
The Effect of Folic Acid Supplementation on Endothelial Function and Arterial Stiffness Markers in Adults: A Systematic Review and Meta-Analysis
 ,
,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection Process, Extraction and Analysis
2.5. Data Item
- 1.
- General information: title of the article, journal name, main author and publication year;
- 2.
- Study characteristics: name and design, country (region), sample size (total number and number of subjects for each group (which included and completed the trial) and study design;
- 3.
- Type and time of intervention: studies that compared the effect of oral folic acid (form and dose) supplementation with placebo on endothelial function (the control group received a placebo or other nutrients excluding folic acid) with an intervention duration of at least two weeks;
- 4.
- Study population characteristics: age (≥18 years old), sex (% of women), body mass index (BMI (kg/m2)) and health condition;
- 5.
- Outcomes measured:
- 5.1.
- Main outcome:
- Endothelial function: flow-mediated dilation (FMD (%)).
- 5.2.
- Endothelial function: flow-mediated dilation (FMD (%)).
- Arterial stiffness parameters: pulse wave velocity (PWV (m/s)); pulse wave analysis (PWA), augmentation index (AIx (%));
- Endothelial function parameters: asymmetric dimethylarginine (ADMA (μmol/L)), endothelial nitric oxide synthase (eNOS (ng/mL)), monocyte chemotactic protein (MCP-1 (pg/mL)), matrix metalloproteinase (MMP), plasminogen activator inhibitor-1 (PAI-1 (AU/mL)), soluble vascular cell adhesion molecule-1 (sVCAM-1 (ng/mL)), intercellular adhesion molecule-1 (ICAM-1 (ng/mL)), vascular endothelial growth factor (VEGF (pg/mL)).
2.6. Risk of Bias of Individual Studies
2.7. Statistical Analysis
3. Results
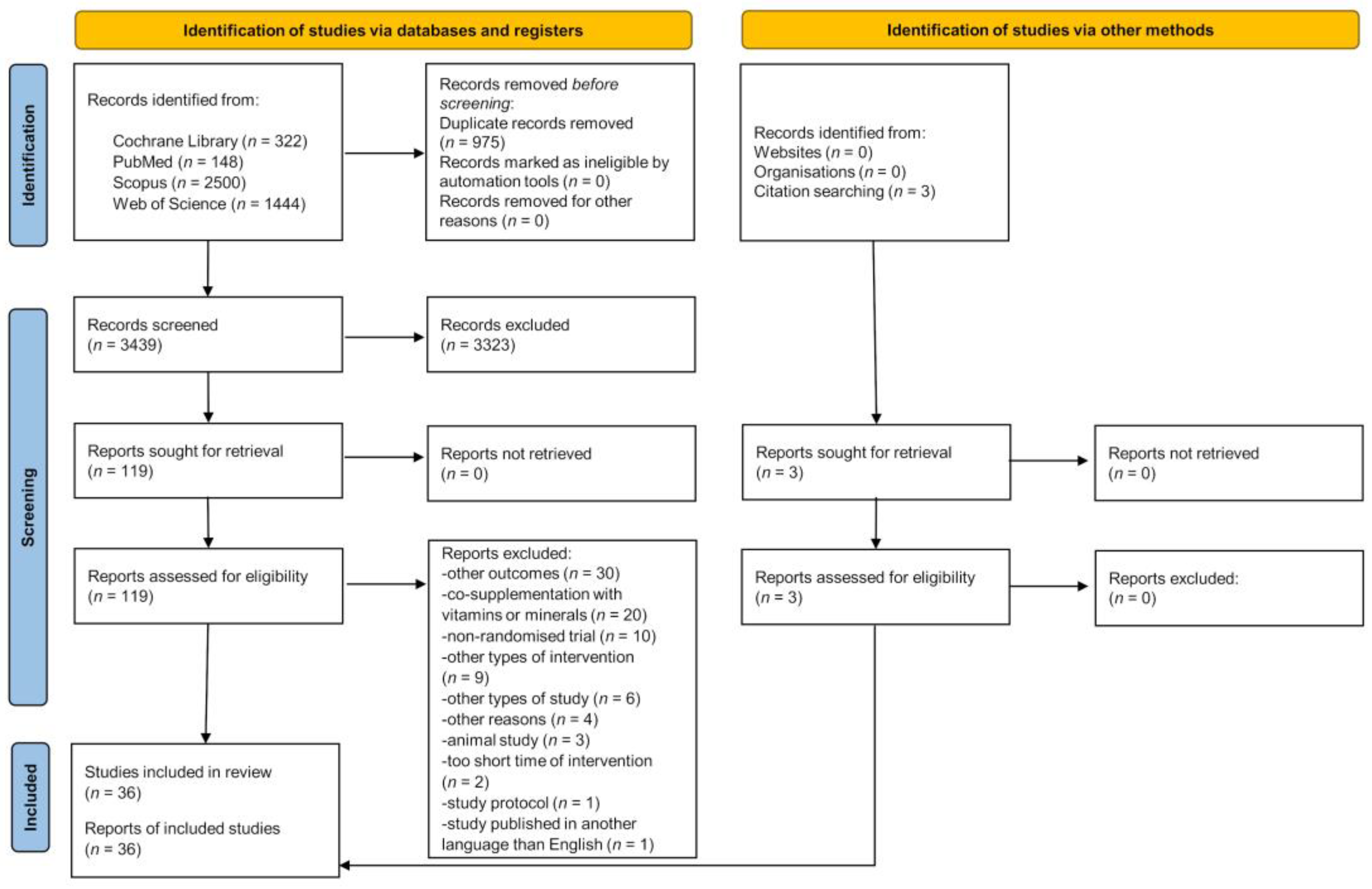
3.1. Search Result
3.2. Characteristics of Included Studies
3.3. Characteristics of Intervention
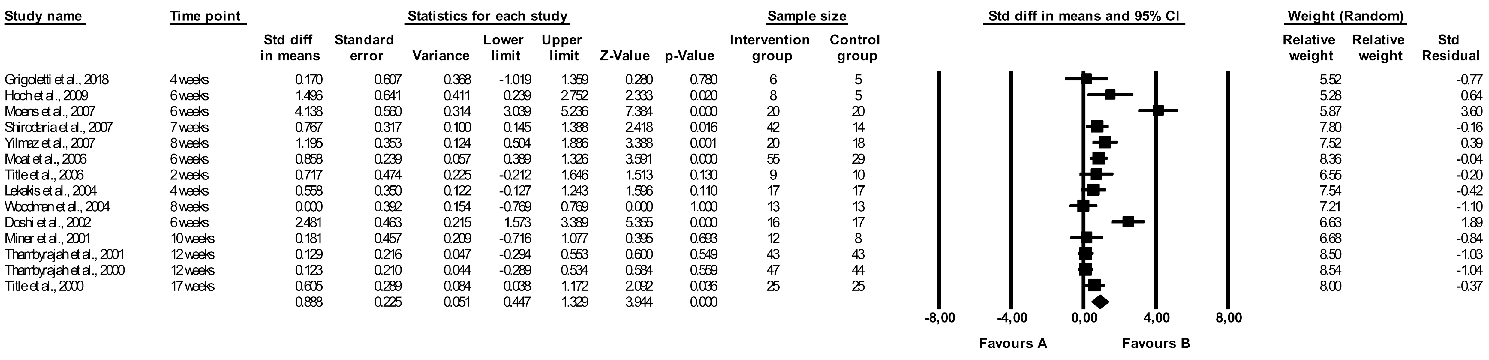
3.4. The Effect of Folic Acid Supplementation on Flow-Mediated Dilation
3.5. The Effect of Folic Acid Supplementation on Pulse Wave Velocity
3.6. The Effect of Folic Acid Supplementation on Monocyte Chemotactic Protein 1
3.7. The Effect of Folic Acid Supplementation on Other Endothelial Parameters
3.8. Subgroup Analysis
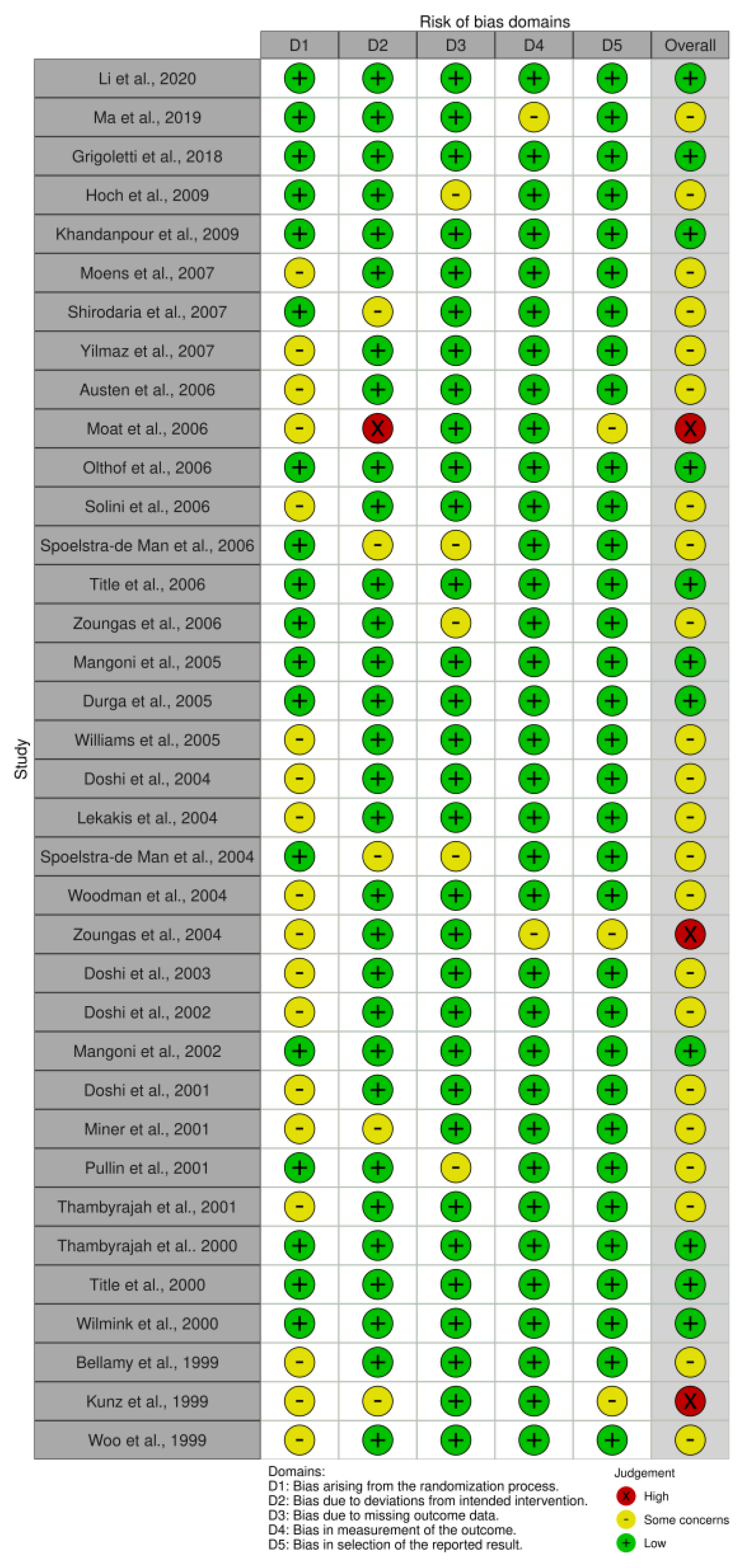
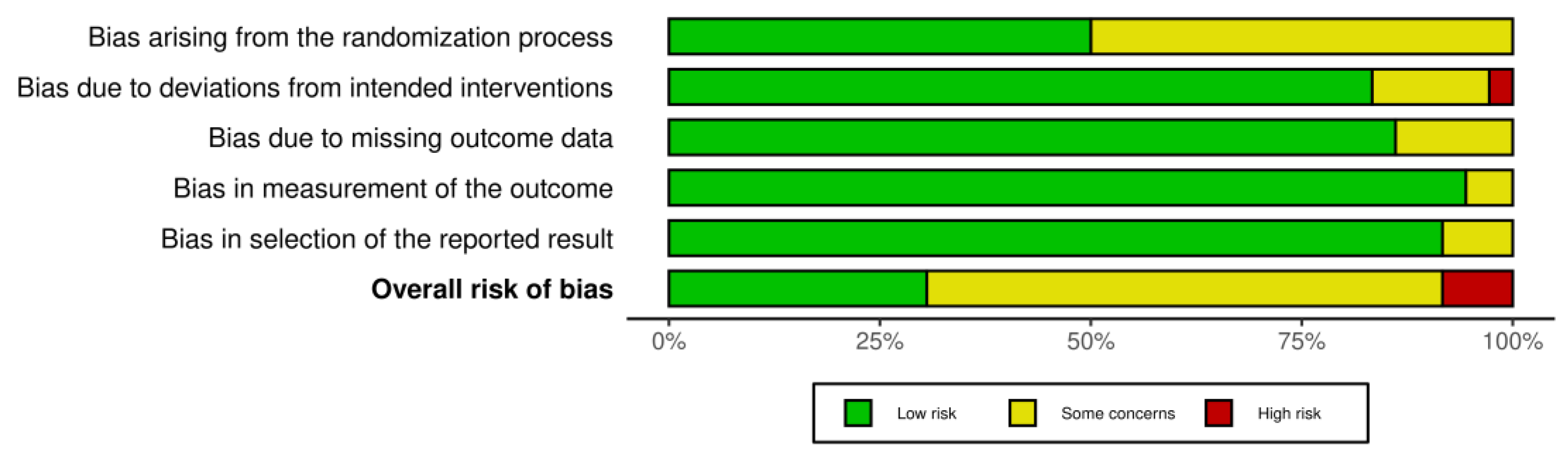
3.9. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Godo, S.; Shimokawa, H. Endothelial Functions. Arterioscler. Thromb. Vasc. Biol. 2017, 37, e108–e114. [Google Scholar] [CrossRef] [PubMed]
- Konukoglu, D.; Uzun, H. Endothelial Dysfunction and Hypertension. Adv. Exp. Med. Biol. 2017, 956, 511–540. [Google Scholar] [CrossRef] [PubMed]
- Durand, M.J.; Gutterman, D.D. Diversity in mechanisms of endothelium-dependent vasodilation in health and disease. Microcirculation 2013, 20, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef]
- Storch, A.S.; Mattos, J.D.; Alves, R.; Galdino, I.S.; Rocha, H.N.M. Methods of endothelial function assessment: Description and applications. Int. J. Cardiovasc. Sci. 2017, 30, 262–273. [Google Scholar] [CrossRef]
- Oh, Y.S. Arterial stiffness and hypertension. Clin. Hypertens. 2018, 24, 17. [Google Scholar] [CrossRef] [PubMed]
- Lacolley, P.; Regnault, V.; Laurent, S. Mechanisms of Arterial Stiffening: From Mechanotransduction to Epigenetics. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1055–1062. [Google Scholar] [CrossRef]
- Reddy, A.K.; Taffet, G.E. Pulse wave velocity: Why is it important to know to estimate? J. Cardiovasc. Aging 2022, 2, 10. [Google Scholar] [CrossRef]
- Janić, M.; Lunder, M.; Sabovič, M. Arterial stiffness and cardiovascular therapy. Biomed Res. Int. 2014, 2014, 621437. [Google Scholar] [CrossRef] [PubMed]
- Esper, R.J.; Nordaby, R.A.; Vilariño, J.O.; Paragano, A.; Cacharrón, J.L.; Machado, R.A. Endothelial dysfunction: A comprehensive appraisal. Cardiovasc. Diabetol. 2006, 5, 4. [Google Scholar] [CrossRef]
- Hirsch, S.; Pia De la Maza, M.; Yañez, P.; Glasinovic, A.; Petermann, M.; Barrera, G.; Gattas, V.; Escobar, E.; Bunout, D. Hyperhomocysteinemia and endothelial function in young subjects: Effects of vitamin supplementation. Clin. Cardiol. 2002, 25, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Mudau, M.; Genis, A.; Lochner, A.; Strijdom, H. Endothelial dysfunction: The early predictor of atherosclerosis. Cardiovasc. J. Afr. 2012, 23, 222–231. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific opinion on dietary reference values for folate. EFSA J. 2014, 12, 3893. [Google Scholar] [CrossRef]
- National Institutes of Health. Folate Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/Folate-HealthProfessional/ (accessed on 12 October 2022).
- Bailey, L.B.; Caudill, M.A. Folate. In Present Knowledge in Nutrition, 10th ed.; Erdman, J.W., Macdonald, I.A., Zeisel, S.H., Eds.; Wiley-Blackwell: Washington, DC, USA, 2012; pp. 321–342. ISBN 978-0470959176. [Google Scholar]
- Symons, J.D.; Mullick, A.E.; Ensunsa, J.L.; Ma, A.A.; Rutledge, J.C. Hyperhomocysteinemia evoked by folate depletion: Effects on coronary and carotid arterial function. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Sherwood, R.A.; Asonganyi, B.; Ouldred, E.L.; Thomas, S.; Jackson, S.H. Folic acid: A marker of endothelial function in type 2 diabetes? Vasc. Health Risk Manag. 2005, 1, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Peña, A.S.; Wiltshire, E.; Gent, R.; Piotto, L.; Hirte, C.; Couper, J. Folic acid does not improve endothelial function in obese children and adolescents. Diabetes Care 2007, 30, 2122–2127. [Google Scholar] [CrossRef] [PubMed]
- Stanhewicz, A.E.; Kenney, W.L. Role of folic acid in nitric oxide bioavailability and vascular endothelial function. Nutr. Rev. 2017, 75, 61–70. [Google Scholar] [CrossRef]
- Bellien, J.; Favre, J.; Iacob, M.; Gao, J.; Thuillez, C.; Richard, V.; Joannidès, R. Arterial stiffness is regulated by nitric oxide and endothelium-derived hyperpolarizing factor during changes in blood flow in humans. Hypertension 2010, 55, 674–680. [Google Scholar] [CrossRef]
- Ozkor, M.A.; Murrow, J.R.; Rahman, A.M.; Kavtaradze, N.; Lin, J.; Manatunga, A.; Quyyumi, A.A. Endothelium-derived hyperpolarizing factor determines resting and stimulated forearm vasodilator tone in health and in disease. Circulation 2011, 123, 2244–2253. [Google Scholar] [CrossRef]
- Holven, K.B.; Aukrust, P.; Holm, T.; Ose, L.; Nenseter, M.S. Folic acid treatment reduces chemokine release from peripheral blood mononuclear cells in hyperhomocysteinemic subjects. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 699–703. [Google Scholar] [CrossRef]
- Jones, P.; Lucock, M.; Scarlett, C.J.; Veysey, M.; Beckett, E.L. Folate and Inflammation—Links between folate and features of inflammatory conditions. J. Nutr. Intermed. Metab. 2019, 18, 100104. [Google Scholar] [CrossRef]
- van Dijk, S.C.; Enneman, A.W.; Swart, K.M.; van Wijngaarden, J.P.; Ham, A.C.; de Jonge, R.; Blom, H.J.; Feskens, E.J.; Geleijnse, J.M.; van Schoor, N.M.; et al. Effect of vitamin B12 and folic acid supplementation on biomarkers of endothelial function and inflammation among elderly individuals with hyperhomocysteinemia. Vasc. Med. 2016, 21, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Arya, R.; Ford, E.; Asonganyi, B.; Sherwood, R.A.; Ouldred, E.; Swift, C.G.; Jackson, S.H. Effects of folic acid supplementation on inflammatory and thrombogenic markers in chronic smokers. A randomised controlled trial. Thromb. Res. 2003, 110, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Sherwood, R.A.; Asonganyi, B.; Swift, C.G.; Thomas, S.; Jackson, S.H. Short-term oral folic acid supplementation enhances endothelial function in patients with type 2 diabetes. Am. J. Hypertens. 2005, 18, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Khandanpour, N.; Armon, M.P.; Jennings, B.; Finglas, P.M.; Willis, G.; Clark, A.; Meyer, F.J. Randomized clinical trial of folate supplementation in patients with peripheral arterial disease. Br. J. Surg. 2009, 96, 990–998. [Google Scholar] [CrossRef]
- Austen, S.K.; Fassett, R.G.; Geraghty, D.P.; Coombes, J.S. Folate supplementation fails to affect vascular function and carotid artery intima media thickness in cyclosporin A-treated renal transplant recipients. Clin. Nephrol. 2006, 66, 373–379. [Google Scholar] [CrossRef]
- Woodman, R.J.; Celermajer, D.E.; Thompson, P.L.; Hung, J. Folic acid does not improve endothelial function in healthy hyperhomocysteinaemic subjects. Clin. Sci. 2004, 106, 353–358. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated August 2022). Cochrane 2022. Available online: https://training.cochrane.org/handbook/current (accessed on 25 October 2022).
- Bokayeva, K.; Jamka, M.; Banaszak, M.; Makarewicz-Bukowska, A.; Adamczak, A.; Chrobot, M.; Janicka, A.; Jaworska, N.; Walkowiak, J. The Effect of Folic Acid Supplementation on Endothelial Function. PROSPERO: International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021290195 (accessed on 28 June 2023).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Sterne, J.A.C.; Savović, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. In Cochrane Methods. Cochrane Database of Systematic Reviews; Chandler, J., McKenzie, J., Boutron, I., Welch, V., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; Volume 10, (Suppl. S1). [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Kunz, K.; Petitjean, P.; Lisri, M.; Chantrel, F.; Koehl, C.; Wiesel, M.L.; Cazenave, J.P.; Moulin, B.; Hannedouche, T.P. Cardiovascular morbidity and endothelial dysfunction in chronic haemodialysis patients: Is homocyst(e)ine the missing link? Nephrol. Dial. Transplant. 1999, 14, 1934–1942. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, M.F.; McDowell, I.F.; Ramsey, M.W.; Brownlee, M.; Newcombe, R.G.; Lewis, M.J. Oral folate enhances endothelial function in hyperhomocysteinaemic subjects. Eur. J. Clin. Investig. 1999, 29, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.S.; Chook, P.; Lolin, Y.I.; Sanderson, J.E.; Metreweli, C.; Celermajer, D.S. Folic acid improves arterial endothelial function in adults with hyperhomocystinemia. J. Am. Coll. Cardiol. 1999, 34, 2002–2006. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, W.; Gao, Y.; Chen, Y.; Bai, D.; Weng, J.; Du, Y.; Ma, F.; Wang, X.; Liu, H.; et al. Effect of folic acid combined with docosahexaenoic acid intervention on mild cognitive impairment in elderly: A randomized double-blind, placebo-controlled trial. Eur. J. Nutr. 2021, 60, 1795–1808. [Google Scholar] [CrossRef] [PubMed]
- Shirodaria, C.; Antoniades, C.; Lee, J.; Jackson, C.E.; Robson, M.D.; Francis, J.M.; Moat, S.J.; Ratnatunga, C.; Pillai, R.; Refsum, H.; et al. Global improvement of vascular function and redox state with low-dose folic acid: Implications for folate therapy in patients with coronary artery disease. Circulation 2007, 115, 2262–2270. [Google Scholar] [CrossRef]
- Moat, S.J.; Madhavan, A.; Taylor, S.Y.; Payne, N.; Allen, R.H.; Stabler, S.P.; Goodfellow, J.; McDowell, I.F.; Lewis, M.J.; Lang, D. High- but not low-dose folic acid improves endothelial function in coronary artery disease. Eur. J. Clin. Investig. 2006, 36, 850–859. [Google Scholar] [CrossRef]
- Doshi, S.N.; Moat, S.J.; Lewis, M.J.; McDowell, I.F.; Giddings, J.C.; Goodfellow, J. Short-term high-dose folic acid does not alter markers of endothelial cell damage in patients with coronary heart disease. Int. J. Cardiol. 2004, 94, 203–207. [Google Scholar] [CrossRef]
- Doshi, S.; McDowell, I.; Moat, S.; Lewis, M.; Goodfellow, J. Folate improves endothelial function in patients with coronary heart disease. Clin. Chem. Lab. Med. 2003, 41, 1505–1512. [Google Scholar] [CrossRef]
- Doshi, S.N.; McDowell, I.F.; Moat, S.J.; Payne, N.; Durrant, H.J.; Lewis, M.J.; Goodfellow, J. Folic acid improves endothelial function in coronary artery disease via mechanisms largely independent of homocysteine lowering. Circulation 2002, 105, 22–26. [Google Scholar] [CrossRef]
- Mangoni, A.A.; Sherwood, R.A.; Swift, C.G.; Jackson, S.H. Folic acid enhances endothelial function and reduces blood pressure in smokers: A randomized controlled trial. J. Intern. Med. 2002, 252, 497–503. [Google Scholar] [CrossRef]
- Doshi, S.N.; McDowell, I.F.; Moat, S.J.; Lang, D.; Newcombe, R.G.; Kredan, M.B.; Lewis, M.J.; Goodfellow, J. Folate improves endothelial function in coronary artery disease: An effect mediated by reduction of intracellular superoxide? Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Pullin, C.H.; Ashfield-Watt, P.A.; Burr, M.L.; Clark, Z.E.; Lewis, M.J.; Moat, S.J.; Newcombe, R.G.; Powers, H.J.; Whiting, J.M.; McDowell, I.F. Optimization of dietary folate or low-dose folic acid supplements lower homocysteine but do not enhance endothelial function in healthy adults, irrespective of the methylenetetrahydrofolate reductase (C677T) genotype. J. Am. Coll. Cardiol. 2001, 38, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Thambyrajah, J.; Landray, M.J.; Jones, H.J.; McGlynn, F.J.; Wheeler, D.C.; Townend, J.N. A randomized double-blind placebo-controlled trial of the effect of homocysteine-lowering therapy with folic acid on endothelial function in patients with coronary artery disease. J. Am. Coll. Cardiol. 2001, 37, 1858–1863. [Google Scholar] [CrossRef] [PubMed]
- Thambyrajah, J.; Landray, M.J.; McGlynn, F.J.; Jones, H.J.; Wheeler, D.C.; Townend, J.N. Does folic acid decrease plasma homocysteine and improve endothelial function in patients with predialysis renal failure? Circulation 2000, 102, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Zoungas, S.; McGrath, B.P.; Branley, P.; Kerr, P.G.; Muske, C.; Wolfe, R.; Atkins, R.C.; Nicholls, K.; Fraenkel, M.; Hutchison, B.G.; et al. Cardiovascular morbidity and mortality in the Atherosclerosis and Folic Acid Supplementation Trial (ASFAST) in chronic renal failure: A multicenter, randomized, controlled trial. J. Am. Coll. Cardiol. 2006, 47, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.; Kingwell, B.A.; Burke, K.; McPherson, J.; Dart, A.M. Folic acid supplementation for 3 wk reduces pulse pressure and large artery stiffness independent of MTHFR genotype. Am. J. Clin. Nutr. 2005, 82, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Zoungas, S.; Branley, P.; Kerr, P.G.; Ristevski, S.; Muske, C.; Demos, L.; Atkins, R.C.; Becker, G.; Fraenkel, M.; Hutchison, B.G.; et al. Atherosclerosis and folic acid supplementation trial in chronic renal failure: Baseline results. Nephrology 2004, 9, 130–141. [Google Scholar] [CrossRef]
- Olthof, M.R.; Bots, M.L.; Katan, M.B.; Verhoef, P. Effect of folic acid and betaine supplementation on flow-mediated dilation: A randomized, controlled study in healthy volunteers. PLoS Clin. Trials 2006, 1, e10. [Google Scholar] [CrossRef]
- Spoelstra-de Man, A.M.E.; Brouwer, C.B.; Terheggen, F.; Bollen, J.M.; Stehouwer, C.D.; Smulders, Y.M. No effect of folic acid on markers of endothelial dysfunction or inflammation in patients with type 2 diabetes mellitus and mild hyperhomocysteinaemia. Neth. J. Med. 2004, 62, 246–253. [Google Scholar]
- Wilmink, H.W.; Stroes, E.S.; Erkelens, W.D.; Gerritsen, W.B.; Wever, R.; Banga, J.D.; Rabelink, T.J. Influence of folic acid on postprandial endothelial dysfunction. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 185–188. [Google Scholar] [CrossRef]
- Spoelstra-de Man, A.M.E.; Teerlink, T.; Brouwer, C.B.; Rauwerda, J.A.; Stehouwer, C.D.; Smulders, Y.M. No effect of B vitamins on ADMA levels in patients at increased cardiovascular risk. Clin. Endocrinol. 2006, 64, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Durga, J.; van Tits, L.J.; Schouten, E.G.; Kok, F.J.; Verhoef, P. Effect of lowering of homocysteine levels on inflammatory markers: A randomized controlled trial. Arch. Intern. Med. 2005, 165, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Title, L.M.; Ur, E.; Giddens, K.; McQueen, M.J.; Nassar, B.A. Folic acid improves endothelial dysfunction in type 2 diabetes—An effect independent of homocysteine-lowering. Vasc. Med. 2006, 11, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Title, L.M.; Cummings, P.M.; Giddens, K.; Genest, J.J., Jr.; Nassar, B.A. Effect of folic acid and antioxidant vitamins on endothelial dysfunction in patients with coronary artery disease. J. Am. Coll. Cardiol. 2000, 36, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Miner, S.E.; Cole, D.E.; Evrovski, J.; Forrest, Q.; Hutchison, S.; Holmes, K.; Ross, H.J. Pyridoxine improves endothelial function in cardiac transplant recipients. J. Heart Lung Transplant. 2001, 20, 964–969. [Google Scholar] [CrossRef]
- Ma, F.; Zhou, X.; Li, Q.; Zhao, J.; Song, A.; An, P.; Du, Y.; Xu, W.; Huang, G. Effects of Folic Acid and Vitamin B12, Alone and in Combination on Cognitive Function and Inflammatory Factors in the Elderly with Mild Cognitive Impairment: A Single-blind Experimental Design. Curr. Alzheimer Res. 2019, 16, 622–632. [Google Scholar] [CrossRef]
- Solini, A.; Santini, E.; Ferrannini, E. Effect of short-term folic acid supplementation on insulin sensitivity and inflammatory markers in overweight subjects. Int. J. Obes. 2006, 30, 1197–1202. [Google Scholar] [CrossRef]
- Grigoletti, S.S.; Ribeiro, J.P.; Sprinz, E.; Ribeiro, P.A.B. Short-term folinic acid supplementation and aerobic exercise improve vascular reactivity in HIV-infected individuals. HIV Clin. Trials 2018, 19, 148–151. [Google Scholar] [CrossRef]
- Hoch, A.Z.; Pajewski, N.M.; Hoffmann, R.G.; Schimke, J.E.; Gutterman, D.D. Possible relationship of folic Acid supplementation and improved flow-mediated dilation in premenopausal, eumenorrheic athletic women. J. Sports Sci. Med. 2009, 8, 123–129. [Google Scholar]
- Moens, A.L.; Claeys, M.J.; Wuyts, F.L.; Goovaerts, I.; Van Hertbruggen, E.; Wendelen, L.C.; Van Hoof, V.O.; Vrints, C.J. Effect of folic acid on endothelial function following acute myocardial infarction. Am. J. Cardiol. 2007, 99, 476–481. [Google Scholar] [CrossRef]
- Yilmaz, H.; Sahin, S.; Sayar, N.; Tangurek, B.; Yilmaz, M.; Nurkalem, Z.; Onturk, E.; Cakmak, N.; Bolca, O. Effects of folic acid and N-acetylcysteine on plasma homocysteine levels and endothelial function in patients with coronary artery disease. Acta Cardiol. 2007, 62, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Lekakis, J.P.; Papamichael, C.M.; Papaioannou, T.G.; Dagre, A.G.; Stamatelopoulos, K.S.; Tryfonopoulos, D.; Protogerou, A.D.; Stamatelopoulos, S.F.; Mavrikakis, M. Oral folic acid enhances endothelial function in patients with hypercholesterolaemia receiving statins. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Moens, A.L.; Vrints, C.J.; Claeys, M.J.; Timmermans, J.P.; Champion, H.C.; Kass, D.A. Mechanisms and potential therapeutic targets for folic acid in cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, H1971–H1977. [Google Scholar] [CrossRef] [PubMed]
- Chalupsky, K.; Kračun, D.; Kanchev, I.; Bertram, K.; Görlach, A. Folic Acid Promotes Recycling of Tetrahydrobiopterin and Protects Against Hypoxia-Induced Pulmonary Hypertension by Recoupling Endothelial Nitric Oxide Synthase. Antioxid. Redox Signal. 2015, 23, 1076–1091. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Li, W.; Lv, X.; Wang, P.; Gao, Y.; Huang, G. Folic Acid Supplementation Delays Atherosclerotic Lesion Development by Modulating MCP1 and VEGF DNA Methylation Levels In Vivo and In Vitro. Int. J. Mol. Sci. 2017, 18, 990. [Google Scholar] [CrossRef] [PubMed]
- de Bree, A.; van Mierlo, L.A.; Draijer, R. Folic acid improves vascular reactivity in humans: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2007, 86, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.; Rezaiian, F.; Saadati, S.; Naseri, K.; Ashtary-Larky, D.; Yousefi, M.; Golalipour, E.; Clark, C.C.T.; Rastgoo, S.; Asbaghi, O. The effects of folic acid supplementation on endothelial function in adults: A systematic review and dose-response meta-analysis of randomized controlled trials. Nutr. J. 2023, 22, 12. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.; Chook, P.; Yip, T.; Kwong, S.; Hu, Y.; Huang, X.; Wu, M.J.; Liu, Y.M.; Lam, C.W.K.; Celermajer, D.S. Folic acid and vitamin B12 supplementation improves arterial function and structure in subjects with subnormal intake. Heart Lung Circ. 2008, 17, S201–S202. [Google Scholar] [CrossRef]
- Hashemi, M.; Heshmat-Ghahdarijani, K.; Zarean, E.; Baktash, F.; Mortazavi, Z.S. Evaluation of the effect of high-dose folic acid on endothelial dysfunction in pre-eclamptic patients: A randomized clinical trial. J. Res. Med. Sci. 2016, 21, 114. [Google Scholar] [CrossRef]
- Palomba, S.; Falbo, A.; Giallauria, F.; Russo, T.; Tolino, A.; Zullo, F.; Colao, A.; Orio, F. Effects of metformin with or without supplementation with folate on homocysteine levels and vascular endothelium of women with polycystic ovary syndrome. Diabetes Care 2010, 33, 246–251. [Google Scholar] [CrossRef]
- McRae, M.P. High-dose folic acid supplementation effects on endothelial function and blood pressure in hypertensive patients: A meta-analysis of randomized controlled clinical trials. J. Chiropr. Med. 2009, 8, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tian, T.; Zhang, H.; Gao, L.; Zhou, X. The effect of homocysteine-lowering therapy with folic acid on flow-mediated vasodilation in patients with coronary artery disease: A meta-analysis of randomized controlled trials. Atherosclerosis 2014, 235, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Zhou, Y.; Jiang, D.; Li, X.; Guo, Y.; Jiang, X. Efficacy of folic acid supplementation on endothelial function and plasma homocysteine concentration in coronary artery disease: A meta-analysis of randomized controlled trials. Exp. Ther. Med. 2014, 7, 1100–1110. [Google Scholar] [CrossRef] [PubMed]
- Winkels, R.M.; Brouwer, I.A.; Verhoef, P.; van Oort, F.V.; Durga, J.; Katan, M.B. Gender and body size affect the response of erythrocyte folate to folic acid treatment. J. Nutr. 2008, 138, 1456–1461. [Google Scholar] [CrossRef]
- Asbaghi, O.; Ghanavati, M.; Ashtary-Larky, D.; Bagheri, R.; Rezaei Kelishadi, M.; Nazarian, B.; Nordvall, M.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2021, 10, 871. [Google Scholar] [CrossRef] [PubMed]
- de Meer, K.; Smulders, Y.M.; Dainty, J.R.; Smith, D.E.; Kok, R.M.; Stehouwer, C.D.; Finglas, P.M.; Jakobs, C. [6S]5-methyltetrahydrofolate or folic acid supplementation and absorption and initial elimination of folate in young and middle-aged adults. Eur. J. Clin. Nutr. 2005, 59, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Köse, S.; Sözlü, S.; Bölükbaşi, H.; Ünsal, N.; Gezmen-Karadağ, M. Obesity is associated with folate metabolism. Int. J. Vitam. Nutr. Res. 2020, 90, 353–364. [Google Scholar] [CrossRef]
- Bird, J.K.; Ronnenberg, A.G.; Choi, S.W.; Du, F.; Mason, J.B.; Liu, Z. Obesity is associated with increased red blood cell folate despite lower dietary intakes and serum concentrations. J. Nutr. 2015, 145, 79–86. [Google Scholar] [CrossRef]
- Mlodzik-Czyzewska, M.A.; Malinowska, A.M.; Chmurzynska, A. Low folate intake and serum levels are associated with higher body mass index and abdominal fat accumulation: A case control study. Nutr. J. 2020, 19, 53. [Google Scholar] [CrossRef]
- Graham, I.M.; Daly, L.E.; Refsum, H.M.; Robinson, K.; Brattström, L.E.; Ueland, P.M.; Palma-Reis, R.J.; Boers, G.H.; Sheahan, R.G.; Israelsson, B.; et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. JAMA 1997, 277, 1775–1781. [Google Scholar] [CrossRef]
- Scaglione, F.; Panzavolta, G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica 2014, 44, 480–488. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country (Region) | Groups | n Included | n Completed | Study Design | Studied Population | Age (Years) 1 | BMI (kg/m2) 1 | Sex [% of Women] |
|---|---|---|---|---|---|---|---|---|---|---|
| Li et al. [39] | 2020 | China (Asia) | Intervention 2 | 60 | 55 | RCT parallel | Elderly subjects with mild cognitive impairment | 70.33 ± 7.70 | 24.41 ± 2.47 | 60 |
| Intervention 3 | 60 | 53 | 70.20 ± 6.13 | 25.47 ± 3.01 | 60 | |||||
| Intervention 4 | 60 | 53 | 71.55 ± 6.62 | 24.70 ± 2.52 | 60 | |||||
| Control | 60 | 51 | 70.38 ± 6.73 | 24.30 ± 2.93 | 55 | |||||
| Ma et al. [61] | 2019 | China (Asia) | Intervention 3 | 60 | 58 | RCT parallel | Elderly subjects with mild cognitive impairment | 68.42 ± 3.62 | NI | 63 |
| Intervention 5 | 60 | 58 | 69.47 ± 2.88 | 65 | ||||||
| Intervention 6 | 60 | 58 | 69.16 ± 2.46 | 65 | ||||||
| Control | 60 | 57 | 68.54 ± 3.90 | 63 | ||||||
| Grigoletti et al. [63] | 2018 | Brazil (South America) | Intervention 3 | 6 | NI | RCT parallel | HIV-infected individuals, antiretroviral therapy (at least 6 months) with undetectable viral load (<50 copies/mL) and CD4 count > 200 cells/mm3 | 53 ± 3 8 | NI | 50 |
| Intervention 7 | 5 | 52 ± 3 8 | 40 | |||||||
| Control | 5 | 48 ± 3 8 | 60 | |||||||
| Hoch et al. [64] | 2009 | USA (North America) | Intervention | NI | 8 | RCT parallel | Eumenorrheic woman who were not taking birth control pills and who ran at least 20 miles/week | 25.0 ± 1.4 9 | 20.7 ± 0.6 9 | 100 |
| Control | 5 | 22.4 ± 0.9 9 | 24.4 ± 1.2 9 | 100 | ||||||
| Khandanpour et al. [27] | 2009 | United Kingdom (Europe) | Intervention 3 | 46 | 45 | RCT parallel | Subjects with peripheral arterial disease | 70.1 ± 9.0 | 27.5 ± 4.5 | 69 |
| Intervention 10 | 51 | 48 | 69.7 ± 7.6 | 27.3 ± 3.6 | 71 | |||||
| Control | 46 | 40 | 69.2 ± 8.2 | 26.8 ± 3.6 | 63 | |||||
| Moens et al. [65] | 2007 | Belgium (Europe) | Intervention | NI | 20 | RCT crossover | Subjects with acute myocardial infarction | 57 ± 11 | NI | 10 |
| Control | 20 | 56 ± 14 | 15 | |||||||
| Shirodaria et al. [40] | 2007 | United Kingdom (Europe) | Intervention 11 | 56 | 20 | RCT parallel | Subjects with coronary artery disease | 62.2 ± 7.6 | 28.2 ± 4.0 | 25 |
| Intervention 12 | 22 | 62.2 ± 8.0 | 28 ± 3.8 | 9 | ||||||
| Control | 14 | 64 ± 8.6 | 26.9 ± 4.5 | 14.3 | ||||||
| Yilmaz et al. [66] | 2007 | Turkey (Asia) | Intervention 3 | 20 | 20 | RCT parallel | Subjects with elevated plasma homocysteine levels (>15 μmol/L) and unequivocal angiographic evidence of coronary artery disease (>50% stenosis in one or more vessels) | 52.2 ± 11.9 | 27.2 ± 3.8 | 35 |
| Intervention 13 | 20 | 16 | 64.8 ± 9.0 | 27.8 ± 3.8 | 15 | |||||
| Control | 20 | 18 | 65.5 ± 7.6 | 28.3 ± 4 | 10 | |||||
| Austen et al. [28] | 2006 | Australia (Australia) | Intervention | NI | 10 | RCT crossover | Renal transplant recipients | 45.5 ± 11.8 | NI | 30 |
| Control | ||||||||||
| Moat et al. [41] | 2006 | United Kingdom (Europe) | Intervention 11 | NI | 30 | RCT parallel | Subjects with coronary artery disease | 61 ± 7 | 28.5 ± 4.4 | 10 |
| Intervention 12 | 25 | 60 ± 7 | 29.9 ± 4.4 | 16 | ||||||
| Control | 29 | 61 ± 7 | 29.6 ± 4.1 | 13.8 | ||||||
| Olthof et al. [53] | 2006 | Netherlands (Europe) | Intervention | 40 | 39 | RCT crossover | Healthy subjects | 59 ± 5 | 25.2 ± 2.8 | NI |
| Control | ||||||||||
| Solini et al. [62] | 2006 | Italy (Europe) | Intervention | 30 | 30 | RCT parallel | Healthy volunteers with normal glucose tolerance and overweight | 50 ± 7 | 27.5 ± 0.6 | 73.3 |
| Control | 30 | 30 | 49 ± 8 | 27.4 ± 0.6 | 63.3 | |||||
| Spoelstra-de Man et al. [56] a | 2006 | Netherlands (Europe) | Intervention | 28 | 23 | RCT parallel | Subjects with a diabetes mellitus type 2, a fasting homocysteine concentration of ≥14 μmol/L and a urinary albumin-to-creatinine ratio of at least 1 mg/mmol | 64 ± 9 | 29 ± 4 | 39 |
| Control | 23 | 18 | 66 ± 9 | 29 ± 3 | 44 | |||||
| Title et al. [58] | 2006 | Canada (North America) | Intervention | NI | 19 | RCT crossover | Subjects with diabetes mellitus type 2 | 54.5 ± 5.9 | NI | 52.6 |
| Control | ||||||||||
| Zoungas et al. [50] b | 2006 | Australia, New Zealand (Oceania) | Intervention | 355 | 156 | RCT parallel | Subjects with chronic renal failure of any cause | 56 ± 13 | 26 ± 5 | 26.9 |
| Control | 159 | 56 ± 14 | 27± 4 | 37.7 | ||||||
| Mangoni et al. [26] | 2005 | Australia (Australia) | Intervention | NI | 13 | RCT parallel | Subjects with diabetes mellitus type 2 | 55.3 ± 4.3 | 30.5 ± 4.0 | 38.5 |
| Control | 13 | 57.6 ± 4.7 | 32.3 ± 6.5 | 46 | ||||||
| Williams et al. [51] | 2005 | Australia (Australia) | Intervention | NI | 41 | RCT crossover | Subjects with normal or high-normal ambulatory blood pressure (systolic: >130 to <145 mm Hg; diastolic: >80 to <90 mm Hg) | 32 ± 7 | 24 ± 4 | NI |
| Control | ||||||||||
| Durga et al. [57] | 2005 | Netherlands (Europe) | Intervention | 530 | 521 | RCT parallel | Men and postmenopausal women aged 50 to 70 years | 60 ± 5 | 27 ± 3 | 29.9 |
| Control | 60 ± 6 | 27 ± 4 | 26.3 | |||||||
| Doshi et al. [42] * | 2004 | United Kingdom (Europe) | Intervention [31] | 52 | 50 | RCT crossover | Subjects with coronary heart disease | 57 ± 8 | 28.5 ± 4.4 | 12 |
| Control [31] | ||||||||||
| Lekakis et al. [67] | 2004 | Greece (Europe) | Intervention | NI | 17 | RCT parallel | Hypercholesterolaemic subjects taking statins | 55.7 ± 8.3 | NI | 17.6 |
| Control | 17 | 57.3 ± 8.8 | 11.8 | |||||||
| Spoelstra-de Man et al. [54] a | 2004 | Netherlands (Europe) | Intervention | 28 | 23 | RCT parallel | Subjects with a diabetes mellitus type 2, a fasting homocysteine concentration of ≥14 μmol/L and a urinary albumin-to-creatinine ratio of at least 1 mg/mmol | 63.7 ± 8.6 | 29.3 ± 3.9 | 39 |
| Control | 23 | 18 | 66.1 ± 8.5 | 28.8 ± 3.4 | 44 | |||||
| Woodman et al. [29] | 2004 | Australia (Australia) | Intervention | NI | 26 | RCT crossover | Healthy hyperhomocysteinaemic subjects | 49 ± 2 | 28.1 ± 1.0 | 30.8 |
| Control | ||||||||||
| Zoungas et al. [52] b | 2004 | Australia, New Zealand (Australia) | Intervention | NI | 315 | RCT parallel | Subjects with chronic renal failure | 58.2 ± 10.2 | NI | 32.4 |
| Control | 213 | 56.6 ± 13.6 | 33.3 | |||||||
| Doshi et al. [43] * | 2003 | United Kingdom (Europe) | Intervention [31] | NI | 50 | RCT crossover | Subjects with coronary heart disease | 57 ± 8 | 28.5 ± 4.4 | 12 |
| Control [31] | ||||||||||
| Intervention [29] | 33 | RCT parallel | Subjects with coronary heart disease | 56 ± 7 | 28.9 ± 5.99 | 9 | ||||
| Control [29] | ||||||||||
| Doshi et al. [44] | 2002 | United Kingdom (Europe) | Intervention | NI | 16 | RCT parallel | Subjects with coronary heart disease | 56 ± 7 | 28.9 ± 5.99 | 9 |
| Control | 17 | |||||||||
| Mangoni et al. [45] | 2002 | United Kingdom (Europe) | Intervention | NI | 12 | RCT parallel | Chronic cigarette smokers | 39.7 ± 3.4 | 25.7 ± 0.8 | 66.7 |
| Control | 12 | 36.0 ± 3.6 | 24.9 ± 0.9 | 58.3 | ||||||
| Doshi et al. [46] | 2001 | United Kingdom (Europe) | Intervention | 52 | 50 | RCT crossover | Subjects with coronary artery disease | 57 ± 8 | 28.5 ± 4.4 | 12 |
| Control | ||||||||||
| Miner et al. [60] | 2001 | Canada (North America) | Intervention 14 | 37 | 11 | RCT parallel | Cardiac transplant recipients | 55 ± 1 | NI | 9.1 |
| Intervention 3 | 12 | 56 ± 1 | 16.7 | |||||||
| Control | 8 | 48 ± 1 | 14.3 | |||||||
| Pullin et al. [47] | 2001 | United Kingdom (Europe) | Intervention 3 | NI | 42 | RCT crossover | Healthy subjects | 39 ± 12 | NI | 58 |
| Intervention 15 | 42 | |||||||||
| Control | 42 | |||||||||
| Thambyrajah et al. [48] | 2001 | United Kingdom (Europe) | Intervention | 90 | 43 | RCT parallel | Subjects with >50% stenosis in one or more vessels | 63.0 ± 8.2 | 28.6 ± 4.7 | 14 |
| Control | 43 | 63.4 ± 7.2 | 27.2 ± 3.5 | 11.6 | ||||||
| Thambyrajah et al. [49] | 2000 | United Kingdom (Europe) | Intervention | 50 | 47 | RCT parallel | Subjects with chronic renal failure (serum creatinine >130 mmol/L) and a plasma homocysteine concentration >12 mmol/L | 61 (57–64) 16 | 28.2 (26.6–29.8) 16 | 26 |
| Control | 50 | 44 | 62 (59–66) 16 | 27.5 (26.1–28.8) 16 | 28 | |||||
| Title et al. [59] | 2000 | Canada (North America) | Intervention 3 | NI | 25 | RCT parallel | Subjects with coronary artery disease | 57.2 ± 9.8 | NI | 24 |
| Intervention 17 | 25 | 58.8 ± 11.6 | 24 | |||||||
| Control | 25 | 60.6 ± 8.6 | 16 | |||||||
| Wilmink et al. [55] | 2000 | Netherlands (Europe) | Intervention | NI | 20 | RCT crossover | Healthy subjects | 23 ± 3.4 | 21.9 ± 2.7 | 50 |
| Control | 20 | 22.8 ± 2.6 | ||||||||
| Bellamy et al. [37] | 1999 | United Kingdom (Europe) | Intervention | NI | 10 | RCT crossover | Healthy volunteers-blood donors and members of hospital staff | NI | NI | NI |
| Control | 8 | |||||||||
| Woo et al. [38] | 1999 | China (Asia) | Intervention | 17 | RCT crossover | Healthy volunteers who had no history of hypertension, diabetes mellitus, hyperlipidemia, ischemic heart disease or family history of premature atherosclerosis | 54 ± 10 | NI | NI | |
| Kunz et al. [36] | 1999 | France (Europe) | Intervention | 63 | 25 | RCT parallel | Stable chronic haemodialysis patients who did not receive anti-epileptic drugs or other folate antagonists or oestrogens; no vitamin B12 or folate supplementation over the past 12 months | 59 ± 13 | NI | 30 |
| Control | 28 |
| Author | Year | Groups | Characteristic of Intervention | Form | Dose (per Day) | Time of Intervention (Weeks) |
|---|---|---|---|---|---|---|
| Li et al. [39] | 2020 | Intervention | Folic acid + docosahexaenoic acid | Tablets + capsules | 800 μg + 800 mg | 26 |
| Intervention | Folic acid | 800 μg | ||||
| Intervention | Docosahexaenoic acid | 800 mg | ||||
| Control | Placebo (corn starch + soybean oil) | NI | ||||
| Ma et al. [61] | 2019 | Intervention | Folic acid | Tablets | 800 μg | 24 |
| Intervention | Vitamin B12 | 25 µg | ||||
| Intervention | Folic acid + vitamin B12 | 800 μg + 25 µg | ||||
| Control | No intervention | NI | NI | |||
| Grigoletti et al. [63] | 2018 | Intervention | Folinic acid | NI | 5 mg | 4 |
| Intervention | Aerobic exercise training | - | ||||
| Control | Placebo | NI | ||||
| Control | Metformin + placebo | 1700 mg + NI | ||||
| Hoch et al. [64] | 2009 | Intervention | Folic acid | NI | 10 mg | 6 |
| Control | Placebo | NI | ||||
| Khandanpour et al. [27] | 2009 | Intervention | Folic acid | Capsules | 400 μg | 16 |
| Intervention | 5-MTHF | 400 μg | ||||
| Control | Placebo | NI | ||||
| Moens et al. [65] | 2007 | Intervention | Folic acid | NI | 10 mg | 6 |
| Control | Placebo | NI | ||||
| Shirodaria et al. [40] | 2007 | Intervention | Folic acid | NI | 400 μg | 7 |
| Intervention | Folic acid | 5 mg | ||||
| Control | Placebo | NI | ||||
| Yilmaz et al. [66] | 2007 | Intervention | Folic acid | NI | 5 mg | 8 |
| Intervention | N-acetylcysteine | 600 mg | ||||
| Control | Placebo | NI | ||||
| Austen et al. [28] | 2006 | Intervention | Folate | NI | 5 mg | 14 |
| Control | Placebo | NI | ||||
| Moat et al. [41] | 2006 | Intervention | Folic acid | Tablets | 400 μg | 6 |
| Intervention | Folic acid | 5 mg | ||||
| Control | Placebo | NI | ||||
| Olthof et al. [53] | 2006 | Intervention | Folic acid + lactose | NI | 0.8 mg + 6 g | 6 |
| Control | Placebo (lactose) | 6 g | ||||
| Solini et al. [62] | 2006 | Intervention | Folic acid + hypocaloric diet (1400 kcal/day, 55% carbohydrate, 25% protein and 20% fat) | NI | 2.5 mg | 12 |
| Control | Placebo + hypocaloric diet (1400 kcal/day, 55% carbohydrate, 25% protein and 20% fat) | NI | ||||
| Spoelstra-de Man et al. [54,56] a | 2006, 2004 | Intervention | Folic acid | Tablets | 5 mg | 26 |
| Control | Placebo | NI | ||||
| Title et al. [58] | 2006 | Intervention | Folic acid | Capsules | 10 mg | 2 |
| Control | Placebo | NI | ||||
| Zoungas et al. [50] b | 2006 | Intervention | Folic acid | NI | 15 mg | 188 1 |
| Control | Placebo | NI | ||||
| Mangoni et al. [26] | 2005 | Intervention | Folic acid | NI | 5 mg | 4 |
| Control | Placebo | NI | ||||
| Williams et al. [51] | 2005 | Intervention | Folic acid | NI | 5 mg | 3 |
| Control | Placebo | NI | ||||
| Durga et al. [57] | 2005 | Intervention | Folic acid | Capsules | 0.8 mg | 52 |
| Control | Placebo | NI | ||||
| Doshi et al. [42] * | 2004 | Intervention | Folic acid | Tablets | 5 mg | 6 |
| Control | Placebo | NI | ||||
| Lekakis et al. [67] | 2004 | Intervention | Folic acid | NI | 5 mg | 4 |
| Control | Placebo | NI | ||||
| Woodman et al. [29] | 2004 | Intervention | Folic acid | NI | 5 mg | 8 |
| Control | Placebo | NI | ||||
| Zoungas et al. [52] b | 2004 | Intervention | Folic acid | Tablets | 15 mg | 206 |
| Control | Placebo | NI | ||||
| Doshi et al. 2 [43] * | 2003 | Intervention | Folic acid | NI | 5 mg | 6 |
| Control | Placebo | NI | ||||
| Doshi et al. 3 [44] | 2002 | Intervention | Folic acid | NI | 5 mg | 6 |
| Control | Placebo | NI | ||||
| Mangoni et al. [45] | 2002 | Intervention | Folic acid | NI | 5 mg | 4 |
| Control | Placebo | NI | ||||
| Doshi et al. [46] | 2001 | Intervention | Folic acid | Tablets | 5 mg | 6 |
| Control | Placebo | NI | ||||
| Miner et al. [60] | 2001 | Intervention | Pyridoxine | NI | 100 mg | 10 |
| Intervention | Folic acid | 5 mg | ||||
| Control | Placebo | NI | ||||
| Pullin et al. [47] | 2001 | Intervention | Folic acid | Tablets | 400 μg | 17 |
| Intervention | Foods naturally high in folate and folic acid–fortified foods | - | ~400 μg | |||
| Control | Placebo | NI | NI | |||
| Thambyrajah et al. [48] | 2001 | Intervention | Folic acid | NI | 5 mg | 12 |
| Control | Placebo | NI | ||||
| Thambyrajah et al. [49] | 2000 | Intervention | Folic acid | NI | 5 mg | 12 |
| Control | Placebo | NI | ||||
| Title et al. [59] | 2000 | Intervention | Folic acid | Capsules | 5 mg | 17 |
| Intervention | Folic acid + vitamin C + vitamin E | 5 mg + 2 g + 800 IU | ||||
| Control | Placebo | NI | ||||
| Wilmink et al. [55] | 2000 | Intervention | Folic acid | NI | 10 mg | 2 |
| Control | Placebo | NI | ||||
| Bellamy et al. [37] | 1999 | Intervention | Folic acid | NI | 5 mg | 6 |
| Control | Placebo | NI | ||||
| Woo et al. [38] | 1999 | Intervention | Folic acid | NI | 10 mg | 4 |
| Control | Placebo | NI | ||||
| Kunz et al. [36] | 1999 | Intervention | Folic acid | NI | 10 mg | 8 |
| Control | Placebo | NI | ||||
| Control | No intervention | NI |
| Author | Year | Group | FMD (%) | PWV (m/s) | Alx (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Changes (%) | Pre | Post | Changes (%) | Pre | Post | Changes (%) | |||
| Grigoletti et al. [63] | 2018 | Intervention 1 | NI | NI | 7.33 ± 2.44 3−5 | NI | NI | NI | NI | NI | NI |
| Intervention 2 | 0.04 ± 0.83 3−5 | ||||||||||
| Control | 6.54 ± 0.91 3−5 | ||||||||||
| Hoch et al. [64] | 2009 | Intervention | 6.6 ± 0.8 3 | 10.0 ± 0.9 3 | 3.5 ± 0.6 3 | NI | NI | NI | NI | NI | NI |
| Control | 6.5 ± 0.7 3 | 6.65 ± 0.7 3 | 0.11 ± 0.2 3 | ||||||||
| Khandanpour et al. [27] | 2009 | Intervention | NI | NI | NI | 10.60 (8.30–13.90) 6,7 9.40 (7.70–12.50) 6,8 | NI | −0.90 (−2.10, 0.00) 6,7,9 −0.50 (−1.50, 0.30) 6,8,9 | NI | NI | NI |
| Control | 11.55 (9.95–15.60) 6,7 9.80 (8.15–12.00) 6,8 | ||||||||||
| Moens et al. [65] | 2007 | Intervention | 3.98 ± 0.35 3 | 6.44 ± 0.56 3 | NI | NI | NI | NI | NI | NI | NI |
| Control | 4.01 ± 0.34 3 | 4.46 ± 0.38 3 | |||||||||
| Shirodaria et al. [40] | 2007 | Intervention 10 | 7.71 ± 1.26 3,5 | 11.95 ± 1.53 3,5 | NI | 9.03 ± 1.023,12 | 7.62 ± 0.78 3,12 | –1.41 ± 0.48 3,12 | NI | NI | NI |
| Intervention 11 | 7.90 ± 1.28 3,5 | 13.12 ± 1.7 3,5 | 8.50 ± 0.613,12 | 7.33 ± 0.51 3,12 | –1.17 ± 0.47 3,12 | ||||||
| Control | 9.71 ± 1.02 3,5 | 7.19 ± 1.52 3,5 | 7.93 ± 0.713,12 | 8.22 ± 0.90 3,12 | 0.29 ± 0.35 3,12 | ||||||
| Yilmaz et al. [66] | 2007 | Intervention 1 | 5.3 ± 2.2 14 | 12.0 ± 6.3 14 | 6.7 15 | NI | NI | NI | NI | NI | NI |
| Intervention13 | 6.0 ± 2.4 14 | 10.4 ± 3.2 14 | 4.4 15 | ||||||||
| Control | 5.8 ± 1.9 14 | 6.1 ± 2.7 14 | 0.3 15 | ||||||||
| Moat et al. [41] | 2006 | Intervention 10 | 27.3 ± 54.5 14,16 | 39.3 ± 31.9 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Intervention 11 | 24.4 ± 26.3 14,16 | 99.6 ± 35.7 14,16 | |||||||||
| Control | 20.3 ± 31.0 14,16 | 33.5 ± 21.6 14,16 | |||||||||
| Olthof et al. [53] | 2006 | Intervention | NI | 2.8 ± 1.9 14 | NI | NI | NI | NI | NI | NI | NI |
| Control | 2.8 ± 1.8 14 | ||||||||||
| Title et al. [58] | 2006 | Intervention | NI | 5.8 ± 4.8 14 | NI | NI | NI | NI | NI | NI | NI |
| Control | NI | 3.2 ± 2.7 14 | |||||||||
| Zoungas et al. [50] b | 2006 | Intervention | NI | NI | NI | –0.31 (–1.20–0.57) 9,17,18 | 0.1 (–5.3–5.5) 9,18 | ||||
| Control | |||||||||||
| Mangoni et al. [26] | 2005 | Intervention | NI | NI | NI | 10.1 ± 0.6 3,19 10.8 ± 0.7 3,20 | NI | +0.7 ± 0.6 3,9,19 −0.1 ± 0.6 3,9,20 | NI | NI | NI |
| Control | 10.0 ± 0.6 3,19 10.9 ± 0.8 3,20 | +0.1 ± 0.4 3,9,19 +0.3 ± 0.4 3,9,20 | |||||||||
| Williams et al. [51] | 2005 | Intervention | NI | NI | NI | 7.2 ± 0.9 14,20 10.6 ± 1.5 14,21 | NI | –0.09 ± 0.21 9,14,21 –0.10 ± 0.11 9,14,20 | NI | NI | NI |
| Control | 0.19 ± 0.25 9,14,21 0.09 ± 0.10 9,14,20 | ||||||||||
| Doshi et al. [42] * | 2004 | Intervention | 52 ± 34 14,16 | 110 ± 43 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Control | 46 ± 33 14,16 | 47 ± 35 14,16 | |||||||||
| Lekakis et al. [67] | 2004 | Intervention | 4.7 ± 3.2 14 | 7.1 ± 3.1 14 | NI | NI | NI | NI | NI | NI | NI |
| Control | 5.7 ± 3.8 14 | 5.6 ± 2.2 14 | |||||||||
| Woodman et al. [29] | 2004 | Intervention | 7.5 ± 1.1 3 | 8.7 ± 1.3 3 | +1.2 ± 1.1 3 | NI | NI | NI | NI | NI | NI |
| Control | 6.5 ± 0.7 3 | 5.3 ± 0.7 3 | −1.2 ± 0.6 3 | ||||||||
| Zoungas et al. [52] b | 2004 | Intervention | NI | NI | NI | NI | 11.0 ± 3.714,17,22 10.2 ± 3.114,17,23 10.5 ± 1.8 14,22,24 10.2 ± 2.014,23,24 | NI | NI | 21.4 ± 11.6 14,22 25.2 ± 11.5 14,23 | NI |
| Control | 9.4 ± 1.8 14,17,22 8.6 ± 1.7 14,17,23 10.8 ± 1.5 14,22,24 10.2 ± 1.6 14,23,24 | 12.0 ± 9.3 14,22 20.4 ± 9.9 14,23 | |||||||||
| Doshi et al. [43] *,25 | 2003 | Intervention | 52 ± 34 14,16 | 110 ± 43 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Control | 46 ± 33 14,16 | 47 ± 35 14,16 | |||||||||
| Doshi et al. [44] 26 | 2002 | Intervention | 52.5 ± 29 14,16 | 111 ± 28 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Control | 48 ± 24 14,16 | 52 ± 19 14,16 | |||||||||
| Mangoni et al. [45] | 2002 | Intervention | NI | NI | NI | 8.4 ± 0.3 3,20 | 7.8 ± 0.4 3,20 | NI | NI | NI | NI |
| Control | 8.3 ± 0.5 3,20 | 7.8 ± 0.3 3,20 | |||||||||
| Doshi et al. [46] | 2001 | Intervention | 52 ± 34 14,16 | 110 ± 43 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Control | 46 ± 33 14,16 | 47 ± 35 14,16 | |||||||||
| Miner et al. [60] | 2001 | Intervention 27 | 2.9 ± 6.7 14 | 6.9 ± 6.3 14 | 4.0 ± 7.6 14 | NI | NI | NI | NI | NI | NI |
| Intervention 1 | 5.9 ± 8.3 14 | 3.1 ± 4.8 14 | −5.1 ± 8.6 14 | ||||||||
| Control | 7.1 ± 5.9 14 | 2.0 ± 7.7 14 | −2.8 ± 9.2 14 | ||||||||
| Pullin et al. [47] | 2001 | Intervention 1 | 98 ± 73 14,16 | 114 ± 59 14,16 | NI | NI | NI | NI | NI | NI | NI |
| Intervention 28 | 110 ± 67 14,16 | ||||||||||
| Control | 118 ± 68 14,16 | ||||||||||
| Thambyrajah et al. [48] | 2001 | Intervention | 3.3 (2.2–4.3) 18 | 4.5 (3.5–5.4) 18 | 1.2 (0.7–1.8) 18 | NI | NI | NI | NI | NI | NI |
| Control | 3.8 (2.6–4.9) 18 | 4.1 (3.2–5.1) 18 | 0.4 (–0.3–1.1) 18 | ||||||||
| Thambyrajah et al. [49] | 2000 | Intervention | 3.7 (2.8–4.6) 18 | 4.3 (3.5–5.2) 18 | NI | NI | NI | NI | NI | NI | NI |
| Control | 2.6 (1.7–3.5) 18 | 3.9 (2.9–5.0) 18 | |||||||||
| Title et al. [59] | 2000 | Intervention 1 | 3.2 ± 3.6 14 | 5.2 ± 3.9 14 | NI | NI | NI | NI | NI | NI | NI |
| Intervention 29 | 2.6 ± 2.4 14 | 4.0 ± 3.7 14 | |||||||||
| Control | 2.7 ± 3.3 14 | 2.9 ± 3.7 14 | |||||||||
| Wilmink et al. [55] | 2000 | Intervention | 9.6 (7.1–12.8) 6 | 9.9 (7.5–14.1) 6 | NI | NI | NI | NI | NI | NI | NI |
| Control | 10.6 (8.3–12.2) 6 | 5.8 (3.0–10.2) 6 | |||||||||
| Bellamy et al. [37] | 1999 | Intervention | 24 ± 17 3,30 | 21 ± 14 3,30 | +50 ± 30 3,30 | NI | NI | NI | NI | NI | NI |
| Control | 26 ± 21 3,30 | +60 ± 53 3,30 | |||||||||
| Woo et al. [38] | 1999 | Intervention | 5.7 ± 1.2 14 | 8.2 ± 1.6 14 | NI | NI | NI | NI | NI | NI | NI |
| Control | 6.0 ± 1.3 14 | ||||||||||
| Author | Year | Group | ADMA (μmol/L) | sVCAM-1 (ng/mL) | ICAM-1 (ng/mL) | MCP-1 (pg/mL) | PAI-1 (ng/L) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Changes (%) | Pre | Post | Changes (%) | Pre | Post | Changes (%) | Pre | Post | Changes (%) | Pre | Post | Changes (%) | |||
| Li et al. [39] | 2020 | Intervention 1 | NI | NI | NI | NI | NI | NI | NI | NI | NI | 316.64 ± 97.65 4 | 230.63 ± 61.81 4 | −86.02 ± 87.30 4 | NI | NI | NI |
| Intervention 2 | 327.39 ± 116.91 4 | 251.38 ± 88.90 4 | −76.01 ± 96.99 4 | NI | NI | NI | |||||||||||
| Intervention 3 | 311.01 ± 83.49 4 | 242.02 ± 87.39 4 | −68.99 ± 77.34 4 | NI | NI | NI | |||||||||||
| Control | 310.97 ± 115.78 4 | 306.04 ± 82.41 4 | −4.94 ± 126.34 4 | NI | NI | NI | |||||||||||
| Ma et al. [61] | 2019 | Intervention 1 | NI | NI | NI | NI | NI | NI | NI | NI | NI | 802.27 ± 6.74 4 | 783.76 ± 3.45 4 | NI | NI | NI | NI |
| Intervention 5 | 805.99 ± 3.65 4 | 796.32 ± 3.59 4 | NI | NI | NI | ||||||||||||
| Intervention 6 | 804.97 ± 6.24 4 | 747.18 ± 3.83 4 | NI | NI | NI | ||||||||||||
| Control | 798.77 ± 7.66 4 | 796.44 ± 7.50 4 | NI | NI | NI | ||||||||||||
| Austen et al. [28] | 2006 | Intervention | 0.41 ± 0.25 4 | 0.33 ± 0.08 4 | –19.8 ± 17.6 4 | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI |
| Control | 0.58 ± 0.23 4 | 0.48 ± 0.25 4 | +8.2 ± 70.3 4 | NI | NI | NI | |||||||||||
| Solini et al. [62] | 2006 | Intervention | NI | NI | NI | NI | NI | NI | NI | NI | NI | 290 ± 85 4 | 247 ± 86 4 | NI | NI | NI | NI |
| Control | 304 ± 71 4 | 316 ± 73 4 | NI | NI | NI | ||||||||||||
| Spoelstra-de Man et al. [56] a | 2006 | Intervention | 0.50 ± 0.08 4 | 0.5 (0.44–0.55) 7,8 | −0.7 9 | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI |
| Control | 0.50 ± 0.07 4 | 0.49 (0.42–0.56) 7,8 | −0.2 9 | NI | NI | NI | |||||||||||
| Title et al. [58] | 2006 | Intervention | NI | NI | NI | 568.5 (486.4–664.5) 10 | 557.8 (465.9–671.2) 10 | NI | 241.5 (222.5–262.2) 10 | 230.2 (212.5–249.4)10 | NI | NI | NI | NI | NI | NI | NI |
| Control | 544.6 (462.2–641.6) 10 | 543.5 (457.6–645.5) 10 | 230.9 (214.4–248.6) 10 | 226.8 (212.3–242.3) 10 | NI | NI | NI | ||||||||||
| Durga et al. [57] | 2005 | Intervention | NI | NI | NI | NI | NI | NI | 139 (118–160) 7 | 139 (119–161) 7 | NI | NI | NI | NI | NI | NI | NI |
| Control | 139 (114–165) 7 | 139 (118–170) 7 | NI | ||||||||||||||
| Spoelstra-de Man et al. [54] a | 2004 | Intervention | NI | NI | NI | 1347 (1070–1640) 7 | NI | −1 (−33–25) 11 | 668 (598–865) 7 | NI | 0 (−45–64) 11 | NI | NI | NI | NI | NI | NI |
| Control | 1399 (1078–1576) 7 | −1 (−41–79) 11 | 797 (513–1046) 7 | 2 (−29–71) 11 | NI | NI | NI | ||||||||||
| Kunz et al. [36] | 1999 | Intervention | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | 13.5 ± 13.5 4 | 10.9 ± 4.3 4 | NI |
| Control | 14.5 ± 11.5 4 | 17.8 ± 12.9 4 | NI | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bokayeva, K.; Jamka, M.; Banaszak, M.; Makarewicz-Bukowska, A.; Adamczak, A.; Chrobot, M.; Janicka, A.; Jaworska, N.; Walkowiak, J. The Effect of Folic Acid Supplementation on Endothelial Function and Arterial Stiffness Markers in Adults: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 2524. https://doi.org/10.3390/healthcare11182524
Bokayeva K, Jamka M, Banaszak M, Makarewicz-Bukowska A, Adamczak A, Chrobot M, Janicka A, Jaworska N, Walkowiak J. The Effect of Folic Acid Supplementation on Endothelial Function and Arterial Stiffness Markers in Adults: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(18):2524. https://doi.org/10.3390/healthcare11182524
Chicago/Turabian StyleBokayeva, Kamila, Małgorzata Jamka, Michalina Banaszak, Aleksandra Makarewicz-Bukowska, Ada Adamczak, Maria Chrobot, Adrianna Janicka, Natalia Jaworska, and Jarosław Walkowiak. 2023. "The Effect of Folic Acid Supplementation on Endothelial Function and Arterial Stiffness Markers in Adults: A Systematic Review and Meta-Analysis" Healthcare 11, no. 18: 2524. https://doi.org/10.3390/healthcare11182524
APA StyleBokayeva, K., Jamka, M., Banaszak, M., Makarewicz-Bukowska, A., Adamczak, A., Chrobot, M., Janicka, A., Jaworska, N., & Walkowiak, J. (2023). The Effect of Folic Acid Supplementation on Endothelial Function and Arterial Stiffness Markers in Adults: A Systematic Review and Meta-Analysis. Healthcare, 11(18), 2524. https://doi.org/10.3390/healthcare11182524