1. Introduction
Suicide is a difficult topic to understand in the current society, even for psychologists, scientists, and researchers who study and deal with it on a daily basis. “How can someone take their own life leaving everything behind? How can they lose so much hope? How can they stop fighting? There is always a way out..., there has to be..., right?” Many questions, whys, and wherefores exist and require a deeper analysis. Abundant factors, which can be infinite, may play an influencing role [
1]. Additional questions can be added if the person who has exercised their option to leave freely and deliberately is an adolescent, given the emptiness and great pain it causes their families.
Durkheim (1928), one of the first to scientifically define suicide, defined it as “any case of death resulting, directly or indirectly, from a positive or negative act, carried out by the victim himself, knowing that it would produce this result” [
2]. When dealing with suicide, certain theoretical obstacles need to be addressed before an adequate analysis can be made. There is consensus when it comes to understanding the act of suicide as the behavior taken by a person with the intention of attempting to take their own life as a response to multiple factors [
3]. Villalobos (2009) states that for an act of suicide to occur, three types of determinants must be met: death as a result of harm, which has been produced by the victim themselves and intentionally inflicted [
4]. Conversely, there is still confusion regarding some terminologies associated with suicide.
Once suicide has been defined, suicidal ideation arises. Llosa-Martinez and Canetti-Wasser (2019) defined suicidal ideation as the thought of the will to take one’s own life, the intrapsychic element that leads a person to commit such an act [
5]. Furthermore, O’Carroll et al. (1996) stated that it could only be detected verbally through self-report [
6]. Researchers warn that suicidal ideation is a highly significant predictor prior to the behavioral act of suicide [
7]. Hence, they stress the importance of performing quality follow-ups that detect such thoughts in advance.
Conversely, attempted suicide would be any failed act intended to take one’s own life by intentionally inflicting harm [
8]. This type of self-injurious action would involve suicidal ideations and plans to commit suicide; however, for one reason or another, it is not achieved [
9]. In addition, suicidal risk is the sum of harmful factors (social, family, psychological, and behavioral) that a person suffers and also increases the likelihood of suicide attempts and subsequently may lead to suicide [
10].
In this work, the modeling approach that was followed is the one proposed in the theoretical framework indicated by Gabilondo [
11]. In coherence with the SESPAS Report (Spanish Society of Public Health and Health Administration), the need arises to follow a multidisciplinary model for suicide prevention in Spain, promoted by the World Health Organization (WHO), which emphasizes the multifactorial nature of suicide and in which different agents such as educational agents must be involved rather than focus only on a healthcare—health model. In this sense, cultural factors are considered in this model as critical risk factors. Specifically, the university setting is a relevant transversal educational agent for suicide prevention, and more evaluations must be conducted to raise awareness and train more effectively for suicide prevention.
It is necessary to differentiate between risk factors related to suicidal ideation and those related to completed suicide. Regarding suicidal ideation, the psycho-emotional dimension that includes variables such as hopelessness or grief in interaction with factors of other nature may be related to suicidal ideation [
12]. Similarly, the negative aspects of the emotional dimension, specifically restlessness and mood disorders such as anxiety and depression, are often symptoms involved before suicidal ideation [
13,
14], and these specific symptoms can be affected by social isolation or low-quality social interactions [
15,
16] and by using a coping strategy that is more or less productive depending on the situation [
17]. In this regard, a recent study [
18] found that the perceived social support strategy [
18] is one of the protective factors of suicidal ideation. Romero-Acosta [
19] found that the experience of victimizing events in the family environment is another risk factor for suicidal ideation in children and adolescents. Miranda-Mendizabal et al. [
20] found that specific risk factors for suicide attempts for males were the following: (a) hopelessness, (b) behavioral problems, (c) access to media, (d) suicidal behavior of a friend, and (e) parental divorce or separation. In addition, Miranda-Mendizabal et al. [
20] found that specific risk factors for suicide attempts for women were the following: (a) post-traumatic stress disorder, (b) eating disorders, (c) having been a victim of dating violence, (d) interpersonal problems, (e) previous abortion, (f) depressive symptomatology, and (g) bipolar disorder.
Regarding the risk of consummated suicide in the future, one of the relevant predictors noted is suicide attempt [
21,
22,
23] and anxiety disorder and depression [
14]. Specifically, in a recent study by Aiartzaguena and Morentin [
21] conducted in Spain on the risk factors for completed suicide in a sample aged between 14 and 55 years, the rate was three times higher in men, increasing with age with respect to demographic factors. Similarly, Aiartzaguena and Morentin [
21] found that the risk factors for completed suicide in young people were as follows: clinical risk factors such as mental and mood disorders such as depression (72%); disorders due to substance use (20.5%) and psychotic disorders (14%); and other factors such as suicide attempt (20.5%), physical illness (23%), and sociofamilial risk factors (9%). The prevalence of alcohol and drug use and substance abuse disorder was higher in women than in men [
21]. Miranda-Mendizabal et al. [
20] pointed out that further research on risk factors for suicide death for women is needed. This study also found that for men, the specific risk factors for death by suicide were access to media; drug abuse; and so-called externalizing disorders such as aggression, delinquency, and antisocial behaviors [
21].
When discussing predictors of suicide risk, whether it is the risk for suicidal ideation, attempted suicide, or completed suicide, it is necessary to address other relevant psychological factors, such as the role of drugs [
14,
24] and smoking [
25]. In this regard, in the meta-analysis conducted by Poorolajal et al. [
24], in which the association between substance use disorder and suicidal risk was examined, statistically significant associations were found between substance use disorder and suicidal ideation, suicide attempt, and suicide death. In addition, further research is needed to investigate the relationships between suicidal risk and specific types of illicit drugs. Echeverria et al. [
25] also recently conducted a meta-analysis with the aim of evaluating the relationships between smoking and suicidal behavior, finding associations between exposure to tobacco (whether current or past smokers) and increased risk for suicidal behavior, whether planning or attempting suicide, suicide intent, or death by suicide. In this sense, these authors suggest that intervention for and assessment of smoking would also be necessary as a preventive strategy for suicidal behavior. In both cases, in terms of ideation and completed suicide, the importance of the care received from an adequate health policy must be pointed out, as well as how cultural variables must be considered [
11,
26], as a certain factor can have more or less weight in a given culture or context. Similarly, in a meta-analysis [
20] of a sample of adolescents and young adults aged 12–26 years (a normative nonclinical population), both males and females, substance abuse disorder, mental disorder, and exposure to interpersonal violence were found to be common risk factors for suicidal behaviors.
Detecting the multiple factors surrounding suicide is extremely important. According to the Spanish National Institute of Statistics [
27], suicide was the primary cause of external deaths (which included accidents, falls, assaults, and homicides) in 2021, with 4003 deaths, of which 2982 were men. Statistics suggested that suicide in early life, such as in adolescence, was the leading cause of unnatural deaths in Spain between those aged 15–29 years [
28]. In 2021, the ANAR Foundation [
29] conducted a study via a telephone call with 748 minors who, at the time of the call, were attempting to take their own lives. Furthermore, they exposed that since 2012, when they started the campaign to now, a significantly exponential increase in cases of suicidal behavior was observed (1921.3%). The post-COVID-19 period that lasted from 2020 to 2022 stood out the most. These data contrasted with those collected by the FAD Foundation and the Queen Sofia Center [
30], which found that more than half of adolescents or young adults (56%) had verbalized having a delicate mental health condition, and practically half had not sought professional help (49%). This report also indicated that women reported more psychosocial problems than men, with a difference of almost 20%.
Therefore, being female may be a risk factor that would increase the probability of committing a suicidal act. However, Gonzalez-Sancho and Picado-Cortés reported that the various risk factors involved among adolescents could be classified into two large blocks: (a) psychosocial risk factors and (b) risk factors due to biological or psychiatric conditions [
31]. Within the first block, the authors created three subgroups: (a) in relation to their peers, (b) family dynamics, and (c) media. Other authors further added to these types, such as those related to negative experiences (bullying) [
32] and even spending more than three hours a day connected to the Internet [
33].
Studies reported that stigmas related to the LGTBI community were prevalent risk factors of psychosocial nature owing to the dichotomy of a human being a man and a woman, and predominantly heterosexual. Furthermore, acts of rejection and violence against those who do not follow these guidelines may cause anxiety, depression, or low self-esteem among them [
34]. Studies reported that rejection by their peers and the rest of society was an important risk factor among LGTBI individuals, given the stage of maturational and vital development that causes the creation of networks beyond those created within the family environment [
35]. Some related factors include null or scarce communication with others, school problems, unwanted pregnancies, lack of emotional resources available to face rejections, and absence of stable affective relationships [
36]. The effect of bullying on suicidal acts, as well as school bullying in person and through social networks (cyberbullying), are important [
37]. The ANAR Foundation reported that 70% of the adolescents evaluated and who presented suicidal ideation at some point declared having suffered mistreatment at school and/or high school [
29]. Bailin et al. stated that cyberbullying could generate cases of depression and functional alterations in school, work, personal hygiene, and/or self-efficacy [
38]. The weight that the media has in society is noteworthy. Hence, studies have evaluated the influence media can have on the contagion effects or “Werther effect”, where the way of reporting the news could influence suicidal behaviors among other adolescents [
39].
Other factors would include those of a psychological or biological nature. Studies on biological factors are scarce, with limited comprehensive results to reach a clear conclusion; however, a statistically significant correlation was observed that conditions in the amygdala or prefrontal cortex, even certain genetic anomalies, were correlated with increased suicide risk [
40]. Psychological factors have been most researched. Many studies have related suicide attempts and the act itself to psychiatric illnesses [
41,
42]. Major depressive disorders in adolescents were a direct cause of suicide [
43]. Furthermore, the probability increased with other related factors, such as an anxiety crisis [
44], panic attacks [
45], or post-traumatic stress attacks [
46]. Some studies observed alterations in emotional processing or even decision making (neural ability within the executive functions) [
47] and coping strategies [
48].
The modeling approach used, as compared with more commonly analyzed models in psychology (e.g., multiple regression and ordinal logistic regression), has advantages since it allows the design of artificial neural networks to analyze the relationships between psycho-emotional constructs and suicidal risk. This aims to clarify, through the proposed model, the previous results obtained from other types of analysis that are still not entirely conclusive. This could help design more effective cross-cutting programs, especially in university settings, for the prevention of suicide risk factors and the promotion of protective factors with the assistance of an “intelligent tutor” from the university teaching environment [
49,
50]. Additionally, it could aid decision-makers in health policies and designing programs for prevention and psycho-educational intervention, leveraging the improved predictive capacity and other advantages of artificial intelligence in this field [
51,
52]. For instance, it could enable even more personalized and effective learning experiences [
53], which is crucial when dealing with aspects related to health education.
Despite the above-mentioned studies, further studies are required to evaluate young ages and confirm inconclusive or contradictory results via an innovative methodology based on an analysis of artificial neural networks to examine whether certain previous results related to these variables, such as the emotional dimension either in its negative or positive pole, were confirmed. This study aimed to examine the psycho-emotional variables associated with suicidal risk and determine their predictive capacity. The specific objectives were: (1) to analyze the relationship between suicidal risk and variables of the model and (2) to design an artificial neural network with predictive capacity of suicidal risk.
4. Discussion
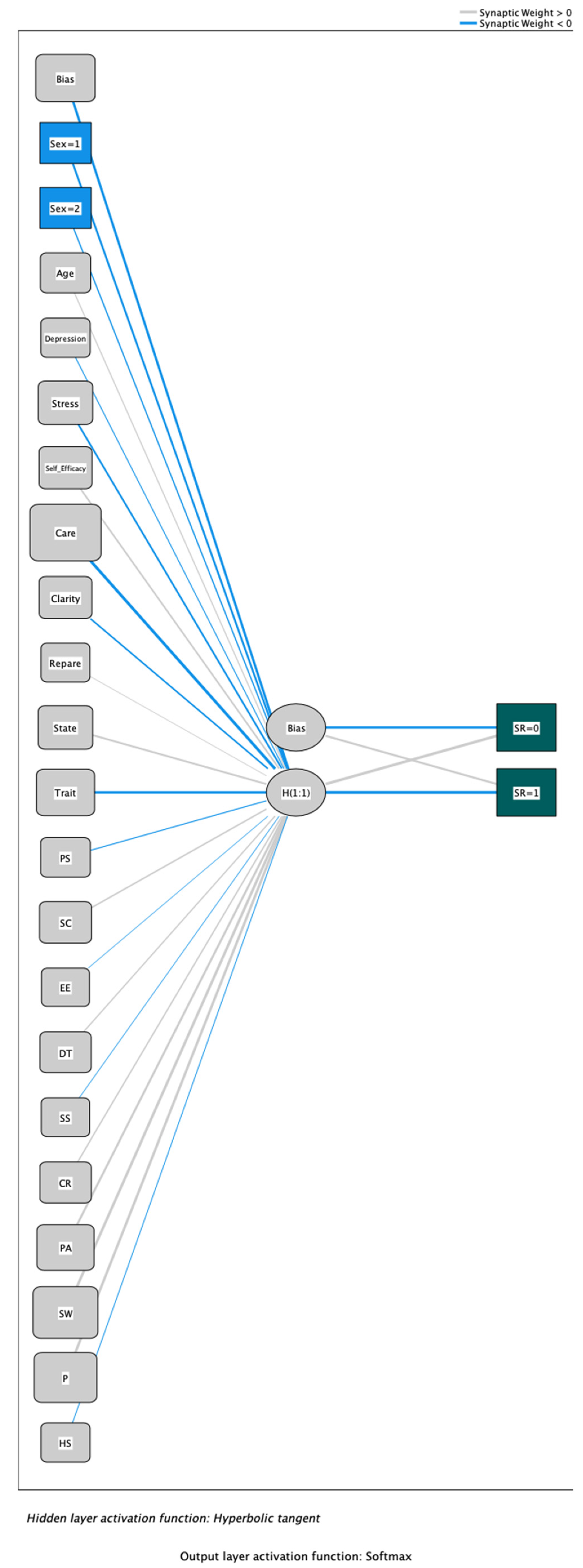
This study aimed to examine the relationship between suicidal risk and other protective and risk factors by designing an artificial neural network with predictive capacity for suicidal risk. Emotional attention had the highest predictive capacity in the ANN, followed by the problem solving coping strategy, level of perfectionism, and trait anxiety. Hence, the findings suggest that key independent variables influencing suicidal risk include emotional intelligence, coping mechanisms, anxiety, and the degree of perfectionism.
Specifically, the emotional care dimension related to the ability to express and experience feelings appropriately shows the highest predictive ability in the artificial neural network-based model. This result is congruent with a previous study [
79] conducted in another context in which a dual model based on RNN neural networks and the analysis of open vocabulary, such as emotional lexical expressions and other characteristics that are a part of the emotional dimension, such as emotional stability. In that study [
79], a greater use of the emotional dimension in its negative aspect, such as a more depressive and anxious language, was found to correlate with a higher level of suicidal risk. Similarly, this study found that users with greater anger as an emotion scored higher on the suicide risk variable. Taliaferro et al.’s [
80] study involving 70,022 students found that hopelessness was one of the risk factors for both suicidal ideation and behavior.
Regarding coping strategies, the use of productive coping strategies, such as problem-solving skills and cooperative skills, as in our study, are considered protective factors for suicidal risk [
81]. Similarly, among the functional strategies, in Mirkovic et al.’s [
81] recent study, the following are also noted: “working hard and achieving”, “physical recreation”, and “seeking relaxing diversions”. Other research [
82] highlights that communication problems and difficulties in problem solving with the presence of family conflicts would be risk factors for suicidal behavior. Similarly, Taliaferro et al. [
80] found that parent connectedness is one of the protective factors. However, the scientific literature [
17] has established that the use of strategies considered a priori as dysfunctional or unproductive, such as social withdrawal and problem avoidance, are generally associated with greater internalized symptomatology, such as anxiety and depression, which is one of the risk factors for suicidal ideation as indicated by Mata et al. [
83].
Regarding the emotional dimension in its negative aspect of anxiety, the results of our study are consistent with Matero et al. [
79], in which statistically significant associations were found between levels of anxiety and depression with a higher level of suicidal risk. Similarly, a meta-analysis and systematic review of longitudinal studies conducted by Gili et al. [
14] found that an anxiety disorder is one of the important risk factors for suicide; therefore, its prevention in combination with other factors is critical for, for example, suicidal ideation to progress to suicide attempt in young people.
Regarding the perfectionism variable, another recent research [
83], as in the present study, found that the level of perfectionism is another relevant factor for suicide risk. Specifically, Mata et al. [
83] evaluated suicidal ideation, level of perfectionism, depressive symptomatology, and negative life events in 224 Portuguese young people aged 18–25 years; they found that the level of perfectionism was one of the risk factors that mediated the relationship between negative life events and suicidal ideation; they pointed out the importance of assessing levels of perfectionism for the prevention of suicidal behavior. In addition, Roxborough et al. [
84] found that so-called maladaptive perfectionism was associated with the level of suicidal ideation and that negative life events constitute another important risk factor for suicidal behavior. Leal [
85] also found statistically significant correlations between the level of maladaptive perfectionism and the tendency for suicidal ideation. Chemisquy [
86] also highlights relationships between so-called unhealthy or maladaptive perfectionism and the variable suicidal ideation.
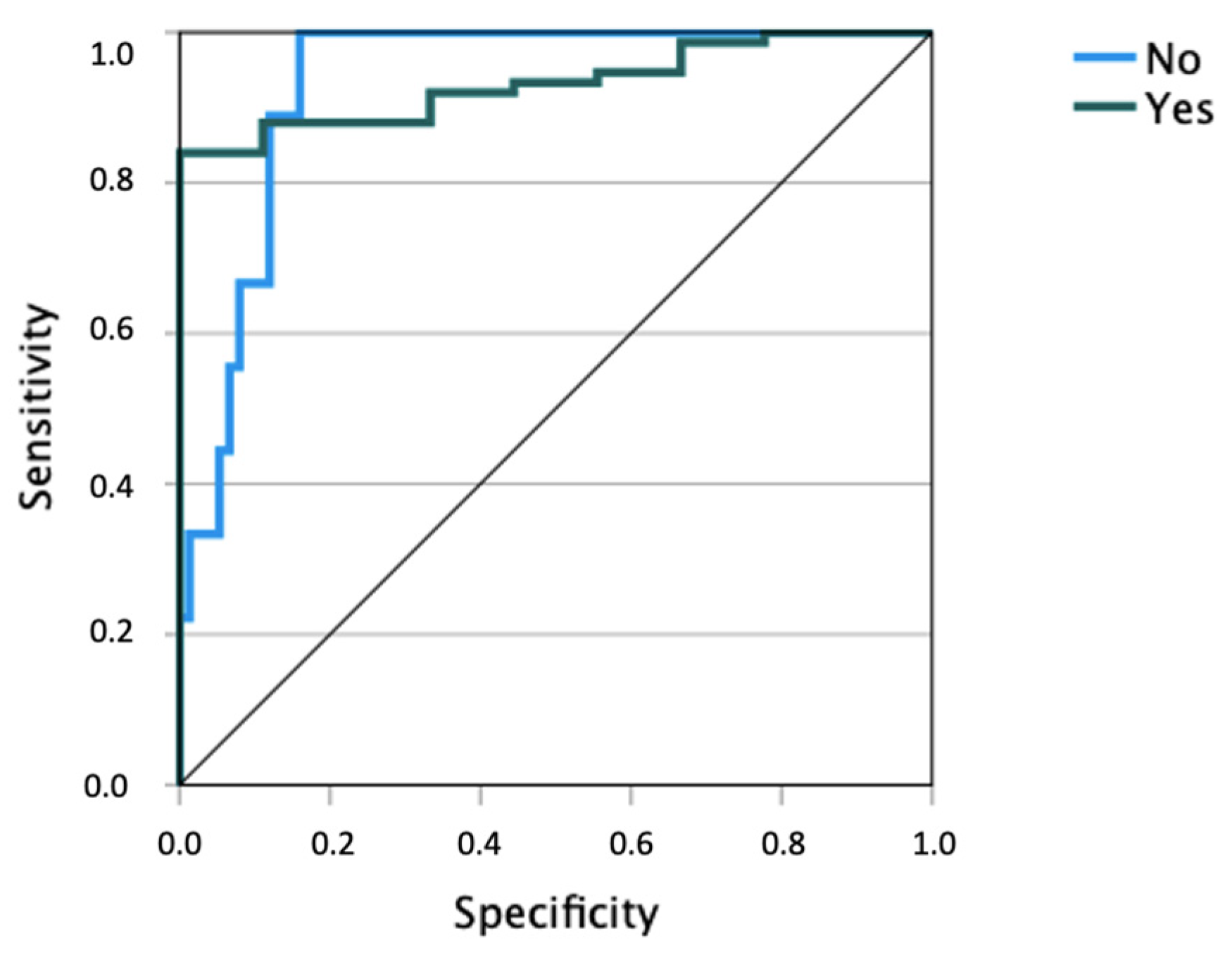
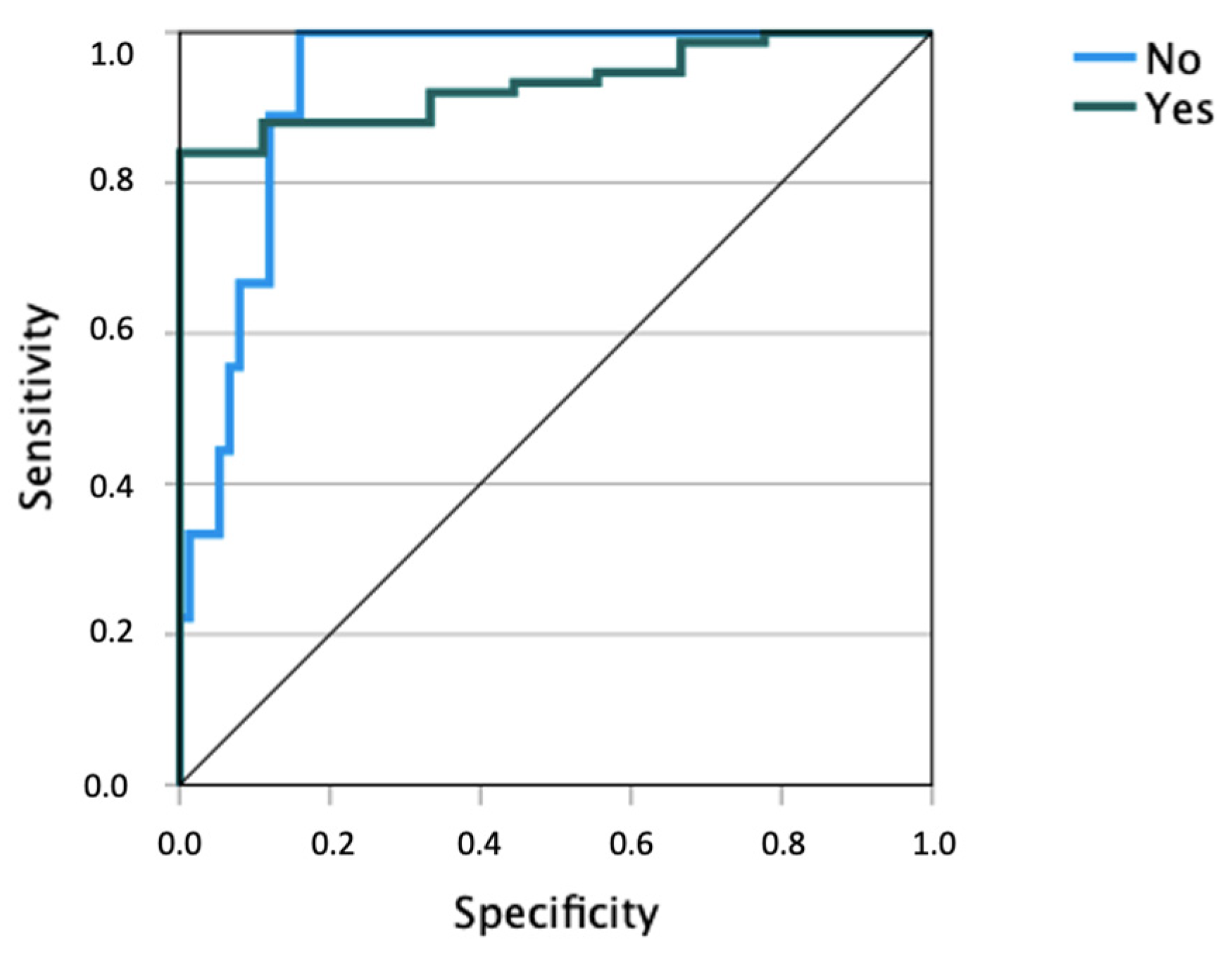
Studies that address the potential uses of ANN, such as its utility in the design of prevention and monitoring programs, are emerging. The ANN achieved a hit rate of 85.7%, much higher than chance, and with only 14.3% of incorrect cases. These results were congruent with those of other previous studies where the emotional dimension was relevant [
43,
44,
46,
47]. However, this study confirmed and clarified previous results based on the current possibilities for psychology offered by artificial intelligence. The variable sex was an important independent variable of ANN. Some previous studies found higher levels of anxiety and predisposition to suicidal risk in women than in men [
87,
88]. Therefore, this variable should be considered in the design of future programs for the prevention of suicidal behavior. In this sense, the results obtained in our context are consistent with a random-effects meta-analysis performed by Miranda-Mendizabal et al. [
20], in which the importance of suicide prevention programs is evident. The importance of the gender variable is evidenced in these programs when discussing general and specific risk factors in young people. Specifically, this meta-analysis found a higher risk of attempted suicide in women and a higher risk of death by suicide in men, finding the following risk factors common to both men and women: mental disorder, previous substance abuse disorder, and previous exposure to interpersonal violence. To detect suicidal risk, knowing the coping strategies that a person would implement was fundamental, together with their emotional intelligence. A previous study demonstrated that the university environment was stressful for students, especially in their first years [
89]. Hence, effective strategies for coping with emotions and the promotion of emotional education from childhood were required [
90]. Another study revealed evidence of the relationships between the suicide risk variable and the stress coping strategies variable [
48]. These types of evaluations were necessary to optimize the prevention of suicidal behavior [
7] and address the issues from all angles [
91]. It was also related to artificial intelligence and considered necessary before proceeding to the design of a program outside a university setting for preventive strategies. This may also contribute to better monitoring aspects and strategies, such as those recently commented on by Al-Halabí and Fonseca-Pedrero [
22], wherein certain deficits, such as those related to emotional regulation, and a lack of psychological flexibility, such as cognitive flexibility, were relevant variables for vulnerability to suicidal behavior [
22]. In addition, these types of evaluations and the book by Al-Halabí and Fonseca-Pedrero [
22] can be useful to improve the strategy that responded to the acronym
PEPE (
Ask,
Listen,
Promote Help and Be in Touch) and the awareness and education proposed in the SOS program [
92].
Other studies conducted on similar populations or Spanish-speaking populations include those by Castillo-Sánchez et al. [
93], Matero et al. [
79], and Vásquez-Escobar et al. [
94]. In a recent review by Castillo-Sánchez et al. on the use of machine learning methods for suicide detection on social networks, Linguistic Inquiry and Word Count was found to be the most frequently used method for suicide risk prediction, according to the information posted on social networks, with machine learning-based models using the Python programming language being very useful in this process. The latter was implemented in 75% of the studies analyzed in this review, and the Supported Vector Machine was implemented in 65% of the studies, demonstrating the importance of the use of algorithms and models applied to social networks for suicide risk assessment. Similarly, another recent research [
79] assessed suicidal risk using a dual context model (with suicide forum content and separated from other content) multilevel analysis of messages and users in forums. This study explored theoretical dimensions such as lexical emotional expression, personality characteristics, and the use of overt vocabulary, for example, in topics. To achieve this, among other aspects, they used a novel dual RNN (Recurrent Neural Network) architecture. They found that by combining suicide context and non-suicide elements, there were significant gains in building these predictive models. This combination allowed them to incorporate features of open vocabulary and theoretical dimensions, confirming the correlation between higher levels of anxious and depressive language with an increased risk for suicide, among other factors. Vásquez-Escobar et al.’s [
94] cross-sectional analytical study on a Spanish-speaking population in Colombia examined factors associated with suicide attempts, specifically intentional intoxication; they found the highest risk associated with sociodemographic factors, with a higher risk for death in men than in women, as well as in people who were not part of a health insurance scheme. They also found that sociodemographic variables such as place of residence, sex, ethnicity, gender, age, and educational level were statistically significant when compared with mortality.
A limitation of this study was that self-reported questions were used. Hence, the responses may be subjective. The bias of having considered only the university population in a branch of knowledge, such as education, psychology, and pedagogy, could be a limitation of the study in terms of the generalization of the results. Similarly, the results were not compared with those of a no-university population. Given the relationship between educational level and suicide risk [
95], the exclusive inclusion of university students may have influenced suicide-related factors. This may also have occurred due to the higher proportion of females included. However, determining the indicators of suicidal behavior and, thus, preventive measures is a social need for research, especially in the university setting, which according to some studies [
90], can generate more stress and anxiety in young people. On a different note, a neural network requires an adequate amount of data to learn relevant patterns and features in the training data and to be able to generalize them correctly to new instances. Since the number of participants is limited, there could be problems in the generalization of the data, as well as an increased risk of overfitting the model to the training data and a bias in the conclusions [
96]. It is also important to mention that dichotomization also has its disadvantages. For example, it can lead to a loss of information if the original variable is continuous in nature or has multiple categories with relevant information.


 ,
, 


{kind=link}
{kind=link}