_Rachiotis.png)
Mindful Self-Compassion as an Antidote to Burnout for Mental Health Practitioners


Abstract
1. Introduction
1.1. Burnout
1.2. Self-Care
1.3. Mindful Self-Compassion Practices as Self-Care
2. Materials and Methods
2.1. Study Design and Sample
2.2. Instrument
2.2.1. Self-Compassion
2.2.2. Burnout
2.3. Procedure
2.4. Ethical Consideration
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Sample
3.2. Levels of Self-Compassion and Burnout
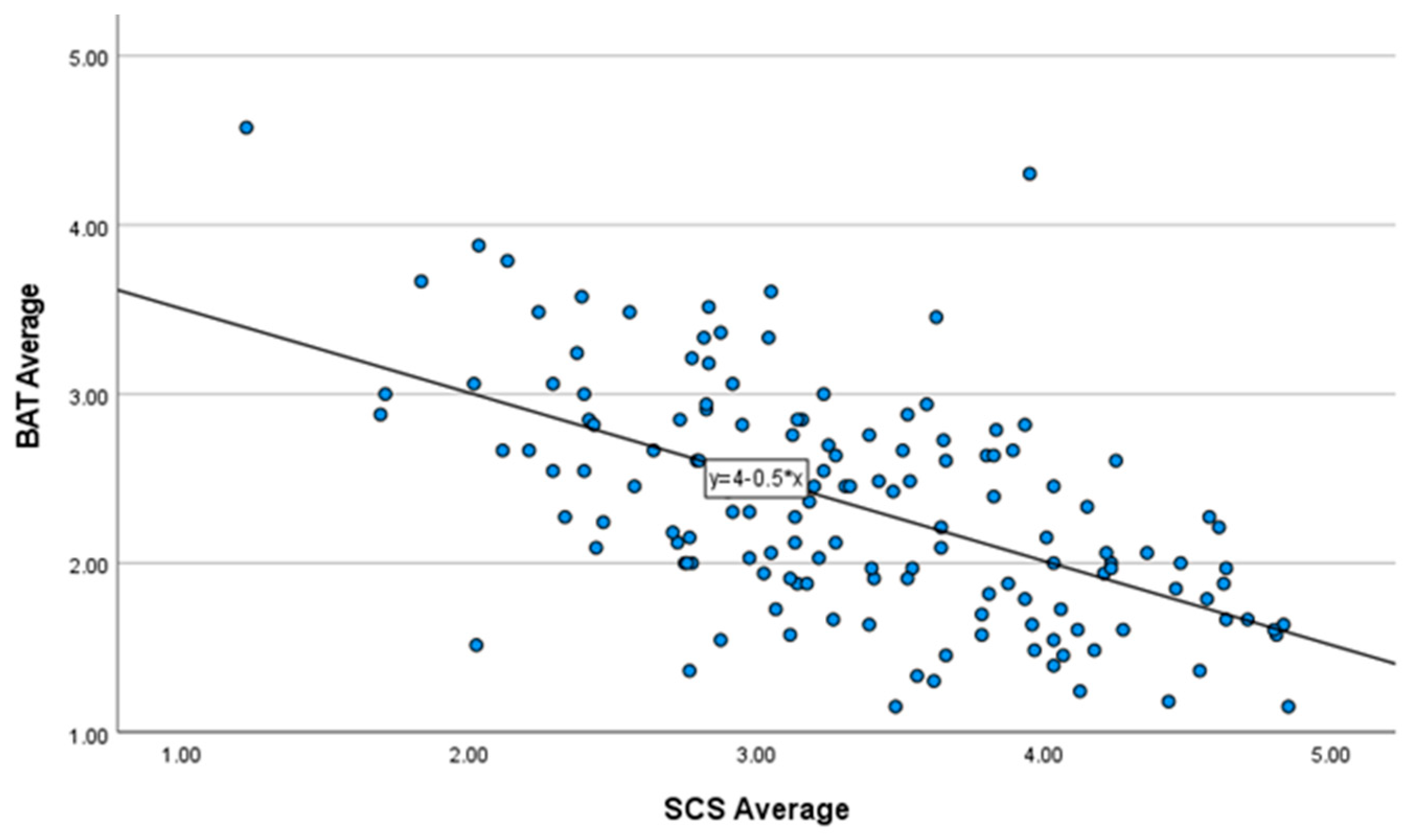
3.3. Regression Analysis
3.4. Scale Statistics
4. Discussion
4.1. Study Limitations
4.2. Recommendations for Practice and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Burn-Out an “Occupational Phenomenon”: International Classification of Diseases. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 1 June 2023).
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The Measurement of Experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Schaufeli, W.; De Witte, H. Work Engagement in Contrast to Burnout: Real or Redundant? Burn. Res. 2017, 5, 1–2. [Google Scholar] [CrossRef]
- Jackson, S.E.; Maslach, C. After-Effects of Job-Related Stress: Families as Victims. J. Organ. Behav. 1982, 3, 63–77. [Google Scholar] [CrossRef]
- Leiter, M.P.; Maslach, C. The Impact of Interpersonal Environment on Burnout and Organizational Commitment. J. Organ. Behav. 1988, 9, 297–308. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)—Development, Validity, and Reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Brenninkmeijer, V. How to Conduct Research on Burnout: Advantages and Disadvantages of a Unidimensional Approach in Burnout Research. Occup. Environ. Med. 2003, 60, i16–i20. [Google Scholar] [CrossRef] [PubMed]
- McCormack, H.M.; MacIntyre, T.E.; O’Shea, D.; Herring, M.P.; Campbell, M.J. The Prevalence and Cause(s) of Burnout among Applied Psychologists: A Systematic Review. Front. Psychol. 2018, 9, 1897. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the Burnout Experience: Recent Research and Its Implications for Psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Nadon, L.; De Beer, L.T.; Morin, A.J.S. Should Burnout Be Conceptualized as a Mental Disorder? Behav. Sci. 2022, 12, 82. [Google Scholar] [CrossRef]
- Schaufeli, W.; De Witte, H. Burnout Assessment Tool (BAT): A Fresh Look at Burnout. In International Handbook of Behavioral Health Assessment; Krägeloh, C.U., Alyami, M., Medvedev, O.N., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 1–24. ISBN 978-3-030-89738-3. [Google Scholar]
- Schaufeli, W.B.; De Witte, H.; Hakanen, J.J.; Kaltiainen, J.; Kok, R. How to Assess Severe Burnout? Cutoff Points for the Burnout Assessment Tool (BAT) Based on Three European Samples. Scand. J. Work Environ. Health 2023, 49, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Mental Health Practitioner Definition. Available online: https://www.lawinsider.com/dictionary/mental-health-practitioner (accessed on 7 June 2023).
- Yang, Y.; Hayes, J.A. Causes and Consequences of Burnout among Mental Health Professionals: A Practice-Oriented Review of Recent Empirical Literature. Psychotherapy 2020, 57, 426–436. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K.; Muller Neff, D.; Pitman, S. Burnout in Mental Health Professionals: A Systematic Review and Meta-Analysis of Prevalence and Determinants. Eur. Psychiatr. 2018, 53, 74–99. [Google Scholar] [CrossRef]
- Springer Publishing Company. Managing Stress during Your Counseling Practicum/Internship; Springer Publishing Company: New York, NY, USA, 2023; ISBN 978-0-8261-4302-0. [Google Scholar]
- Reed, K.; Cochran, K.L.; Edelblute, A.; Manzanares, D.; Sinn, H.; Henry, M.; Moss, M. Creative Arts Therapy as a Potential Intervention to Prevent Burnout and Build Resilience in Health Care Professionals. AACN Adv. Crit. Care 2020, 31, 179–190. [Google Scholar] [CrossRef]
- Simionato, G.K.; Simpson, S. Personal Risk Factors Associated with Burnout among Psychotherapists: A Systematic Review of the Literature. J. Clin. Psychol. 2018, 74, 1431–1456. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Sloan, J.A.; Shanafelt, T.D. Single Item Measures of Emotional Exhaustion and Depersonalization Are Useful for Assessing Burnout in Medical Professionals. J. Gen. Intern. Med. 2009, 24, 1318–1321. [Google Scholar] [CrossRef]
- Byrne, Z.S.; Peters, J.M.; Weston, J.W. The Struggle with Employee Engagement: Measures and Construct Clarification Using Five Samples. J. Appl. Psychol. 2016, 101, 1201–1227. [Google Scholar] [CrossRef] [PubMed]
- Taris, T.W.; Ybema, J.F.; Beek, I.V. Burnout and Engagement: Identical Twins or Just Close Relatives? Burn. Res. 2017, 5, 3–11. [Google Scholar] [CrossRef]
- Edú-Valsania, S.; Laguía, A.; Moriano, J.A. Burnout: A Review of Theory and Measurement. Int. J. Environ. Res. Public Health 2022, 19, 1780. [Google Scholar] [CrossRef] [PubMed]
- Shoji, K.; Cieslak, R.; Smoktunowicz, E.; Rogala, A.; Benight, C.C.; Luszczynska, A. Associations between Job Burnout and Self-Efficacy: A Meta-Analysis. Anxiety Stress Coping 2016, 29, 367–386. [Google Scholar] [CrossRef]
- Ekman, E.; Halpern, J. Professional Distress and Meaning in Health Care: Why Professional Empathy Can Help. Soc. Work. Health Care 2015, 54, 633–650. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, J.N.; Still, M. Relationships between Burnout, Turnover Intention, Job Satisfaction, Job Demands and Job Resources for Mental Health Personnel in an Australian Mental Health Service. BMC Health Serv. Res. 2019, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.E.; Prins, A.; Bush, N.E.; Hsia, J.F.; Bourn, L.E.; Earley, M.D.; Walser, R.D.; Ruzek, J. Reduction of Burnout in Mental Health Care Providers Using the Provider Resilience Mobile Application. Community Ment. Health J. 2017, 53, 452–459. [Google Scholar] [CrossRef]
- Auerbach, J.; Miller, B.F. COVID-19 Exposes the Cracks in Our Already Fragile Mental Health System. Am. J. Public Health 2020, 110, 969–970. [Google Scholar] [CrossRef] [PubMed]
- Bressi, S.K.; Vaden, E.R. Reconsidering Self Care. Clin. Soc. Work J. 2017, 45, 33–38. [Google Scholar] [CrossRef]
- Crowder, R.; Sears, A. Building Resilience in Social Workers: An Exploratory Study on the Impacts of a Mindfulness-Based Intervention. Aust. Soc. Work 2017, 70, 17–29. [Google Scholar] [CrossRef]
- Narasimhan, M.; Kapila, M. Implications of Self-Care for Health Service Provision. Bull. World Health Organ. 2019, 97, 76. [Google Scholar] [CrossRef]
- Norcross, J.C.; Phillips, C.M. Psychologist Self-Care during the Pandemic: Now More than Ever. J. Health Serv. Psychol. 2020, 46, 59–63. [Google Scholar] [CrossRef]
- Posluns, K.; Gall, T.L. Dear Mental Health Practitioners, Take Care of Yourselves: A Literature Review on Self-Care. Int. J. Adv. Couns. 2020, 42, 1–20. [Google Scholar] [CrossRef]
- Wei, H.; Kifner, H.; Dawes, M.E.; Wei, T.L.; Boyd, J.M. Self-Care Strategies to Combat Burnout among Pediatric Critical Care Nurses and Physicians. Crit. Care Nurse 2020, 40, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Dattilio, F.M. The Self-Care of Psychologists and Mental Health Professionals: A Review and Practitioner Guide. Aust. Psychol. 2015, 50, 393–399. [Google Scholar] [CrossRef]
- Pakenham, K.I. Comment on “The Self-Care of Psychologists and Mental Health Professionals” (Dattilio, 2015). Aust. Psychol. 2015, 50, 405–408. [Google Scholar] [CrossRef]
- Butts, C.M.; Gutierrez, D. Dispositional Mindfulness and Personal Distress as Predictors of Counseling Self-Efficacy. Couns. Educ. Superv. 2018, 57, 271–284. [Google Scholar] [CrossRef]
- Rudaz, M.; Twohig, M.P.; Ong, C.W.; Levin, M.E. Mindfulness and Acceptance-Based Trainings for Fostering Self-Care and Reducing Stress in Mental Health Professionals: A Systematic Review. J. Context. Behav. Sci. 2017, 6, 380–390. [Google Scholar] [CrossRef]
- Butler, L.D.; Mercer, K.A.; McClain-Meeder, K.; Horne, D.M.; Dudley, M. Six Domains of Self-Care: Attending to the Whole Person. J. Hum. Behav. Soc. Environ. 2019, 29, 107–124. [Google Scholar] [CrossRef]
- Edwards, J.L.; Crisp, D.A. Seeking Help for Psychological Distress: Barriers for Mental Health Professionals. Aust. J. Psychol. 2017, 69, 218–225. [Google Scholar] [CrossRef]
- Kissil, K.; Niño, A. Does the Person-of-the-Therapist Training (POTT) Promote Self-Care? Personal Gains of MFT Trainees Following POTT: A Retrospective Thematic Analysis. J. Marital. Fam. Ther. 2017, 43, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Prasada, K.D.V.; Vaidyab, R.W.; Mangipudic, M.R. Effect of Occupational Stress and Remote Working on Psychological Well-Being of Employees: An Empirical Analysis during COVID-19 Pandemic Concerning Information Technology Industry in Hyderabad. Indian J. Commer. Manag. Stud. 2020, XI, 1. [Google Scholar] [CrossRef]
- Rokach, A.; Boulazreg, S. The COVID-19 Era: How Therapists Can Diminish Burnout Symptoms through Self-Care. Curr. Psychol. 2022, 41, 5660–5677. [Google Scholar] [CrossRef]
- Creswell, J.D. Mindfulness Interventions. Annu. Rev. Psychol. 2017, 68, 491–516. [Google Scholar] [CrossRef]
- De Vibe, M.; Solhaug, I.; Rosenvinge, J.H.; Tyssen, R.; Hanley, A.; Garland, E. Six-Year Positive Effects of a Mindfulness-Based Intervention on Mindfulness, Coping and Well-Being in Medical and Psychology Students; Results from a Randomized Controlled Trial. PLoS ONE 2018, 13, e0196053. [Google Scholar] [CrossRef]
- Nelson, J.R.; Hall, B.S.; Anderson, J.L.; Birtles, C.; Hemming, L. Self–Compassion as Self-Care: A Simple and Effective Tool for Counselor Educators and Counseling Students. J. Creat. Ment. Health 2018, 13, 121–133. [Google Scholar] [CrossRef]
- Sonnentag, S. Burnout Research: Adding an off-Work and Day-Level perspective. Work Stress 2005, 19, 271–275. [Google Scholar] [CrossRef][Green Version]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A Systematic Review of the Impact of Mindfulness on the Well-Being of Healthcare Professionals. J. Clin. Psychol. 2018, 74, 319–355. [Google Scholar] [CrossRef] [PubMed]
- Beer, O.W.; Phillips, R.; Stepney, L.; Quinn, C.R. OUP Accepted Manuscript. Br. J. Soc. Work 2020, 50, 243–263. [Google Scholar] [CrossRef]
- Coaston, S.C. Self-Care Through Self-Compassion: A Balm for Burnout. Prof. Couns. 2017, 7, 285–297. [Google Scholar] [CrossRef]
- Germer, C.K.; Neff, K.D. Self-Compassion in Clinical Practice: Self-Compassion. J. Clin. Psychol. 2013, 69, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Lakioti, A.; Stalikas, A.; Pezirkianidis, C. The Role of Personal, Professional, and Psychological Factors in Therapists’ Resilience. Prof. Psychol. Res. Pract. 2020, 51, 560–570. [Google Scholar] [CrossRef]
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude toward Oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef]
- Eriksson, T.; Germundsjö, L.; Åström, E.; Rönnlund, M. Mindful Self-Compassion Training Reduces Stress and Burnout Symptoms among Practicing Psychologists: A Randomized Controlled Trial of a Brief Web-Based Intervention. Front. Psychol. 2018, 9, 2340. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D.; Tóth-Király, I.; Knox, M.C.; Kuchar, A.; Davidson, O. The Development and Validation of the State Self-Compassion Scale (Long- and Short Form). Mindfulness 2021, 12, 121–140. [Google Scholar] [CrossRef]
- Jaarsma, T.; Strömberg, A.; Dunbar, S.B.; Fitzsimons, D.; Lee, C.; Middleton, S.; Vellone, E.; Freedland, K.E.; Riegel, B. Self-Care Research: How to Grow the Evidence Base? Int. J. Nurs. Stud. 2020, 105, 103555. [Google Scholar] [CrossRef] [PubMed]
- Eller, L.S.; Lev, E.L.; Yuan, C.; Watkins, A.V. Describing Self-Care Self-Efficacy: Definition, Measurement, Outcomes, and Implications: Describing Self-Care Self-Efficacy. Int. J. Nurs. Termin. Knowl. 2018, 29, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D.; Costigan, A. Self-Compassion, Wellbeing, and Happiness. Psychol. Osterr. 2014, 2, 114–119. [Google Scholar]
- Bluth, K.; Eisenlohr-Moul, T.A. Response to a Mindful Self-compassion Intervention in Teens: A within-Person Association of Mindfulness, Self-Compassion, and Emotional Well-Being Outcomes. J. Adolesc. 2017, 57, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Olson, K.; Kemper, K.J. Factors Associated with Well-Being and Confidence in Providing Compassionate Care. J. Evid. Based Complement. Altern. Med. 2014, 19, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations: Burnout in Healthcare Providers. Arch. Acad. Emerg. Med. 2020, 9, e7. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, S.; Kondejewski, J.; Raffin-Bouchal, S.; King-Shier, K.M.; Singh, P. Can Self-Compassion Promote Healthcare Provider Well-Being and Compassionate Care to Others? Results of a Systematic Review. Appl. Psychol. Health Well-Being 2017, 9, 168–206. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D. The Development and Validation of a Scale to Measure Self-Compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill Series in Psychology; Tata McGraw Hill Education Private Ltd.: New Delhi, India, 2010; ISBN 978-0-07-107088-1. [Google Scholar]
- Azizi, A.; Mohammadkhani, P.; Foroughi, A.A.; Lotfi, S.; Bahramkhani, M. The Validity and Reliability of the Iranian Version of the Self-Compassion Scale. Pract. Clin. Psychol. 2013, 1, 149–155. [Google Scholar]
- Chen, J.; Yan, L.; Zhou, L. Reliability and Validity of Chinese Version of Self-compassion Scale. Chin. J. Clin. Psychol. 2011, 19, 734–736. [Google Scholar]
- American Psychological Association Ethical Principles of Psychologists and Code of Conduct. Available online: https://www.apa.org/ethics/code (accessed on 1 June 2023).
- IBM SPSS Statistics. Available online: https://www.ibm.com/products/spss-statistics (accessed on 1 June 2023).
- Corrales, D.; Corrales, J.; Ledezma, A. How to Address the Data Quality Issues in Regression Models: A Guided Process for Data Cleaning. Symmetry 2018, 10, 99. [Google Scholar] [CrossRef]
- Laerd Statistics. Multiple Regression Using SPSS Statistics. Statistical Tutorials and Software Guides. Available online: https://statistics.laerd.com/ (accessed on 28 July 2022).
- Tadiri, C.P.; Raparelli, V.; Abrahamowicz, M.; Kautzy-Willer, A.; Kublickiene, K.; Herrero, M.-T.; Norris, C.M.; Pilote, L. Methods for Prospectively Incorporating Gender into Health Sciences Research. J. Clin. Epidemiol. 2021, 129, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.P.; Einstein, D.A. Self-Compassion Interventions and Psychosocial Outcomes: A Meta-Analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [Google Scholar] [CrossRef]
- Beaumont, E.; Durkin, M.; Hollins Martin, C.J.; Carson, J. Measuring Relationships between Self-Compassion, Compassion Fatigue, Burnout and Well-Being in Student Counsellors and Student Cognitive Behavioural Psychotherapists: A Quantitative Survey. Couns. Psychother. Res. 2016, 16, 15–23. [Google Scholar] [CrossRef]
- George, L.; Wallace, J.C.; Snider, J.B.; Suh, H. Self-Compassion, Performance, and Burnout: Surfacing an Unknown Work Construct. Group Organ. Manag. 2023, 105960112311611. [Google Scholar] [CrossRef]
- Luo, X.; Qiao, L.; Che, X. Self-Compassion Modulates Heart Rate Variability and Negative Affect to Experimentally Induced Stress. Mindfulness 2018, 9, 1522–1528. [Google Scholar] [CrossRef]
- Westwood, S.; Morison, L.; Allt, J.; Holmes, N. Predictors of Emotional Exhaustion, Disengagement and Burnout among Improving Access to Psychological Therapies (IAPT) Practitioners. J. Ment. Health 2017, 26, 172–179. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, L.M.-H. Impact of Working from Home on Addressing Practitioner Burnout and Work–Life Balance in Mental Health. Perm. J. 2022, 26, 77–82. [Google Scholar] [CrossRef]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE: Los Angeles, CA, USA, 2018; ISBN 978-1-5063-8670-6. [Google Scholar]
- Trochim, W.M.K.; Donnelly, J.P.; Arora, K. Research Methods: The Essential Knowledge Base; Student ed.; Cengage Learning: Boston, MA, USA, 2016; ISBN 978-1-133-95477-4. [Google Scholar]
- Rohrer, J.M. Thinking Clearly About Correlations and Causation: Graphical Causal Models for Observational Data. Adv. Methods Pract. Psychol. Sci. 2018, 1, 27–42. [Google Scholar] [CrossRef]
- Kashner, T.M.; Henley, S.S.; Golden, R.M.; Zhou, X.-H. Making Causal Inferences about Treatment Effect Sizes from Observational Datasets. Biostat. Epidemiol. 2020, 4, 48–83. [Google Scholar] [CrossRef]
- Jackson, S.L. Research Methods and Statistics: A Critical Thinking Approach, 5th ed.; Cengage Learning: Melbourne, Australia, 2015; ISBN 978-1-305-25779-5. [Google Scholar]
- Prior, M. The Immensely Inflated News Audience: Assessing Bias in Self-Reported News Exposure. Public Opin. Q. 2009, 73, 130–143. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM® SPSS® Statistics, North American edition, 5th ed.; Seaman, J., Ed.; SAGE: Los Angeles, CA, USA; London, UK; New Delhi, India, 2018; ISBN 978-1-5264-3656-6. [Google Scholar]
- Parker, C.; Scott, S.; Geddes, A. Snowball Sampling. In SAGE Research Methods Foundations; SAGE Publications Ltd.: London, UK, 2020; ISBN 978-1-5264-2103-6. [Google Scholar]
- Greenacre, Z.A. The Importance of Selection Bias in Internet Surveys. Open J. Stat. 2016, 6, 397–404. [Google Scholar] [CrossRef]
- Wright, G. An Empirical Examination of the Relationship between Nonresponse Rate and Nonresponse Bias. Stat. J. IAOS 2015, 31, 305–315. [Google Scholar] [CrossRef]
- Schabram, K.; Heng, Y.T. How Other- and Self-Compassion Reduce Burnout through Resource Replenishment. Acad. Manag. J. 2021, 65, 453–478. [Google Scholar] [CrossRef]
- Zhang, L.; Ren, Z.; Jiang, G.; Hazer-Rau, D.; Zhao, C.; Shi, C.; Lai, L.; Yan, Y. Self-Oriented Empathy and Compassion Fatigue: The Serial Mediation of Dispositional Mindfulness and Counselor’s Self-Efficacy. Front. Psychol. 2021, 11, 613908. [Google Scholar] [CrossRef]
- New Nationwide Poll Shows an Increased Popularity for Telehealth Services. Available online: https://www.psychiatry.org:443/news-room/news-releases/new-nationwide-poll-shows-an-increased-popularity (accessed on 8 September 2023).
- Telehealth Is Here to Stay. Psychologists Should Equip Themselves to Offer It. Available online: https://www.apa.org/monitor/2022/10/future-of-telehealth (accessed on 8 September 2023).
- Hadžibajramović, E.; Schaufeli, W.; De Witte, H. A Rasch Analysis of the Burnout Assessment Tool (BAT). PLoS ONE 2020, 15, e0242241. [Google Scholar] [CrossRef]
- Dodson, S.J.; Heng, Y.T. Self-compassion in Organizations: A Review and Future Research Agenda. J. Organ. Behav. 2022, 43, 168–196. [Google Scholar] [CrossRef]
- Cunningham, S. Causal Inference: The Mixtape; Yale University Press: New Haven, CT, USA; London, UK, 2021; ISBN 978-0-300-25168-5. [Google Scholar]


{kind=link}
| Scale | M | SD | Min. | Max. |
|---|---|---|---|---|
| Total SCS | 3.34 | 0.77 | 1.23 | 4.85 |
| Self-kindness | 3.36 | 0.85 | 1.20 | 5.00 |
| Self-judgment | 3.15 | 0.96 | 1.00 | 5.00 |
| Common Humanity | 3.45 | 0.90 | 1.50 | 5.00 |
| Isolation | 3.20 | 1.02 | 1.00 | 5.00 |
| Mindfulness | 3.68 | 0.80 | 1.25 | 5.00 |
| Over-identification | 3.21 | 0.93 | 1.00 | 5.00 |
| Total BAT | 2.34 | 0.67 | 1.15 | 4.58 |
| Exhaustion | 2.83 | 0.94 | 1.00 | 5.00 |
| Mental Distance | 2.00 | 0.81 | 1.00 | 5.00 |
| Cognitive Impairment | 2.20 | 0.82 | 1.00 | 4.80 |
| Emotional Impairment | 1.62 | 0.66 | 1.00 | 5.00 |
| Psychological Distress | 2.84 | 0.95 | 1.00 | 4.80 |
| Psychosomatic Distress | 2.25 | 0.80 | 1.00 | 4.20 |
| Scale | Cutoff Values | n (%) |
|---|---|---|
| SCS | ||
| Low self-compassion | 1.0–2.5 | 22 (15.3) |
| Moderate self-compassion | 2.5–3.5 | 61 (42.4) |
| High self-compassion | 3.5–5.0 | 61 (42.4) |
| BAT | ||
| Green (No burnout) | ≤2.58 | 100 (69.4) |
| Orange (At risk of burnout) | 2.59 to 3.01 | 23 (16.0) |
| Red (Likely burnout) | ≥3.02 | 21 (14.6) |
| 95% CI for B | |||||||
|---|---|---|---|---|---|---|---|
| B | LL | UL | SE B | β | p | R2 | |
| Model 1 | <0.001 | 0.313 | |||||
| Constant | 30.990 | 30.566 | 40.414 | 0.214 | <0.001 | ||
| Self-compassion | −0.492 | −0.617 | −0.368 | 0.063 | −0.560 | <0.001 | |
| Model 2 | <0.001 | 0.368 | |||||
| Constant | 30.516 | 20.941 | 40.091 | 0.291 | <0.001 | ||
| Self-compassion | −0.451 | −0.576 | −0.327 | 0.063 | −0.513 | <0.001 | |
| Years of experience | −0.009 | −0.022 | 0.003 | 0.006 | −0.110 | 0.136 | |
| Hrs. Worked/Week | 0.012 | 0.003 | 0.020 | 0.004 | 0.205 | 0.008 | |
| Telepsychology | 0.001 | −0.001 | 0.004 | 0.001 | 0.081 | 0.276 | |
| SCS Scale | Scale Items | SCS Test Sample | U.S. MHP Sample |
|---|---|---|---|
| Total | 1–26 | 0.92 | 0.95 |
| Self-kindness | 5, 12, 19, 23, 26 | 0.78 | 0.86 |
| Self-judgment | 1, 8, 11, 16, 21 | 0.77 | 0.87 |
| Common humanity | 3, 7, 10, 15 | 0.80 | 0.80 |
| Isolation | 4, 13, 18, 25 | 0.79 | 0.84 |
| Mindfulness | 9, 14, 17, 22 | 0.75 | 0.82 |
| Over-identification | 2, 6, 20, 24 | 0.81 | 0.81 |
| BAT Scale | Scale Items | Flanders Sample | Netherlands Sample | U.S. MHP Sample |
|---|---|---|---|---|
| Total core symptoms | 1–23 | 0.96 | 0.97 | 0.95 |
| Exhaustion | 1–8 | 0.92 | 0.94 | 0.92 |
| Mental distance | 9–13 | 0.91 | 0.93 | 0.82 |
| Emotional impairment | 14–18 | 0.90 | 0.94 | 0.83 |
| Cognitive impairment | 19–23 | 0.92 | 0.94 | 0.90 |
| Total secondary symptoms | 24–33 | 0.89 | 0.94 | 0.82 |
| Psychological complaints | 24–28 | * | * | 0.82 |
| Psychosomatic complaints | 29–33 | * | * | 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyon, T.R.; Galbraith, A. Mindful Self-Compassion as an Antidote to Burnout for Mental Health Practitioners. Healthcare 2023, 11, 2715. https://doi.org/10.3390/healthcare11202715
Lyon TR, Galbraith A. Mindful Self-Compassion as an Antidote to Burnout for Mental Health Practitioners. Healthcare. 2023; 11(20):2715. https://doi.org/10.3390/healthcare11202715
Chicago/Turabian StyleLyon, T. Richelle, and Anne Galbraith. 2023. "Mindful Self-Compassion as an Antidote to Burnout for Mental Health Practitioners" Healthcare 11, no. 20: 2715. https://doi.org/10.3390/healthcare11202715
APA StyleLyon, T. R., & Galbraith, A. (2023). Mindful Self-Compassion as an Antidote to Burnout for Mental Health Practitioners. Healthcare, 11(20), 2715. https://doi.org/10.3390/healthcare11202715