
Exploring Communication Practices in Italian Physiotherapy: Knowledge and Use of Effective Communication Strategies—A National Descriptive Study

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
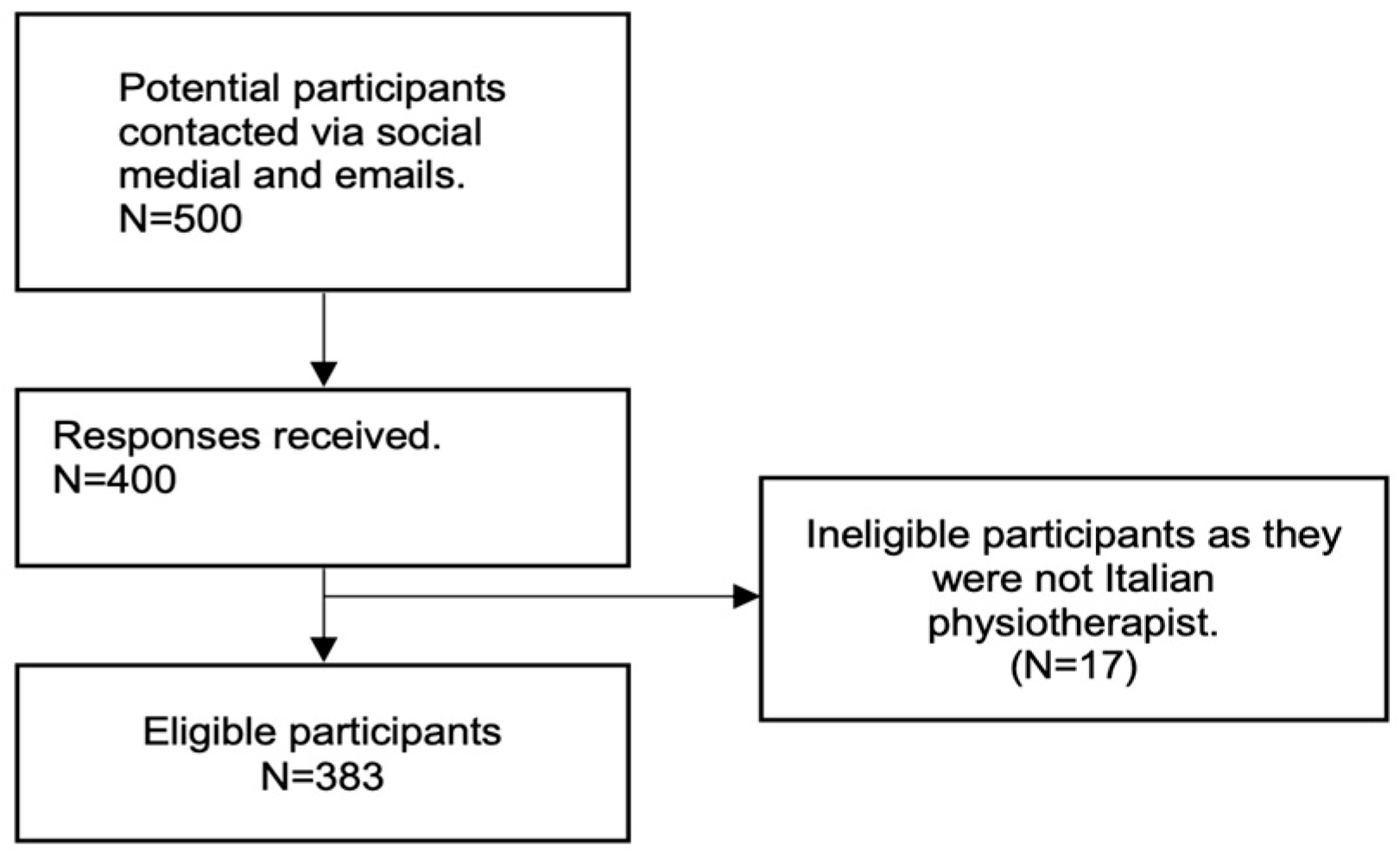
2.2. Participants and Methods of Administration of the Survey
2.3. Development of the Questionnaire
2.4. Data Collection and Analysis
3. Results
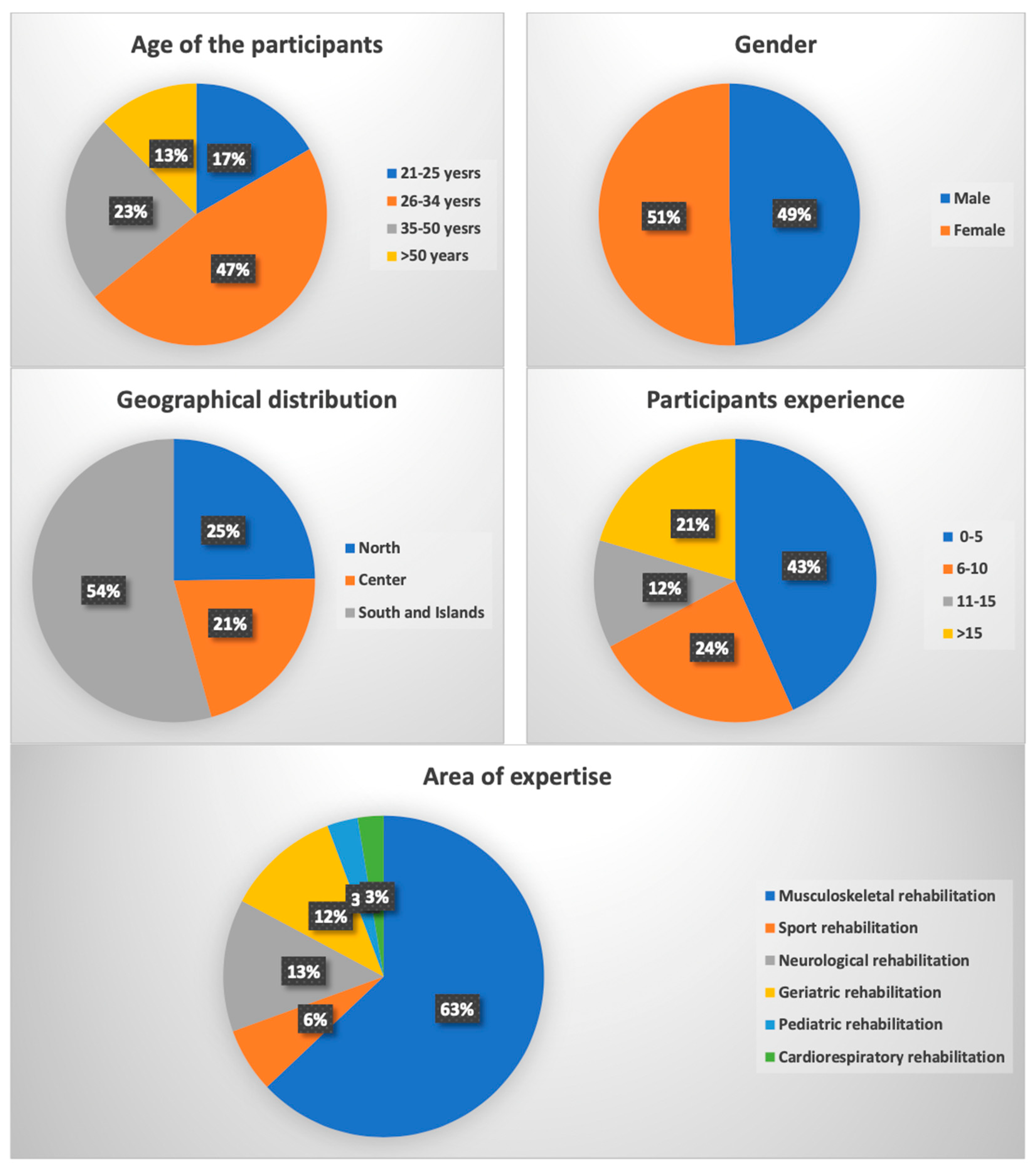
3.1. Sociodemographic Characteristics of the Respondents
3.2. Results of the Questions in the Understanding and Implementation of Effective Communication Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Q1.
- How old are you?
- 21–25
- 26–34
- 35–50
- >50
- Q2.
- Please select your gender from the following options:
- Female
- Male
- Q3.
- Which specific geographic region serves as the primary location for your professional activities?
- North
- Center
- South and islands
- Q4.
- What is the highest level of education you have attained?
- Three-year degree
- High diploma (1 year)
- Master’s degree
- Q5.
- For how many years have you been actively practicing your profession?
- 0–5
- 6–10
- 11–15
- >15
- Q6.
- Which of the following options best represents your preferred working environment?
- Employee
- Freelance
- Q7.
- In which therapeutic area do you predominantly work?
- Musculoskeletal rehabilitation
- Sport rehabilitation
- Neurological rehabilitation
- Geriatric rehabilitation
- Pediatric rehabilitation
- Cardiorespiratory rehabilitation
- Q8.
- In which context did you hear about communication related to the profession of physiotherapist “for the first time”?
- I never heard of it
- Three-year degree
- Master’s degree
- University Masters
- Private course university course
- Other
- Q9.
- Among the following, which “non” represents an example of “non-verbal language”?
- Gestures of the physiotherapist.
- Physiotherapist eye movements.
- Using metaphors to explain concepts to the patient.
- Tone and timbre of the physiotherapist’s voice.
- I don’t know the difference between verbal and non-verbal language.
- Q10.
- During the interview with the patient:
- I don’t pay attention to the words I use and how I use them.
- I pay little attention to the words I use and how I use them.
- I pay moderate attention to the words I use and how I use them.
- I pay “a lot” of attention to the words I use and how I use them.
- Q11.
- In relation to the statement “Words can harm the patient,” please select the option that best aligns with your agreement:
- Not at all
- Slightly
- Moderately
- Strongly
- Q12.
- The use of effective therapeutic communication represents:
- A strategy “not at all” effective in increasing the patient’s therapeutic adherence.
- An “ineffective” strategy in increasing the patient’s therapeutic adherence.
- A “moderately” effective strategy in increasing the patient’s therapeutic adherence.
- A “very” effective strategy in increasing the patient’s therapeutic adherence.
- Q13.
- How much time do you typically dedicate to ensuring that the patient has correctly understood the concepts conveyed during the session (e.g., summarizing aloud, inviting the patient to explain the learned concepts in their own words, watching summary videos together)?
- I do not engage in this practice.
- Approximately 2 min.
- 3 to 5 min.
- 6 to 10 min.
- More than 10 min.
- Q14.
- Which option among the following is utilized to facilitate the patient’s comprehension of the explanations provided during the session?
- I don’t use any media.
- Words.
- Images.
- Brochures to read.
- Audiovisual material or online resources.
- Other.
- Q15.
- During the collection of medical history, which approach do you typically follow regarding patient interruptions?
- Only a few seconds pass before interrupting the patient.
- Approximately 1-min passes before interrupting the patient.
- 2 to 3 min pass before interrupting the patient.
- I let the patient talk until they stop on their own.
- Q16.
- Once the type of patient has been identified:
- I use a communication register similar to that of the patient.
- I remain fixed on my communicative register.
- Q17.
- Have you ever heard of “Motivational Interviewing”?
- Yes
- No
- Q18.
- During the medical history collection:
- I don’t” use open-ended questions.
- I use “few” open questions.
- I use “moderately” open-ended questions.
- I use “many” open-ended questions.
- Q19.
- During the treatment session, please indicate your use of metaphors to help the patient better understand concepts:
- “I don’t” use metaphors to allow the patient to better grasp the concepts.
- “I use few” metaphors to allow the patient to better grasp the concepts.
- “I use metaphors moderately” to allow the patient to better grasp the concepts.
- “I use many” metaphors to allow the patient to better grasp the concepts.
References
- Engel, G.L. The Clinical Application of the Biopsychosocial Model. J. Med. Philos. 1981, 6, 101–124. [Google Scholar] [CrossRef]
- Zolnierek, K.B.H.; DiMatteo, M.R. Physician Communication and Patient Adherence to Treatment: A Meta-Analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.G.; Fuhrel-Forbis, A.; Rogers, M.A.M.; Eggly, S. Association between Nonverbal Communication during Clinical Interactions and Outcomes: A Systematic Review and Meta-Analysis. Patient Educ. Couns. 2012, 86, 297–315. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.M.; Ferreira, P.H.; Maher, C.G.; Latimer, J.; Ferreira, M.L. The Influence of the Therapist-Patient Relationship on Treatment Outcome in Physical Rehabilitation: A Systematic Review. Phys. Ther. 2010, 90, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.D.; Watzlawick, P.; Bevin, J.H.; Jackson, D.D. Pragmatics of Human Communication: A Study of Interactional Patterns, Pathologies, and Paradoxes. Man 1969, 4, 471. [Google Scholar]
- Mehrabian, A. “Silent Messages”—A Wealth of Information About Nonverbal Communication (Body Language). In Personality & Emotion Tests & Software: Psychological Books & Articles of Popular Interest; Self-Published: Los Angeles, CA, USA, 1981; pp. 3–4. [Google Scholar]
- Harris, T.E.; Nelson, M.D. Verbal Communication. In Applied Organizational Communication; Routledge: Oxfordshire, UK, 2019; pp. 82–92. [Google Scholar] [CrossRef]
- Burnard, P. The Skilled Helper. Nurse Educ. Today 1991, 11, 158. [Google Scholar] [CrossRef]
- Stickley, T. From SOLER to SURETY for Effective Non-Verbal Communication. Nurse Educ. Pract. 2011, 11, 395–398. [Google Scholar] [CrossRef]
- Rossettini, G.; Carlino, E.; Testa, M. Clinical Relevance of Contextual Factors as Triggers of Placebo and Nocebo Effects in Musculoskeletal Pain. BMC Musculoskelet. Disord. 2018, 19, 27. [Google Scholar] [CrossRef]
- Testa, M.; Rossettini, G. Enhance Placebo, Avoid Nocebo: How Contextual Factors Affect Physiotherapy Outcomes. Man. Ther. 2016, 24, 65–74. [Google Scholar] [CrossRef]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for Enhancing Medication Adherence. Cochrane Database Syst. Rev. 2014, 2014, CD000011. [Google Scholar] [CrossRef]
- EBSCOhost: Assessing Nursing Students’ Basic Communication and Interviewing Skills: The development and testing of a rating scale. J. Adv. Nurs. 1999, 29, 658–665.
- Murray, A.; Hall, A.; Williams, G.C.; McDonough, S.M.; Ntoumanis, N.; Taylor, I.; Jackson, B.; Copsey, B.; Hurley, D.A.; Matthews, J. Assessing Physiotherapists’ Communication Skills for Promoting Patient Autonomy for Self-Management: Reliability and Validity of the Communication Evaluation in Rehabilitation Tool. Disabil. Rehabil. 2019, 41, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
- Dyche, L.; Swiderski, D. The Effect of Physician Solicitation Approaches on Ability to Identify Patient Concerns. J. Gen. Intern. Med. 2005, 20, 267–270. [Google Scholar] [CrossRef]
- Beckman, H.B.; Frankel, R.M. The Effect of Physician Behavior on the Collection of Data. Ann. Intern. Med. 1984, 101, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Mauksch, L.B. Questioning a Taboo: Physicians’ Interruptions during Interactions with Patients. JAMA 2017, 317, 1021–1022. [Google Scholar]
- Hettema, J.; Steele, J.; Miller, W.R. Motivational Interviewing. Annu. Rev. Clin. Psychol. 2005, 1, 91–111. [Google Scholar]
- Oosterhof, B.; Dekker, J.H.M.; Sloots, M.; Bartels, E.A.C.; Dekker, J. Success or Failure of Chronic Pain Rehabilitation: The Importance of Good Interaction—A Qualitative Study under Patients and Professionals. Disabil. Rehabil. 2014, 36, 1903–1910. [Google Scholar]
- O’Halloran, P.D.; Blackstock, F.; Shields, N.; Holland, A.; Iles, R.; Kingsley, M.; Bernhardt, J.; Lannin, N.; Morris, M.E.; Taylor, N.F. Motivational Interviewing to Increase Physical Activity in People with Chronic Health Conditions: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2014, 28, 1159–1171. [Google Scholar] [CrossRef]
- Resnicow, K.; DiIorio, C.; Soet, J.E.; Borrelli, B.; Hecht, J.; Ernst, D. Motivational Interviewing in Health Promotion: It Sounds like Something Is Changing. Health Psychol. 2002, 21, 444–451. [Google Scholar] [CrossRef]
- Pinto, R.Z.; Ferreira, M.L.; Oliveira, V.C.; Franco, M.R.; Adams, R.; Maher, C.G.; Ferreira, P.H. Patient-Centred Communication Is Associated with Positive Therapeutic Alliance: A Systematic Review. J. Physiother. 2012, 58, 77–87. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Murray, A.; Hall, A.M.; Williams, G.C.; McDonough, S.M.; Ntoumanis, N.; Taylor, I.M.; Jackson, B.; Matthews, J.; Hurley, D.A.; Lonsdale, C. Effect of a Self-Determination Theory–Based Communication Skills Training Program on Physiotherapists’ Psychological Support for Their Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 809–816. [Google Scholar] [PubMed]
- O’Keeffe, M.; Cullinane, P.; Hurley, J.; Leahy, I.; Bunzli, S.; O’Sullivan, P.B.; O’Sullivan, K. What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy? Qualitative Systematic Review and Meta-Synthesis. Phys. Ther. 2016, 96, 609–622. [Google Scholar] [PubMed]
- Benedetti, F.; Lanotte, M.; Lopiano, L.; Colloca, L. When Words Are Painful: Unraveling the Mechanisms of the Nocebo Effect. Neuroscience 2007, 147, 260–271. [Google Scholar] [PubMed]
- Ritter, A.; Franz, M.; Puta, C.; Dietrich, C.; Miltner, W.H.R.; Weiss, T. Enhanced Brain Responses to Pain-Related Words in Chronic Back Pain Patients and Their Modulation by Current Pain. Healthcare 2016, 4, 54. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Eck, J.; Straube, T.; Miltner, W.H.R.; Weiss, T. Do Words Hurt? Brain Activation during the Processing of Pain-Related Words. Pain 2010, 148, 198–205. [Google Scholar]
- Eck, J.; Richter, M.; Straube, T.; Miltner, W.H.R.; Weiss, T. Affective Brain Regions Are Activated during the Processing of Pain-Related Words in Migraine Patients. Pain 2011, 152, 1104–1113. [Google Scholar]
- Coudeyre, E.; Givron, P.; Vanbiervliet, W.; Benaim, C.; Herisson, C.; Pelissier, J.; Poiraudeau, S. The Role of an Information Booklet or Oral Information about Back Pain in Reducing Disability and Fear-Avoidance Beliefs among Patients with Subacute and Chronic Low Back Pain. A Randomized Controlled Trial in a Rehabilitation Unit. Ann. Readapt. Med. Phys. 2006, 49, 600–608. [Google Scholar]
- Ospina, N.S.; Phillips, K.A.; Rodriguez-Gutierrez, R.; Castaneda-Guarderas, A.; Gionfriddo, M.R.; Branda, M.E.; Montori, V.M. Eliciting the Patient’s Agenda-Secondary Analysis of Recorded Clinical Encounters. J. Gen. Intern. Med. 2019, 34, 36–40. [Google Scholar]
- Vogel, D.; Meyer, M.; Harendza, S. Verbal and Non-Verbal Communication Skills Including Empathy during History Taking of Undergraduate Medical Students. BMC Med. Educ. 2018, 18, 157. [Google Scholar] [CrossRef]
- Hattie, J.; Timperley, H. The Power of Feedback. Rev. Educ. Res. 2007, 77, 81–112. [Google Scholar] [CrossRef]
- Hendrix, R.E.; Morrison, C.C. Student Emotional Responses to Different Communication Situations. J. Appl. Commun. 2020, 104, 2. [Google Scholar] [CrossRef]
- Alperstein, D.; Sharpe, L. The Efficacy of Motivational Interviewing in Adults with Chronic Pain: A Meta-Analysis and Systematic Review. J. Pain 2016, 17, 393–403. [Google Scholar] [PubMed]
- McGrane, N.; Galvin, R.; Cusack, T.; Stokes, E. Addition of Motivational Interventions to Exercise and Traditional Physiotherapy: A Review and Meta-Analysis. Physiotherapy 2015, 101, 1–12. [Google Scholar] [PubMed]
- Takemura, Y.; Sakurai, Y.; Yokoya, S.; Otaki, J.; Matsuoka, T.; Ban, N.; Hirata, I.; Miki, T.; Tsuda, T. Open-Ended Questions: Are They Really Beneficial for Gathering Medical Information from Patients? Tohoku J. Exp. Med. 2005, 206, 151–154. [Google Scholar]
- Cowell, I.; McGregor, A.; O’Sullivan, P.; O’Sullivan, K.; Poyton, R.; Schoeb, V.; Murtagh, G. How Do Physiotherapists Solicit and Explore Patients’ Concerns in Back Pain Consultations: A Conversation Analytic Approach. Physiother. Theory Pract. 2021, 37, 693–709. [Google Scholar]
- Hashim, M.J. Patient-Centered Communication: Basic Skills. Am. Fam. Physician 2017, 95, 29–34. [Google Scholar]
- Loftus, S. Pain and Its Metaphors: A Dialogical Approach. J. Med. Humanit. 2011, 32, 213–230. [Google Scholar] [CrossRef]
- Stewart, M. The Hidden Influence of Metaphor within Rehabilitation. Touch 2015, 153, 8–13. [Google Scholar]
- Bisconti, M.; Venturin, D.; Bianco, A.; Capurso, V.; Giovannico, G. Understanding Contextual Factors Effects and Their Implications for Italian Physiotherapists: Findings from a National Cross-Sectional Study. Healthcare 2021, 9, 689. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Questions | n (%) | 95% CI |
|---|---|---|
| In which context did you hear about communication related to the profession of physiotherapist “for the first time”? | ||
| Private course | 56 (14.6%) | 11.1–18.2 |
| University course | 11 (2.9%) | 1.2–4.5 |
| Master’s degree | 9 (2.3%) | 0.8–3.9 |
| Three-year degree | 137 (35.8%) | 31–40.6 |
| University master’s | 80 (20.9%) | 16.8–25 |
| I have never heard of it | 33 (8.6%) | 5.8–11.4 |
| Other | 57 (14.9%) | 11.3–18.4 |
| Among the following, which “non” represents an example of “non-verbal language”? | ||
| Gestures of the physiotherapist. | 41 (10.7%) | 7.6–13.8 |
| Physiotherapist eye movements. | 23 (6%) | 3.6–8.6 |
| Using metaphors to explain concept to the patient. | 276 (72.1%) | 67.6–76.6 |
| Tone and timbre of the physiotherapist’s voice. | 32 (8.4%) | 5.6–11.1 |
| I don’t know the difference | 11 (2.9%) | 1.2–4.5 |
| During the interview with the patient. | ||
| I don’t pay attention to the words I use and how I use them | 2 (0.5%) | −0.2–1.2 |
| I pay little attention to the words I use and how I use them. | 4 (1%) | 0–2.1 |
| I pay moderate attention to the words I use and how I use them | 87 (22.7%) | 18.5–26.9 |
| I pay “a lot” of attention to the words I use and how I use them. | 290 (75.7%) | 71.4–80 |
| In relation to the statement “Words can harm the patient,” please select the option that best aligns with your agreement: | ||
| Not at all | 5 (1.3%) | 0.2–2.4 |
| Slightly | 5 (1.3%) | 0.2–2.4 |
| Moderately | 41 (10.7%) | 7.6–13.8 |
| Strongly | 352 (86.7%) | 83.3–90.1 |
| The use of effective therapeutic communication represents. | ||
| A strategy “not at all” effective in increasing the patient’s therapeutic adherence. | 1 (0.3%) | −0.2–0.8 |
| An “ineffective” strategy in increasing the patient’s therapeutic adherence | 4 (1%) | 0–2.1 |
| A “moderately” effective strategy in increasing the patient’s adherence. | 39 (10.2%) | 7.2–13.2 |
| A “very” effective strategy to increasing the patient’s therapeutic adherence. | 339 (88.5%) | 85.3–91.7 |
| How much time do you typically dedicate to ensuring that the patient has correctly understood the concepts conveyed during the session (e.g., summarizing aloud, inviting the patient to explain the learned concepts in their own words, watching summary videos together)? | ||
| Approximately 2 min. | 57 (14.9%) | 11.3–18.4 |
| 3 to 5 min. | 117 (30.5%) | 25.9–35.2 |
| 6 to 10 min. | 111 (29%) | 24.4–33.5 |
| More than 10 min. | 75 (19.6%) | 15.6–23.6 |
| I do not engage in this practice. | 23 (6%) | 3.6–8.4 |
| Which option among the following is utilized to facilitate the patient’s comprehension of the explanations provided during the session? | ||
| Words. | 225 (58.7%) | 53.8–63.7 |
| Images. | 71 (18.5%) | 14.6–22.4 |
| Brochures to read. | 12 (3.1%) | 1.4–4.9 |
| Audiovisual material or online resources. | 41 (10.7%) | 7.6–13.8 |
| I don’t use any media. | 8 (2.1%) | 0.7–3.5 |
| Other. | 26 (6.8%) | 4.3–9.3 |
| During the collection of medical history, which approch do you typically follow regarding patient interruptions. | ||
| Only a few seconds pass before interrupting the patient. | 8 (2.1%) | 0.7–3.5 |
| Approximately 1 min passes before interrupting the patient. | 61 (15.9%) | 12.3–19.6 |
| 2 to 3 min pass before interrupting the patient. | 121 (31.6%) | 26.9–36.2 |
| I let the patient talk until they stop on their own. | 193 (50.4%) | 45.4–55.4 |
| Once the type of patient has been identified. | ||
| I remain fixed on my communicative register. | 24 (6.3%) | 3.8–8.7 |
| I use a communication register similar to that of the patient. | 359 (93.7%) | 91.3–96.2 |
| Have you ever heard of “Motivational Interviewing”? | ||
| No | 212 (55.4%) | 50.4–60.4 |
| Yes | 171 (44.6%) | 39.7–49.6 |
| During the medical history collection. | ||
| I don’t use open-ended questions. | 7 (1.8%) | 0.5–3.2 |
| I use “few” open questions. | 69 (18%) | 14.2–21.9 |
| I use “moderately” open-ended questions. | 209 (54.6%) | 49.6–59.6 |
| I use “many” open-ended questions. | 98 (25.6%) | 21.2–30 |
| During the treatment session, please indicate your use of metaphors to help the patient better understand concepts: | ||
| I “don’t” use metaphors to allow the patient to better grasp the concepts. | 15 (3.9%) | 2–5.9 |
| I use “few” metaphors to allow the patient to better grasp the concepts. | 53 (13.8%) | 10.4–17.3 |
| I use metaphors “moderately” to allow the patient to better grasp the concepts. | 199 (52%) | 47–57 |
| I use “many” metaphors to allow the patient to better grasp the concepts. | 116 (30.3%) | 25.7–34.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Wardat, M.; Etoom, M.; Lena, F.; Pellicciari, L.; D’Amone, F.; Kossi, O.; Brindisino, F.; Abdullahi, A. Exploring Communication Practices in Italian Physiotherapy: Knowledge and Use of Effective Communication Strategies—A National Descriptive Study. Healthcare 2023, 11, 2247. https://doi.org/10.3390/healthcare11162247
Al-Wardat M, Etoom M, Lena F, Pellicciari L, D’Amone F, Kossi O, Brindisino F, Abdullahi A. Exploring Communication Practices in Italian Physiotherapy: Knowledge and Use of Effective Communication Strategies—A National Descriptive Study. Healthcare. 2023; 11(16):2247. https://doi.org/10.3390/healthcare11162247
Chicago/Turabian StyleAl-Wardat, Mohammad, Mohammad Etoom, Francesco Lena, Leonardo Pellicciari, Francesco D’Amone, Oyéné Kossi, Fabrizio Brindisino, and Auwal Abdullahi. 2023. "Exploring Communication Practices in Italian Physiotherapy: Knowledge and Use of Effective Communication Strategies—A National Descriptive Study" Healthcare 11, no. 16: 2247. https://doi.org/10.3390/healthcare11162247
APA StyleAl-Wardat, M., Etoom, M., Lena, F., Pellicciari, L., D’Amone, F., Kossi, O., Brindisino, F., & Abdullahi, A. (2023). Exploring Communication Practices in Italian Physiotherapy: Knowledge and Use of Effective Communication Strategies—A National Descriptive Study. Healthcare, 11(16), 2247. https://doi.org/10.3390/healthcare11162247