
Group Therapy with Peer Support Provider Participation in an Acute Psychiatric Ward: 1-Year Analysis
 ,
,
Abstract
:1. Introduction
1.1. The Group Therapy in Acute Psychiatric Setting
1.2. Peer Support Provider
1.3. Objectives of the Study
1.4. Expected Results
2. Materials and Methods
2.1. Study Design, Period, and Setting
2.2. Quantitative Analysis
2.3. Qualitative Analysis
- Analysis of the functioning mode of the therapeutic group according to Bion’s classification [6]:
- “the fight-flight group”, or oppositional group, occurs when group participants ally against the therapists identified as the cause of their conditions, consider hospitalization as a detention, show mistrust towards the therapeutic processes, and/or criticize the rules of ward;
- ”the dependency group” or psychoeducational group occurs when the group participants ask for health information (clarification on psychiatric pathologies, length of hospitalization, drugs and their side effects, criteria for compulsory medical treatment, etc.) and need to be continuously reassured and supported by therapists, showing passive and immature behavior;
- “the pairing group” or psychological confrontation group is characterized by hoping and waiting for rescue through two parties uniting to create the perfect solution for the participants’ current conditions, which they are not able to actively modify;
- “the disorganized group” in which participants, often suffering from an acute psychiatric condition, are unable to find adequate verbal communication and an effective relationship with therapists and other members, showing aggressive, conflicting, and incoherent behavior;
- “the work group”, different from other basic assumption groups, is based on good cooperation between participants on a topic, theme, or problem to be solved without the interference of strong emotions or destructive conflicts, showing the participants’ ability to cooperate and control their emotions.
- Thematic analysis related to the main narrative nuclei, using an inductive approach in 5 phases: (1) becoming familiar with the topic, (2) creation of initial codes, (3) identification of the main themes, (4) qualitative review of the main themes, (5) definition and naming of final themes. The main narrative cores were identified by thematic analysis, i.e., a systematic method for identifying, organizing, and investigating themes within a data collection by using an inductive approach [27]. We conducted the thematic analysis on the collection of data recorded by the therapists at the end of each group session.
- Overall, the thematic analysis was conducted through 5 stages by the therapists who participated in the group session:
- Step 1. Becoming familiar with the topic: we proceeded by analytically re-reading expressed themes, becoming familiar with them in order to identify the relevant ones;
- Step 2. Creation of initial codes: codes can be defined as a kind of label or concise summary of the expressed themes created by interpreting both semantic and latent contents. The initial codes created were the following: inside/outside relating to the internal or external environment of the department; mistrust in the healthcare system; stigma of mental illness; mental suffering; perception of the passage of time; disease awareness; doctor–patient relationship; meaningful interpersonal relationships; emotion regulation; search for daily recreational activities; paranoid ideas; hospitalization experience; somatizations and bodily concerns;
- Step 3. Identifying the main themes: a theme is defined as a significant central concept or idea that recurs within multiple topics. Generating main themes was an active process of re-viewing initial codes, identifying areas of similarity or overlap between them, generating subthemes, and bringing together codes that appear to have a common characteristic so that they can describe a consistent pattern within all codes;
- Step 4. Review of the main themes: themes were reviewed assessing their relationship to all other themes and their ability to synthesize the most relevant and important elements in relation to the research question;
- Step 5. Definition and naming of main narrative themes: any emerging narrative nuclei were named based on the following 5 themes: Interpersonal relationships; Healing process; Introspective experiences; Paranoid ideas; Daily life activities. In some sessions, multiple main narrative themes emerged. Therefore, we grouped multiple main narrative themes together into the three following ones: (A) Treatment programs + Interpersonal relationship; (B) Treatment programs + Introspective experience; (C) Interpersonal relationship + Introspective experience. Finally, we collected a total of 8 main narrative themes.
2.4. Psychometric Analysis for Mentalization
2.5. Statistical Analysis
- For continuous variables: mean, standard deviation;
- For categorical variables: percentages, chi2 test, and Fisher’s exact text;
- Forward and backward multiple linear regression was applied between the overall occurrence score of MBT-G-AQS quality (dependent variable) and the following selected variables as independent ones: number of subjects who attended groups, number of subjects who intervened in the group session by speaking, number of subjects who abandoned the group session before the end, type of group, and main narrative cores.
2.6. Ethical Considerations
3. Results
3.1. Quantitative Analysis
3.2. Qualitative Analysis According to Bion’s Assumption Classification
3.3. Qualitative Analysis According to the Main Narrative Themes
3.4. Psychometric Analysis by Completing the Mentalization-Based Therapy-Group-Adherence and Quality Rating Scale (MBT-G-AQS)
3.5. Multiple Linear Regression Model
4. Discussion
Limitations and Advantages of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunningham, J.; Strassberg, D.; Roback, H. Group Psychotherapy for Medical Patients. Compr. Psychiatry 1978, 19, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Daubney, M.; Bateman, A. Mentalization-Based Therapy (MBT): An Overview. Australas. Psychiatry 2015, 23, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.; Sales, C.M.D.; Alves, P.; Moita, G. The Core Techniques of Morenian Psychodrama: A Systematic Review of Literature. Front. Psychol. 2018, 9, 1263. [Google Scholar] [CrossRef] [PubMed]
- Ron, Y. Psychodrama’s Role in Alleviating Acute Distress: A Case Study of an Open Therapy Group in a Psychiatric Inpatient Ward. Front. Psychol. 2018, 9, 2075. [Google Scholar] [CrossRef] [PubMed]
- Scheidlinger, S. Freudian Group Psychology and Group Psychotherapy. Am. J. Orthopsychiatry 1952, 22, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Bion, W.R. Experiences in Groups, and Other Papers; Routledge: London, UK, 1989; ISBN 978-0-415-04020-4. [Google Scholar]
- Neri, C.; Bernabei, M.; Fadda, P.; Neri, C. Alcune Osservazioni su Gruppo di Lavoro e Assunti di Base. [Observations on Work Group and on Group with Basic Assumptions]. In Letture Bioniane, 1st ed.; Borla: Roma, Italy, 1987; pp. 297–304. [Google Scholar]
- Di Muro, R.; Sancini, M.; Aurigemma, C. Psicoterapia di Gruppo nel Servizio Psichiatrico di Diagnosi e Cura. L’Esperienza di Rimini. [Group Therapy in Service of Psychiatric Diagnosis and Care. The Experience in Rimini]. Available online: http://www.bleger.org/psicoterapia-di-gruppo-nel-servizio-psichiatrico-di-diagnosi-e-cura-esperienza-di-rimini/ (accessed on 1 July 2023).
- Yalom, I.D. The Theory and Practice of Group Psychotherapy, 3rd ed.; Basic Books: New York, NY, USA, 1985; ISBN 978-0-465-08447-0. [Google Scholar]
- Leszcz, M.; Yalom, I.D.; Norden, M. The Value of Inpatient Group Psychotherapy: Patients’ Perceptions. Int. J. Group Psychother. 1985, 35, 411–433. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Lechevallier, Z.; Buhagiar, K. A Qualitative Study of Service User Non-engagement in Psychological Therapy Groups on Acute Mental Health Wards. Couns. Psychother. Res. 2021, 21, 370–381. [Google Scholar] [CrossRef]
- Sánchez Morales, L.; Eiroa-Orosa, F.J.; Valls Llagostera, C.; González Pérez, A.; Alberich, C. From Feelings of Imprisonment to Group Cohesion: A Qualitative Analysis of Group Analytic Psychotherapy with Dual Diagnosed Patients Admitted to an Acute Inpatient Psychiatric Unit. Psychother. Res. 2018, 28, 433–445. [Google Scholar] [CrossRef]
- Yalom, I.D.; Leszcz, M. The Theory and Practice of Group Psychotherapy, 6th ed.; Basic Books: New York, NY, USA, 2020; ISBN 978-1-5416-1757-5. [Google Scholar]
- Kapur, N.; Ibrahim, S.; While, D.; Baird, A.; Rodway, C.; Hunt, I.M.; Windfuhr, K.; Moreton, A.; Shaw, J.; Appleby, L. Mental Health Service Changes, Organisational Factors, and Patient Suicide in England in 1997–2012: A before-and-after Study. Lancet Psychiatry 2016, 3, 526–534. [Google Scholar] [CrossRef]
- Rutan, J.S. Reasons for Suggesting Group Psychotherapy to Patients. Am. J. Psychother. 2021, 74, 67–70. [Google Scholar] [CrossRef]
- Emond, S.; Rasmussen, B. The Status of Psychiatric Inpatient Group Therapy: Past, Present, and Future. Soc. Work Groups 2012, 35, 68–91. [Google Scholar] [CrossRef]
- Ngooi, B.X.; Wong, S.R.; Chen, J.D.; Yin Koh, V.S. Exploring the Use of Activity-Based Group Therapy in Increasing Self-Efficacy and Subjective Well-Being in Acute Mental Health. Hong Kong J. Occup. Ther. 2022, 35, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Clough, B.; Spriggens, L.; Stainer, M.; Casey, L. Working Together: An Investigation of the Impact of Working Alliance and Cohesion on Group Psychotherapy Attendance. Psychol. Psychother. Theory Res. Pract. 2022, 95, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Hajek, K. Interpersonal Group Therapy on Acute Inpatient Wards. Groupwork 2007, 17, 7–19. [Google Scholar] [CrossRef]
- Kösters, M.; Burlingame, G.M.; Nachtigall, C.; Strauss, B. A Meta-Analytic Review of the Effectiveness of Inpatient Group Psychotherapy. Group Dyn. Theory Res. Pract. 2006, 10, 146–163. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Handbook of Mentalizing in Mental Health Practice, 2nd ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2019; ISBN 978-1-61537-140-2. [Google Scholar]
- Fonagy, P.; Allison, E. The Role of Mentalizing and Epistemic Trust in the Therapeutic Relationship. Psychotherapy 2014, 51, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Karterud, S. Mentalization-Based Group Therapy (MBT-G): A Theoretical, Clinical, and Research Manual; Oxford University Press: Oxford, UK, 2015; ISBN 978-0-19-875374-2. [Google Scholar]
- Karterud, S.; Pedersen, G.; Engen, M.; Johansen, M.S.; Johansson, P.N.; Schlüter, C.; Urnes, Ø.; Wilberg, T.; Bateman, A.W. The MBT Adherence and Competence Scale (MBT-ACS): Development, Structure and Reliability. Psychother. Res. 2013, 23, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Mutschler, C.; Bellamy, C.; Davidson, L.; Lichtenstein, S.; Kidd, S. Implementation of Peer Support in Mental Health Services: A Systematic Review of the Literature. Psychol. Serv. 2022, 19, 360–374. [Google Scholar] [CrossRef]
- Carugati, C.M. Gli Esperti Supporto Tra Pari: Dall’ Esperienza Personale ad Una Futura Professione. [The Experts Peer Support: From Personal Experience to a Future Profession]. Available online: https://www.centropsicologiamonza.it/psicoterapia/gli-esperti-supporto-tra-pari/ (accessed on 1 July 2023).
- Folmo, E.J.; Karterud, S.W.; Bremer, K.; Walther, K.L.; Kvarstein, E.H.; Pedersen, G.A.F. The Design of the MBT-G Adherence and Quality Scale. Scand. J. Psychol. 2017, 58, 341–349. [Google Scholar] [CrossRef]
- Di Lorenzo, R.; Montardi, G.; Panza, L.; Del Giovane, C.; Saraceni, S.; Rovesti, S.; Ferri, P. Retrospective Analysis of Factors Associated with Long-Stay Hospitalizations in an Acute Psychiatric Ward. Risk Manag. Healthc. Policy 2020, 13, 433–442. [Google Scholar] [CrossRef]
- Bello, F.; Mei, A. Gruppo e Dimensioni Gruppali in un Servizio Psichiatrico di Diagnosi e Cura. [Group Therapy and Dynamics in One Service of Psychiatric Diagnosis and Care]. Available online: https://www.funzionegamma.it/wp-content/uploads/2022/11/dimensioni-gruppali.pdf (accessed on 1 July 2023).
- Ferrari, P. Chi è e Come si Diventa Esperto in Supporto fra Pari. [Who is Peer Support Expert and How to Become a Peer Support Expert]. Available online: https://180gradi.org/salute-mentale/180gradi/lesp-esperto-in-supporto-fra-pari (accessed on 1 July 2023).
- Di Lorenzo, R.; Paguni, R. Modalita di Espressione e di Funzionamento del Gruppo Terapeutico in un Presidio Psichiatrico di Diagnosi E Cura. [Different Expression and Functioning of a Psychotherapic Group in a Psychiatric Ward for Acute Patients]. Psichiatr. Psicoter. 2005, 24, 216–230. [Google Scholar]
- Bernard, H.; Burlingame, G.; Flores, P.; Greene, L.; Joyce, A.; Kobos, J.C.; Leszcz, M.; MacNair-Semands, R.R.; Piper, W.E.; McEneaney, A.M.S.; et al. Clinical Practice Guidelines for Group Psychotherapy. Int. J. Group Psychother. 2008, 58, 455–542. [Google Scholar] [CrossRef]
- Landi, G.; Simoni, E.; Landi, I.; Galeazzi, G.M.; Moscara, M.; Pighi, M.; Ferri, P.; Di Lorenzo, R. Therapeutic Factors in a Psychiatric Group Therapy: A Preliminary Validation of Therapeutic Factors Inventory-8, Italian Version. Psychiatr. Q. 2021, 92, 523–536. [Google Scholar] [CrossRef]


{kind=link}
| Variables | M ± SD |
|---|---|
| Age (years) | 39.2 ± 3.8 |
| N° women | 6.0 ± 2.0 |
| N° men | 7.3 ± 2.0 |
| N° subjects involuntary hospitalized | 3.9 ± 1.4 |
| Schizophrenia spectrum disorders | 6.7 ± 1.8 |
| Bipolar disorders | 2.4 ± 1.2 |
| Personality disorders | 1.9 ± 1.6 |
| Intellective disability | 0.6 ± 0.6 |
| Organic psychotic conditions | 0.2 ± 0.5 |
| Dysthymia and depressive disorders | 0.4 ± 0.6 |
| Anorexia | 0.3 ± 0.6 |
| Others | 0.8 ± 0.8 |
| Duration of hospitalization (days) | 11.2 ± 2.1 |
| Type of Group n (%) | Subjects Hospitalized at the Time of Group Sessions (M ± SD) | Subjects Who Attended Group Sessions (M ± SD) | Subjects Who Intervened in the Group Sessions by Speaking (M ± SD) | Subjects Who Abandoned the Group Session before the End (M ± SD) |
|---|---|---|---|---|
| Fight and flight 5 (13%) | 13.8 ± 3.1 | 8.2 ± 2.7 | 5.2 ± 1.9 | 1.2 ± 2.7 |
| Dependency 3 (8%) | 13.7 ± 0.5 | 7.7 ± 0.5 | 5 ± 1.6 | 0 |
| Pairing 3 (8%) | 14.3 ± 1.2 | 6.7 ± 2.9 | 4.3 ± 2.3 | 0.7 ± 0.6 |
| Disorganized 5 (13%) | 12.2 ± 2.2 | 7.6 ± 2.3 | 5 ± 2.3 | 0 |
| Working 24 (60%) | 13.3 ± 1.7 | 7.2 ± 2.1 | 6 ± 1.3 | 0.4 ± 0.7 |
| Total 40 (100%) | 13.4 ± 1.9 | 7.4 ± 2.1 | 5.6 ± 1.6 | 0.4 ± 1.0 |
| N° Group | Initial Narrative Themes | Codes | Main Narrative Themes |
|---|---|---|---|
| 1 | Inside/outside the ward Ambivalence toward safe places | Inside/outside | Healing process |
| 2 | Projection into the future: fear of discharge Projection into the past: not processing the past | Inside/outside Time | Healing process Introspective experiences |
| 3 | Communication Somatization | Healing process Psychic suffering | Healing process Introspective experiences |
| 4 | Anger both as what led to hospitalization and as experienced during the stay in the ward and which can characterize coexistence with others | Emotion regulation | Introspective experiences |
| 5 | “Feeling that I have suffered an injustice”, “we acted as guinea pigs”, “I was tied up”, “little trust in the doctor” | Distrust in the healing system | Paranoid ideas |
| 6 | Fear and psychic suffering “How others see us, how others feel our suffering that we think only we have” | Stigma Psychic suffering | Interpersonal relationships Introspective experiences |
| 7 | Time lived/time perceived | Time | Introspective experiences |
| 8 | Why and how the crisis comes: “it’s so fast that we can’t understand” | Disease awareness | Healing process |
| 9 | Difficulty in accepting the diagnosis | Disease awareness | Healing process |
| 10 | Anxiety about the outside world and a need to research a safe place | Inside/outside | Healing process |
| 11 | Life “outside the ward” | Inside/outside | Healing process |
| 12 | Stigma related to mental illness | Stigma | Interpersonal relationships |
| 13 | Boundary and vulnerability, strong mirroring among all group participants | Inside/outside Disease awareness | Healing process |
| 14 | Illness onset also understood as something yet to be “disposed of”, mentalization | Disease awareness | Healing process |
| 15 | Report of help from the group, need for support from others | Interpersonal relationships | Interpersonal relationships |
| 16 | Hospitalization | Healing process | Healing process |
| 17 | It was hard to keep a main theme | / | No main theme |
| 18 | Violence | Violence | Interpersonal relationships |
| 19 | Hospitalization | Healing process | Healing process |
| 20 | Understanding the reasons for hospitalization Attributing meaning to hospitalization through relationships with others | Disease awareness Interpersonal relationships | Healing process Interpersonal relationships |
| 21 | Length and utility of hospitalization | Healing process | Healing process |
| 22 | Healing process | Healing process | Healing process |
| 23 | Hospitalization experience | Healing process | Healing process |
| 24 | Wishes and expectations with respect to the Christmas holidays. Correct lifestyles (nutrition and physical activity) | Psychoeducation | Daily life activities |
| 25 | Internal and external persecutors | Paranoid ideas | Paranoid ideas |
| 26 | “Theory of the scapegoat”: patients—do they reinforce each other in a paranoid sense. Only one patient criticizes her aggressive behavior saying she lost control (“because provoked”) | Paranoid ideas | Paranoid ideas |
| 27 | Difficulty in finding a job (“the job that can’t be found”) | Stigma | Interpersonal relationships |
| 28 | Relationship with the outside The judgment of others Disease awareness | Inside/outside Stigma Disease awareness | Healing process Interpersonal relationships |
| 29 | Resignification of the “hospitalization” moment | Healing process | Healing process |
| 30 | Subjectivity of psychiatric disorder, patient’s point of view and doctor’s point of view | Disease awareness | Healing process |
| 31 | Moods | Emotion regulation | Introspective experiences |
| 32 | Ward criticalities | Healing process | Healing process |
| 33 | Physical activity and its benefits | Psychoeducation | Daily life |
| 34 | Hospitalization utility | Healing process | Healing process |
| 35 | Managing your own mental health | Disease awareness | Healing process |
| 36 | Importance of a good psychiatric team | Healing process/patient–doctor relationship | Healing process |
| 37 | Cause of discomfort leading to hospitalization Trust in the possibility of being able to recover and that there may be a way out | Disease awareness | Healing process |
| 38 | Isolation and trust | Stigma Path of care/ doctor–patient relationship | Healing process Interpersonal relationships |
| 39 | Life experiences with considerable suffering | Psychic suffering | Introspective experiences |
| 40 | Tension and tension management strategies | Disease awareness Psychic suffering | Healing process |
| Main Narrative Cores * | Types of Groups According to Bion’s Classification * | Total | ||||
|---|---|---|---|---|---|---|
| Fight and Flight | Dependency | Pairing | Disorganized | Working | ||
| Treatment programs | 0 | 1 | 1 | 1 | 16 | 19 |
| Paranoid ideas | 2 | 0 | 0 | 0 | 1 | 3 |
| Interpersonal relationships | 1 | 0 | 2 | 0 | 1 | 4 |
| Introspective experiences | 0 | 1 | 0 | 1 | 2 | 4 |
| Daily activities | 0 | 0 | 0 | 1 | 1 | 2 |
| (A) Treatment programs + Interpersonal relationship | 0 | 0 | 0 | 1 | 2 | 3 |
| (B) Treatment programs + Introspective experience | 1 | 1 | 0 | 0 | 1 | 3 |
| (C) Interpersonal relationship + Introspective experience | 1 | 0 | 0 | 0 | 0 | 1 |
| No narrative core identified | 0 | 0 | 0 | 1 | 0 | 1 |
| Total | 5 | 3 | 3 | 5 | 24 | 40 |
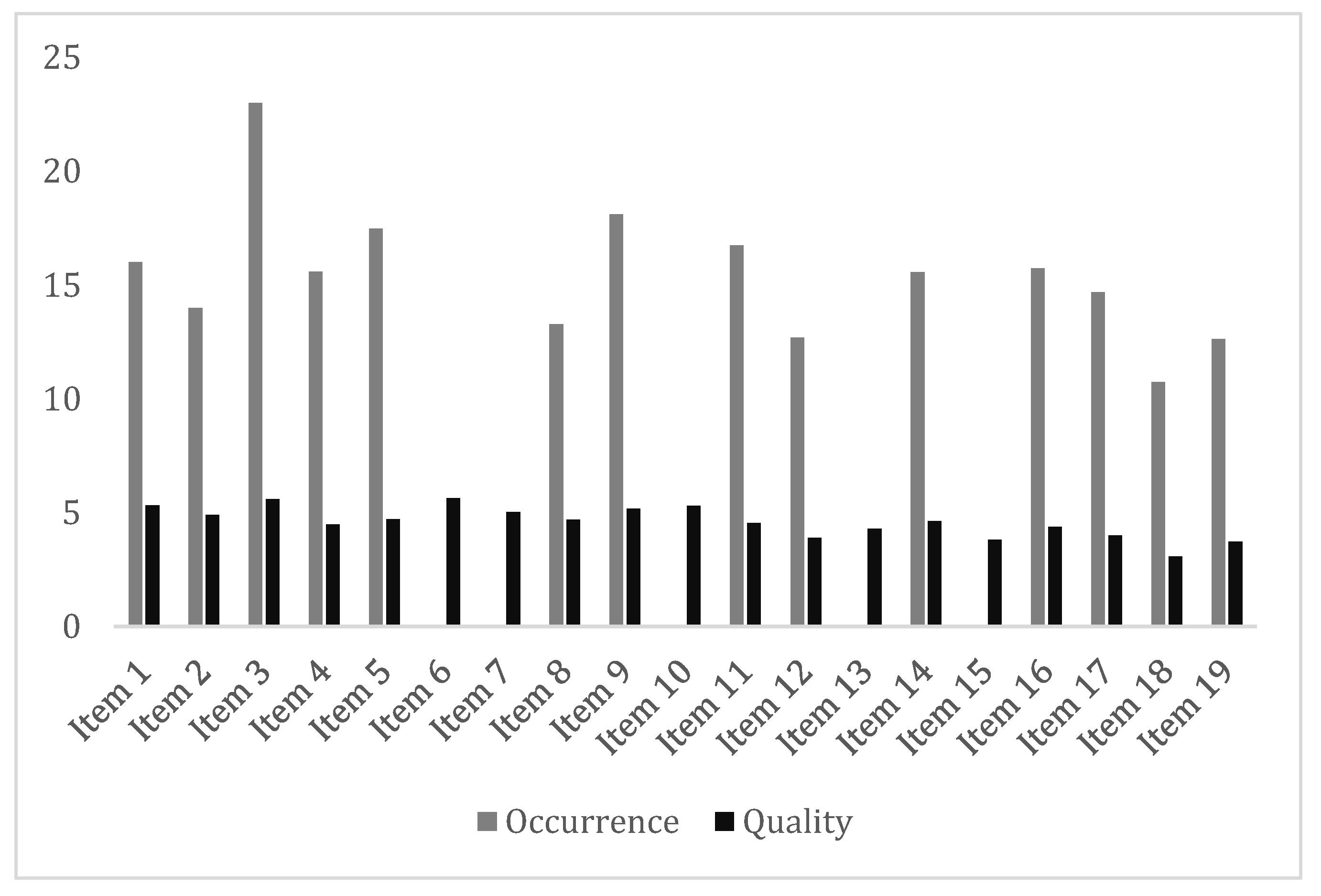
| N. | Item | Occurrence (Range 0–30) M ± SD | Quality (Range 0–7) M ± SD |
|---|---|---|---|
| 1 | Managing group boundaries | 16.03 ± 8.19 | 5.33 ± 1.38 |
| 2 | Regulating group phasing | 14 ± 7.89 | 4.9 ± 1.41 |
| 3 | Initiating and fulfilling turn taking | 23 ± 6.58 | 5.6 ± 1.17 |
| 4 | Engaging group members in mentalizing external events | 15.6 ± 7.93 | 4.48 ± 1.80 |
| 5 | Identifying and mentalizing events in the group | 17.5 ± 7.28 | 4.73 ± 1.40 |
| 6 | Caring for the group and each member | / | 5.65 ± 1.37 |
| 7 | Managing authority | / | 5.03 ± 1.95 |
| 8 | Stimulating discussions about group norms | 13.3 ± 8.25 | 4.69 ± 1.79 |
| 9 | Cooperation between co-therapists | 18.13 ± 7.90 | 5.18 ± 1.48 |
| 10 | Engagement, interest, and warmth | / | 5.3 ± 1.54 |
| 11 | Exploration, curiosity, and not-knowing stance | 16.75 ± 8.29 | 4.55 ± 1.78 |
| 12 | Challenging unwarranted beliefs | 12.7 ± 7.62 | 3.9 ± 1.93 |
| 13 | Regulation of emotional arousal | / | 4.3 ± 1.77 |
| 14 | Acknowledgment of good mentalization | 15.58 ± 7.31 | 4.63 ± 1.58 |
| 15 | Handling pretend mood | / | 3.82 ± 2.02 |
| 16 | Handling psychic equivalence | 15.75 ± 6.76 | 4.38 ± 1.53 |
| 17 | Focus on emotions | 14.7 ± 8.55 | 4 ± 1.89 |
| 18 | Stop and rewind | 10.75 ± 8.59 | 3.08 ± 2.05 |
| 19 | Focus on the relationship between therapists and patients | 12.63 ± 8.84 | 3.74 ± 1.86 |
| Total | 15.46 ± 4.65 | 4.60 ± 0.91 | |
| Variables | Coef. | Conf. Int. 95% | Probability |
|---|---|---|---|
| MBT-G-AQS Overall Occurrence Score | |||
| Subjects who attended groups | 14.87 | 3.57; 26.18 | p = 0.011 |
| Subjects who intervened in the group session by speaking | −16.87 | −31.52; 2.23 | p = 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Lorenzo, R.; D’Amore, J.; Amoretti, S.; Bonisoli, J.; Gualtieri, F.; Ragazzini, I.; Rovesti, S.; Ferri, P. Group Therapy with Peer Support Provider Participation in an Acute Psychiatric Ward: 1-Year Analysis. Healthcare 2023, 11, 2772. https://doi.org/10.3390/healthcare11202772
Di Lorenzo R, D’Amore J, Amoretti S, Bonisoli J, Gualtieri F, Ragazzini I, Rovesti S, Ferri P. Group Therapy with Peer Support Provider Participation in an Acute Psychiatric Ward: 1-Year Analysis. Healthcare. 2023; 11(20):2772. https://doi.org/10.3390/healthcare11202772
Chicago/Turabian StyleDi Lorenzo, Rosaria, Jessica D’Amore, Sara Amoretti, Jessica Bonisoli, Federica Gualtieri, Ilaria Ragazzini, Sergio Rovesti, and Paola Ferri. 2023. "Group Therapy with Peer Support Provider Participation in an Acute Psychiatric Ward: 1-Year Analysis" Healthcare 11, no. 20: 2772. https://doi.org/10.3390/healthcare11202772
APA StyleDi Lorenzo, R., D’Amore, J., Amoretti, S., Bonisoli, J., Gualtieri, F., Ragazzini, I., Rovesti, S., & Ferri, P. (2023). Group Therapy with Peer Support Provider Participation in an Acute Psychiatric Ward: 1-Year Analysis. Healthcare, 11(20), 2772. https://doi.org/10.3390/healthcare11202772