
Effects of Infection Control Education Program Using Flipped Learning Based on the ARCS Model for Nursing Students: A Mixed Method


Abstract
:1. Introduction
2. Methods
2.1. Study Design
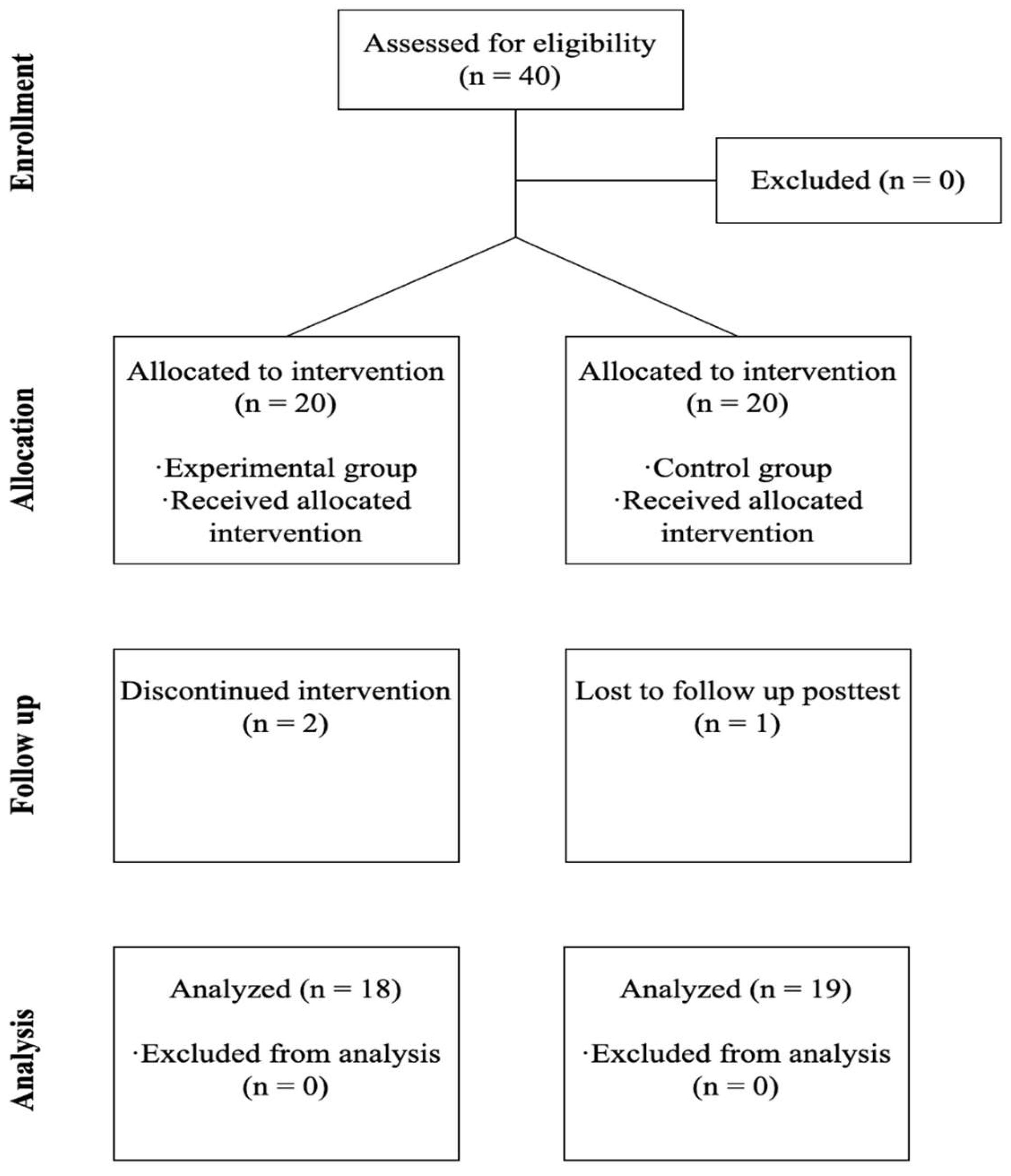
2.2. Participants
2.3. Process of This Study
2.4. Quantitative Study Progress
2.4.1. Interventions
Pre-Class
In-Class
Post-Class
2.4.2. Experimental Group and Control Group
2.4.3. Measurements
Learning Motivation
Self-Directed Learning Ability
Academic Self-Efficacy
Knowledge and Confidence in Infection Control Practice
Anxiety
2.5. Qualitative Study Progress
2.6. Data Analysis
2.6.1. Quantitative Analysis
2.6.2. Qualitative Analysis
2.7. Ethical Consideration
3. Results
3.1. Quantitative Results
3.1.1. Homogeneity Test of General Characteristics and Variables in Pretest
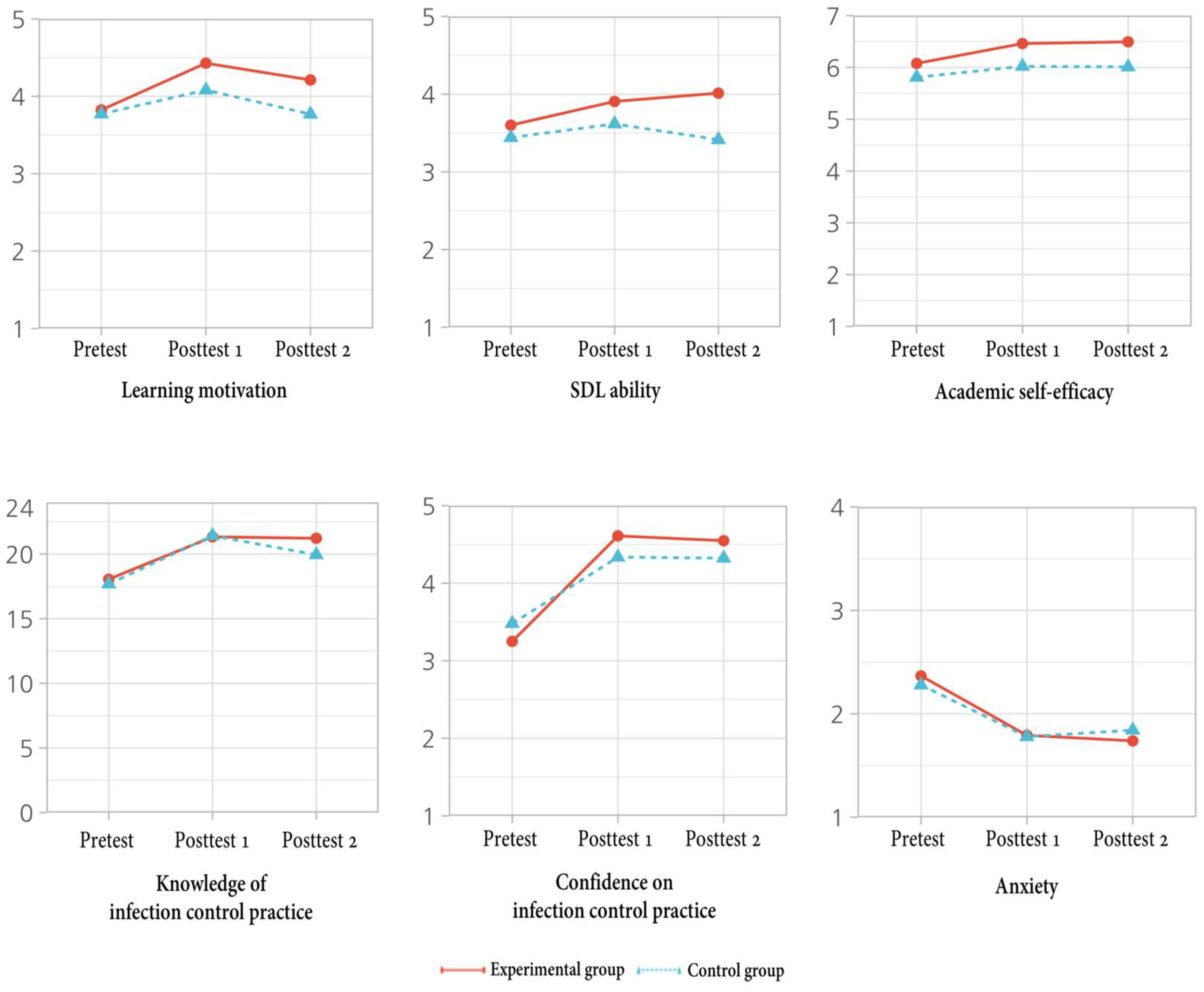
3.1.2. Effects of the Infection Control Education Program Using Flipped Learning Based on the ARCS Model
3.2. Qualitative Results
3.2.1. Theme 1: Studying with Learning Motivation
“In the pre-class,I got really curious with the introduction of gaps, so I ended up diving deep into the material.”(Participant 4)
“The instructor presented real cases and examples aiding my understanding and attention. Learning about infection control through videos and images made it easier to grasp.”(Participant 7)
“Having prepared before class, I actively participated and developed the confidence to engage.”(Participant 3)
3.2.2. Theme 2: Self-Directed Learning
“Setting my own learning goals was a memorable experience. This self-set target motivated me to work harder. And post-class reflection enabled me to identify areas where I lacked and prompted me to address those gaps.”(Participant 6)
“Filling out a reflection helped me evaluate my progress rather than merely completing the class. I focused on improving my weak points.”(Participant 8)
“I went over what I learned and asked questions while studying on my own, trying to find more ways to get better.”(Participant 4)
3.2.3. Theme 3: Interesting Learning Infection Control
“I really got the idea of infection control from the interesting class.”(Participant 1)
“Understanding why we need infection control and how it’s done was really helpful. The class was enjoyable, and that really helped comprehend the concept of infection control.”(Participant 3)
3.2.4. Theme 4: ‘Difficulty in New Ways of Learning’
“Even though it seemed easy to just watch those videos before class, it actually required more time, which kind of made it a bit harder. And also, some difficulties during team activity when the pre-class didn’t do actively.”(Participant 2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Report on Infection Prevention and Control. 2022. Available online: https://iris.who.int/bitstream/handle/10665/330080/9789241516945-eng.pdf?sequence=1&isAllowed=y (accessed on 27 September 2023).
- Ahmed, S.; Hassan, M.M.; Khan, F.; Sultan, A.; Shah, M.S. The Mpox Disease: Awareness and Apprehensions among the Medical Undergraduates and Nursing Staff. J. Pure. Appl. Microbiol. 2022, 6, 3155–3167. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.; Burnett, E. Hand hygiene knowledge and attitudes: Comparisons between student nurses. J. Infect. Control 2011, 12, 246–250. [Google Scholar] [CrossRef]
- Parreira, P.; Santos-Costa, P.; Pardal, J.; Neves, T.; Bernardes, R.A.; Serambeque, B.; Sousa, L.B.; Myllymäki, M.; Macho, A.I.; Mayens, A.L.W. Nursing Students’ perceptions on healthcare-associated infection control and prevention teaching and learning experience in Portugal. J. Pers. Med. 2022, 12, 180. [Google Scholar] [CrossRef]
- Kim, E.; Kim, S.S.; Kim, S. Effects of infection control education for nursing students using standardized patients vs. peer role-play. Int. J. Environ. Res. Public Health 2021, 18, 107. [Google Scholar] [CrossRef]
- Calik, A.; Cakmak, B.; Kapucu, S.; Inkaya, B. The effectiveness of serious games designed for infection prevention and promotion of safe behaviors of senior nursing students during the COVID-19 pandemic. Am. J. Infect. Control 2022, 50, 1360–1367. [Google Scholar] [CrossRef]
- Bouchoucha, S.L.; Phillips, N.M.; Lucas, J.; Kilpatrick, M.; Hutchinson, A. An investigation into nursing students’ application of infection prevention and control precautions. Nurse Educ. Today 2021, 104, 104987. [Google Scholar] [CrossRef]
- Grow, G. Teaching learners to be self-directed. Adult Educ. Q. 1991, 41, 125–149. [Google Scholar] [CrossRef]
- Wong, F.M.F.; Tang, A.C.Y.; Cheng, W.L.S. Factors associated with self-directed learning among undergraduate nursing students: A systematic review. Nurse Educ. Today 2021, 104, 104998. [Google Scholar] [CrossRef]
- Bergmann, J.; Sams, A. Flip Your Classroom: Reach Every Student in Every Class Every Day; International Society for Technology in Education: Washington, DC, USA, 2012. [Google Scholar]
- Lee, D.Y. Research on developing instructional design models for flipped learning. J. Digit. Converg. 2013, 11, 83–92. [Google Scholar] [CrossRef]
- Fuchs, K. Innovative teaching: A qualitative review of flipped classrooms. Int. J. Learn. Teach. Educ. Res. 2021, 20, 18–32. [Google Scholar] [CrossRef]
- Berdida, D.J.E. Resilience and academic motivation’s mediation effects in nursing students’ academic stress and self-directed learning: A multicenter cross-sectional study. Nurse Educ. Pract. 2023, 69, 103639. [Google Scholar] [CrossRef] [PubMed]
- Pintrich, P.R. A motivational science perspective on the role of student motivation in learning and teaching contexts. J. Educ. Psychol. 2003, 95, 667–686. [Google Scholar] [CrossRef]
- Li, K.; Keller, J.M. Use of the ARCS model in education: A literature review. Comput. Edu. 2018, 122, 54–63. [Google Scholar] [CrossRef]
- Keller, J.M. Motivational design research and development. In Motivational Design for Learning and Performance; Springer: Boston, MA, USA, 2010. [Google Scholar] [CrossRef]
- Goksu, I.; Islam Bolat, Y. Does the ARCS motivational model affect students’ achievement and motivation? A meta-analysis. Rev. Educ. 2021, 9, 27–52. [Google Scholar] [CrossRef]
- Chang, T.S.; Teng, Y.K.; Chien, S.Y.; Tzeng, Y.L. Use of an interactive multimedia e-book to improve nursing students’ sexual harassment prevention knowledge, prevention strategies, coping behavior, and learning motivation: A randomized controlled study. Nurse Educ. Today 2021, 105, 104883. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Li, Z.; Zhang, J.; Peng, M.; Yang, S.; Tian, X.; Yang, S.; Yan, F. Effects of ARCS model-based motivational teaching strategies in community nursing: A mixed-methods intervention study. Nurse Educ. Today 2022, 119, 105583. [Google Scholar] [CrossRef]
- Turel, Y.K.; Sanal, S.O. The effects of an ARCS based e-book on student’s achievement, motivation and anxiety. Comput. Educ. 2018, 127, 130–140. [Google Scholar] [CrossRef]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Salmon, S.; Wang, X.B.; Seetoh, T.; Lee, S.Y.; Fisher, D.A. A novel approach to improve hand hygiene compliance of student nurses. Antimicrob. Resist. Infect. Control 2013, 2, 16. [Google Scholar] [CrossRef]
- Tawalbeh, L.I.; Al-Rawajfah, O.M.; Habiballah, L. The effect of infection control course on nursing students’ knowledge of and compliance with universal precautions: A quasi-experimental study. Dimens. Crit. Care. Nurs. 2019, 38, 137–145. [Google Scholar] [CrossRef]
- Kim, H.; Kim, E.K. A systematic review of infection management education program for nursing students. J. Korean Assn. Learn. Cent. Curric. 2020, 20, 1359–1375. [Google Scholar] [CrossRef]
- Park, H.; Kim, Y. Infection control education programs for nursing students: A systematic review. J. Korean Acad. Fundam. Nurs. 2021, 28, 237–248. [Google Scholar] [CrossRef]
- The Korean Society of Infectious Diseases. Standard Prevention Guidelines for Health-Associated Infection. 2017. Available online: https://www.ksid.or.kr/board/list.html?num=2758&start=0&sort=top%20desc,thread%20desc,pos&code=pds&key=&keyword= (accessed on 1 April 2022).
- Zainuddin, Z.; Haruna, H.; Li, X.; Zhang, Y.; Chu, S.K.W. A systematic review of flipped classroom empirical evidence from different fields: What are the gaps and future trends? Horizon 2019, 27, 72–86. [Google Scholar] [CrossRef]
- Lee, M.H.; Park, M.S. The effect of case-based learning based on flipped learning for nursing students. J. Korean Acad. Soc. Nurs. Educ. 2021, 27, 107–116. [Google Scholar] [CrossRef]
- Hwang, S.Y. Effects of Problem-Based Learning on the Knowledge Achievement, Critical Thinking Ability, Attitude and Motivation toward Learning of Nursing Students. Ph.D. Thesis, Chonnam National University, Gwangju, Republic of Korea, 2003. [Google Scholar]
- Keller, J.M.; Song, S.H. Engaging Instructional Design; Kyoyookbook: Gyeonggi, Republic of Korea, 1999. [Google Scholar]
- Yoo, K. Analysis relationships and effects of pre-service early childhood teacher’s motivations of choosing a teaching profession related to educational belief and self-directed learning readiness. Korean J. Community Living Sci. 2017, 28, 115–130. [Google Scholar] [CrossRef]
- West, R.; Bentley, E.L. Relationship between Scores on the Self-Directed Learning Readiness Scale, ODDI Continuing Learning Inventory and Participation in Continuing Professional Education; Oklahoma Research Center for Continuing Professional and Higher Education, University of Oklahoma: Norman, OK, USA, 1991. [Google Scholar]
- Park, S.Y.; Kweon, Y.R. The effect of using standardized patients in psychiatric nursing practical training for nursing college student. J Korean Acad. Psychiatr. Ment. Health Nurs. 2012, 21, 79–88. [Google Scholar] [CrossRef]
- Ayres, H.W. Factors Related to Motivation to Learn and Motivation to Transfer Learning in a Nursing Population. Ph.D. Thesis, North Carolina State University, Raleigh, NC, USA, 2005. [Google Scholar]
- Korean Hospital Nurses Association. Guideline for Isolation Precautions in Healthcare Settings. 2017. Available online: https://khna.or.kr/home/data/khna_guide_ebp08.pdf (accessed on 10 April 2022).
- Spielberger, C.D. Anxiety: State-trait process. In Stress and Anxiety; Speilberger, C.D., Sarason, I.G., Eds.; Hemisphere: Washington, DC, USA, 1975. [Google Scholar]
- Kim, J.T.; Shin, D.K. A study based on the standardization of the STAI for Korea. New Med. J. 1978, 21, 69–75. [Google Scholar]
- Schwandt, T.A.; Lincoln, Y.S.; Guba, E.G. Judging interpretations: But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir. Eval. 2007, 114, 11–25. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Ongor, M.; Uslusoy, E.C. The effect of multimedia-based education in e-learning on nursing students’ academic success and motivation: A randomised controlled study. Nurse Educ. Pract. 2023, 71, 103686. [Google Scholar] [CrossRef]
- Zhang, D.; Zhang, J.; Cao, M.; Zhu, Y.; Yang, G. Testing the effectiveness of motivation-based teaching in Nursing English course: A quasi-experimental study. Nurse Educ. Today 2023, 122, 105723. [Google Scholar] [CrossRef] [PubMed]
- Khodaei, S.; Hasanvand, S.; Gholami, M.; Mokhayeri, Y.; Amini, M. The effect of the online flipped classroom on self-directed learning readiness and metacognitive awareness in nursing students during the COVID-19 pandemic. BMC Nurs. 2022, 21, 22. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Suh, E.E. The effects of an interactive nursing skills mobile application on nursing students’ knowledge, self-efficacy, and skills performance: A randomized controlled trial. Asian Nurs. Res. 2018, 12, 17–25. [Google Scholar] [CrossRef]
- Bandura, A. The assessment and predictive generality of self-percepts of efficacy. J. Behav. Ther. Exp. Psychiatry 1982, 13, 95–199. [Google Scholar] [CrossRef]
- Cho, M.-K.; Kim, M.Y. Factors associated with student satisfaction and self-confidence in simulation learning among nursing students in Korea. Healthcare 2023, 11, 1060. [Google Scholar] [CrossRef]
- Yang, S.Y.; Oh, Y.H. The effects of neonatal resuscitation gamification program using immersive virtual reality: A quasi-experimental study. Nurse Educ. Today 2022, 117, 105464. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Learning Subject | Flipped Learning | ARCS Strategies |
|---|---|---|
| Week 1 Health-associated infection diseases Weeks 2 Standard precautions and transmission-based precautions Weeks 3 Case study of infection control | Pre-class Watching a series of pre-recorded videos for learning subjects (15–20 min per video). Self-directed and asynchronous learning Setting learning objectives Summarizing pre-videos in notes Researching related cases or literature and summarizing Formulating questions Completing quizzes In-class Discussing questions and feedback Doing team activities Searching guidelines Making posters related to standard precautions and transmission-based precautions Case studies of various scenarios Presenting findings from team activity Mini lecture to recall Completing multiple-choice quizzes Post class Formulating the reflective journal Sharing their reflective journal Assessing their achievement of set learning objectives Receiving feedback from instructor | Attention Use multimedia materials such as voice, text, picture, and video for learning contents Provide related videos for motivation at every session, curiosity through pre-quiz Provide paper for summarizing, Make learners complete pre-quiz and create questions for an effective pre-class Empower learners to establish their own learning objectives. Diversify teaching methods, including video-based and written materials for instruction Relevance Emphasize that infection control is a fundamental and essential practice in clinical settings Explain the benefits of infection control Communicate that learners can actively engage in infection control practice and contribute to infection prevention Providing contents consistent with learning goals while showing cases of infection control in clinical practice Provide activity tasks based on the knowledge, experience, and information known to learners Explain concepts using precise terminology, accompanied by illustrative visuals and videos Confidence Foster learner expectations for the learning process by providing guidance on content and tasks Present challenges and opportunities for success through quizzes and team activities in each class Enable learners to choose their tasks, promoting a sense of autonomy Structure learning content by linking it to clinical practice experiences Satisfaction Provide positive feedback on learners’ learning efforts Evaluate the learning achievement through self-reflection and self-assessment |
| Variables | Categories | Exp. (n = 18) | Cont. (n = 19) | χ2 or t | p |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age (years) | 23.22 ± 2.60 | 25.37 ± 7.36 | −1.19 | 0.244 | |
| Sex | Male | 1 (5.6) | 2 (10.5) | - | 0.100 † |
| Female | 17 (94.4) | 17 (89.5) | |||
| Period of clinical practice (weeks) | 6.00 ± 0.00 | 5.89 ± 0.32 | 1.46 | 0.163 | |
| Major satisfaction | Unsatisfied | 0 (0.0) | 1 (5.2) | 1.08 | 0.100 † |
| Moderate | 5 (27.8) | 6 (31.6) | |||
| Satisfied | 13 (72.2) | 12 (63.2) | |||
| College life satisfaction | Unsatisfied | 0 (0.0) | 0 (0.0) | - | 0.062 † |
| Moderate | 2 (11.1) | 8 (42.1) | |||
| Satisfied | 16 (88.9) | 11 (57.9) | |||
| Clinical practice satisfaction | Unsatisfied | 0 (0.0) | 0 (0.0) | - | 0.151 † |
| Moderate | 3 (16.7) | 8 (42.1) | |||
| Satisfied | 15 (83.3) | 11 (57.9) | |||
| Experience of exposure to infection diseases | Yes | 3 (16.7) | 4 (21.1) | - | 0.100 † |
| No | 15 (83.3) | 15 (78.9) | |||
| Experience of COVID-19 | Yes | 14 (77.8) | 13 (68.4) | - | 0.714 † |
| No | 4 (22.2) | 6 (31.6) | |||
| Mean ± SD | t | p | |||
| Learning motivation | 3.83 ± 0.27 | 3.78 ± 0.33 | 0.46 | 0.651 | |
| SDL ability | 3.60 ± 0.33 | 3.44 ± 0.29 | 1.55 | 0.13 | |
| Academic self-efficacy | 6.08 ± 0.76 | 5.81 ± 0.23 | 1.43 | 0.167 | |
| Knowledge of infection control practice | 18.06 ± 2.58 | 17.68 ± 2.83 | 0.42 | 0.68 | |
| Confidence in infection control practice | 3.25 ± 0.46 | 3.48 ± 0.37 | −1.67 | 0.103 | |
| Anxiety | 2.37 ± 0.15 | 2.28 ± 0.24 | 1.34 | 0.189 | |
| Variables | Source | Estimate | SE | t | p | 95% CI | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Learning motivation | Intercept | 3.89 | 0.14 | 28.05 | <0.001 | 3.61 | 4.16 |
| Group | −0.12 | 0.2 | −0.58 | 0.56 | −0.51 | 0.28 | |
| Time | −0.01 | 0.06 | −0.01 | 0.923 | −0.13 | 0.11 | |
| Group × Time | 0.2 | 0.08 | 2.29 | 0.025 | 0.03 | 0.37 | |
| SDL ability | Intercept | 3.52 | 0.13 | 27.22 | <0.001 | 3.26 | 3.77 |
| Group | −0.09 | 0.19 | −0.50 | 0.622 | −0.46 | 0.28 | |
| Time | −0.01 | 0.06 | −0.23 | 0.818 | −0.13 | 0.1 | |
| Group × Time | 0.22 | 0.08 | 2.69 | 0.009 | 0.06 | 0.38 | |
| Academic self-efficacy | Intercept | 5.75 | 0.16 | 36.59 | <0.001 | 5.44 | 6.06 |
| Group | 0.18 | 0.23 | 0.8 | 0.425 | −0.27 | 0.63 | |
| Time | 0.1 | 0.07 | 1.46 | 0.148 | −0.04 | 0.24 | |
| Group × Time | 0.11 | 0.1 | 1.11 | 0.272 | −0.09 | 0.3 | |
| Knowledge of infection control practice | Intercept | 17.42 | 0.93 | 18.75 | <0.001 | 15.58 | 19.26 |
| Group | −0.38 | 1.33 | −0.29 | 0.774 | −3.03 | 2.26 | |
| Time | 1.13 | 0.42 | 2.67 | 0.009 | 0.29 | 1.98 | |
| Group × Time | 0.45 | 0.61 | 0.74 | 0.459 | −0.76 | 1.66 | |
| Confidence in infection control practice | Intercept | 3.24 | 0.14 | 22.37 | <0.001 | 2.95 | 3.53 |
| Group | −0.34 | 0.21 | −1.63 | 0.111 | −0.76 | 0.08 | |
| Time | 0.42 | 0.07 | 6.43 | <0.001 | 0.29 | 0.56 | |
| Group × Time | 0.23 | 0.09 | 2.41 | 0.022 | 0.03 | 0.42 | |
| Anxiety | Intercept | 2.41 | 0.13 | 17.95 | <0.001 | 2.14 | 2.67 |
| Group | 0.19 | 0.19 | 0.99 | 0.325 | −0.19 | 0.57 | |
| Time | −0.22 | 0.54 | −4.02 | <0.001 | −0.33 | −0.11 | |
| Group × Time | −0.10 | 0.08 | −1.23 | 0.224 | −0.25 | 0.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, D.; Park, C.; Eun, Y. Effects of Infection Control Education Program Using Flipped Learning Based on the ARCS Model for Nursing Students: A Mixed Method. Healthcare 2023, 11, 2731. https://doi.org/10.3390/healthcare11202731
Jeong D, Park C, Eun Y. Effects of Infection Control Education Program Using Flipped Learning Based on the ARCS Model for Nursing Students: A Mixed Method. Healthcare. 2023; 11(20):2731. https://doi.org/10.3390/healthcare11202731
Chicago/Turabian StyleJeong, Dain, Chang Park, and Young Eun. 2023. "Effects of Infection Control Education Program Using Flipped Learning Based on the ARCS Model for Nursing Students: A Mixed Method" Healthcare 11, no. 20: 2731. https://doi.org/10.3390/healthcare11202731
APA StyleJeong, D., Park, C., & Eun, Y. (2023). Effects of Infection Control Education Program Using Flipped Learning Based on the ARCS Model for Nursing Students: A Mixed Method. Healthcare, 11(20), 2731. https://doi.org/10.3390/healthcare11202731