Parent-Reported Child and Parent Quality of Life during COVID-19 Testing at an Australian Paediatric Hospital Outpatient Clinic: A Cross-Sectional Study

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Methods
2.1. Study Setting
- (1)
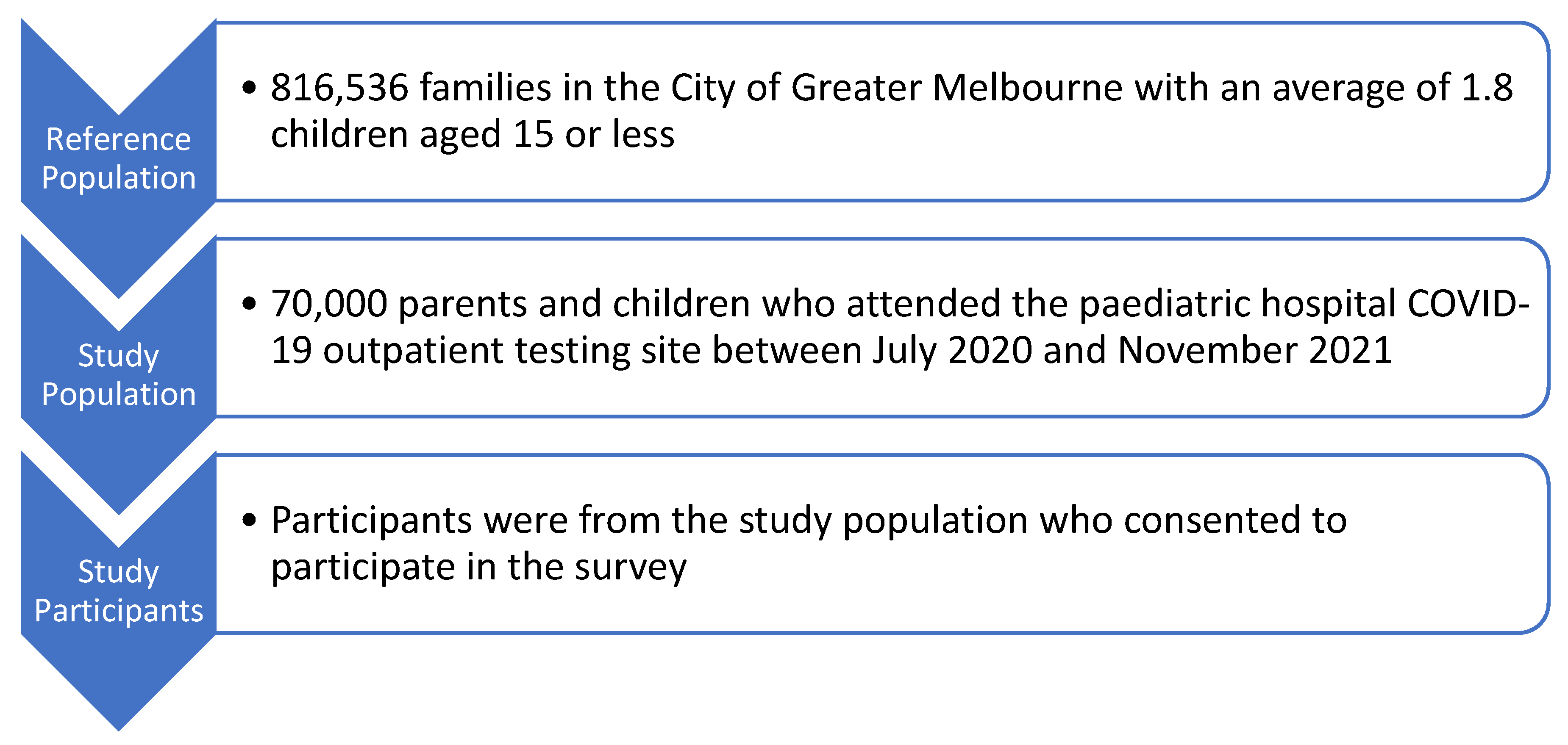
- This single-centre study was conducted at Victoria’s largest tertiary paediatric hospital, and this hospital was the only dedicated testing centre for children under five years of age in Victoria. As such, it captured the largest cohort of children under 5 years old in urban Melbourne and was also accessed by many regional families due to the anticipated distress of testing in young children;
- (2)
- We acknowledge that this study is not representative of children and families across Australia, and this was not the intention. Each state and territory in Australia experienced differing levels of COVID-19 waves of infection and subsequent public health restrictions. These results are specific to children and families in metropolitan Melbourne, Victoria, who visited the paediatric hospital outpatient clinic for COVID-19 testing and experienced the most stringent and long-lasting lockdowns in Australia. The experience of children and families would almost certainly have been different in the other Australian states, especially Western Australia, where no lockdowns were applied. These data are representative of populations undergoing harsh pandemic restrictions and the potential impact on QOL and wellbeing;
- (3)
- Our data have been time-stamped to allow comparison between periods of home and on-site schooling, which has generated intense debate in the media and between political parties in Australia and globally and, as such, will be of broad interest.
2.2. Study Design
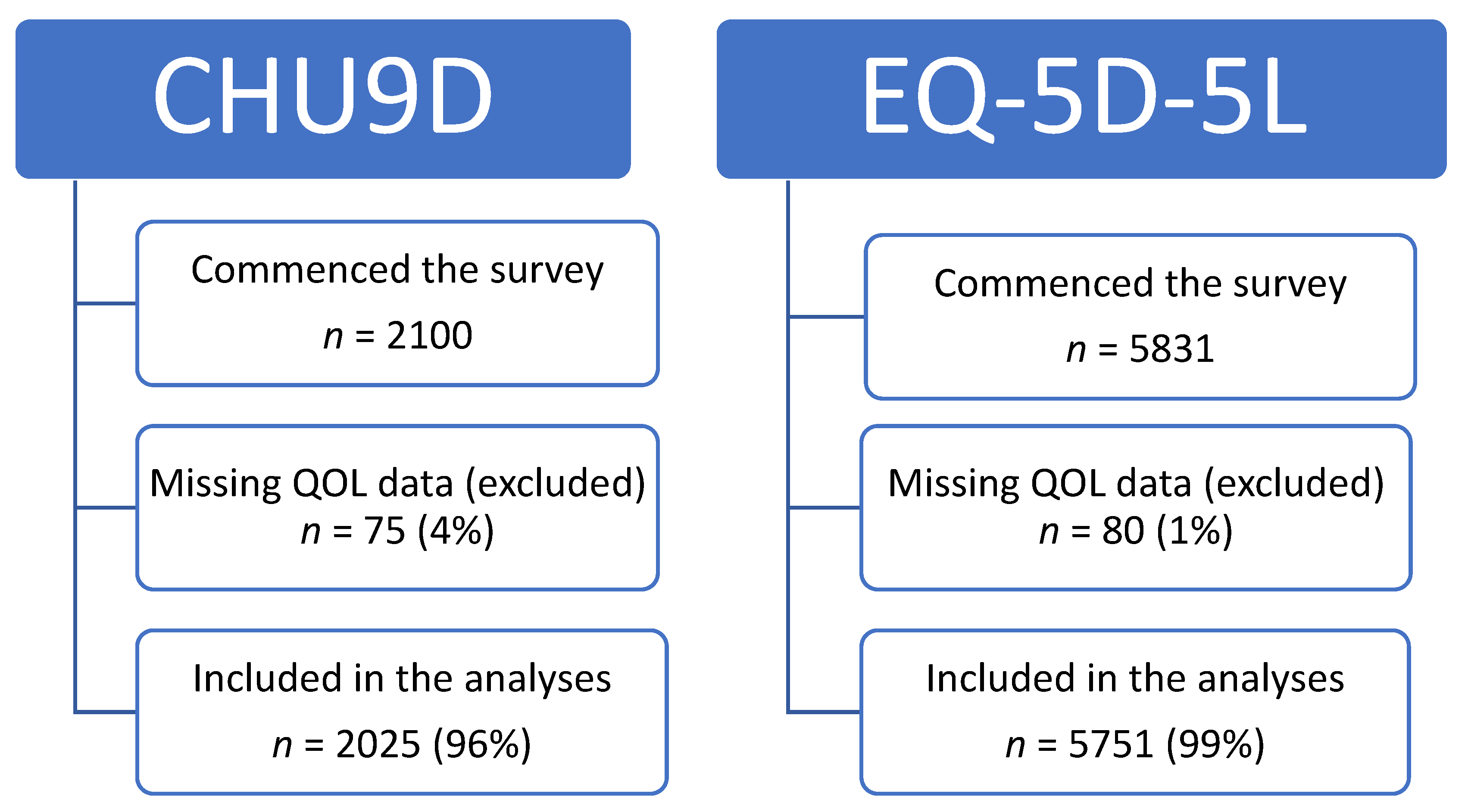
2.3. Participants and Consent
2.4. Data Collection
2.5. Outcome Measures
2.6. Data Coding
2.7. Analysis
3. Results
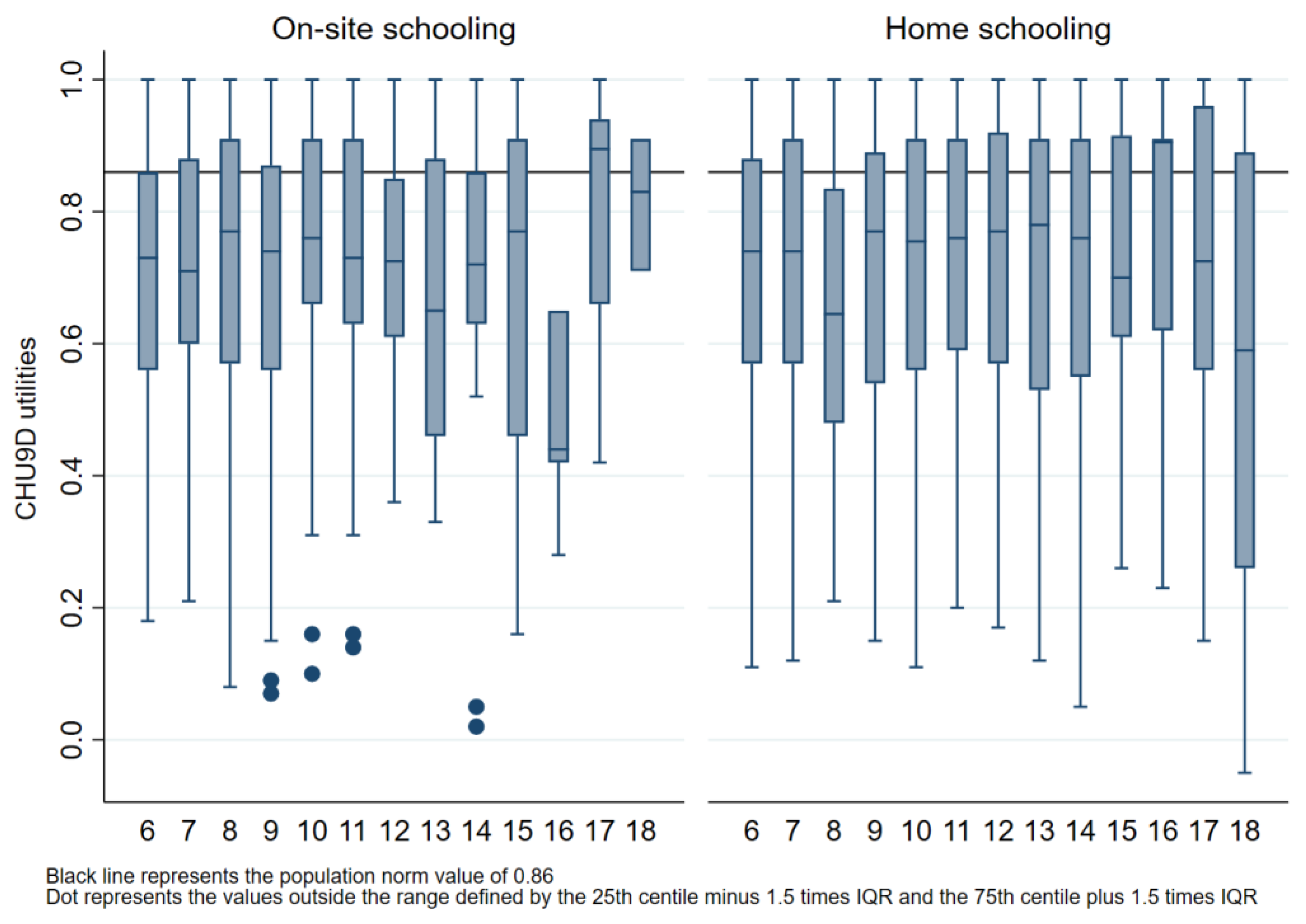
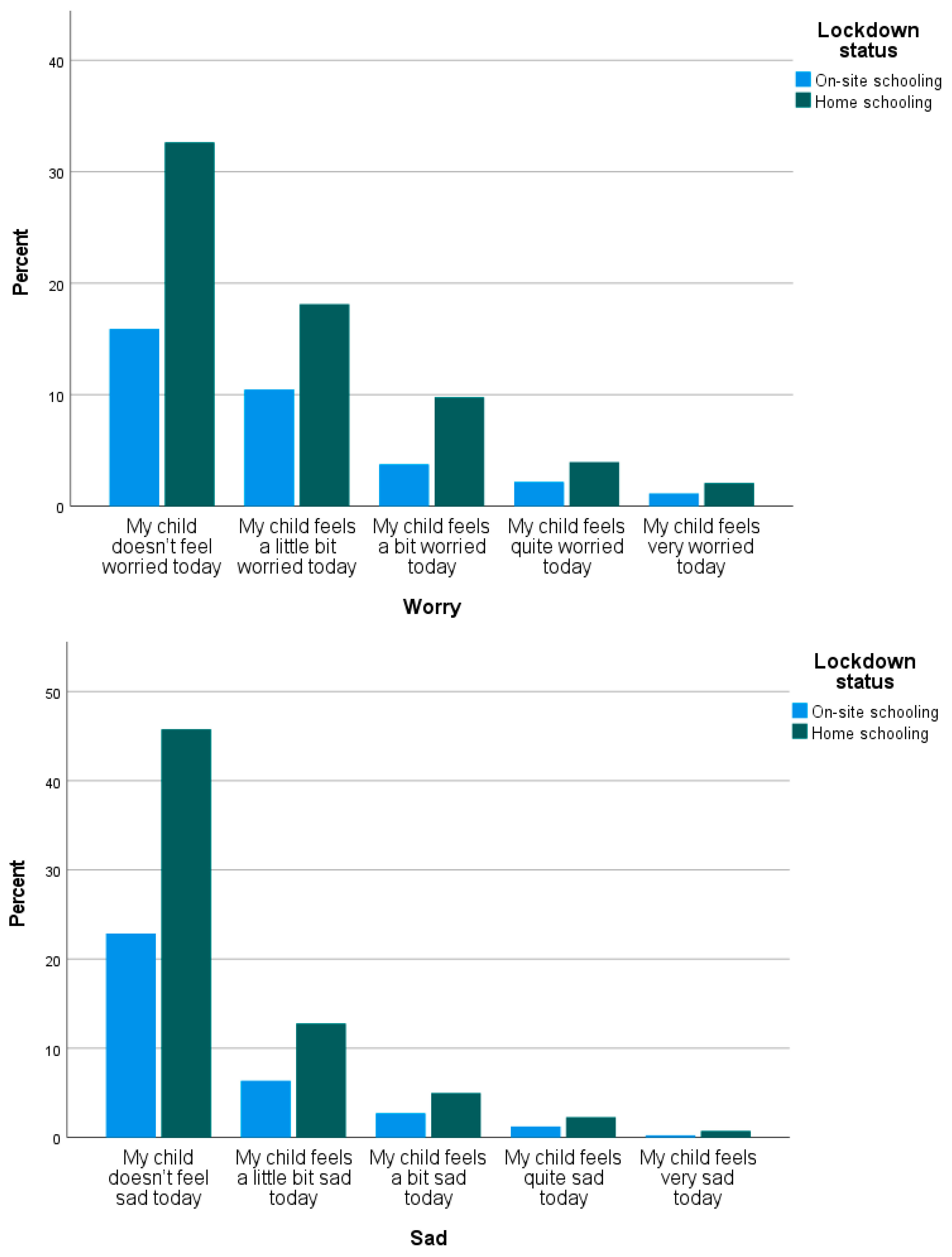
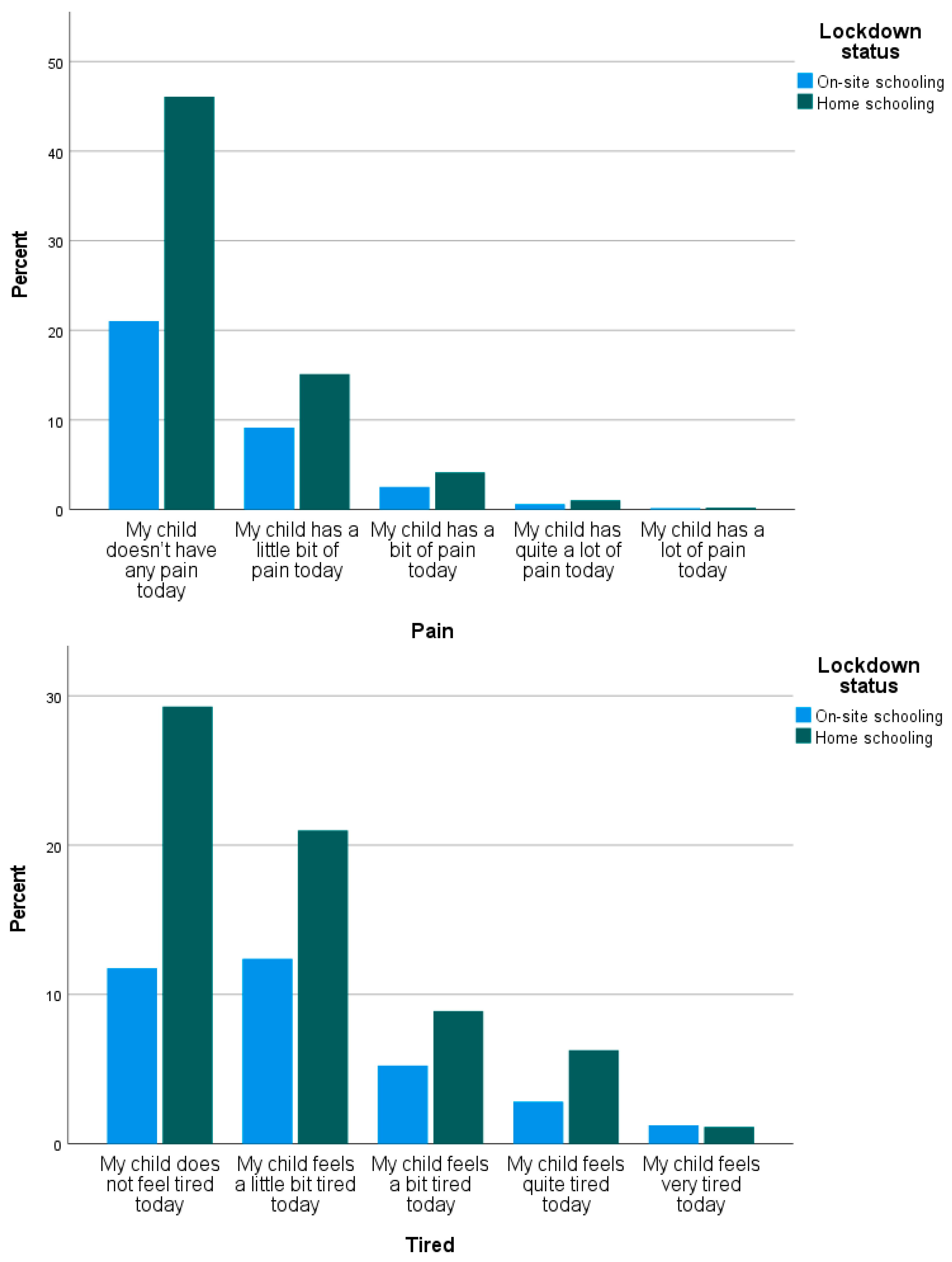
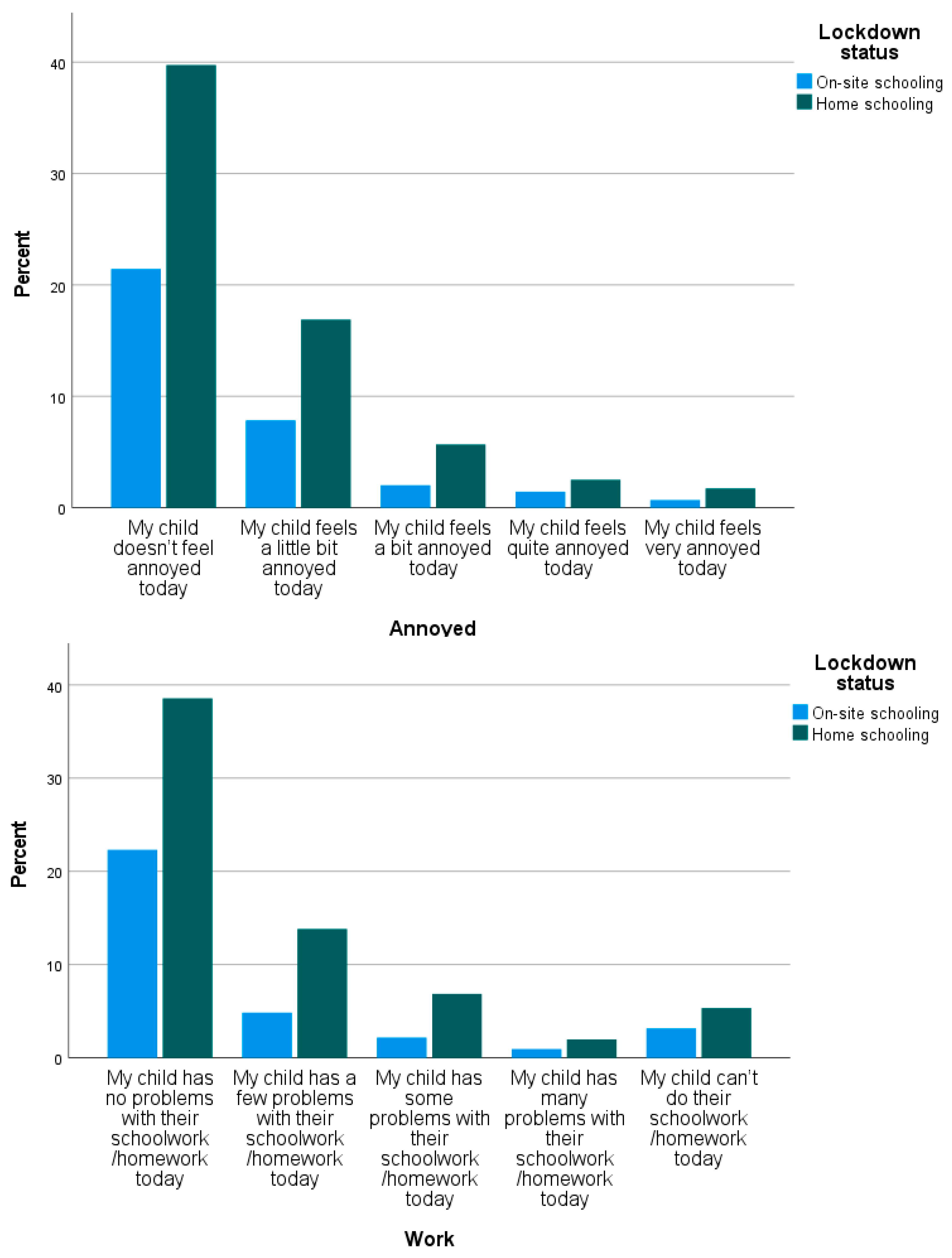
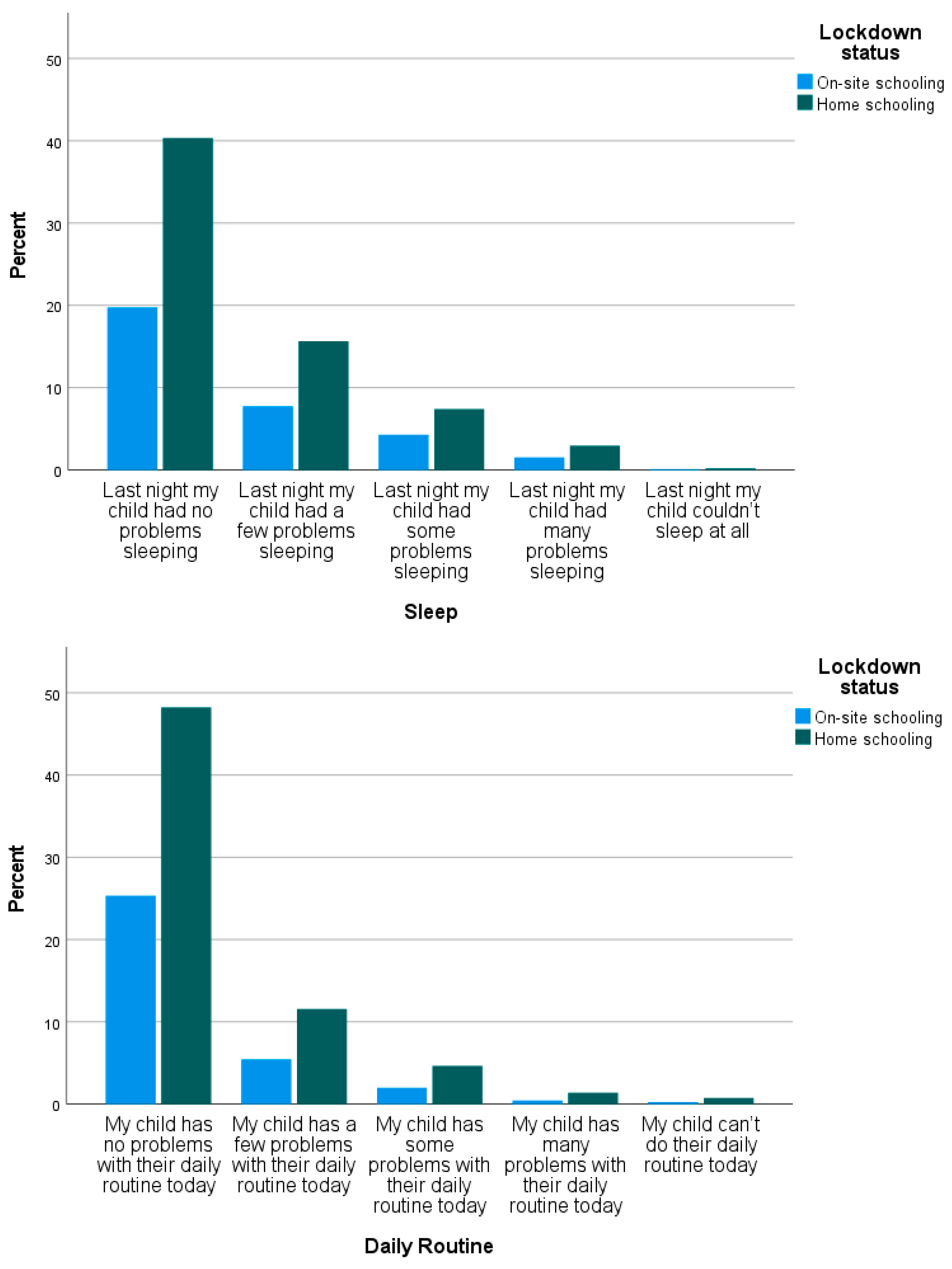
3.1. CHU9D
3.2. CHU9D Presented as Parametric Data to Enable Comparison with the Literature
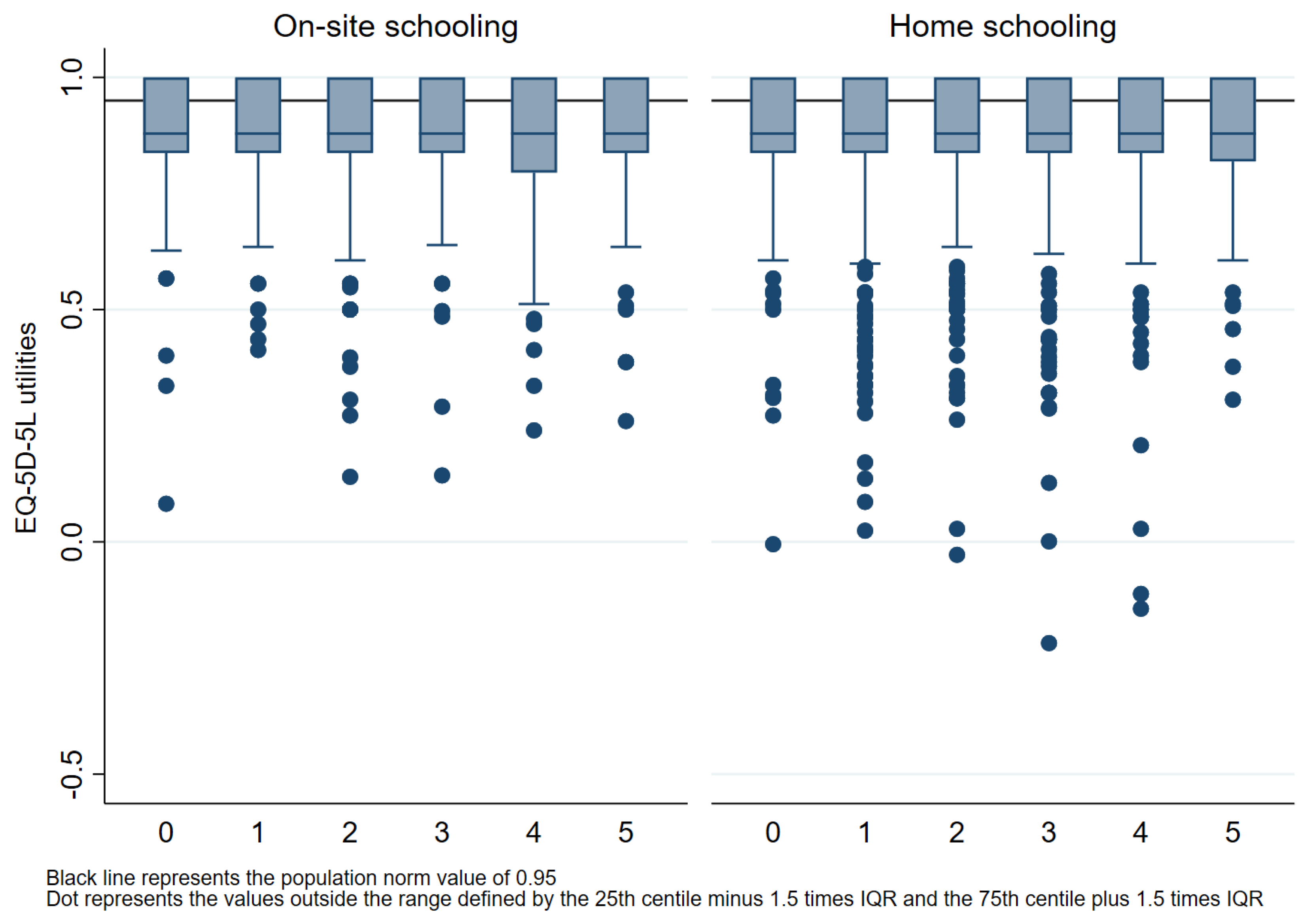
3.3. EQ-5D-5L
3.4. EQ-5D-5L Presented as Parametric Data to Enable Comparison with the Literature
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| On-Site Schooling (n = 677) | Home Schooling (n = 1348) | Mean Difference * On-Site Minus Home Schooling | |
|---|---|---|---|
| CHU9D Utility Index | 0.710 (SD 0.215) | 0.710 (SD 0.222) | −0.0003 (95% CI −0.021 to 0.020), p = 0.981 |
| CHU9D Worry Domain | 1.869 (SD 1.067) | 1.869 (SD 1.067) | 0.000 (95% CI −0.099 to 0.098), p = 0.998 |
| CHU9D Sad Domain | 1.493 (SD 0.851) | 1.489 (SD 0.859) | 0.004 (95% CI −0.075 to 0.084), p = 0.912 |
| CHU9D Pain Domain | 1.495 (SD 0.749) | 1.410 (SD 0.704) | 0.085 (95% CI 0.018 to 0.151), p = 0.013 |
| CHU9D Tired Domain | 2.084 (SD 1.083) | 1.933 (SD 1.049) | 0.151 (95% CI 0.053 to 0.249), p = 0.003 |
| CHU9D Annoyed Domain | 1.567 (SD 0.934) | 1.642 (SD 0.969) | −0.074 (95% CI −0.163 to 0.014), p = 0.099 |
| CHU9D Work Domain | 1.737 (SD 1.276) | 1.823 (SD 1.222) | −0.086 (95% CI −0.201 to 0.028), p = 0.139 |
| CHU9D Sleep Domain | 1.638 (SD 0.894) | 1.603 (SD 0.875) | 0.035 (95% CI −0.046 to 0.116), p = 0.399 |
| CHU9D Daily Domain | 1.350 (SD 0.718) | 1.420 (SD 0.801) | −0.070 (95% CI −0.141 to 0.002), p = 0.056 |
| CHU9D Activity Domain | 2.2902 (SD 1.467) | 2.116 (SD 1.401) | 0.173 (95% CI 0.042 to 0.305), p = 0.010 |



| On-Site Schooling (n = 1705) | Home Schooling (n = 4046) | Mean Difference * On-Site Minus Home Schooling | |
|---|---|---|---|
| EQ-5D-5L Utility Index | 0.887 (SD 0.124) | 0.880 (SD 0.134) | 0.007 (95% CI −0.0004 to 0.014), p = 0.065 |
| EQ-5D-5L Mobility Domain | 1.042 (SD 0.271) | 1.043 (SD 0.274) | −0.001 (95% CI −0.016 to 0.015), p = 0.946 |
| EQ-5D-5L Usual Care Domain | 1.023 (SD 0.204) | 1.039 (SD 0.319) | −0.016 (95% CI −0.032 to 0.001), p = 0.058 |
| EQ-5D-5L Activity Domain | 1.248 (SD 0.688) | 1.230 (SD 0.626) | 0.017 (95% CI −0.019 to 0.054), p = 0.350 |
| EQ-5D-5L Pain Domain | 1.282 (SD 0.536) | 1.294 (SD 0.563) | −0.013 (95% CI −0.044 to 0.019), p = 0.432 |
| EQ-5D-5L Anxiety Domain | 1.603 (SD 0.732) | 1.668 (SD 0.781) | −0.065 (95% CI −0.108 to −0.021), p = 0.003 |
References
- Macreadie, I. Reflections from Melbourne, the World’s Most Locked-Down City, through the COVID-19 Pandemic and Beyond; The Australian Society for Microbiology Inc.: Melbourne, Australia, 2022; p. 3. [Google Scholar]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfeld, C.; Packer, J.; Hudson, L. Impacts of school closures on physical and mental health of children and young people: A systematic review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Otto, C.; Devine, J.; Löffler, C.; Hurrelmann, K.; Bullinger, M.; Barkmann, C.; Siegel, N.A.; et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: Results of a two-wave nationwide population-based study. Eur. Child Adolesc. Psychiatry 2021, 32, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Adıbelli, D.; Sümen, A. The effect of the coronavirus (COVID-19) pandemic on health-related quality of life in children. Child. Youth Serv. Rev. 2020, 119, 105595. [Google Scholar] [CrossRef] [PubMed]
- Geirdal, A.K.Ø.; Price, D.; Schoultz, M.; Thygesen, H.; Ruffolo, M.; Leung, J.; Bonsaksen, T. The significance of demographic variables on psychosocial health from the early stage and nine months after the COVID-19 pandemic outbreak. A Cross-National Study. Int. J. Environ. Res. Public Health 2021, 18, 4345. [Google Scholar] [CrossRef]
- Shamblaw, A.L.; Rumas, R.L.; Best, M.W. Coping during the COVID-19 pandemic: Relations with mental health and quality of life. Can. Psychol. Psychol. Can. 2021, 62, 92. [Google Scholar] [CrossRef]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A.; Gupte, N. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10, e01837. [Google Scholar] [CrossRef]
- Imran, N.; Zeshan, M.; Pervaiz, Z. Mental health considerations for children & adolescents in COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, S67. [Google Scholar]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.L.; Lapierre, N.; Ouellet, M.C. Impact of the COVID-19 pandemic on older adults: Rapid review. JMIR Aging 2021, 4, e26474. [Google Scholar] [CrossRef]
- Persson, U.; Olofsson, S.; Gu, N.Y.; Gong, C.L.; Jiao, X.; Hay, J.W. Quality of Life in the Swedish General Population During COVID-19-Based on pre-and post-pandemic outbreak measurement. Nord. J. Health Econ. 2021, 9, 56–73. [Google Scholar] [CrossRef]
- Schuster, N.A.; de Breij, S.; Schaap, L.A.; van Schoor, N.M.; Peters, M.J.; de Jongh, R.T.; Hoogendijk, E.O. Older adults report cancellation or avoidance of medical care during the COVID-19 pandemic: Results from the Longitudinal Aging Study Amsterdam. Eur. Geriatr. Med. 2021, 12, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Kasar, K.S.; Karaman, E. Life in lockdown: Social isolation, loneliness and quality of life in the elderly during the COVİD-19 pandemic: A scoping review. Geriatr. Nurs. 2021, 42, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.D.; Chen, G.; Mpundu-Kaambwa, C.; Stevens, K.; Brazier, J.; Ratcliffe, J. Measuring Health-Related Quality of Life in Adolescent Populations: An Empirical Comparison of the CHU9D and the PedsQL TM 4.0 Short Form 15. Patient-Patient-Centered Outcomes Res. 2018, 11, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Stobart, A.; Duckett, S. Australia’s Response to COVID-19. Health Econ. Policy Law 2022, 17, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Vonneilich, N.; Lüdecke, D.; Kofahl, C. The impact of care on family and health-related quality of life of parents with chronically ill and disabled children. Disabil. Rehabil. 2016, 38, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Thorell, L.B.; Skoglund, C.; de la Peña, A.G.; Baeyens, D.; Fuermaier, A.B.; Groom, M.J.; Mammarella, I.C.; Van der Oord, S.; van den Hoofdakker, B.J.; Luman, M.; et al. Parental experiences of homeschooling during the COVID-19 pandemic: Differences between seven European countries and between children with and without mental health conditions. Eur. Child Adolesc. Psychiatry 2021, 31, 649–661. [Google Scholar] [CrossRef]
- Victorian State Government (Department of Health). Pandemic Order Register. 2022. Available online: https://www.health.vic.gov.au/covid-19/coronavirus-covid-19 (accessed on 21 January 2022).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- EuroQOL. EQ-5D. 2020. Available online: https://euroqol.org/ (accessed on 30 June 2021).
- Stark, P.A.; Myles, P.S.; Burke, J.A. Development and Psychometric Evaluation of a Postoperative Quality of Recovery Score The QoR-15. J. Am. Soc. Anesthesiol. 2013, 118, 1332–1340. [Google Scholar] [CrossRef]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef]
- Norman, R.; Mulhern, B.; Lancsar, E.; Lorgelly, P.; Ratcliffe, J.; Street, D.; Viney, R. The Use of a Discrete Choice Experiment Including Both Duration and Dead for the Development of an EQ-5D-5L Value Set for Australia. PharmacoEconomics 2023, 41, 427–438. [Google Scholar] [CrossRef]
- McCaffrey, N.; Kaambwa, B.; Currow, D.C.; Ratcliffe, J. Health-related quality of life measured using the EQ-5D–5L: South Australian population norms. Health Qual. Life Outcomes 2016, 14, 133. [Google Scholar] [CrossRef]
- Ribeiro Santiago, P.H.; Haag, D.; Macedo, D.M.; Garvey, G.; Smith, M.; Canfell, K.; Hedges, J.; Jamieson, L. Psychometric properties of the EQ-5D-5L for aboriginal Australians: A multi-method study. Health Qual. Life Outcomes 2021, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.A.; Ahmad, H.; Chen, G.; van der Mei, I.; Taylor, B.V.; Claflin, S.; Henson, G.J.; Simpson-Yap, S.; Laslett, L.L.; Hawkes, K.; et al. Validation of the EQ-5D-5L and psychosocial bolt-ons in a large cohort of people living with multiple sclerosis in Australia. Qual. Life Res. 2023, 32, 553–568. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.-Y.; Cheok, T.S.; Samson, A.J.; Kaambwa, B.; Brown, B.; Wilson, C.; Kroon, H.M.; Jaarsma, R.L. A longitudinal validation of the EQ-5D-5L and EQ-VAS stand-alone component utilising the Oxford Hip Score in the Australian hip arthroplasty population. J. Patient-Rep. Outcomes 2022, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Orji, N.C.; Cox, I.A.; Jason, L.A.; Chen, G.; Zhao, T.; Rogerson, M.J.; Kelly, R.M.; Wills, K.; Hensher, M.; Palmer, A.J.; et al. Assessing health state utilities for people with myalgic encephalomyelitis/chronic fatigue syndrome in Australia using the EQ-5D-5L, AQoL-8D and EQ-5D-5L-psychosocial instruments. Qual. Life Res. 2023. [CrossRef]
- Cheng, Q.; Kularatna, S.; Lee, X.J.; Graves, N.; Pacella, R.E. Comparison of EQ-5D-5L and SPVU-5D for measuring quality of life in patients with venous leg ulcers in an Australian setting. Qual. Life Res. 2019, 28, 1903–1911. [Google Scholar] [CrossRef]
- Palacios-Cartagena, R.P.; Pastor-Cisneros, R.; Adsuar, J.C.; Pérez-Gómez, J.; García-Gordillo, M.Á.; Mendoza-Muñoz, M. CHU9D Normative Data in Peruvian Adolescents. J. Pers. Med. 2021, 11, 1272. [Google Scholar] [CrossRef]
- Calzada-Rodríguez, J.I.; Denche-Zamorano, M.; Pérez-Gómez, J.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Barrios-Fernandez, S.; Adsuar, J.C. Health-Related Quality of Life and Frequency of Physical Activity in Spanish Students Aged 8–14. Int. J. Environ. Res. Public Health 2021, 18, 9418. [Google Scholar] [CrossRef]
- Lindvall, K.; Vaezghasemi, M.; Feldman, I.; Ivarsson, A.; Stevens, K.J.; Petersen, S. Feasibility, reliability and validity of the health-related quality of life instrument Child Health Utility 9D (CHU9D) among school-aged children and adolescents in Sweden. Health Qual. Life Outcomes 2021, 19, 193. [Google Scholar] [CrossRef]
- Rowen, D.; Mulhern, B.; Stevens, K.; Vermaire, J.H. Estimating a Dutch value set for the pediatric preference-based CHU9D using a discrete choice experiment with duration. Value Health 2018, 21, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Bashir, N.S.; Walters, T.D.; Griffiths, A.M.; Ungar, W.J. An Assessment of the Validity and Reliability of the Pediatric Child Health Utility 9D in Children with Inflammatory Bowel Disease. Children 2021, 8, 343. [Google Scholar] [CrossRef] [PubMed]
- Foster Page, L.A.; Thomson, W.M.; Marshman, Z.; Stevens, K.J. The potential of the Child Health Utility 9D Index as an outcome measure for child dental health. BMC Oral Health 2014, 14, 90. [Google Scholar] [CrossRef] [PubMed]
- Rogers, H.J.; Vermaire, J.H.; Gilchrist, F.; Schuller, A.A. The Relationship between Caries-Specific Quality of Life and Generic Wellbeing in a Dutch Pediatric Population. Dent. J. 2019, 7, 67. [Google Scholar] [CrossRef]
- Petersen, K.D.; Ratcliffe, J.; Chen, G.; Serles, D.; Frøsig, C.S.; Olesen, A.V. The construct validity of the Child Health Utility 9D-DK instrument. Health Qual. Life Outcomes 2019, 17, 187. [Google Scholar] [CrossRef]
- Wolf, R.T.; Ratcliffe, J.; Chen, G.; Jeppesen, P. The longitudinal validity of proxy-reported CHU9D. Qual. Life Res. 2021, 30, 1747–1756. [Google Scholar] [CrossRef]
- Boyer, N.R.; Miller, S.; Connolly, P.; McIntosh, E. Paving the way for the use of the SDQ in economic evaluations of school-based population health interventions: An empirical analysis of the external validity of SDQ mapping algorithms to the CHU9D in an educational setting. Qual. Life Res. 2016, 25, 913–923. [Google Scholar] [CrossRef]
- Stevens, K. Valuation of the child health utility 9D index. Pharmacoeconomics 2012, 30, 729–747. [Google Scholar] [CrossRef]
- Ratcliffe, J.; Flynn, T.; Terlich, F.; Stevens, K.; Brazier, J.; Sawyer, M. Developing adolescent-specific health state values for economic evaluation: An application of profile case best-worst scaling to the Child Health Utility 9D. Pharmacoeconomics 2012, 30, 713–727. [Google Scholar] [CrossRef]
- Furber, G.; Segal, L. The validity of the Child Health Utility instrument (CHU9D) as a routine outcome measure for use in child and adolescent mental health services. Health Qual. Life Outcomes 2015, 13, 22. [Google Scholar] [CrossRef]
- Hayes, A.; Raghunandan, R.; Killedar, A.; Smith, S.; Cvejic, E.; Howell, M.; Petrou, S.; Lancsar, E.; Wong, G.; Craig, J.; et al. Reliability, acceptability, validity and responsiveness of the CHU9D and PedsQL in the measurement of quality of life in children and adolescents with overweight and obesity. Int. J. Obes. 2023, 47, 622–629. [Google Scholar] [CrossRef]
- Jones, R.; Mulhern, B.; Devlin, N.; O’loughlin, R.; Xiong, X.; Bahrampour, M.; McGregor, K.; Yip, S.; Hiscock, H.; Dalziel, K. PCR62 The Australian Paediatric Multi-Instrument Comparison (P-MIC) Study: Data Quality, Feasibility, Acceptability, and Construct Validity of the EQ-5D-Y-3L, EQ-5D-Y5L, CHU9D, PedsQL, HUI, PROMIS-25 and AQoL-6D. Value Health 2022, 25, S401–S402. [Google Scholar] [CrossRef]
- Chen, G.; Flynn, T.; Stevens, K.; Brazier, J.; Huynh, E.; Sawyer, M.; Ratcliffe, J. Assessing the health-related quality of life of Australian adolescents: An empirical comparison of the child health utility 9D and EQ-5D-Y instruments. Value Health 2015, 18, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, J.; Huynh, E.; Chen, G.; Stevens, K.; Swait, J.; Brazier, J.; Flynn, T. Valuing the child health utility 9D: Using profile case best worst scaling methods to develop a new adolescent specific scoring algorithm. Soc. Sci. Med. 2016, 157, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.Y.; Li, T.; Gong, F.H.; Zhang, J.S.; Li, X.K. Predictors of health-related quality of life and influencing factors for COVID-19 patients, a follow-up at one month. Front. Psychiatry 2020, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Fuerboeter, M.; Boettcher, J.; Barkmann, C.; Zapf, H.; Nazarian, R.; Wiegand-Grefe, S.; Boettcher, M. Quality of life and mental health of children with rare congenital surgical diseases and their parents during the COVID-19 pandemic. Orphanet J. Rare Dis. 2021, 16, 498. [Google Scholar] [CrossRef] [PubMed]
- Riiser, K.; Helseth, S.; Haraldstad, K.; Torbjørnsen, A.; Richardsen, K.R. Adolescents’ health literacy, health protective measures, and health-related quality of life during the COVID-19 pandemic. PLoS ONE 2020, 15, e0238161. [Google Scholar] [CrossRef]
- Canaway, A.G.; Frew, E.J. Measuring preference-based quality of life in children aged 6–7 years: A comparison of the performance of the CHU-9D and EQ-5D-Y—The WAVES Pilot Study. Qual. Life Res. 2013, 22, 173–183. [Google Scholar] [CrossRef]
- Chen, P.; Lin, K.C.; Liing, R.J.; Wu, C.Y.; Chen, C.L.; Chang, K.C. Validity, responsiveness, and minimal clinically important difference of EQ-5D-5L in stroke patients undergoing rehabilitation. Qual. Life Res. 2016, 25, 1585–1596. [Google Scholar] [CrossRef]
- Kaplan, R.M. The minimally clinically important difference in generic utility-based measures. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 91–97. [Google Scholar] [CrossRef]
- McClure, N.S.; Al Sayah, F.; Xie, F.; Luo, N.; Johnson, J.A. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health 2017, 20, 644–650. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, L.A.; Veloso, C.F.; de Campos Souza, M.; de Azevedo, J.M.C.; Tarro, G. The potential impact of the COVID-19 pandemic on child growth and development: A systematic review. J. Pediatr. 2020, 97, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Westrupp, E.M.; Greenwood, C.J.; Fuller-Tyszkiewicz, M.; Olsson, C.A.; Sciberras, E.; Mikocka-Walus, A.; Wood, A.G. Parent and child mental health trajectories April 2020 to May 2021: Strict lockdown versus no lockdown in Australia. Aust. N. Z. J. Psychiatry 2021, 56, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Guessoum, S.B.; Lachal, J.; Radjack, R.; Carretier, E.; Minassian, S.; Benoit, L.; Moro, M.R. Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Res. 2021, 291, 113264. [Google Scholar] [CrossRef]
- Babicki, M.; Malchrzak, W.; Hans-Wytrychowska, A.; Mastalerz-Migas, A. Impact of vaccination on the sense of security, the anxiety of COVID-19 and quality of life among polish. A nationwide online survey in Poland. Vaccines 2021, 9, 1444. [Google Scholar]
- Freund, O.; Tau, L.; Weiss, T.E.; Zornitzki, L.; Frydman, S.; Jacob, G.; Bornstein, G. Associations of vaccine status with characteristics and outcomes of hospitalized severe COVID-19 patients in the booster era. PLoS ONE 2022, 17, e0268050. [Google Scholar] [CrossRef]
- Bilge, Y.; Keles, E.; Baydili, K.N. The impact of COVID-19 vaccination on mental health. J. Loss Trauma 2022, 27, 285–288. [Google Scholar] [CrossRef]
- Webster, P. COVID-19 timeline of events. Nat. Med. 2021, 27, 2054–2055. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary behaviors and physical activity of Italian undergraduate students during lockdown at the time of COVID−19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Alkeridy, W.A.; Alquaydheb, H.; Almuhaidib, S.; Sindi, N.A.; Aljasser, A.; Kow, J.K.; Alqahtani, A.S. Determinants of Vaccine Hesitancy among Home Health Care Service Recipients in Saudi Arabia. Vaccines 2023, 11, 1436. [Google Scholar] [CrossRef]
- Kang, H.; Chung, I.-J.; Oh, S. Impact of the COVID-19 Pandemic on the Developmental Outcomes among Korean Kinship Foster Care Children: Gender Differences. Societie 2023, 13, 202. [Google Scholar] [CrossRef]
- Teng, C.-C.; Cheng, Y.-J.; Yen, W.-S.; Shih, P.-Y. COVID-19 Perceived Risk, Travel Risk Perceptions and Hotel Staying Intention: Hotel Hygiene and Safety Practices as a Moderator. Sustainability 2023, 15, 13048. [Google Scholar] [CrossRef]
- Ruotolo, F.; Ruggiero, G.; Cattaneo, Z.; Arioli, M.; Candini, M.; Frassinetti, F.; Pazzaglia, F.; Fornara, F.; Bosco, A.; Iachini, T. Psychological Reactions during and after a Lockdown: Self-Efficacy as a Protective Factor of Mental Health. Int. J. Environ. Res. Public Health 2023, 20, 6679. [Google Scholar] [CrossRef]
- Pietersma, S.; van den Akker-van, M.E.; de Vries, M. Generic quality of life utility measures in health-care research: Conceptual issues highlighted for the most commonly used utility measures. Int. J. Wellbeing 2013, 3, 2. [Google Scholar]



| CHU9D (n = 2025) | EQ-5D-5L (n = 5751) | |
|---|---|---|
| Age, mean (SD) | 8.41 (3.63) | 2.78 (1.74) |
| Female, n (%) | 980 (48.4%) | 3002 (52.2%) |
| Chronic conditions Yes, n (%) | 241 (11.9%) | 274 (4.8%) |
| COVID Symptoms, n (%) * | ||
| Fever | 186 (9.2%) | 1120 (19.5%) |
| Chills or shakes | 54 (2.7%) | 127(2.2%) |
| Cough | 696 (34.4%) | 3070 (53.4%) |
| Diarrhea | 21 (1.0%) | 146 (2.5%) |
| Sore throat | 789 (39.0%) | 807 (14.0%) |
| Breathing difficulties | 47(2.3%) | 221 (3.8%) |
| Loss of appetite | 70 (3.5%) | 431 (7.5%) |
| Headache | 240 (11.9%) | 136 (2.4%) |
| Muscle ache | 61 (3.0%) | 38 (0.6%) |
| Abdominal pain | 77 (3.8%) | 94 (1.6%) |
| Stuffy or runny nose | 1051 (51.9%) | 3708 (64.5%) |
| Loss of smell | 29 (1.4%) | 11 (0.2%) |
| Nausea | 79 (3.9%) | 98 (1.7%) |
| No symptoms | 531 (26.2%) | 918 (16%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brusco, N.K.; Danchin, M.; Watts, J.J.; Jos, C.; Loughnan, M.; Williams, T.; Ratcliffe, J.; Hoq, M.; Tosif, S.; Kaufman, J. Parent-Reported Child and Parent Quality of Life during COVID-19 Testing at an Australian Paediatric Hospital Outpatient Clinic: A Cross-Sectional Study. Healthcare 2023, 11, 2555. https://doi.org/10.3390/healthcare11182555
Brusco NK, Danchin M, Watts JJ, Jos C, Loughnan M, Williams T, Ratcliffe J, Hoq M, Tosif S, Kaufman J. Parent-Reported Child and Parent Quality of Life during COVID-19 Testing at an Australian Paediatric Hospital Outpatient Clinic: A Cross-Sectional Study. Healthcare. 2023; 11(18):2555. https://doi.org/10.3390/healthcare11182555
Chicago/Turabian StyleBrusco, Natasha K., Margie Danchin, Jennifer J. Watts, Carol Jos, Myles Loughnan, Tria Williams, Julie Ratcliffe, Monsurul Hoq, Shidan Tosif, and Jessica Kaufman. 2023. "Parent-Reported Child and Parent Quality of Life during COVID-19 Testing at an Australian Paediatric Hospital Outpatient Clinic: A Cross-Sectional Study" Healthcare 11, no. 18: 2555. https://doi.org/10.3390/healthcare11182555
APA StyleBrusco, N. K., Danchin, M., Watts, J. J., Jos, C., Loughnan, M., Williams, T., Ratcliffe, J., Hoq, M., Tosif, S., & Kaufman, J. (2023). Parent-Reported Child and Parent Quality of Life during COVID-19 Testing at an Australian Paediatric Hospital Outpatient Clinic: A Cross-Sectional Study. Healthcare, 11(18), 2555. https://doi.org/10.3390/healthcare11182555