

Validation of the Romanian Version of the Halitosis Associated Life-Quality Test (HALT) in a Cross-Sectional Study among Young Adults




 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. HALT Overview
2.2. Study Design and Ethics
2.3. Creating the Romanian Version of the HALT (R-HALT)
2.4. Assessment of Psychometric Properties
2.5. Statistical Analysis
3. Results
3.1. Background Data
3.2. Reliability of HALT Results
3.3. Analysis of Results
4. Discussion
4.1. Literature Analysis
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zalewska, A.; Zatoński, M.; Jabłonka-Strom, A.; Paradowska, A.; Kawala, B.; Litwin, A. Halitosis—A common medical and social problem. A review on pathology, diagnosis and treatment. Acta Gastroenterol. Belg. 2012, 75, 300–309. [Google Scholar]
- Bicak, D.A. A Current Approach to Halitosis and Oral Malodor—A Mini Review. Open Dent. J. 2018, 12, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Aylıkcı, B.U.; Colak, H. Halitosis: From diagnosis to management. J. Nat. Sci. Biol. Med. 2013, 4, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, U.; Sharma, G.; Juneja, M.; Nagpal, A. Halitosis: Current concepts on etiology, diagnosis and management. Eur. J. Dent. 2016, 10, 292–300. [Google Scholar] [CrossRef]
- Moreno, L.B.; Colussi, P.R.G.; Marostega, M.G.; Rosalen, N.P.; Rösing, C.K.; Muniz, F.W.M.G. Self-reported halitosis and associated factors among older adults: A cross-sectional study. J. Oral Biol. Craniofac. Res. 2022, 12, 431–436. [Google Scholar] [CrossRef]
- Briceag, R.; Caraiane, A.; Raftu, G.; Horhat, R.M.; Bogdan, I.; Fericean, R.M.; Shaaban, L.; Popa, M.; Bumbu, B.A.; Bratu, M.L.; et al. Emotional and Social Impact of Halitosis on Adolescents and Young Adults: A Systematic Review. Medicina 2023, 59, 564. [Google Scholar] [CrossRef]
- Olszewska-Czyz, I.; Sozkes, S.; Dudzik, A. Clinical Trial Evaluating Quality of Life in Patients with Intra-Oral Halitosis. J. Clin. Med. 2022, 11, 326. [Google Scholar] [CrossRef]
- Vali, A.; Roohafza, H.; Keshteli, A.H.; Afghari, P.; Javad Shirani, M.; Afshar, H.; Savabi, O.; Adibi, P. Relationship between subjective halitosis and psychological factors. Int. Dent. J. 2015, 65, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Zini, A.; Levine, J.; Weiss, M.; Lev, R.; Chebath Taub, D.; Hai, A.; Almoznino, G. Demographic profile, Oral Health Impact Profile and Dental Anxiety Scale in patients with chronic periodontitis: A case-control study. Int. Dent. J. 2018, 68, 269–278. [Google Scholar] [CrossRef]
- Buj-Acosta, C.; García-Sanz, V.; Bellot-Arcis, C.; Paredes-Gallardo, V.; Tarazona-Álvarez, B.; Tortajada-Girbés, M.; Montiel-Company, J. Prevalence of Halitosis in Children and Associated Factors: A Systematic Review and Meta-Analysis. Lancet 2023, preprint. [Google Scholar] [CrossRef]
- Bollen, C.M.; Beikler, T. Halitosis: The multidisciplinary approach. Int. J. Oral Sci. 2012, 4, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Dudzik, A.; Chomyszyn-Gajewska, M.; Łazarz-Bartyzel, K. An Evaluation of Halitosis using Oral Chroma™ Data Manager, Organoleptic Scores and Patients’ Subjective Opinions. J. Int. Oral Health. 2015, 7, 6–11. [Google Scholar] [PubMed]
- Tudoroniu, C.; Popa, M.; Iacob, S.M.; Pop, A.L.; Năsui, B.A. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6923. [Google Scholar] [CrossRef]
- Saveanu, C.I.; Cretu, C.C.; Bamboi, I.; Săveanu, A.E.; Anistoroaei, D. Title Cross-Sectional Study to Evaluate Knowledge and Attitudes on Oral Hygiene of Romanian Students. Medicina 2022, 58, 406. [Google Scholar] [CrossRef]
- Zanetti, F.; Zivkovic Semren, T.; Battey, J.N.D.; Guy, P.A.; Ivanov, N.V.; van der Plas, A.; Hoeng, J. A Literature Review and Framework Proposal for Halitosis Assessment in Cigarette Smokers and Alternative Nicotine-Delivery Products Users. Front Oral Health. 2021, 2, 777442. [Google Scholar] [CrossRef]
- He, S.L.; Wang, J.H.; Wang, M.H.; Deng, Y.M. Validation of the Chinese version of the Halitosis Associated Life-quality Test (HALT) questionnaire. Oral Dis. 2012, 18, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Iosif, L.; Preoteasa, C.T.; Preoteasa, E.; Ispas, A.; Ilinca, R.; Murariu-Mǎgureanu, C.; Amza, O.E. Oral Health Related Quality of Life and Prosthetic Status among Institutionalized Elderly from the Bucharest Area: A Pilot Study. Int. J. Environ. Res. Public. Health 2021, 18, 6663. [Google Scholar] [CrossRef]
- Teodorescu, I.M.; Preoteasa, E.; Preoteasa, C.T.; Murariu-Măgureanu, C.; Teodorescu, C. The perceived association of oral diseases and general pathology among doctors of different specialties. J. Med. Life. 2022, 15, 1052–1057. [Google Scholar] [CrossRef]
- Kizhner, V.; Xu, D.; Krespi, Y.P. A new tool measuring oral malodor quality of life. Eur. Arch. Otorhinolaryngol. 2011, 268, 1227–1232. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11 (Suppl. S1), S80–S89. [Google Scholar] [CrossRef]
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Greenman, J.; Duffield, J.; Spencer, P.; Rosenberg, M.; Corry, D.; Saad, S.; Lenton, P.; Majerus, G.; Nachnani, S.; El-Maaytah, M. Study on the organoleptic intensity scale for measuring oral malodor. J. Dent. Res. 2004, 83, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Silveira, J.O.D.; Cota, L.O.M.; Bendo, C.B.; Faria, S.F.S.; Costa, F.O. Validation of the Brazilian version of the Halitosis Associated Life-Quality Test (HALT). Braz. Oral Res. 2020, 34, e098. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.R.; Gonthier, C.; Barch, D.M.; Braver, T.S. The Role of Psychometrics in Individual Differences Research in Cognition: A Case Study of the AX-CPT. Front. Psychol. 2017, 8, 1482. [Google Scholar] [CrossRef] [PubMed]
- Bin Mubayrik, A.; Al Hamdan, R.; Al Hadlaq, E.M.; AlBagieh, H.; AlAhmed, D.; Jaddoh, H.; Demyati, M.; Abu Shryei, R. Self-perception, knowledge, and awareness of halitosis among female university students. Clin. Cosmet. Investig. Dent. 2017, 9, 45–52. [Google Scholar] [CrossRef]
- Mento, C.; Lombardo, C.; Milazzo, M.; Whithorn, N.I.; Boronat-Catalá, M.; Almiñana-Pastor, P.J.; Fernàndez, C.S.; Bruno, A.; Muscatello, M.R.A.; Zoccali, R.A. Adolescence, Adulthood and Self-Perceived Halitosis: A Role of Psychological Factors. Medicina 2021, 57, 614. [Google Scholar] [CrossRef]
- Setia, S.; Pannu, P.; Gambhir, R.S.; Galhotra, V.; Ahluwalia, P.; Sofat, A. Correlation of oral hygiene practices, smoking and oral health conditions with self perceived halitosis amongst undergraduate dental students. J. Nat. Sci. Biol. Med. 2014, 5, 67–72. [Google Scholar] [CrossRef]
- Suzuki, N.; Yoneda, M.; Naito, T.; Iwamoto, T.; Yamada, K.; Hisama, K.; Okada, I.; Hirofuji, T. The relationship between alcohol consumption and oral malodour. Int. Dent. J. 2009, 59, 31–34. [Google Scholar]
- Shon, H.S.; Kim, K.O.; Jung, J.K.; Cha, E.J.; Lee, S.O.; Kim, K.A. Intra-Oral Factors Influencing Halitosis in Young Women. Osong Public Health Res. Perspect. 2018, 9, 340–347. [Google Scholar] [CrossRef]
- Ogunbodede, E.O.; Kida, I.A.; Madjapa, H.S.; Amedari, M.; Ehizele, A.; Mutave, R.; Sodipo, B.; Temilola, S.; Okoye, L. Oral Health Inequalities between Rural and Urban Populations of the African and Middle East Region. Adv. Dent. Res. 2015, 27, 18–25. [Google Scholar] [CrossRef]
- Deshpande, N.C.; Amrutiya, M.R. Obesity and oral health—Is there a link? An observational study. J. Indian Soc. Periodontol. 2017, 21, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Aydin, M. Criticism of the organoleptic examination for the diagnosis of oral halitosis. J. Breath. Res. 2022, 17, 014001. [Google Scholar] [CrossRef]
- McKeown, L. Social relations and breath odour. Int. J. Dent. Hyg. 2003, 1, 213–217. [Google Scholar] [CrossRef]
- Quirynen, M.; Dadamio, J.; Van den Velde, S.; De Smit, M.; Dekeyser, C.; Van Tornout, M.; Vandekerckhove, B. Characteristics of 2000 patients who visited a halitosis clinic. J. Clin. Periodontol. 2009, 36, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.M.; Kislig, K.; Hoti, B.B.; Seemann, R.; Lussi, A. Prevalence of halitosis in the population of the city of Bern, Switzerland: A study comparing self-reported and clinical data. Eur. J. Oral Sci. 2009, 117, 261–267. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Number | % |
|---|---|---|
| Age (mean ± SD) | 23.6 ± 1.8 | – |
| Age range | ||
| 16–18 years | 12 | 8% |
| 18–20 years | 37 | 25% |
| 20–22 years | 52 | 35% |
| 22–24 years | 33 | 22% |
| 24–26 years | 16 | 10% |
| Gender | ||
| Male | 77 | 51% |
| Female | 73 | 49% |
| Area of residence | ||
| Urban | 112 | 75% |
| Rural | 38 | 25% |
| BMI | ||
| Overweight | 44 | 29% |
| Obese | 22 | 15% |
| Normal | 84 | 56% |
| Smoking (yes, %) | 29 | 19% |
| Alcohol consumption (yes, %) | 78 | 52% |
| Self-reported halitosis (yes, %) | 31 | 21% |
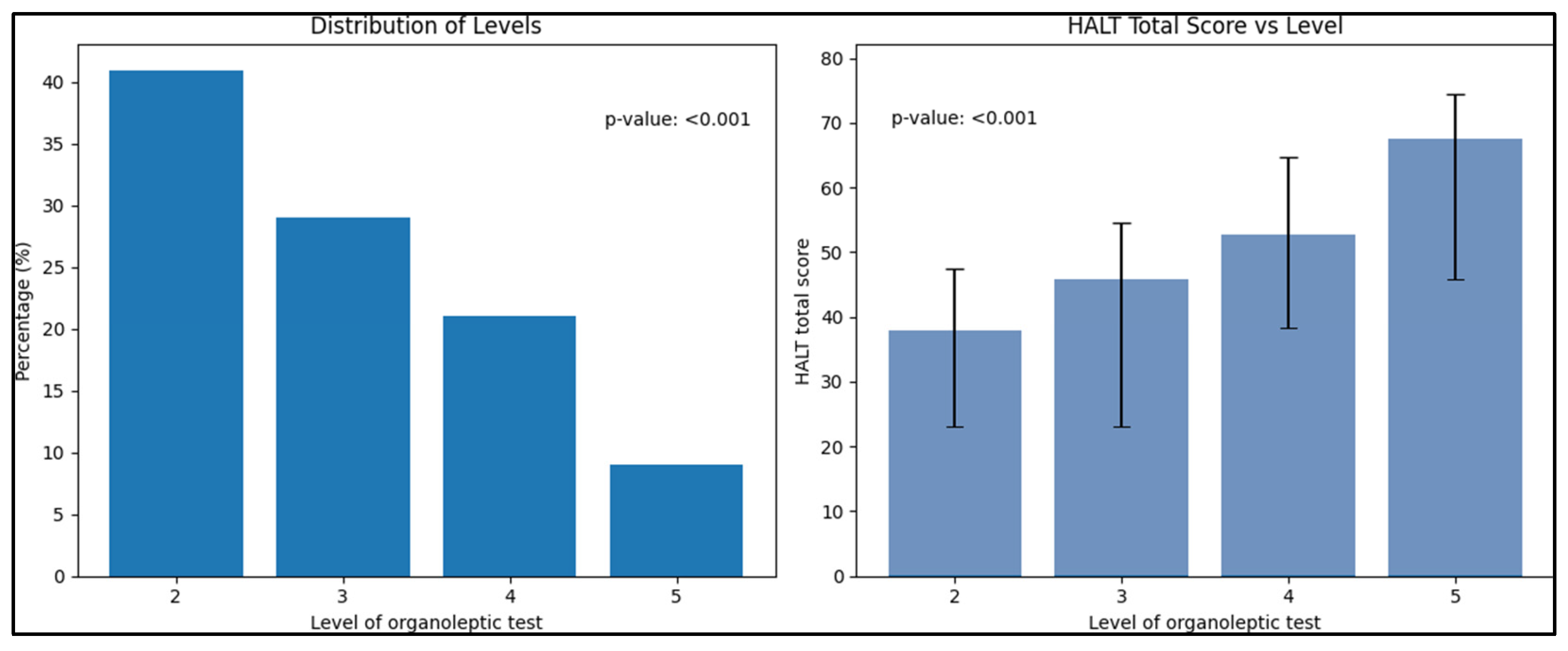
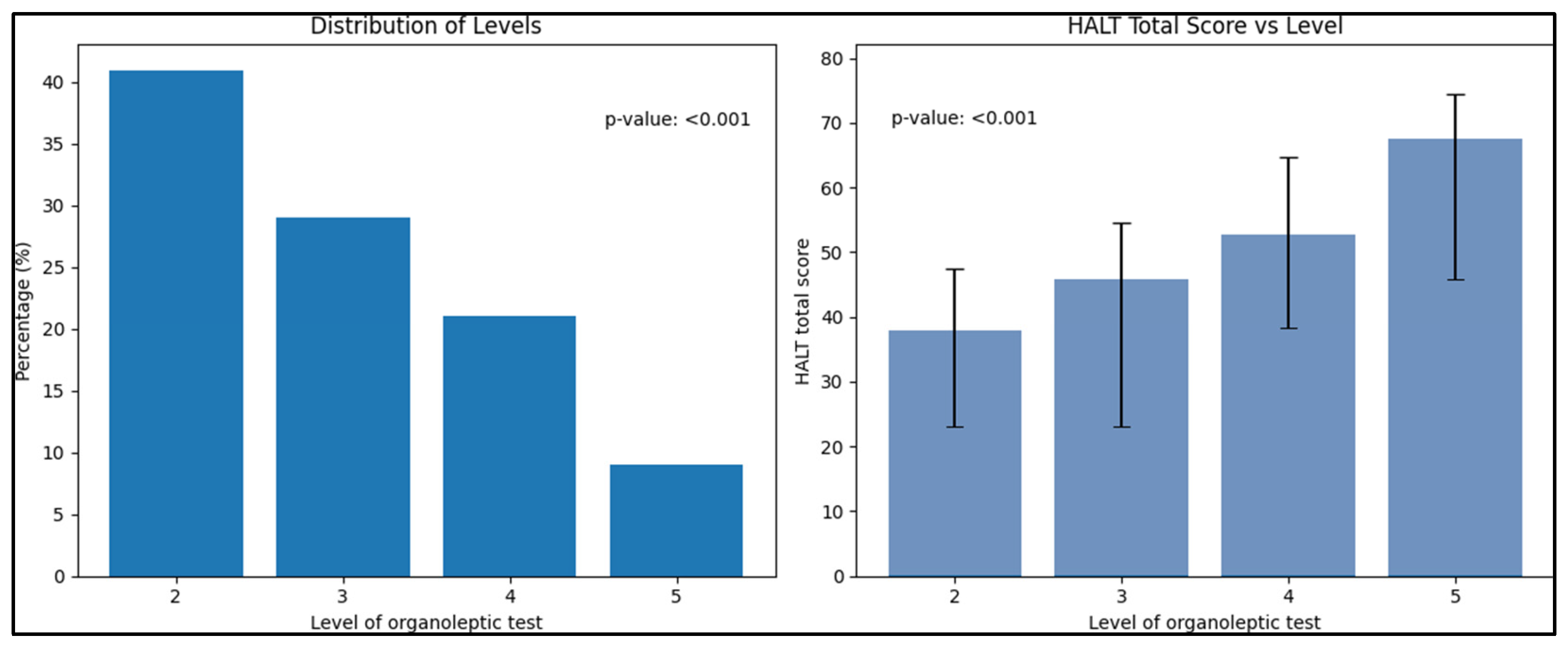
| Organoleptic test score | ||
| 2 | 62 | 41% |
| 3 | 44 | 29% |
| 4 | 31 | 21% |
| 5 | 13 | 9% |
| Item | Mean ± SD | Corrected Item– Total Correlation | Cronbach’s Alpha If Item Deleted |
|---|---|---|---|
| Q1 | 2.00 ± 1.10 | 0.49 | 0.95 |
| Q2 | 1.05 ± 0.83 | 0.30 | 0.94 |
| Q3 | 0.82 ± 0.94 | 0.42 | 0.94 |
| Q4 | 3.10 ± 1.25 | 0.67 | 0.94 |
| Q5 | 3.15 ± 1.18 | 0.71 | 0.95 |
| Q6 | 2.35 ± 0.95 | 0.70 | 0.95 |
| Q7 | 1.58 ± 0.92 | 0.75 | 0.93 |
| Q8 | 2.45 ± 0.85 | 0.52 | 0.93 |
| Q9 | 1.38 ± 0.79 | 0.60 | 0.93 |
| Q10 | 3.18 ± 1.20 | 0.69 | 0.93 |
| Q11 | 3.23 ± 1.15 | 0.74 | 0.94 |
| Q12 | 2.92 ± 0.92 | 0.82 | 0.95 |
| Q13 | 2.95 ± 1.00 | 0.77 | 0.95 |
| Q14 | 3.07 ± 1.05 | 0.80 | 0.96 |
| Q15 | 2.05 ± 0.75 | 0.83 | 0.94 |
| Q16 | 2.75 ± 1.08 | 0.85 | 0.94 |
| Q17 | 2.43 ± 0.90 | 0.71 | 0.94 |
| Q18 | 2.78 ± 0.88 | 0.59 | 0.94 |
| Q19 | 3.12 ± 0.70 | 0.90 | 0.94 |
| Q20 | 3.22 ± 0.72 | 0.82 | 0.93 |
| Item | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| Q1 | 0.91 | 0.33 | 0.06 | 0.5 |
| Q2 | 0.88 | 0.32 | 0.25 | 0.19 |
| Q3 | 0.81 | 0.41 | 0.23 | 0.30 |
| Q4 | 0.80 | 0.44 | 0.11 | 0.23 |
| Q5 | 0.78 | 0.21 | 0.40 | 0.21 |
| Q6 | 0.76 | 0.09 | 0.48 | 0.16 |
| Q7 | 0.63 | 0.57 | 0.10 | 0.36 |
| Q8 | 0.15 | 0.93 | 0.17 | 0.09 |
| Q9 | 0.24 | 0.92 | 0.08 | 0.12 |
| Q10 | 0.23 | 0.9 | 0.18 | 0.10 |
| Q11 | 0.29 | 0.88 | 0.17 | −0.14 |
| Q12 | 0.31 | 0.58 | 0.53 | 0.27 |
| Q13 | 0.05 | 0.11 | 0.82 | 0.23 |
| Q14 | 0.34 | 0.45 | 0.73 | −0.08 |
| Q15 | 0.23 | 0.34 | 0.65 | 0.33 |
| Q16 | 0.33 | 0.03 | 0.68 | 0.44 |
| Q17 | 0.38 | 0.33 | 0.52 | 0.42 |
| Q18 | −0.10 | 0.02 | 0.31 | 0.85 |
| Q19 | 0.51 | −0.08 | −0.06 | 0.69 |
| Q20 | 0.18 | −0.02 | 0.40 | 0.76 |
| Eigenvalue | 5.40 | 5.11 | 3.55 | 2.89 |
| Percent variance | 27.2% | 25.5% | 17.8% | 14.0% |
| Variable | n (%) | HALT Total Score (Mean ± SD) | p-Value |
|---|---|---|---|
| Level of organoleptic test | <0.001 | ||
| 2 | 62 (41%) | 38.0 ± 9.4 | |
| 3 | 44 (29%) | 45.9 ± 11.8 | |
| 4 | 31 (21%) | 52.7 ± 12.0 | |
| 5 | 13 (9%) | 67.5 ± 10.7 | |
| Self-reported halitosis | <0.001 | ||
| Yes | 31 (21%) | 58.4 ± 10.3 | |
| No | 119 (79%) | 50.1 ± 1.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briceag, R.; Caraiane, A.; Raftu, G.; Bratu, M.L.; Buzatu, R.; Dehelean, L.; Bondrescu, M.; Bratosin, F.; Bumbu, B.A. Validation of the Romanian Version of the Halitosis Associated Life-Quality Test (HALT) in a Cross-Sectional Study among Young Adults. Healthcare 2023, 11, 2660. https://doi.org/10.3390/healthcare11192660
Briceag R, Caraiane A, Raftu G, Bratu ML, Buzatu R, Dehelean L, Bondrescu M, Bratosin F, Bumbu BA. Validation of the Romanian Version of the Halitosis Associated Life-Quality Test (HALT) in a Cross-Sectional Study among Young Adults. Healthcare. 2023; 11(19):2660. https://doi.org/10.3390/healthcare11192660
Chicago/Turabian StyleBriceag, Raluca, Aureliana Caraiane, Gheorghe Raftu, Melania Lavinia Bratu, Roxana Buzatu, Liana Dehelean, Mariana Bondrescu, Felix Bratosin, and Bogdan Andrei Bumbu. 2023. "Validation of the Romanian Version of the Halitosis Associated Life-Quality Test (HALT) in a Cross-Sectional Study among Young Adults" Healthcare 11, no. 19: 2660. https://doi.org/10.3390/healthcare11192660
APA StyleBriceag, R., Caraiane, A., Raftu, G., Bratu, M. L., Buzatu, R., Dehelean, L., Bondrescu, M., Bratosin, F., & Bumbu, B. A. (2023). Validation of the Romanian Version of the Halitosis Associated Life-Quality Test (HALT) in a Cross-Sectional Study among Young Adults. Healthcare, 11(19), 2660. https://doi.org/10.3390/healthcare11192660