
Oscillation of Sympathetic Activity in Patients with Obstructive Sleep Apnea during the First Hour of Sleep


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Participants
2.3. PSG and HRV Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jafari, B. Sleep Architecture and Blood Pressure. Sleep Med. Clin. 2017, 12, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Somers, V.K.; Dyken, M.E.; Mark, A.L.; Abboud, F.M. Sympathetic-nerve activity during sleep in normal subjects. N. Engl. J. Med. 1993, 328, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef]
- Yacoub, M.; Youssef, I.; Salifu, M.O.; McFarlane, S.I. Cardiovascular Disease Risk in Obstructive Sleep apnea: An Update. J. Sleep Disord. Ther. 2017, 7, 283. [Google Scholar] [CrossRef]
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA 2020, 323, 1389–1400. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Guilleminault, C.; Priest, R.G.; Caulet, M. Snoring and breathing pauses during sleep: Telephone interview survey of a United Kingdom population sample. BMJ 1997, 314, 860–863. [Google Scholar] [CrossRef]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef]
- Stoohs, R.A.; Blum, H.C.; Haselhorst, M.; Duchna, H.W.; Guilleminault, C.; Dement, W.C. Normative data on snoring: A comparison between younger and older adults. Eur. Respir. J. 1998, 11, 451–457. [Google Scholar] [CrossRef]
- Young, T.; Finn, L.; Hla, K.M.; Morgan, B.; Palta, M. Snoring as part of a dose-response relationship between sleep-disordered breathing and blood pressure. Sleep 1996, 19 (Suppl. 10), S202–S205. [Google Scholar] [CrossRef]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Ten Have, T.; Leiby, B.E.; Vela-Bueno, A.; Kales, A. Association of hypertension and sleep-disordered breathing. Arch. Intern. Med. 2000, 160, 2289–2295. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, D.S.; Oksenberg, A. Are sleep-related breathing disorders important contributing factors to the production of essential hypertension? Curr. Hypertens. Rep. 2001, 3, 209–215. [Google Scholar] [CrossRef]
- Guilleminault, C.; Stoohs, R.; Shiomi, T.; Kushida, C.; Schnittger, I. Upper airway resistance syndrome, nocturnal blood pressure monitoring, and borderline hypertension. Chest 1996, 109, 901–908. [Google Scholar] [CrossRef]
- Kohler, M.; Stradling, J.R. Mechanisms of vascular damage in obstructive sleep apnea. Nat. Rev. Cardiol. 2010, 7, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, P.; Perrault, H.; Dinh, T.P.; Eberhard, A.; Benchetrit, G. Cardiorespiratory interactions during resistive load breathing. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R2208–R2213. [Google Scholar] [CrossRef] [PubMed]
- Henke, K.G.; Sullivan, C.E. Effects of high-frequency oscillating pressures on upper airway muscles in humans. J. Appl. Physiol. 1993, 75, 856–862. [Google Scholar] [CrossRef]
- Stoohs, R.; Guilleminault, C. Snoring during NREM sleep: Respiratory timing, esophageal pressure and EEG arousal. Respir. Physiol. 1991, 85, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Abeyratne, U.R.; Wakwella, A.S.; Hukins, C. Pitch jump probability measures for the analysis of snoring sounds in apnea. Physiol. Meas. 2005, 26, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Kao, H.H.; Lin, Y.C.; Chiang, J.K.; Yu, H.C.; Wang, C.L.; Kao, Y.H. Dependable algorithm for visualizing snoring duration through acoustic analysis: A pilot study. Medicine 2022, 101, e32538. [Google Scholar] [CrossRef]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Kamandulis, S.; Juodsnukis, A.; Stanislovaitiene, J.; Zuoziene, I.J.; Bogdelis, A.; Mickevicius, M.; Eimantas, N.; Snieckus, A.; Olstad, B.H.; Venckunas, T. Daily Resting Heart Rate Variability in Adolescent Swimmers during 11 Weeks of Training. Int. J. Environ. Res. Public Health 2020, 17, 2097. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, V.C.C.; Bandeira, P.M.; Azevedo, J.C.M. Heart rate variability in adults with obstructive sleep apnea: A systematic review. Sleep Sci. 2019, 12, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Boudreau, P.; Yeh, W.H.; Dumont, G.A.; Boivin, D.B. Circadian variation of heart rate variability across sleep stages. Sleep 2013, 36, 1919–1928. [Google Scholar] [CrossRef] [PubMed]
- AlQatari, A.A.; Alturki, J.A.; Abdulali, K.A.; Alhumud, D.A.; Alibrahim, M.A.; Alarab, Y.A.; Salem, A.M.; Yar, T.; Alqurashi, Y.D.; Alsunni, A.A.; et al. Changes in Heart Rate Variability and Baroreflex Sensitivity During Daytime Naps. Nat. Sci. Sleep 2020, 12, 661–669. [Google Scholar] [CrossRef]
- Lin, Y.C.; Chiang, J.K.; Lu, C.M.; Kao, Y.H. Association of Heart Rate Variability with Obstructive Sleep Apnea in Adults. Medicina 2023, 59, 471. [Google Scholar] [CrossRef]
- Castro-Diehl, C.; Diez Roux, A.V.; Redline, S.; Seeman, T.; McKinley, P.; Sloan, R.; Shea, S. Sleep Duration and Quality in Relation to Autonomic Nervous System Measures: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2016, 39, 1927–1940. [Google Scholar] [CrossRef]
- Oliver, M.D.; Baldwin, D.R.; Datta, S. The relationship between sleep and autonomic health. J. Am. Coll. Health 2020, 68, 550–556. [Google Scholar] [CrossRef]
- Dimyan, M.A.; Cohen, L.G. Contribution of transcranial magnetic stimulation to the understanding of functional recovery mechanisms after stroke. Neurorehabil. Neural Repair 2010, 24, 125–135. [Google Scholar] [CrossRef]
- Alves, C.L.; Fagundes, D.M.; Soares, P.B.F.; Ferreira, M.C. Knowledge of parents/caregivers about bruxism in children treated at the pediatric dentistry clinic. Sleep Sci. 2019, 12, 185–189. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef] [PubMed]
- Domenico, C.; Michele, T.; Giuseppe, B.; Donatella, F.; Pia, C.A.; Michele, L.; Gaetano, I.; Carmela, S.; Michele, C. Respiratory and Cardiovascular Parameters Evaluation in OSA Patients Treated with Mandibular Advancement Device. Appl. Sci. 2020, 10, 8175. [Google Scholar] [CrossRef]
- Venkataraman, S.; Vungarala, S.; Covassin, N.; Somers, V.K. Sleep Apnea, Hypertension and the Sympathetic Nervous System in the Adult Population. J. Clin. Med. 2020, 9, 591. [Google Scholar] [CrossRef]
- Maier, L.E.; Matenchuk, B.A.; Vucenovic, A.; Sivak, A.; Davenport, M.H.; Steinback, C.D. Influence of Obstructive Sleep Apnea Severity on Muscle Sympathetic Nerve Activity and Blood Pressure: A Systematic Review and Meta-Analysis. Hypertension 2022, 79, 2091–2104. [Google Scholar] [CrossRef] [PubMed]
- Narkiewicz, K.; Kato, M.; Phillips, B.G.; Pesek, C.A.; Davison, D.E.; Somers, V.K. Nocturnal continuous positive airway pressure decreases daytime sympathetic traffic in obstructive sleep apnea. Circulation 1999, 100, 2332–2335. [Google Scholar] [CrossRef] [PubMed]
- Kufoy, E.; Palma, J.A.; Lopez, J.; Alegre, M.; Urrestarazu, E.; Artieda, J.; Iriarte, J. Changes in the heart rate variability in patients with obstructive sleep apnea and its response to acute CPAP treatment. PLoS ONE 2012, 7, e33769. [Google Scholar] [CrossRef]
- Coruzzi, P.; Gualerzi, M.; Bernkopf, E.; Brambilla, L.; Brambilla, V.; Broia, V.; Lombardi, C.; Parati, G. Autonomic cardiac modulation in obstructive sleep apnea: Effect of an oral jaw-positioning appliance. Chest 2006, 130, 1362–1368. [Google Scholar] [CrossRef]
- Glos, M.; Penzel, T.; Schoebel, C.; Nitzsche, G.R.; Zimmermann, S.; Rudolph, C.; Blau, A.; Baumann, G.; Jost-Brinkmann, P.G.; Rautengarten, S.; et al. Comparison of effects of OSA treatment by MAD and by CPAP on cardiac autonomic function during daytime. Sleep Breath 2016, 20, 635–646. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Mild–Moderate: 5 < AHI ≤ 30 | Severe: AHI > 30 | T or W or χ2 | df | p | |
|---|---|---|---|---|---|---|
| Number | 45 | 27 | 18 | |||
| Age, years | 43.8 ± 11.9 | 45.4 ± 12.8 | 41.5 ± 10.4 | 1.080 | 43 | 0.286 |
| BMI, kg/m2 | 29.1 ± 5.4 | 27.6 ± 4.1 | 31.3 ± 6.4 | −2.174 | 26.3 | 0.039 |
| Neck circumference, cm | 40.0 (38.0, 43.0) | 39.0 (37.0, 41.5) | 42.0 (40.0, 45.5) | 116.5 | 0.003 | |
| AHI | 20.6 (9.1, 56.6) | 10.6 (7.6, 19.4) | 62.3 (41.2, 73.6) | 0 | <0.001 | |
| Center of pre-S episode, min | 7.5 (2.5, 15.0) | 15.0 (7.5, 15.0) | 2.5 (2.5, 13.1) | 341 | 0.019 | |
| Center of S episode, min | 15.0 (7.5, 25.0) | 25.0 (15.0, 35.0) | 7.5 (7.5, 22.5) | 344.5 | 0.016 | |
| Center of S episode within 10 min, yes vs. no | 17/28 | 5/22 | 12/6 | 10.6 | 1 | 0.001 |
| Center of S episode within 30 min, yes vs. no | 34/11 | 19/8 | 15/3 | 1.0 | 1 | 0.322 |
| Pre-S episode LF/HF ratio | 1.83 ± 1.00 | 1.9 ± 1.1 | 1.8 ± 0.9 | 0.4 | 43 | 0.712 |
| Pre-S episode RMSSD, msec | 39.8 (26.8, 72.2) | 35.8 (26.6, 63.3) | 59.7 (28.4, 72.1) | 202 | 0.354 | |
| S episode LF/HF ratio | 1.77 ± 0.99 | 1.61 ± 0.99 | 1.99 ± 0.97 | −1.3 | 43 | 0.212 |
| S episode RMSSD, msec | 46.5 (29.7, 101.3) | 39.6 (29.8, 71.8) | 67.2 (30.8, 121.9) | 197 | 0.295 |
| 0–5 min | 5–10 min | 10–20 min | 20–30 min | 30–40 min | 40–50 min | 50–60 min | Df | F | p | |
|---|---|---|---|---|---|---|---|---|---|---|
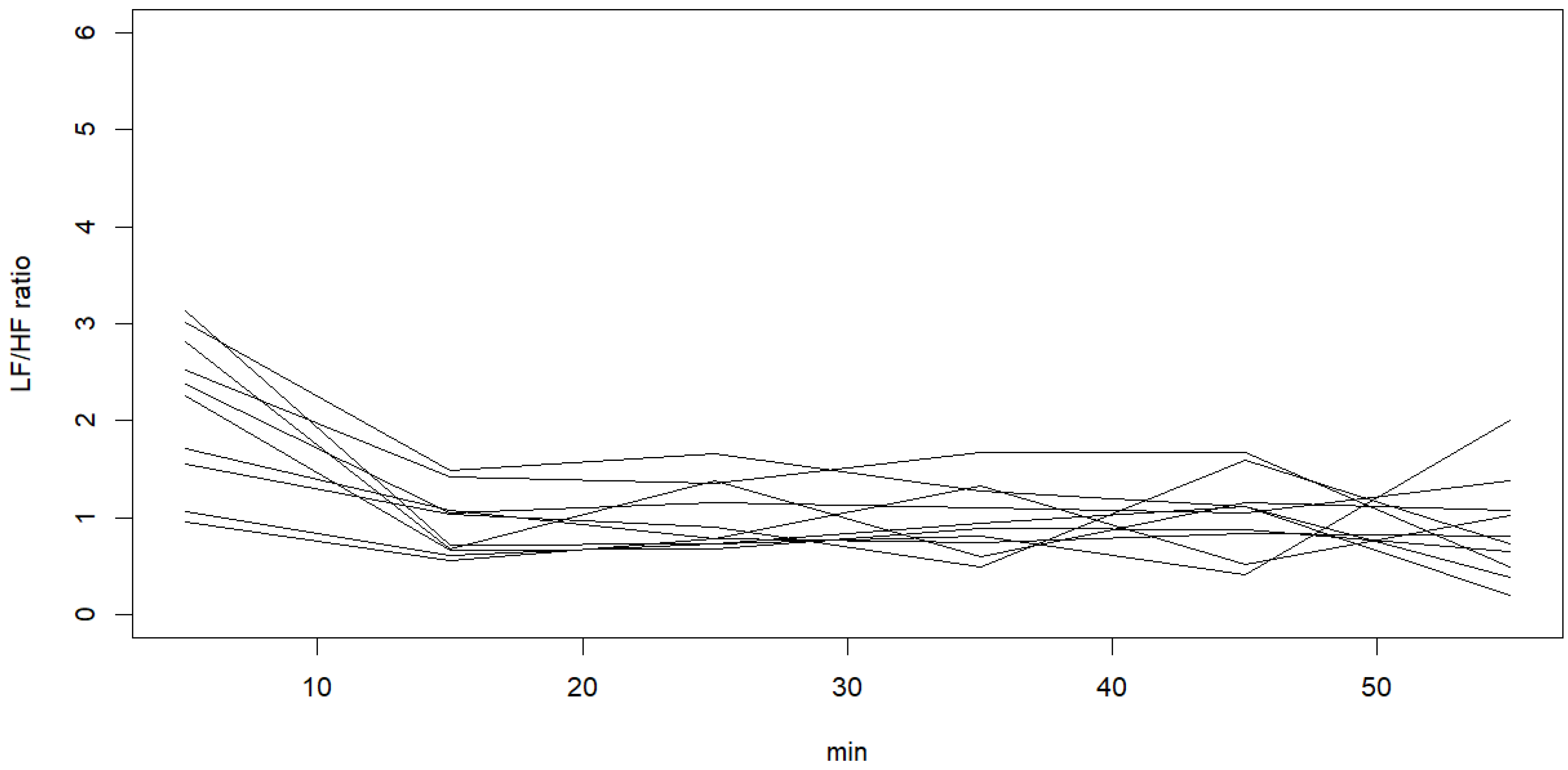
| LF/HF ratio | 2.40 ± 0.78 | 2.29 ± 0.65 | 1.15 ± 0.85 | 1.20 ± 0.85 | 1.13 ± 0.76 | 1.07 ± 0.59 | 1.87 ± 2.49 | 1 | 13.19 | <0.001 |
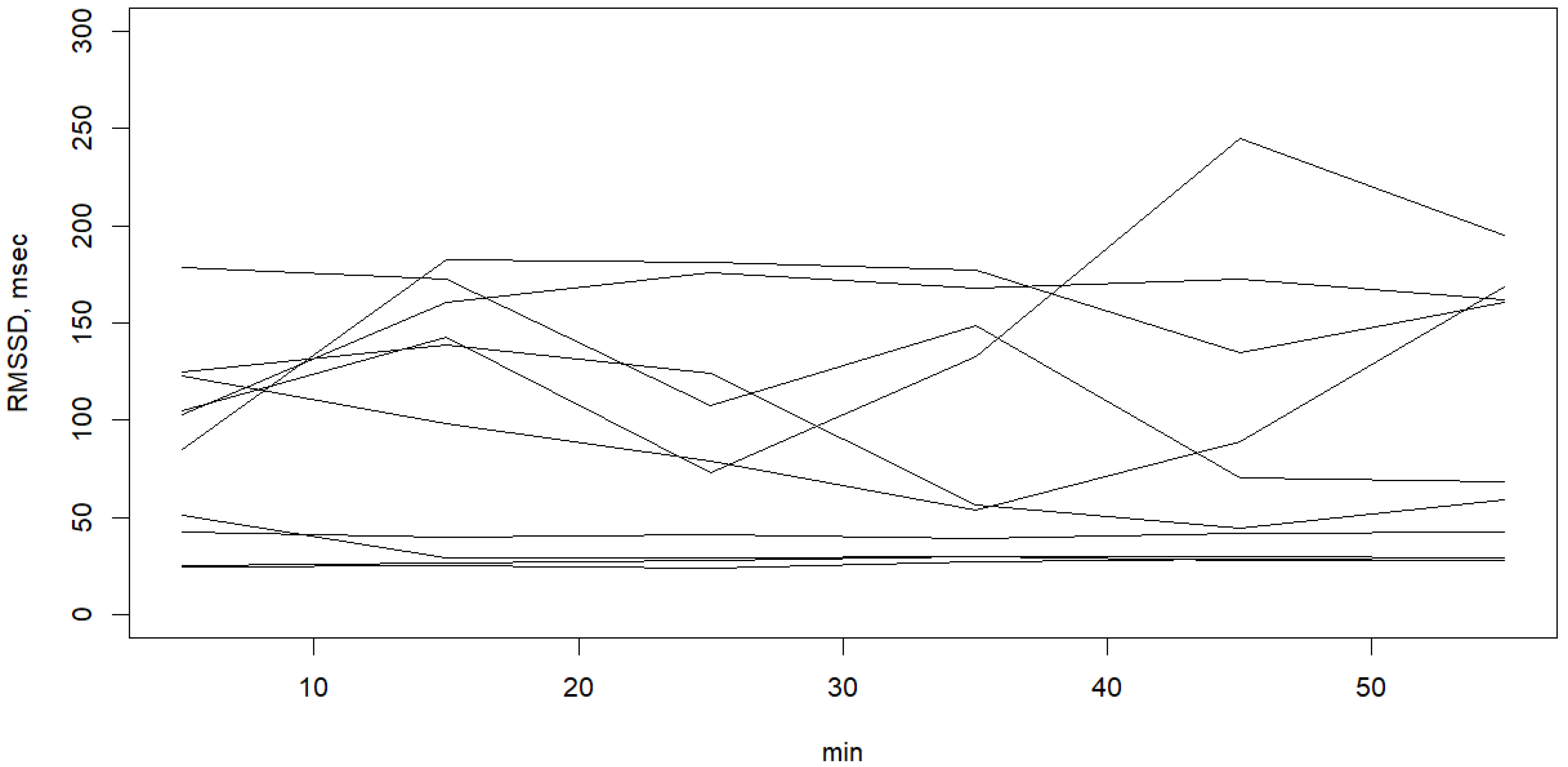
| RMSSD, msec | 62.17 ± 51.37 | 60.81 ± 49.84 | 67.48 ± 50.65 | 70.90 ± 52.53 | 71.73 ± 52.24 | 78.66 ± 58.20 | 80.41 ± 60.31 | 1 | 5.12 | 0.024 |
| Variables | Total | Increased Group | Decreased Group | t or W | df | p Value |
|---|---|---|---|---|---|---|
| N (female/male) | 45 (7/28) | 25 (3/22) | 20 (4/16) | 0.682 | ||
| AHI | 0.359 | |||||
| Mild–moderate, 5 < AHI ≤ 30 | 27 (60%) | 13 (52%) | 14 (70%) | |||
| Severe, AHI > 30 | 18 (40%) | 12 (48%) | 6 (30%) | |||
| Center of pre-S episode, min | 7.5 (2.5, 15.0) | 15 (2.5, 25) | 7.5 (2.5, 7.5) | 186.5 | 0.134 | |
| Center of S episode, min | 15.0 (7.5, 25.0) | 25.0 (7.5, 35.0) | 15.0 (7.5, 15.0) | 197 | 0.216 | |
| t | −11.95 | −6.69 | ||||
| df | 24 | 19 | ||||
| p value | <0.001 | <0.001 | ||||
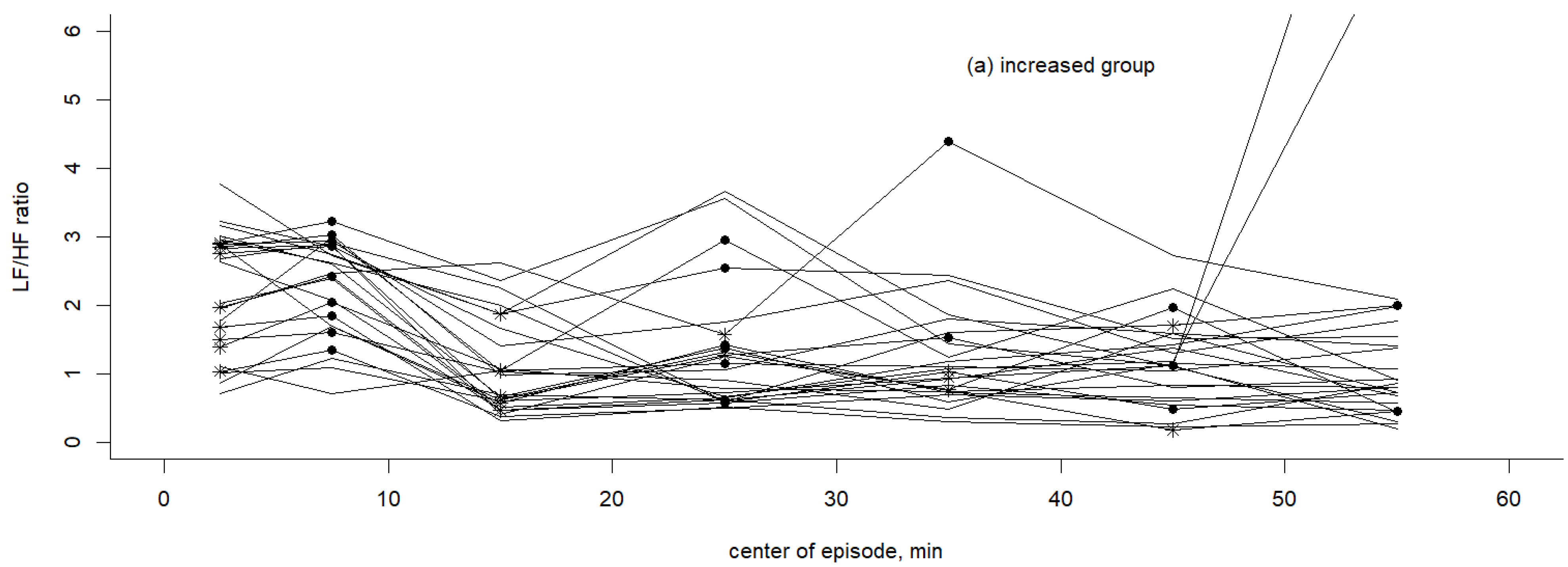
| Pre-S episode LF/HF ratio | 1.8 ± 1.0 | 1.4 ± 0.8 | 2.4 ± 1.0 | 3.656 | 43 | 0.001 |
| S episode LF/HF ratio | 1.8 ± 1.0 | 2.0 ± 1.0 | 1.5 ± 0.9 | −1.68 | 43 | 0.100 |
| t | −4.45 | 5.53 | ||||
| df | 24 | 19 | ||||
| p value | <0.001 | <0.001 |
| O.R. | Estimate | S.E. | z | p | |
|---|---|---|---|---|---|
| Snoring after lying down more than 20 min | 10.9 | 2.39 | 0.82 | 2.90 | 0.004 |
| Severe OSA | 5.01 | 1.61 | 0.80 | 2.01 | 0.045 |
| Intercept | −1.35 | 0.65 | −2.1 | 0.037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, J.-K.; Lin, Y.-C.; Kao, Y.-H. Oscillation of Sympathetic Activity in Patients with Obstructive Sleep Apnea during the First Hour of Sleep. Healthcare 2023, 11, 2701. https://doi.org/10.3390/healthcare11192701
Chiang J-K, Lin Y-C, Kao Y-H. Oscillation of Sympathetic Activity in Patients with Obstructive Sleep Apnea during the First Hour of Sleep. Healthcare. 2023; 11(19):2701. https://doi.org/10.3390/healthcare11192701
Chicago/Turabian StyleChiang, Jui-Kun, Yen-Chang Lin, and Yee-Hsin Kao. 2023. "Oscillation of Sympathetic Activity in Patients with Obstructive Sleep Apnea during the First Hour of Sleep" Healthcare 11, no. 19: 2701. https://doi.org/10.3390/healthcare11192701
APA StyleChiang, J.-K., Lin, Y.-C., & Kao, Y.-H. (2023). Oscillation of Sympathetic Activity in Patients with Obstructive Sleep Apnea during the First Hour of Sleep. Healthcare, 11(19), 2701. https://doi.org/10.3390/healthcare11192701