
Basic Health Service Delivery to Vulnerable Populations in Post-Conflict Eastern Congo: Asset Mapping
 ,
,
Abstract
:1. Introduction
Theoretical Framework
2. Material and Methods
2.1. Study Settings and Participants
2.2. Study Procedures
2.3. Data Sources
2.4. Data Analysis
2.5. Ethics Statement
3. Results
3.1. Participants’ Characteristics
3.2. Study Phase One: Asset-Mapping Survey and Community Walk(s)
3.3. Phase Two: Community Engagement Mapping
“…if a member of the local association becomes ill, he/she can borrow money from the association, use it to pay for basic healthcare, and pay it back to the association gradually. As a member of the local association, you can also borrow money and start a small business.”CEM participant, Walungu
“The local associations are not negatively linked to health inequalities, on the contrary, the members of a solidarity association must ensure that one of them benefits from good quality care by making contributions, each according to his or her means, if the sick person is not able to take care of him or herself.”CEM participant, Bukavu
“…young people need fields to practice their sports and discover their talents. But, sports fields are not always ready to be used because rivers flood in many areas. Other physical areas are used as reception centers for victims of conflict where physical and psychological care are offered, and also the same areas are used by the community for income-generating activities.”CEM participant, Walungu
“Sport is very important for everyone’s health, especially young people who need these spaces to train in football and basketball.”CEM participant, Bukavu
“We don’t think that these places could be linked to health inequalities. We don’t think it’s related.”CEM participant, Goma
“Often these physical spaces are only involved in tourism.”CEM participant, Kigonze
“Schools must teach children and young people that we are all equal, with or without money, and we all have the right to health care. But also our children are often injured by their peers at school when we cannot afford to take them to the health center.”CEM participant, Shasha
“Local institutions take care of their workers and offer them health insurance. With this, the workers will have better access to health care. Often the people who are best taken care of in hospitals are those who have health care insurance from these institutions.”CEM participant, Bukavu
“Speaking of health, doctors and nurses are the most concerned, as they are the ones who experience health inequalities in hospitals, health centers, and communities.”CEM participant, Bukavu
“…these people create jobs in our area. If you have a job, you will be able to feed your family and help everyone to be in good health.”CEM participants, Walungu
“If we don’t have money, we cannot access basic health care. So, we work every day to gain money, buy food and feed our families, buy medicines in case of illnesses, or go to the hospital if very sick.”CEM participant, Ihimbi
“We all know that inequalities in health are much more linked to the economy, as soon as you don’t have the money you can’t be taken care of.”CEM participant, Shasha
3.4. Mobilizing Identified Assets for Collective Action
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABAs | Assets-based approaches |
| ABCD | Asset-based community development |
| AMS | Asset mapping survey |
| BHS | Basic health service |
| BDOM | Bureau Diocésain des Œuvres Médicales |
| CEM | Community engagement mapping |
| DRC | Democratic Republic of Congo |
| HA | Health assets |
| NACCHO | National Association of County and City Health Officials |
| NBAs | Needs-based approaches |
| PCHR | Post-conflict health rehabilitation |
| PHAB | Public Health Accreditation Board |
| RISD | Research initiatives for social development |
| WHO | World Health Organization |
Appendix A. Asset-Mapping Survey: Interview Guide
| Where Do You Go for/to…? (Include Approximate Location) | Do You Consider This Place an Asset? | Do You Consider This Place a “Source of Pride”? | |
| Mental health services? | |||
| Healthcare? | |||
| Become involved in community issues? | |||
| Have fun? | |||
| Socialize and get together with friends? | |||
| Work? | |||
| School? | |||
| Buy groceries? | |||
| Purchase non-food items? |
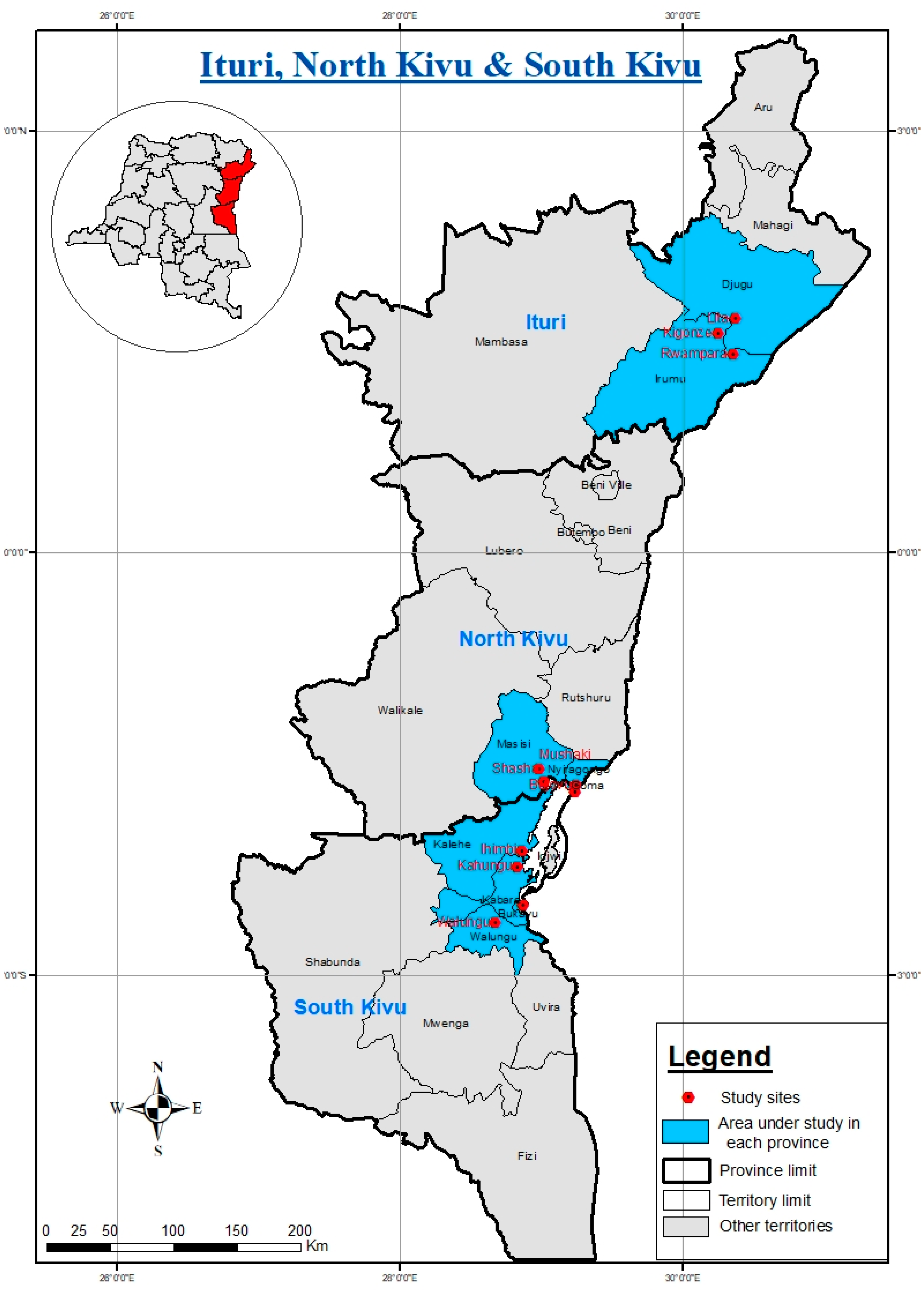
Appendix B. DRC Map Showing Study Area in Ituri, North and South Kivu
References
- Kruk, M.E.; Rockers, P.C.; Williams, E.H.; Varpilah, S.T.; Macauley, R.; Saydee, G.; Galea, S. Availability of essential health services in post-conflict Liberia. Bull. World Health Organ. 2010, 88, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.S.; Sidel, V.W. Documenting the effects of armed conflict on population health. Annu. Rev. Public Health 2016, 37, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Batniji, R.; Khatib, L.; Cammett, M.; Sweet, J.; Basu, S.; Jamal, A.; Wise, P.; Giacaman, R. Governance and health in the Arab world. Lancet 2014, 383, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Mowafi, H. Conflict, displacement and health in the Middle East. Glob. Public Health 2011, 6, 472–487. [Google Scholar] [CrossRef]
- Martineau, T.; McPake, B.; Theobald, S.; Raven, J.; Ensor, T.; Fustukian, S.; Ssengooba, F.; Chirwa, Y.; Vong, S.; Wurie, H. Leaving no one behind: Lessons on rebuilding health systems in conflict-and crisis-affected states. BMJ Glob. Health 2017, 2, e000327. [Google Scholar] [CrossRef]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promot. Educ. 2007, 14, 17–22. [Google Scholar] [CrossRef]
- Tones, K.; Green, J. Health Promotion: Planning and Strategies; Sage Publications: Glasgow, UK, 2004. [Google Scholar]
- World Health Organization. Report on Social Determinants of Health and the Health Divide in the WHO European Region: Executive Summary; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2012; p. 45. [Google Scholar]
- McLean, J.; McNeice, V.; Mitchell, C. Asset-Based Approaches in Service Settings: Striking a Balance; Glasgow Centre for Population Health: Glaslow, UK, 2017; p. 194. [Google Scholar]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef]
- Sigerson, D.; Gruer, L. Asset-Based Approaches to Health Improvement; NHS Health Scotland: Glasgow, UK, 2011. [Google Scholar]
- Ruiz-Rosendo, L.; Martin, C. Interpreting for Vulnerable Populations. Available online: https://ojs.uv.es/index.php/JUST/pages/view/3.1 (accessed on 10 July 2023).
- Bwirire, D.; Crutzen, R.; Ntabe Namegabe, E.; Letschert, R.; de Vries, N. Health inequalities in post-conflict settings: A systematic review. PLoS ONE 2022, 17, e0265038. [Google Scholar] [CrossRef]
- McKnight, J.; Kretzmann, J. Introduction to “Building Communities from the Inside Out: A path toward finding and mobilizing a community’s assets”. In A Path toward Finding and Mobilizing a Community’s Assets; ACTA Publications: Chicago, IL, USA, 1993. [Google Scholar]
- Sharpe, P.A.; Greaney, M.L.; Lee, P.R.; Royce, S.W. Assets-oriented community assessment. Public Health Rep. 2000, 115, 205. [Google Scholar] [CrossRef]
- Hormozdyaran, N. Definitions of Health Project. In Modernity, Medicine, and Health; Scambler, G., Higgs, P., Eds.; Routledge: London, UK, 2004. [Google Scholar]
- Lunt, N. Asset-based and strengths-based community initiatives in the UK. Glob. Soc. Secur. Rev. 2019, 1–19. [Google Scholar]
- Waters, H.; Garrett, B.; Burnham, G. Rehabilitating health systems in post-conflict situations. In Making Peace Work: The Challenges of Social and Economic Reconstruction; Springer: London, UK, 2009; pp. 200–227. [Google Scholar]
- Hopkins, T.; Rippon, S. Head, Hands and Heart: Asset-Based Approaches in Health Care; Health Foundations: London, UK, 2015. [Google Scholar]
- Springer, A.E.; Evans, A.E. Assessing environmental assets for health promotion program planning: A practical framework for health promotion practitioners. Health Promot. Perspect. 2016, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Bastick, M.; Grimm, K.; Kunz, R. Sexual violence in armed conflict: Global Overview and Implications for the Security Sector; Geneva Centre for the Democratic Control of Armed Forces: Geneva, Switzerland, 2007. [Google Scholar]
- Turner, T. The Congo Wars: Conflict, Myth and Reality; Zed Books: London, UK, 2007. [Google Scholar]
- Wakabi, W. Sexual Violence Increasing in Democratic Republic of Congo. Lancet 2008, 371, 15–16. [Google Scholar] [CrossRef]
- Ahere, J. The peace process in the DRC: A transformation quagmire. Policy and Practice Brief African Centre for the Constructive Resolution of Disputes (ACCORD). Available online: https://reliefweb.int/report/democratic-republic-congo/peace-process-drc-transformation-quagmire (accessed on 10 July 2023).
- McKnight, J.; Kretzmann, J. Building Communities from the Inside Out: A Path toward Finding and Mobilizing a Community’s Assets; ACTA Publications: Chicago, IL, USA, 1993. [Google Scholar]
- Legard, R.K.; Keegan, J.J.; Ward, K. In-depth interviews. Qual. Res. Pract. Guide Soc. Sci. Stud. Res. 2003, 6, 138–169. [Google Scholar]
- Hughes, E.; Kean, S.; Cuthill, F. Fluctuating power: An exploration of refugee health nursing within the resettlement context in Victoria, Australia. J. Res. Nurs. 2022, 27, 217–228. [Google Scholar] [CrossRef]
- McKnight, J. Asset-Based Community Development: The Essentials; Asset-Based Community Development Institute: Chicago, IL, USA, 2017; p. 4. [Google Scholar]
- Cunningham, G.; Mathie, A. Mobilizing Assets for Community Driven Development; Training Manual; Coady International Institute: Antigonish, NS, Canada, 2008. [Google Scholar]
- Phillips, R.; Pittman, R. An Introduction to Community Development; Routledge: London, UK, 2008. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Drisko, J.W.; Maschi, T. Content Analysis; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Schreier, M. Qualitative Content Analysis in Practice; Sage Publications Inc.: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; GESIS: Klagenfurt, Austria, 2014. [Google Scholar]
- Azungah, T. Qualitative research: Deductive and inductive approaches to data analysis. Qual. Res. J. 2018, 18, 383–400. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol. Rev. 2023, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Basit, T. Manual or electronic? The role of coding in qualitative data analysis. Educ. Res. 2003, 45, 143–154. [Google Scholar] [CrossRef]
- Stuckey, H.L. The second step in data analysis: Coding qualitative research data. J. Soc. Health Diabetes 2015, 3, 007–010. [Google Scholar] [CrossRef]
- Saldaña, J. The Coding Manual for Qualitative Researchers; SAGE Publications Limited: Thousand Oaks, CA, USA, 2021; pp. 1–440. [Google Scholar]
- Kramer, S.; Amos, T.; Lazarus, S.; Seedat, M. The Philosophical Assumptions, Utility and Challenges of Asset Mapping. J. Psychol. Afr. 2012, 22, 537–546. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M. Fair Society, Healthy Lives: The Marmot Review: Strategic Review of Health Inequalities in England Post-2010; Institute of Health Equity: London, UK, 2019. [Google Scholar]
- Mathie, A.; Cunningham, G. From clients to citizens: Asset-based community development as a strategy for community-driven development. Dev. Pract. 2003, 13, 474–486. [Google Scholar] [CrossRef]
- Sacks, E.; Swanson, R.C.; Schensul, J.J.; Gleave, A.; Shelley, K.D.; Were, M.K.; Chowdhury, A.M.; LeBan, K.; Perry, H.B. Community involvement in health systems strengthening to improve global health outcomes: A review of guidelines and potential roles. Int. Q. Community Health Educ. 2017, 37, 139–149. [Google Scholar] [CrossRef]
- Nicolau, M.; Delport, C. A community asset mapping programme for roots-driven sustainable socio-economic change in rural South Africa. Int. J. Sustain. Econ. Soc. Cult. Context 2015, 10, 1. [Google Scholar] [CrossRef]
- WHO. Quality of Care in Fragile, Conflict-Affected and Vulnerable Settings: Taking Action; 9240015205; WHO: Geneva, Switzerland, 2020; p. 72. [Google Scholar]
- Treuhaft, S. Community Mapping for Health Equity Advocacy; Opportunity Agenda and Health Policy Institute: New York, NY, USA, 2009. [Google Scholar]
- Baird, M. Service Delivery in Fragile and Conflict-Affected States; World Bank: Washington, DC, USA, 2011; p. 60. [Google Scholar]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef]
- Bebbington, A.; Woolcock, M.; Guggenheim, S.E.; Olson, E. The Search for Empowerment: Social Capital as Idea and Practice at the World Bank; Kumarian Press: West Hartford, CT, USA, 2006. [Google Scholar]
- Jeannotte, M.S. Story-telling about place: Engaging citizens in cultural mapping. City Cult. Soc. 2016, 7, 35–41. [Google Scholar] [CrossRef]
- Meit, M. Exploring Strategies to Improve Health and Equity in Rural Communities; NORC Walsh Center for Rural Health Analysis: Bethesda, MD, USA, 2018. [Google Scholar]
- Muysken, J. Health as a Principal Determinant of Economic Growth; Maastricht University, Maastricht Economic Research Institute on Innovation: Maastricht, The Netherland, 2003; p. 35. [Google Scholar]
- Cunningham, G.; Peters, B. Asset-Based AND Citizen-Led Development (ABCD); Coady International Institute: Antigonish, NS, Canada, 2018; p. 148. [Google Scholar]
- Lightfoot, E.; McCleary, J.S.; Lum, T. Asset mapping as a research tool for community-based participatory research in social work. Soc. Work. Res. 2014, 38, 59–64. [Google Scholar] [CrossRef]
- Pérez-Wilson, P.; Hernán, M.; Morgan, A.R.; Mena, A. Health assets for adolescents: Opinions from a neighbourhood in Spain. Health Promot. Int. 2015, 30, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Rütten, A.; Abu-Omar, K.; Levin, L.; Morgan, A.; Groce, N.; Stuart, J. Research note: Social catalysts in health promotion implementation. J. Epidemiol. Community Health 2008, 62, 560–565. [Google Scholar] [CrossRef] [PubMed]

| Codes | Definitions | Examples Identified in Transcripts | Creation |
|---|---|---|---|
| Social assets | Connections or relationships formed between individuals who live in the community and their unique skills and contributions | Friends, neighbors, family members, etc. | Before analysis, subject to modification during analysis |
| Physical assets | Physical and virtual spaces, including land, natural resources, and built environments, where information is encountered, gathered, interacted with, and used | Pathways for walking | Before analysis, subject to modification during analysis |
| Institutional assets | Associations of groups of people who come together around a common purpose | Grocery stores, businesses, schools, and other private or government entities | Before analysis, subject to modification during analysis |
| Individual | A person belonging to a community, group of relatives, or other people who have capabilities, abilities, and gifts | This is about individuals and relationships. | Before analysis, subject to modification during analysis |
| Local economy and exchange | Representing the monetary conditions of a community and its people. It also provides information about the business economy of a community. | Local people are working, running their businesses, and purchasing from local stores. Local people and businesses invest in the community. | Before analysis, subject to modification during analysis |
| Culture, history, and stories | An overview of relevant components that should be found in the community | Cinemas, performing arts venues, theaters, live music venues, cultural events, festivals, sporting events, family events, heritage sites, and attractions. | Before analysis, subject to modification during analysis |
| Eastern Congo Provinces | Study Site | Asset-Mapping Survey | Community Walk | Community-Engaged Mapping (CEM) |
|---|---|---|---|---|
| North Kivu | Location | |||
| Goma | 1 | 11 | 11 | |
| Mushake (Masisi) | 1 | 10 | 10 | |
| Bujovu (Nyiragongo) | 1 | 10 | 10 | |
| Shasha (Kirotshe) | 1 | 10 | 10 | |
| South Kivu | Location | |||
| Bukavu | 1 | 15 | 15 | |
| Ihimbi (Kalehe) | 1 | 12 | 12 | |
| Kahungu (Katana) | 1 | 12 | 12 | |
| Walungu | 1 | 15 | 15 | |
| Ituri Province | Location | |||
| Kigonze (Bunia) | 1 | 30 | 30 | |
| Lita (Bahwere) | 1 | 13 | 13 | |
| Rwampara (Shari) | 1 | 15 | 15 | |
| Number of participants | 11 | 153 | 153 |
| Questions | Quotes |
|---|---|
| What are the skills or capabilities that you would like to share with your community? | “I love children because God gave me the grace to have twins three times, So I have a great affection for children. I also live with my parents, they are old and I take care of them.” AMS respondent, Bujovu “I pray for the sick who suffer from evil spirits, I am also a teacher and principal of a primary school.” AMS respondent, Ihimbi “I have lived with my grandmother since the death of my parents, and as soon as she gets sick, I take care of her, using traditional medicines.” AMS respondent, Kahungu “I often intervene when there are conflicts in the community, by directing the victim to the health center or the police. I also take care of victims of sexual violence.” AMS respondent, Shasha “I am more interested in gardening and childcare, these are the two jobs I do the most when I am not in the fields so I am at home with my children.” AMS respondent, Walungu “Childcare, I am a mother in the SOS Bukavu youth home, from house 11 in the Pageco district. We also provide orphans with advice like their biological mothers would do.” AMS respondent, Bukavu “I take care of the sick because I have been a nurse at the Mama RITA dispensary for 4 years, and this is the job I love the most.” AMS respondent Goma “Children’s health and education.” AMS participant, Bahwere “I am very interested in agriculture.” AMS respondent, Rwampara “Advise, when there are problems or a need in the community.” AMS respondent, Kigonze |
| What do you care the most about? | “Issues relating to children care, and teenage pregnancies. Children live with difficulty and often without a stable family and do not grow up in the warmth of a home. This phenomenon is often at the root of street children and banditry.” AMS respondent, Bujovu “Children’s education, these children are our future.” AMS respondent, Ihimbi “Issues relating to the elderly.” AMS participant, Kahungu “Teenage pregnancies. I would like to help them if at least we had a space or give them advice, many of them are uneducated.” AMS respondent, Mushake “Teenage pregnancies, education, and nutrition, because the number of malnourished children is increasing day by day.” AMS respondent, Shasha “Issues relating to children, and family. When the children are well-educated everything goes well in the community over time.” AMS respondent, Walungu “Child and family care.” AMS respondent, Bukavu “Saving the lives of sick people and those in need, inequalities in health that we observe every day. It would be a very big process to eradicate this situation because we are not all financially equal, it is difficult to be all treated the same way.” AMS respondent, Goma “Security in the region but also Breeding.” AMS respondent, Bawerhe “Issues relating to children care and malnutrition.” AMS respondent, Rwampara “issues relating to children, their food, and their health.” AMS respondent, Kigonze |
| Which associations do you belong to? | “I am a member of the association of resellers. I am also a member of the Church.” AMS respondent, Bujovu “I am a member of different associations such as AVEC, Groups of men, the local development committee, and the Church.” AMS respondent, Ihimbi “I belong to different associations such as AVEC, GADIP, and youth parliament.” AMS respondent, Kahungu “I am part of the Solidarity for Social Promotion and Peace, AVEC, AJVDI, and the CEPAC church.” AMS respondent, Shasha “I am a member of the Church but also a member of AVEC.” AMS respondent, Walungu “I don’t belong to any associations because the work I do takes up a lot of my time.” AMS respondent, Bukavu “For the moment, I am only a member of the church.” AMS respondent, Goma “I am a member of the footballer’s committee and a member of the motorcycle drivers committee (ATAMOI).” AMS respondent, Bahwere “I am a member of the motorcycle drivers committee of Ituri (ATAMOI).” AMS respondent, Kigonze |
| Who else do you know (and share the same passion with) in the community? | “The local development committee and the Mutual solidarity fund.” AMS respondent, Ihimbi “The people who help us are the traditional healers.” Kahungu “The MMR association (Maternity at lower risk), which helps pregnant women.” AMS respondent, Shasha “In our church, there are people who educate others on issues concerning their health and how to take care of themselves.” AMS respondent, Walungu “There are many people who have the same passions as me, women who take care of orphaned children.” AMS respondent, Bukavu “I know other nurses I work with, and maybe in the future we will no longer be able to observe these inequalities.” AMS respondent, Goma “Motorcycle taxi drivers.” AMS respondent, Kigonze |
| Community Assets Categorization | Sample Quotes |
|---|---|
| Local Associations | “Educating members of these associations on how to rebuild a community, and how people should live together, Bujovu” “These associations can help by teaching their members health-related subjects. Kahungu” “These associations are not involved in health issues, therefore they cannot be linked to health inequalities. Shasha” “Most of these associations are involved in agriculture. Others provide funding to their members as they look for this money to be well taken care of in health centers and hospitals in case of illness. Ihimbi” “For example, AVEC makes funds available for the payment of medical care of its members. The people who do not participate in AVEC are the most impacted and do not have access to healthcare, Mushake” “There are advantages of being a member of these associations: …if a member becomes ill, he/she can borrow money from these associations, use it to pay for basic healthcare, and pay it back to the association gradually. As a member of these associations, you can also borrow money and start a small business. Walungu” “The local associations ensure that their members benefit from good quality care by making financial contributions. Bukavu” “…most of these associations are non-profit, they are much more interested in community development, and there are not immediately focussing on issues related to health inequalities. Goma” “These local associations can help us in case of illness or any other problem, Kingoze” “In case of illness, community workers will bring the patient to the hospital where she/he will be treated first, Bahwere” |
| Land and Physical Assets | “Often young people are educated about sexuality at the youth corner. In our community, the youth club organizes football tournaments, Ihimbi” “Sport is very necessary for everyone’s health, especially young people who need these spaces to train in football and basketball. Bukavu” “Our young people need fields to practice their sports and discover their talents. However, sports fields are not always ready to be used because rivers flood in many areas. Other physical areas are used as reception centers for victims of conflict. So, physical and psychological treatment are offered in these areas but also the same areas are used by the community for income-generating activities. Walungu” “We don’t think that these places could be linked to health inequalities. We don’t think it’s related. Goma” “No links with health inequalities here. Bahwere” “They are not related to these health inequalities. Shasha” “Often these physical spaces are only involved in tourism. Kigonze” |
| Local Institutions | “We receive subsidies from these organizations, such as agricultural inputs, farming tools for field work, seeds, and sometimes food products. (Flour, cooking oil…)—Ihimbi” “…they also give us farming tools, and seeds for our fields, but also training in agro-pastoral, nutrition, health, and sanitation. Kahungu” “Temperance heals people for nothing, many go to temperance before going to the hospital. Mushake” “Schools teach children and young people that we are all equal, and we all have the right to health care. But also our children are often injured by their peers at school when we cannot afford to take them to the health center. Shasha” “People who work for local institutions are often better placed and better served in our community, compared to those who live only from agriculture. Walungu” “Local institutions take care of their workers and offer them health insurance. With this, the workers will have better access to health care. Often the people who are best taken care of in hospitals are those who have health care insurance from these institutions. Bukavu” “In our country, there is no such thing as health discrimination, even for the Lendu. Bahwere” “…neighborhood offices look after our safety while schools provide education. Unfortunately, local institutions cannot help us in addressing our health needs. Kigonze” |
| Individuals | “…are willing to help the community but as individuals, they lack the means. If they were supported by the state, they could help the community better, Bujovu” “…young people are our future, and need to be educated so that they can become nurses and doctors in the future, Bujovu” “These individuals give subsidies to families, often in the form of food products (flour, oil), Kahungu.” “Speaking of health, nurses and doctors are the most concerned, as they are the ones who experience these inequalities in hospitals and health centers. Bukavu” “Nurses and doctors are often linked to these health inequalities because they are often the ones who do not take care of the patients properly, and there is often negligence among the nursing staff. Goma” “…they help us in different situations like illness, education of children, advice, etc. Ihimbi” “…these people help us by paying either part of the bill or all of it for the most vulnerable, especially widows and orphans. Shasha” “…these people create jobs in our area. If you have a job, you will be able to feed your family and help everyone to be in good health. Walungu” “…these are just good people in our community, the chiefs protect us well and the MPs assist us. Bahwere” “Sometimes these people assist us in cases of serious illness or bereavement. Kigonze” |
| Local economy and exchange | “If we don’t have money we cannot access basic health care. So, we work every day to gain money, buy food and feed our families, buy medicines in case of illnesses, or go to the hospital if very sick, Ihimbi” “It’s what sustains us, it doesn’t just help us with accessing basic health care, but it also helps us pay for our children’s education, Kahungu” “With these activities, we have money that allows us to take care of ourselves in certain situations. Mushake” “We all know that inequalities in health are much more linked to the economy, as soon as you don’t have the money you can’t be taken care of. Shasha” “These activities allow us and our families to survive. We have no other help. Here in our area, if you don’t do one of these activities, you will starve. And we all know that good health is linked to good nutrition. Walungu” “Financial means are often at the root of health inequalities. Those with the greatest financial means are well taken care of, and those without are neglected. Bukavu” “These activities help to fight against health inequalities because when you have the money you are treated very well in hospitals, and when you don’t you are neglected and sometimes you are not even welcomed or taken care of without paying the deposit in some hospitals. Goma” “Having a market next door or shops helps us a lot with supplies because of the proximity, Kigonze” |
| Culture, history, and stories. | (-) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bwirire, D.; Crutzen, R.; Letschert, R.; Namegabe, E.N.; de Vries, N. Basic Health Service Delivery to Vulnerable Populations in Post-Conflict Eastern Congo: Asset Mapping. Healthcare 2023, 11, 2778. https://doi.org/10.3390/healthcare11202778
Bwirire D, Crutzen R, Letschert R, Namegabe EN, de Vries N. Basic Health Service Delivery to Vulnerable Populations in Post-Conflict Eastern Congo: Asset Mapping. Healthcare. 2023; 11(20):2778. https://doi.org/10.3390/healthcare11202778
Chicago/Turabian StyleBwirire, Dieudonne, Rik Crutzen, Rianne Letschert, Edmond Ntabe Namegabe, and Nanne de Vries. 2023. "Basic Health Service Delivery to Vulnerable Populations in Post-Conflict Eastern Congo: Asset Mapping" Healthcare 11, no. 20: 2778. https://doi.org/10.3390/healthcare11202778
APA StyleBwirire, D., Crutzen, R., Letschert, R., Namegabe, E. N., & de Vries, N. (2023). Basic Health Service Delivery to Vulnerable Populations in Post-Conflict Eastern Congo: Asset Mapping. Healthcare, 11(20), 2778. https://doi.org/10.3390/healthcare11202778