
The Key Role of Empathy in the Relationship between Age and Social Support




Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Instruments
2.2.1. Social Support Measures
2.2.2. Empathy Measures
2.3. Procedure
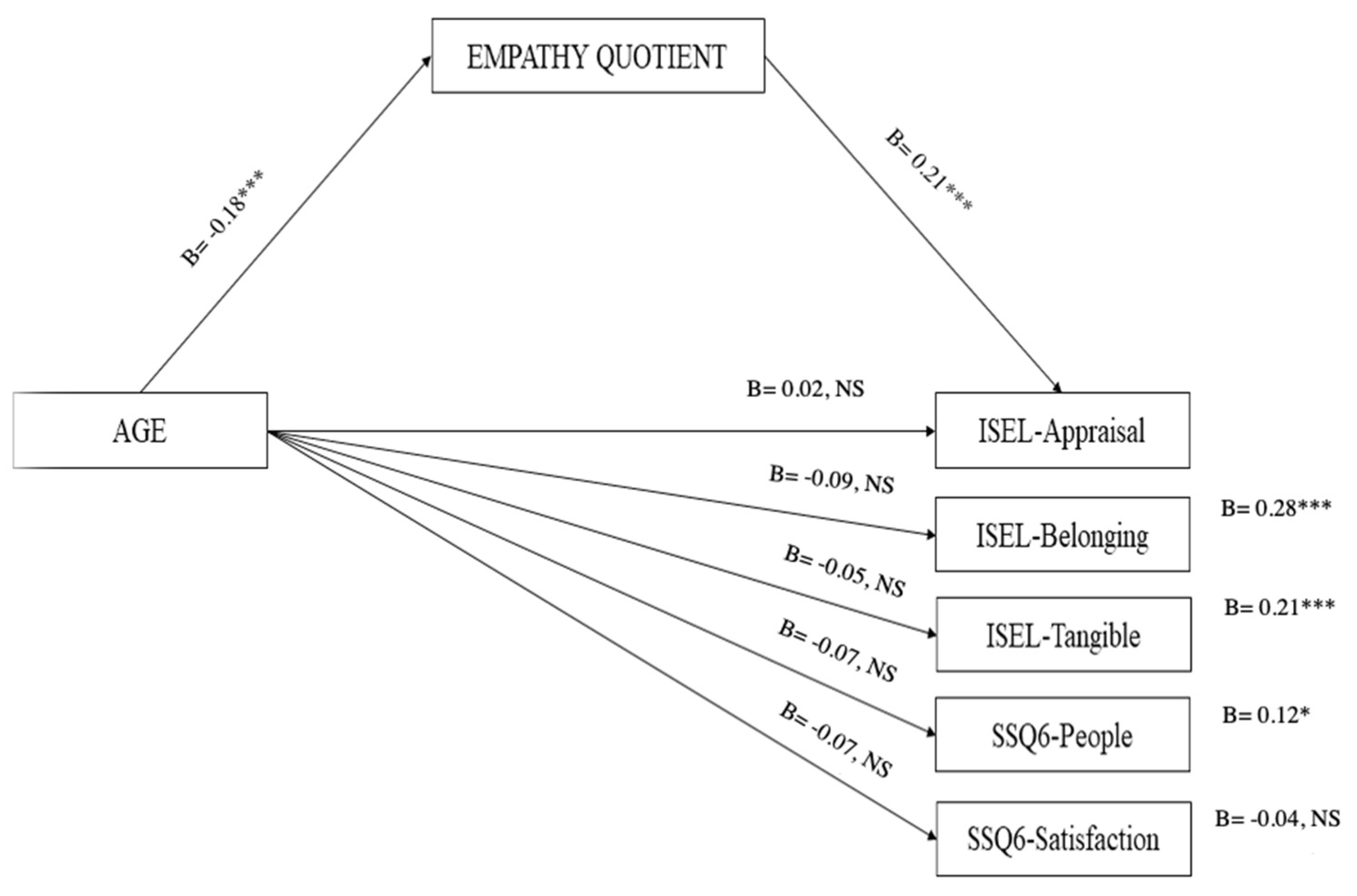
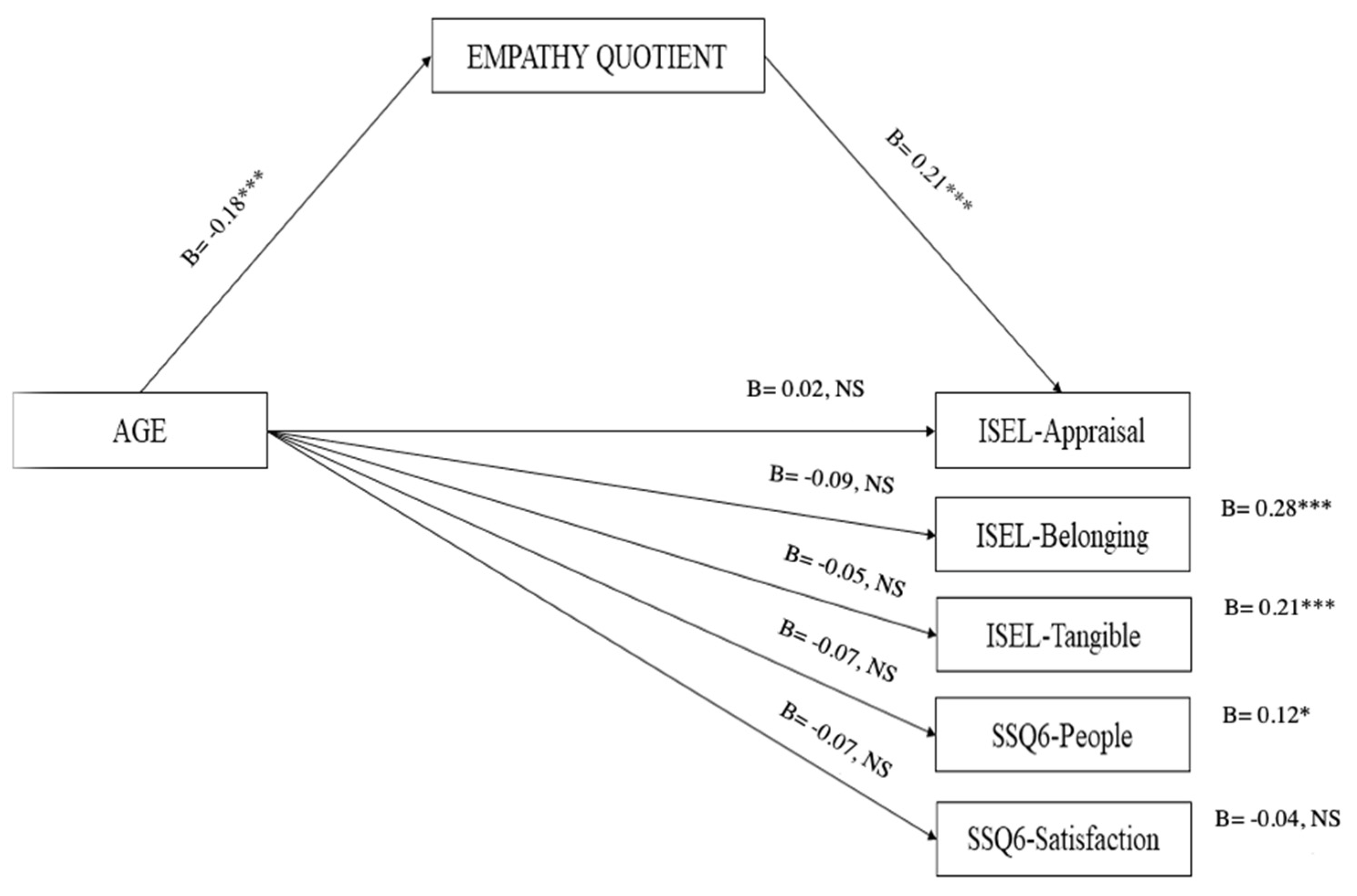
3. Statistical Analysis and Results
4. Discussion
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finfgeld-Connett, D. Clarification of social support. J. Nurs. Scholarsh. 2005, 37, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E. Social support: A review. In Oxford Library of Psychology, The Oxford Handbook of Health Psychology; Friedman, H.S., Ed.; Oxford University Press: Oxford, UK, 2011; pp. 189–214. [Google Scholar]
- Alemán-Ruíz, I.; Calvo-Francés, F. Validation of the Interpersonal Support Links Scale VIDA. Ann. Psychol. 2017, 33, 168–179. [Google Scholar] [CrossRef]
- Stallman, H. Embedding resilience within the tertiary curriculum: A feasibility study. High. Educ. Res. Dev. 2011, 30, 121–133. [Google Scholar] [CrossRef]
- Xerri, M.J.; Radford, K.; Shacklock, K. Student engagement in academic activities: A social support perspective. High. Educ. 2018, 75, 589–605. [Google Scholar] [CrossRef]
- Helgeson, V.S. Two important distinctions in social support: Kind of support and perceived versus received. J. Appl. Soc. Psychol. 1993, 23, 825–845. [Google Scholar] [CrossRef]
- Norris, F.H.; Kaniasty, K. Received and perceived social support in times of stress: A test of the social support deterioration deterrence model. J. Personal. Soc. Psychol. 1996, 71, 498–511. [Google Scholar] [CrossRef]
- Wethington, E.; Kessler, R.C. Perceived support, received support, and adjustment to stressful life events. J. Health Soc. Behavior 1986, 27, 78–89. [Google Scholar] [CrossRef]
- Cohen, S.; Gottlieb, B.H.; Underwood, L.G. Social relationships and health. In Social Support and Health; Cohen, S., Underwood, L.G., Gottlieb, B.H., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 3–25. [Google Scholar]
- Lau, E.Y.H.; Chan, K.K.S.; Lam, C.B. Social Support and Adjustment Outcomes of First-Year University Students in Hong Kong: Self-Esteem as a Mediator. J. Coll. Stud. Dev. 2018, 59, 129–134. [Google Scholar] [CrossRef]
- Schulz, R.; Heckhausen, J. A life span model of successful aging. Am. Psychol. 1996, 51, 702–714. [Google Scholar] [CrossRef]
- Piccardi, L.; Pecchinenda, A.; Palmiero, M.; Giancola, M.; Boccia, M.; Giannini, A.M.; Guariglia, C. Successful aging through physical activity. Front. Hum. Neurosci. 2023. submitted. [Google Scholar]
- English, T.; Carstensen., L.L. Socioemotional selectivity theory. In Encyclopedia of Geropsychology; Pachana, N., Ed.; Springer: Singapore, 2016. [Google Scholar] [CrossRef]
- Pecchinenda, A.; Yankouskaya, A.; Boccia, M.; Piccardi, L.; Guariglia, C.; Giannini, A.M. Exploring the relationship between perceived loneliness and subjective cognitive decline in older individuals. Aging Ment. Health 2023, 1–10. [Google Scholar] [CrossRef]
- Lang, F.R.; Carstensen, L.L. Time counts: Future time perspective, goals, and social relationships. Psychol. Aging 2002, 17, 125–139. [Google Scholar] [CrossRef]
- Wrzus, C.; Hänel, M.; Wagner, J.; Neyer, F.J. Social network changes and life events across the life span: A meta-analysis. Psychol. Bull. 2013, 139, 53–80. [Google Scholar] [CrossRef]
- Ha, J.H. The effects of positive and negative support from children on widowed older adults’ psychological adjustment: A longitudinal analysis. Gerontologist 2010, 50, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Kasper, J.D. Caregivers of frail elders: Updating a national profile. Gerontologist 2006, 46, 344–356. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S. The Empathy Quotient (EQ): An investigation of adults with Asperger syndrome or high functioning autism and normal sex differences. J. Autism Dev. Disord. 2004, 4, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J.; Perry, D. Two systems for empathy: A double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 2009, 132, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Shamay-Tsoory, S.G. The neural bases for empathy. Neuroscientist 2011, 17, 18–24. [Google Scholar] [CrossRef]
- Abramson, L.; Uzefovsky, F.; Toccaceli, V.; Knafo-Noam, A. The genetic and environmental origins of emotional and cognitive empathy: Review and meta-analyses of twin studies. Neurosci. Biobehav. Rev. 2020, 114, 113–133. [Google Scholar] [CrossRef] [PubMed]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J. Dissociable prefrontal network for cognitive and affective theory of mind: A lesion study. Neuropsychologia 2007, 45, 3054–3067. [Google Scholar] [CrossRef]
- Dziobek, I.; Rogers, K.; Fleck, S.; Bahnemann, M.; Heekeren, H.R.; Wolf, O.T.; Convit, A. Dissociation of cognitive and emotioinal empathy in adults with asperger syndrome using the multifaceted empathy test (MET). J. Autism Dev. Disord. 2008, 38, 464–473. [Google Scholar] [CrossRef]
- Guariglia, P.; Piccardi, L.; Giaimo, F.; Alaimo, S.; Miccichè, G.; Antonucci, G. The eyes test is influenced more by artistic inclination and less by sex. Front. Hum. Neurosci. 2015, 22, 292. [Google Scholar] [CrossRef]
- Beadle, J.N.; Sheehan, A.H.; Dahlben, B.; Gutchess, A.H. Aging, empathy, and prosociality. J. Gerontol. B Psychol. Sci. Soc. Sci. 2013, 70, 215–224. [Google Scholar] [CrossRef]
- Bailey, P.E.; Henry, J.D.; Von Hippel, W. Empathy and social functioning in late adulthood. Aging Ment. Health 2008, 12, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Tully, E.C.; Ames, A.M.; Garcia, S.E.; Donohue, M.R. Quadratic associations between empathy and depression as moderated by emotion dysregulation. J. Psychol. 2016, 150, 15–35. [Google Scholar] [CrossRef] [PubMed]
- Beadle, J.N.; de la Vega, C.E. Impact of Aging on Empathy: Review of Psychological and Neural Mechanisms. Front. Psychiatry 2019, 10, 331. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen, C.C.; Decety, J.; Cheng, Y. Aging is associated with changes in the neural circuits underlying empathy. Neurobiol. Aging 2014, 35, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.D.; Phillips, L.H.; Ruffman, T.; Bailey, P.E. A meta-analytic review of age differences in theory of mind. Psychol. Aging 2013, 28, 826. [Google Scholar] [CrossRef]
- Fischer, A.L.; Rourke, N.O.; Thornton, W.L. Age differences in cognitive and affective theory of mind: Concurrent contributions of neurocognitive performance, sex, and pulse pressure. J. Gerontol. Psychol. Sci. 2017, 72, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Warrier, V.; Grasby, K.; Uzefovsky, F.; Toro, R.; Smith, P.; Chakrabarti, B.; Khadake, J.; Mawbey-Adamson, E.; Litterman, N.; Hottenga, J.J.; et al. Genome-wide meta-analysis of cognitive empathy: Heritability, and correlates with sex, neuropsychiatric conditions and cognition. Mol. Psychiatry 2018, 23, 1402–1409. [Google Scholar] [CrossRef]
- Roth-Hanania, R.; Davidov, M.; Zahn-Waxler, C. Empathy development from 8 to 16 months: Early signs of concern for others. Infant Behav. Dev. 2011, 34, 447–458. [Google Scholar] [CrossRef]
- Van der Graaff, J.; Branje, S.; De Wied, M.; Hawk, S.; Van Lier, P.; Meeus, W. Perspective taking and empathic concern in adolescence: Gender differences in developmental changes. Dev. Psychol. 2014, 50, 881–888. [Google Scholar] [CrossRef]
- Tousignant, B.; Eugene, F.; Jackson, P.L. A developmental perspective on the neural bases of human empathy. Infant Behave. Dev. 2017, 48, 5–12. [Google Scholar] [CrossRef]
- Labouvie-Vief, G. Cognition and equilibrium regulation in development and aging. Restor. Neurol. Neurosci. 2009, 27, 551–565. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Konrath, S.H.; Grühn, D.; Hagen, A.L. Empathic concern and perspective taking: Linear and quadratic effects of age across the adult life span. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 68, 168–175. [Google Scholar] [CrossRef]
- Gutiérrez-Cobo, M.; Cabello, R.; Megías-Robles, A.; Gómez-Leal, R.; Baron-Cohen, S.; Fernández-Berrocal, P. Does our cognitive empathy diminish with age? The moderator role of educational level. Int. Psychogeriatr. 2023, 35, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Cuff, B.; Brown, S.J.; Taylor, L.; Howat, D. Empathy: A review of the concept. Emot. Rev. 2016, 8, 144–153. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the mind in the eyes” test revised version: A study with normal adults and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, I.; Rutanen, T.; Luciani, R.S.; Jola, C. Feeling for the Other with Ease: Prospective Actors Show High Levels of Emotion Recognition and Report Above Average Empathic Concern, but Do Not Experience Strong Distress. Front. Psychol. 2021, 1, 543846. [Google Scholar] [CrossRef]
- Betzler, M. The relational value of empathy. Int. J. Philos. Stud. 2019, 27, 136–161. [Google Scholar] [CrossRef]
- Hu, T.; Zheng, X.; Huang, M. Absence and presence of human interaction: The relationship between loneliness and empathy. Front. Psychol. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-mental state examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. Basic Psychometrics for the ISEL-12. 2008. Available online: http://www.psy.cmu.edu/~scohen/scales.html (accessed on 24 February 2012).
- Kim, D.H.; Lee, H.K.; Kim, J.W.; Lee, K. Reliability and Validity of the Korean Version of Interpersonal Support Evaluation List-12 (ISEL-12). J. Korean Neuropsychiatr. Assoc. 2012, 51, 416–421. [Google Scholar] [CrossRef]
- Merz, E.L.; Roesch, S.; Malcarne, V.L.; Penedo, F.; Llabre, M.; Weitzman, O.B.; Navas-Nacher, E.L.; Perreira, K.; Gonzalez, F.; Ponguta, L.A.; et al. Validation of Interpersonal Support Evaluation List-12 (ISEL-12) Scores Among English-and Spanish-Speaking Hispanics/Latinos From the HCHS/SOL Sociocultural Ancillary Study. Psychol. Assess. 2014, 26, 384–394. [Google Scholar] [CrossRef]
- Sarason, I.G.; Sarason, B.R.; Shearin, E.N.; Pierce, G.R. A Brief Measure of Social Support: Practical and Theoretical Implications. J. Soc. Pers. Relatsh. 1987, 4, 497–510. [Google Scholar] [CrossRef]
- Friedman, L.E.; Manriquez Prado, A.K.; Santos Malavé, G.F.; Vélez, J.C.; Gillibrand Esquinazi, R.W.; Sanchez, S.E.; Zhong, Q.Y.; Gelaye, B.; Williams, M.A. Construct validity and factor structure of a Spanish-language Social Support Questionnaire during early pregnancy. Int. J. Womens Health 2018, 10, 379–385. [Google Scholar] [CrossRef]
- Lawrence, E.J.; Shaw, P.; Baker, D.; Baron-Cohen, S.; David, A.S. Measuring empathy: Reliability and validity of the Empathy Quotient. Psychol. Med. 2004, 34, 911–919. [Google Scholar] [CrossRef]
- Vellante, M.; Baron-Cohen, S.; Melis, M.; Marrone, M.; Petretto, D.R.; Masala, C.; Preti, A. The ‘‘reading the mind in the eyes’’ test: Systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 2013, 18, 326–354. [Google Scholar] [CrossRef]
- Kittel, A.F.D.; Olderbak, S.; Wilhelm, O. Sty in the Mind’s Eye: A Meta-Analytic Investigation of the Nomological Network and Internal Consistency of the “Reading the Mind in the Eyes” Test. Assessment 2022, 29, 872–895. [Google Scholar] [CrossRef]
- Mertler, C.A.; Vannatta, R.A. Advanced and Multivariate Statistical Methods: Practical Application and Interpretation (3.Basm); Pyrczak Publishing: Glendale, CA, USA, 2005. [Google Scholar]
- Giancola, M. Who complies with prevention guidelines during the fourth wave of COVID-19 in Italy? An empirical study. Personal Individ. Diff. 2022, 199, 111845. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Bollen, K.A.; Stine, R. Direct and indirect effects: Classical and bootstrap estimates of variability. Sociol. Methodol. 1990, 20, 115–140. [Google Scholar] [CrossRef]
- Giancola, M.; Palmiero, M.; D’Amico, S. Social sustainability in late adolescence: Trait Emotional Intelligence mediates the impact of the Dark Triad on Altruism and Equity. Front. Psychol. 2022, 13, 840113. [Google Scholar] [CrossRef] [PubMed]
- Dermody, N.; Wong, S.; Ahmed, R.; Piguet, O.; Hodges, J.R.; Irish, M. Uncovering the neural bases of cognitive and affective empathy deficits in Alzheimer’s disease and the behavioral-variant of frontotemporal dementia. J. Alzheimers Dis. 2016, 53, 801–816. [Google Scholar] [CrossRef] [PubMed]
- Eslinger, P.J.; Moore, P.; Anderson, C.; Grossman, M. Social cognition, executive functioning, and neuroimaging correlates of empathic deficits in frontotemporal dementia. Neuropsychiatry Clin. Neurosci. 2011, 23, 74–82. [Google Scholar] [CrossRef]
- Gouveia, V.V.; Milfont, T.L.; Gouveia, R.S.; Neto, J.R.; Galvão, L. Brazilian-portuguese empathy quotient: Evidences of its construct validity and reliability. Span. J. Psychol. 2012, 15, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Schieman, S.; Van Gundy, K. The personal and social links between age and self-reported empathy. Soc. Psychol. Q 2000, 63, 152–174. [Google Scholar] [CrossRef]
- Voracek, M.; Dressler, S.G. Lack of correlation between digit ratio (2D:4D) and Baron-Cohen’s “Reading the Mind in the Eyes” test, empathy, systemising, and autism-spectrum quotients in a general population sample. Personal. Individ. Differ. 2006, 41, 1481–1491. [Google Scholar] [CrossRef]
- Olderbak, S.; Wilhelm, O.; Olaru, G.; Geiger, M.; Brenneman, M.W.; Roberts, R.D. A psychometric analysis of the reading the mind in the eyes test: Toward a brief form for research and applied settings. Front. Psychol. 2015, 6, 1503. [Google Scholar] [CrossRef]
- Dodell-Feder, D.; Ressler, K.J.; Germine, L.T. Social cognition or social class and culture? On the interpretation of differences in social cognitive performance. Psychol. Med. 2020, 50, 133–145. [Google Scholar] [CrossRef]
- Richter, D.; Kunzmann, U. Age differences in three facets of empathy: Performance-based evidence. Psychol. Aging 2011, 26, 60–70. [Google Scholar] [CrossRef]
- Riva, F.; Tschernegg, M.; Chiesa, P.A.; Wagner, I.C.; Kronbichler, M.; Lamm, C.; Silani, G. Age-related differences in the neural correlates of empathy for pleasant and unpleasant touch in a female sample. Neurobiol. Aging 2018, 65, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.K.; Perceval, G.; Davies, I.; Su, P.; Huang, J.; Meinze, M. Visual Perspective taking in young and older adults. J. Exp. Psychol. Gen. 2019, 148, 2006–2026. [Google Scholar] [CrossRef] [PubMed]
- Stepien, K.A.; Baernstein, A. Educating for empathy: A review. J. Gen. Intern. Med. 2006, 21, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Kelm, Z.; Womer, J.; Walter, J.K.; Feudtner, C. Interventions to cultivate physician empathy: A systematic review. BMC Med. Educ. 2014, 14, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Iwase, T.; Ogawa, H.; Mahmood, S.; Sato, M.; DeSantis, J.; Gonnella, J.S. Can communication skills training improve empathy? A six-year longitudinal study of medical students in Japan. Med. Teach. 2018, 22, 1–6. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]
- Ricciardi, E.; Spano, G.; Tinella, L.; Lopez, A.; Clemente, C.; Bosco, A.; Caffò, A.O. Perceived social support mediates the relationship between use of greenspace and geriatric depression: A cross-sectional study in a sample of south-Italian older adults. Int. J. Environ. Res. Public Health 2023, 20, 5540. [Google Scholar] [CrossRef]

{kind=link}
| Mean (SD) | Age | Gender | Edu. | EQ | RMET | ISEL-12-A | ISEL-12-B | ISEL-12-T | SSQ6-P | SSQ6-S | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 42.17 (16.75) | 1 | |||||||||
| Gender | --- | −0.017 | 1 | ||||||||
| Edu | 7.45 (3.02) | −0.194 ** | 0.014 | 1 | |||||||
| EQ | 44.24 (12.04) | −0.170 ** | 0.161 ** | 0.066 | 1 | ||||||
| RMET | 21.94 (5.10) | −0.186 ** | 0.088 | −0.038 | 0.068 | 1 | |||||
| ISEL-12-A | 12.61 (2.81) | −0.093 | 0.093 | 0.007 | 0.305 ** | 0.024 | 1 | ||||
| ISEL-12-B | 12.63 (2.32) | −0.160 ** | −0.035 | −0.021 | 0.312 ** | 0.023 | 0.502 ** | 1 | |||
| ISEL-12-T | 13.13 (2.23) | −0.111 * | −0.027 | −0.020 | 0.242 ** | −0.015 | 0.565 ** | 0.586 ** | 1 | ||
| SSQ6-P | 22.42 (10.81) | 0.011 | 0.028 | −0.017 | 0.136 ** | 0.017 | 0.253 ** | 0.090 | 0.143 ** | 1 | |
| SSQ6-S | 7.45 (7.49) | 0.089 | 0.076 | −0.008 | 0.168 ** | 0.091 | 0.265 ** | 0.241 ** | 0.225 ** | 0.193 ** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guariglia, P.; Palmiero, M.; Giannini, A.M.; Piccardi, L. The Key Role of Empathy in the Relationship between Age and Social Support. Healthcare 2023, 11, 2464. https://doi.org/10.3390/healthcare11172464
Guariglia P, Palmiero M, Giannini AM, Piccardi L. The Key Role of Empathy in the Relationship between Age and Social Support. Healthcare. 2023; 11(17):2464. https://doi.org/10.3390/healthcare11172464
Chicago/Turabian StyleGuariglia, Paola, Massimiliano Palmiero, Anna Maria Giannini, and Laura Piccardi. 2023. "The Key Role of Empathy in the Relationship between Age and Social Support" Healthcare 11, no. 17: 2464. https://doi.org/10.3390/healthcare11172464
APA StyleGuariglia, P., Palmiero, M., Giannini, A. M., & Piccardi, L. (2023). The Key Role of Empathy in the Relationship between Age and Social Support. Healthcare, 11(17), 2464. https://doi.org/10.3390/healthcare11172464