 118.5 | 199.0–309.9 | 250.3–120.5 | 193.9–306.8 | 256.0 ± 108.1 | 205.4–306.6 |
| T pre [ng∙dL−1] | 888.6 ± 278.7 | 758.1–1019.0 | 892.9 ± 271.8 | 765.7–1020.1 | 1074.2 ± 319.4 | 924.7–1223.7 | 1012.5 ± 317.7 | 863.8–1161.2 |
| T post [ng∙dL−1] | 855.2 ± 246.5 | 739.8–970.5 | 805.9 ± 305.2 | 663.1–948.8 | 1048.1 ± 303.2 | 906.2–1190.0 | 969.5 ± 367.3 | 797.5–1141.4 |
| C pre [ng∙mL−1] | 164.8 ± 62.5 | 135.6–194 | 149.8 ± 68.1 | 117.9–181.7 | 155.2 ± 74.3 | 120.4–190.0 | 145.6 ± 84.7 | 106.0–185.2 |
| C post [ng∙mL−1] | 93.0 ± 25.2 * | 76.6–109.5 | 82.4 ± 37.0 * | 65.1–99.7 | 90.1 ± 44.7 * | 69.2–111.1 | 87.2 ± 42.6 * | 67.2–107.1 |
| E pre [pg∙mL−1] | 64.2 ± 15.0 | 57.1–71.2 | 64.7 ± 16.3 | 57.1–72.4 | 62.3 ± 13.2 | 56.1–68.4 | 58.1 ± 13.5 | 51.7–64.4 |
| E post [pg∙mL−1] | 62.3 ± 15.6 | 54.9–69.6 | 59.8 ± 14.4 | 53.0–66.5 | 62.6 ± 13.3 | 56.4–68.8 | 58.4 ± 13.3 | 52.2–64.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalik, K.; Smolarek, M.; Borkowski, J.; Tchorowski, M.; Korczuk, N.; Gorczyca, P.; Wojtarowicz, N.; Zatoń, M. Changes in Reaction Time, Balance and Neuroplasticity after Exercise with a Face Mask in Male Adults with Mild COVID-19 Symptoms. Healthcare 2023, 11, 2800. https://doi.org/10.3390/healthcare11202800
Michalik K, Smolarek M, Borkowski J, Tchorowski M, Korczuk N, Gorczyca P, Wojtarowicz N, Zatoń M. Changes in Reaction Time, Balance and Neuroplasticity after Exercise with a Face Mask in Male Adults with Mild COVID-19 Symptoms. Healthcare. 2023; 11(20):2800. https://doi.org/10.3390/healthcare11202800
Chicago/Turabian StyleMichalik, Kamil, Marcin Smolarek, Jacek Borkowski, Miłosz Tchorowski, Natalia Korczuk, Piotr Gorczyca, Natalia Wojtarowicz, and Marek Zatoń. 2023. "Changes in Reaction Time, Balance and Neuroplasticity after Exercise with a Face Mask in Male Adults with Mild COVID-19 Symptoms" Healthcare 11, no. 20: 2800. https://doi.org/10.3390/healthcare11202800
APA StyleMichalik, K., Smolarek, M., Borkowski, J., Tchorowski, M., Korczuk, N., Gorczyca, P., Wojtarowicz, N., & Zatoń, M. (2023). Changes in Reaction Time, Balance and Neuroplasticity after Exercise with a Face Mask in Male Adults with Mild COVID-19 Symptoms. Healthcare, 11(20), 2800. https://doi.org/10.3390/healthcare11202800