
Correlation between Physical Performance and Tensiomyographic and Myotonometric Parameters in Older Adults
 , , ,
, , ,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
2.4. Procedure
2.5. Variables
2.5.1. Muscle Quality
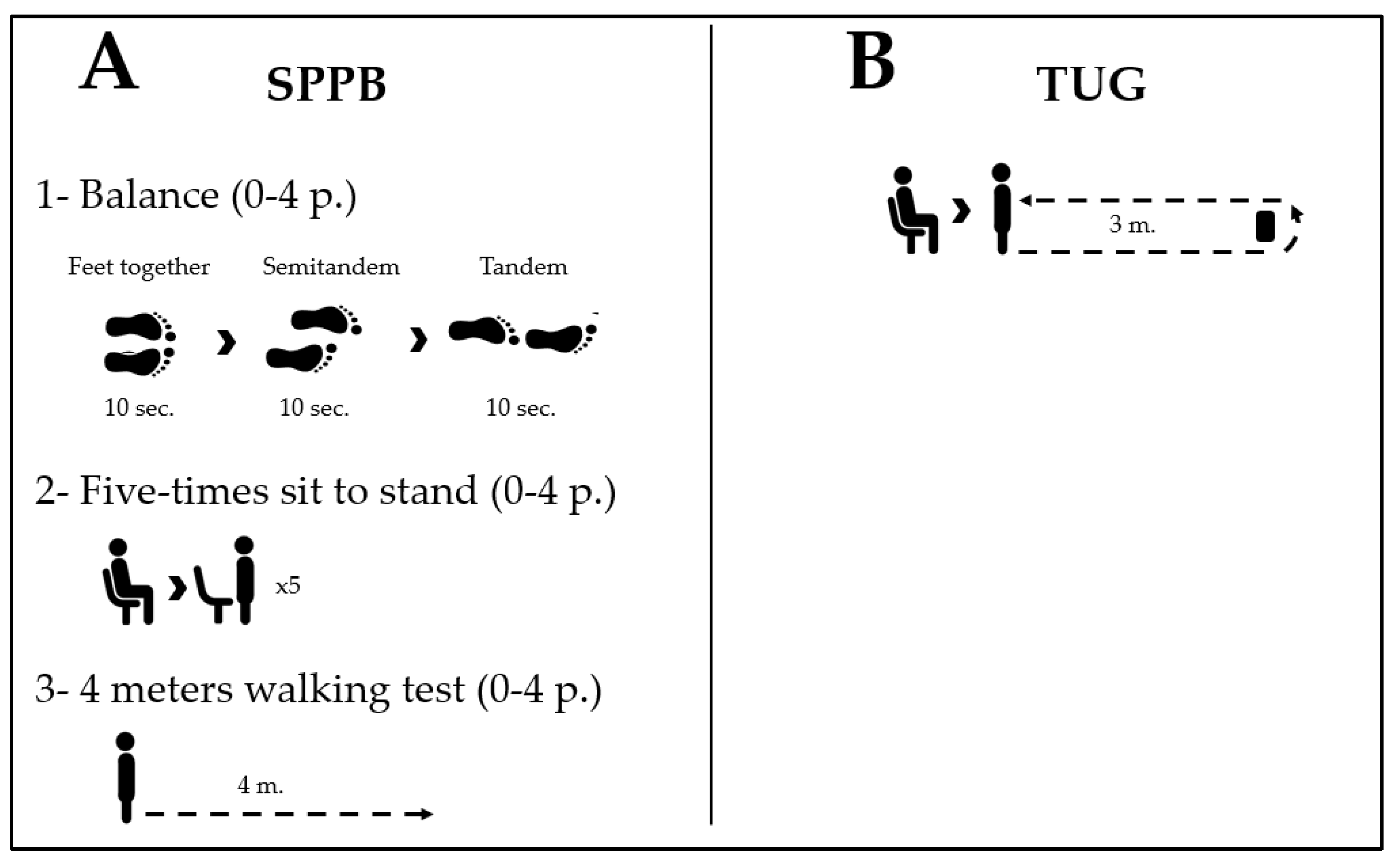
2.5.2. Physical Performance
2.5.3. Muscle Strength
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; Izquierdo, M.; Serra-Rexach, J.A.; Santos-Lozano, A.; Lucia, A. Physical Exercise in the Oldest Old. In Comprehensive Physiology; Wiley: Hoboken, NJ, USA, 2019; Volume 9, pp. 1281–1304. [Google Scholar]
- Pus, K.; Paravlic, A.H. The use of tensiomyography in older adults: A systematic review. Front. Physiol. 2023, 14, 1213993. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Bruyère, O.; Beaudart, C.; Reginster, J.Y.; Buckinx, F.; Schoene, D.; Hirani, V.; Cooper, C.; Kanis, J.A.; Rizzoli, R.; McCloskey, E.; et al. Assessment of muscle mass, muscle strength and physical performance in clinical practice: An international survey. Eur. Geriatr. Med. 2016, 7, 243–246. [Google Scholar] [CrossRef]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; Araujo de Carvalho, I.; Bautmans, I.; Bernabei, R.; et al. Assessment of Muscle Function and Physical Performance in Daily Clinical Practice: A position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Woo, J.; Scott, D.; Hoogendijk, E.O. Sarcopenia measurement in research and clinical practice. Eur. J. Intern. Med. 2021, 90, 1–9. [Google Scholar] [CrossRef]
- Sayer, A.A.; Kirkwood, T.B.L. Grip strength and mortality: A biomarker of ageing? Lancet 2015, 386, 226–227. [Google Scholar] [CrossRef]
- McGrath, R.P.; Kraemer, W.J.; Snih, S.A.; Peterson, M.D. Handgrip Strength and Health in Aging Adults. Sport. Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef]
- Soysal, P.; Hurst, C.; Demurtas, J.; Firth, J.; Howden, R.; Yang, L.; Tully, M.A.; Koyanagi, A.; Ilie, P.C.; López-Sánchez, G.F.; et al. Handgrip strength and health outcomes: Umbrella review of systematic reviews with meta-analyses of observational studies. J. Sport Health Sci. 2021, 10, 290–295. [Google Scholar] [CrossRef]
- McGrath, R.; Johnson, N.; Klawitter, L.; Mahoney, S.; Trautman, K.; Carlson, C.; Rockstad, E.; Hackney, K.J. What are the association patterns between handgrip strength and adverse health conditions? A topical review. SAGE Open Med. 2020, 8, 205031212091035. [Google Scholar] [CrossRef]
- Aadahl, M.; Beyer, N.; Linneberg, A.; Thuesen, B.H.; Jørgensen, T. Grip strength and lower limb extension power in 19-72-year-old Danish men and women: The Health2006 study. BMJ Open 2011, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Magasi, S.R.; Bubela, D.J.; Wang, Y.C.; Gershon, R.C. Grip and Knee extension muscle strength reflect a common construct among adults. Muscle Nerve 2012, 46, 555–558. [Google Scholar] [CrossRef]
- Pérez-Bellmunt, A.; Llurda-Almuzara, L.; Simon, M.; Navarro, R.; Casasayas, O.; López-de-Celis, C. Review Article Neuromuscular Response What is it and How to Measure it ? Phys. Med. Rehabil. J. 2019, 2, 118. [Google Scholar]
- Lohr, C.; Schmidt, T.; Medina-Porqueres, I.; Braumann, K.-M.; Reer, R.; Porthun, J. Diagnostic accuracy, validity, and reliability of Tensiomyography to assess muscle function and exercise-induced fatigue in healthy participants. A systematic review with meta-analysis. J. Electromyogr. Kinesiol. 2019, 47, 65–87. [Google Scholar] [CrossRef] [PubMed]
- Šimunič, B.; Degens, H.; Rittweger, J.; Narici, M.; Mekjavić, I.B.; Pišot, R. Noninvasive Estimation of Myosin Heavy Chain Composition in Human Skeletal Muscle. Med. Sci. Sport. Exerc. 2011, 43, 1619–1625. [Google Scholar] [CrossRef]
- Šimunič, B.; Pišot, R.; Rittweger, J.; Degens, H. Age-Related Slowing of Contractile Properties Differs Between Power, Endurance, and Nonathletes: A Tensiomyographic Assessment. J. Gerontol. Ser. A 2018, 73, 1602–1608. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.V. The heat of shortening and the dynamic constants of muscle. Proc. R. Soc. Lond. Ser. B-Biol. Sci. 1938, 126, 136–195. [Google Scholar] [CrossRef]
- Šimunič, B.; Koren, K.; Rittweger, J.; Lazzer, S.; Reggiani, C.; Rejc, E.; Pišot, R.; Narici, M.; Degens, H. Tensiomyography detects early hallmarks of bed-rest-induced atrophy before changes in muscle architecture. J. Appl. Physiol. 2019, 126, 815–822. [Google Scholar] [CrossRef]
- Fabiani, E.; Herc, M.; Šimunič, B.; Brix, B.; Löffler, K.; Weidinger, L.; Ziegl, A.; Kastner, P.; Kapel, A.; Goswami, N. Correlation between timed up and go test and skeletal muscle tensiomyography in female nursing home residents. J. Musculoskelet. Neuronal Interact. 2021, 21, 247–254. [Google Scholar]
- Pruyn, E.C.; Watsford, M.L.; Murphy, A.J. Validity and reliability of three methods of stiffness assessment. J. Sport Health Sci. 2016, 5, 476–483. [Google Scholar] [CrossRef]
- Labata-Lezaun, N.; López-de-Celis, C.; Llurda-Almuzara, L.; González-Rueda, V.; Cadellans-Arróniz, A.; Pérez-Bellmunt, A. Correlation between maximal radial muscle displacement and stiffness in gastrocnemius muscle. Physiol. Meas. 2020, 41, 125013. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191. [Google Scholar] [CrossRef] [PubMed]
- Labata-Lezaun, N.; Canet-Vintró, M.; López-de-Celis, C.; Rodríguez-Sanz, J.; Aiguadé, R.; Cuadra-Llopart, L.; Jovell-Fernández, E.; Bosch, J.; Pérez-Bellmunt, A. Effectiveness of a Multicomponent Training Program on Physical Performance and Muscle Quality in Older Adults: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2022, 20, 222. [Google Scholar] [CrossRef]
- Martín-Rodríguez, S.; Loturco, I.; Hunter, A.M.; Rodríguez-Ruiz, D.; Munguia-Izquierdo, D. Reliability and Measurement Error of Tensiomyography to Assess Mechanical Muscle Function: A Systematic Review. J. Strength Cond. Res. 2017, 31, 3524–3536. [Google Scholar] [CrossRef]
- Pérez-Bellmunt, A.; Labata-Lezaun, N.; Llurda-Almuzara, L.; Rodríguez-Sanz, J.; González-Rueda, V.; Bueno-Gracia, E.; Celik, D.; López-de-Celis, C. Effects of a Massage Protocol in Tensiomyographic and Myotonometric Proprieties. Int. J. Environ. Res. Public Health 2021, 18, 3891. [Google Scholar] [CrossRef]
- Huang, J.; Qin, K.; Tang, C.; Zhu, Y.; Klein, C.S.; Zhang, Z.; Liu, C. Assessment of Passive Stiffness of Medial and Lateral Heads of Gastrocnemius Muscle, Achilles Tendon, and Plantar Fascia at Different Ankle and Knee Positions Using the MyotonPRO. Med. Sci. Monit. 2018, 24, MET7570–MET7576. [Google Scholar] [CrossRef]
- Peters, D.M.; Fritz, S.L.; Krotish, D.E. Assessing the reliability and validity of a shorter walk test compared with the 10-Meter Walk Test for measurements of gait speed in healthy, older adults. J. Geriatr. Phys. Ther. 2013, 36, 24–30. [Google Scholar] [CrossRef]
- Schaap, L.A.; Fox, B.; Henwood, T.; Bruyère, O.; Reginster, J.Y.; Beaudart, C.; Buckinx, F.; Roberts, H.; Cooper, C.; Cherubini, A.; et al. Grip strength measurement: Towards a standardized approach in sarcopenia research and practice. Eur. Geriatr. Med. 2016, 7, 247–255. [Google Scholar] [CrossRef]
- Peolsson, A.; Hedlund, R.; Oberg, B. Intra- and inter-tester reliability and reference values for hand strength. J. Rehabil. Med. 2001, 33, 36–41. [Google Scholar] [CrossRef]
- Buckinx, F.; Croisier, J.L.; Reginster, J.Y.; Dardenne, N.; Beaudart, C.; Slomian, J.; Leonard, S.; Bruyère, O. Reliability of muscle strength measures obtained with a hand-held dynamometer in an elderly population. Clin. Physiol. Funct. Imaging 2017, 37, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M.; Meijers, J.M.M.; Halfens, R.J.G.; Ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; Van Loon, L.J.C.; Schols, J.M.G.A. Validity and Reliability of Tools to Measure Muscle Mass, Strength, and Physical Performance in Community-Dwelling Older People: A Systematic Review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Teraž, K.; Marusic, U.; Kalc, M.; Šimunič, B.; Pori, P.; Grassi, B.; Lazzer, S. Sarcopenia parameters in active older adults—An eight-year longitudinal study. BMC Public Health 2023, 23, 917. [Google Scholar] [CrossRef]
- Jacob, I.; Johnson, M.I.; Jones, G.; Jones, A.; Francis, P. Age-related differences of vastus lateralis muscle morphology, contractile properties, upper body grip strength and lower extremity functional capability in healthy adults aged 18 to 70 years. BMC Geriatr. 2022, 22, 538. [Google Scholar] [CrossRef]
- Agyapong-Badu, S.; Warner, M.; Samuel, D.; Stokes, M. Measurement of ageing effects on muscle tone and mechanical properties of rectus femoris and biceps brachii in healthy males and females using a novel hand-held myometric device. Arch. Gerontol. Geriatr. 2016, 62, 59–67. [Google Scholar] [CrossRef]
- Gervasi, M.; Sisti, D.; Amatori, S.; Andreazza, M.; Benelli, P.; Sestili, P.; Rocchi, M.B.L.; Calavalle, A.R. Muscular viscoelastic characteristics of athletes participating in the European Master Indoor Athletics Championship. Eur. J. Appl. Physiol. 2017, 117, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Do, Y.; Lall, P.S.; Lee, H. Assessing the effects of aging on muscle stiffness using shear wave elastography and myotonometer. Healthcare 2021, 9, 1733. [Google Scholar] [CrossRef]
- Pišot, R.; Narici, M.V.; Šimunič, B.; De Boer, M.; Seynnes, O.; Jurdana, M.; Biolo, G.; Mekjavić, I.B. Whole muscle contractile parameters and thickness loss during 35-day bed rest. Eur. J. Appl. Physiol. 2008, 104, 409–414. [Google Scholar] [CrossRef]
- Paravlić, A.H.; Pisot, R.; Simunic, B. Muscle-specific changes of lower extremities in the early period after total knee arthroplasty: Insight from tensiomyography. J. Musculoskelet. Neuronal Interact. 2020, 20, 390. [Google Scholar]
- Agyapong-Badu, S.; Warner, M.B.; Samuel, D.; Koutra, V.; Stokes, M. Non-Invasive Biomarkers of Musculoskeletal Health with High Discriminant Ability for Age and Gender. J. Clin. Med. 2021, 10, 1352. [Google Scholar] [CrossRef] [PubMed]
- Zubac, D.; Paravlić, A.; Koren, K.; Felicita, U.; Šimunič, B. Plyometric exercise improves jumping performance and skeletal muscle contractile properties in seniors. J. Musculoskelet. Neuronal Interact. 2019, 19, 38–49. [Google Scholar] [PubMed]
- Macgregor, L.J.; Hunter, A.M.; Orizio, C.; Fairweather, M.M.; Ditroilo, M. Assessment of Skeletal Muscle Contractile Properties by Radial Displacement: The Case for Tensiomyography. Sport. Med. 2018, 48, 1607–1620. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Mean (SD) or N (%) |
|---|---|
| Sex | |
| Male | 31 (60%) |
| Female | 21 (40%) |
| Dominance | |
| Right | 50 (96%) |
| Left | 2 (4%) |
| Age | 73.7 (7.44) |
| Height | 159 (10.3) |
| Weight | 67.4 (80.5; 60.1) * |
| BMI | 28.3 (4.12) |
| Variable | Mean (SD) | IQR |
|---|---|---|
| SPPB | 12 (12; 11) | |
| TUG | 8.50 (10.1; 7.39) | |
| 5XSST | 10.3 (11.9; 9.43) | |
| 4WT | 1.07 (0.26) | |
| KE-MS | 37.8 (15.8) | |
| HS | 30.4 (39.9; 21.1) | |
| Dm-RF | 4.28 (2.26) | |
| Tc-RF | 44.6 (14.7) | |
| St-RF | 292 (45.1) | |
| Dm-VL | 2.34 (3.42; 1.13) | |
| Tc-VL | 34.2 (58.2; 23.4) | |
| St-VL | 311 (36.7) |
| Rectus Femoris | Vastus Lateralis | ||||||
|---|---|---|---|---|---|---|---|
| Dm | Tc | St | Dm | Tc | St | ||
| SPPB | Correlation | 0.491 † | 0.137 † | 0.073 † | 0.329 † | 0.113 † | 0.273 † |
| p-value | < 0.001 | 0.348 | 0.609 | 0.021 | 0.438 | 0.053 | |
| TUG | Correlation | −0.172 † | 0.103 † | 0.101 † | −0.067 † | 0.032 † | 0.040 † |
| p-value | 0.237 | 0.483 | 0.481 | 0.645 | 0.825 | 0.780 | |
| 5XSST | Correlation | −0.340 † | −0.038 † | −0.108 † | −0.304 † | −0.076 † | −0.345 † |
| p-value | 0.016 | 0.793 | 0.447 | 0.032 | 0.602 | 0.012 | |
| 4WT | Correlation | 0.093 * | −0.076 * | −0.174 * | 0.094 † | 0.036 † | −0.098 * |
| p-value | 0.522 | 0.601 | 0.216 | 0.518 | 0.804 | 0.490 | |
| HS | Correlation | 0.140 † | 0.129 † | 0.002 † | −0.047 † | −0.017 † | −0.092 † |
| p-value | 0.341 | 0.383 | 0.992 | 0.752 | 0.907 | 0.535 | |
| KE-MS | Correlation | 0.220 * | −0.088 * | 0.092 * | 0.115 † | −0.085 † | 0.108 * |
| p-value | 0.125 | 0.542 | 0.515 | 0.428 | 0.557 | 0.448 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labata-Lezaun, N.; González-Rueda, V.; Llurda-Almuzara, L.; López-de-Celis, C.; Rodríguez-Sanz, J.; Cadellans-Arróniz, A.; Bosch, J.; Pérez-Bellmunt, A. Correlation between Physical Performance and Tensiomyographic and Myotonometric Parameters in Older Adults. Healthcare 2023, 11, 2169. https://doi.org/10.3390/healthcare11152169
Labata-Lezaun N, González-Rueda V, Llurda-Almuzara L, López-de-Celis C, Rodríguez-Sanz J, Cadellans-Arróniz A, Bosch J, Pérez-Bellmunt A. Correlation between Physical Performance and Tensiomyographic and Myotonometric Parameters in Older Adults. Healthcare. 2023; 11(15):2169. https://doi.org/10.3390/healthcare11152169
Chicago/Turabian StyleLabata-Lezaun, Noé, Vanessa González-Rueda, Luis Llurda-Almuzara, Carlos López-de-Celis, Jacobo Rodríguez-Sanz, Aida Cadellans-Arróniz, Joan Bosch, and Albert Pérez-Bellmunt. 2023. "Correlation between Physical Performance and Tensiomyographic and Myotonometric Parameters in Older Adults" Healthcare 11, no. 15: 2169. https://doi.org/10.3390/healthcare11152169
APA StyleLabata-Lezaun, N., González-Rueda, V., Llurda-Almuzara, L., López-de-Celis, C., Rodríguez-Sanz, J., Cadellans-Arróniz, A., Bosch, J., & Pérez-Bellmunt, A. (2023). Correlation between Physical Performance and Tensiomyographic and Myotonometric Parameters in Older Adults. Healthcare, 11(15), 2169. https://doi.org/10.3390/healthcare11152169