
The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region



Abstract
1. Introduction
Aim
2. Construct Validity and Internal Reliability of the EBPQ
2.1. Phase-1: Ensuring Face and Content Validity of the EBPQ
2.2. Phase-2: Conducting the Cognitive Debriefing by Pilot Sample
2.3. Phase-3: Assessment of the Validity and Reliability of the EBPQ
3. Materials and Methods
3.1. Design and Setting
3.2. Population and Sampling Method
3.3. Sample Size
3.4. Instruments
3.4.1. Sheet of Background Data about the Participants
3.4.2. The Evidence-Based Practice Questionnaire (EBPQ)
3.5. Recruitment Method
3.6. Ethical Considerations
3.7. Data Analysis
4. Results
4.1. Characteristics of HCPs
4.2. Experience of HCPs in Research and EBP
4.3. Reliability and Divergent Validity of the EBPQ
4.4. Construct Validity of the EBPQ
4.4.1. Exploratory Factor Analysis
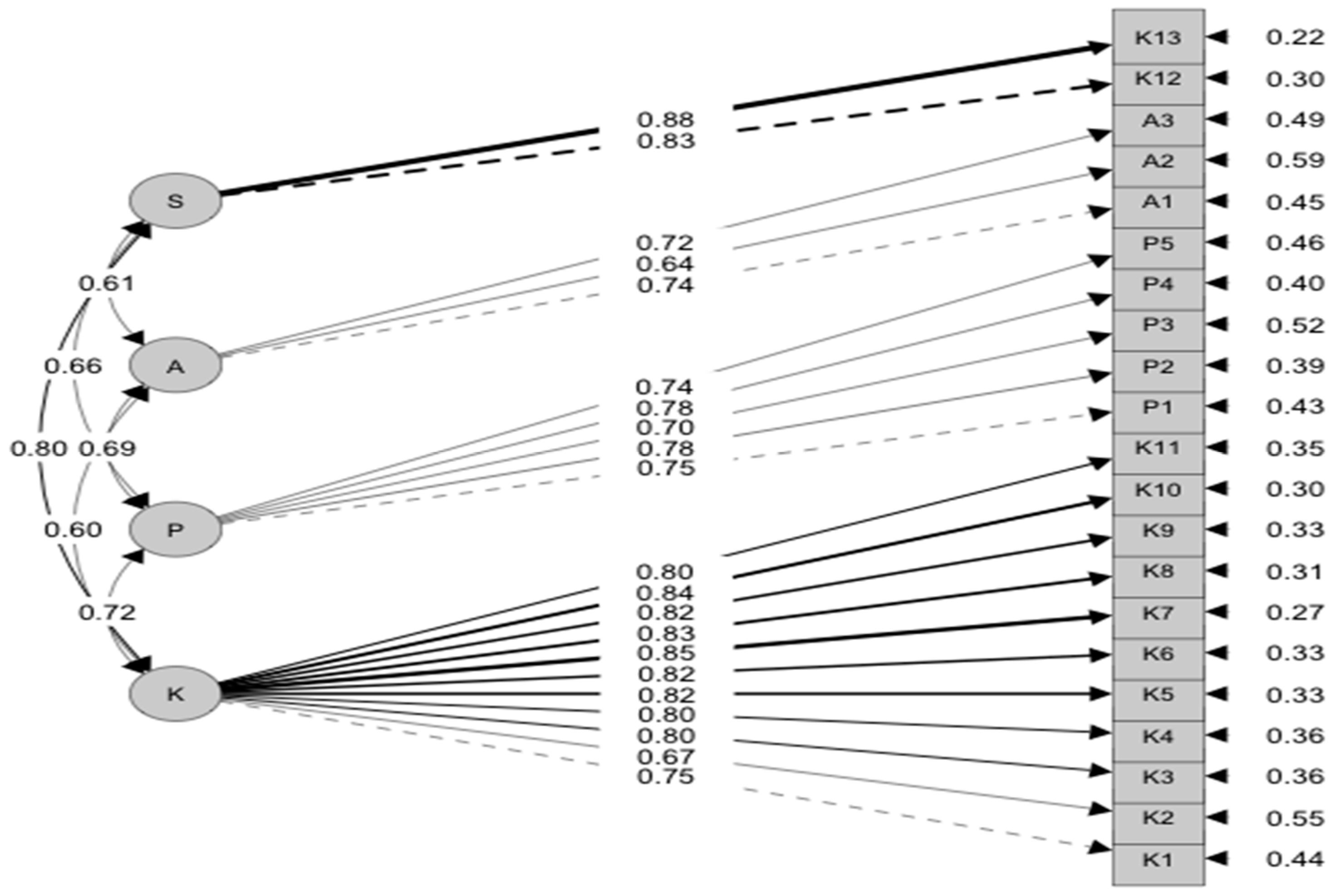
4.4.2. Confirmatory Factor Analysis (CFA)
4.4.3. Convergent Validity of EBPQ
4.5. The Internal Reliability
4.6. Divergent (Discriminant) Validity
4.7. Known Group Validity
5. Discussion
5.1. Construct Validity
5.2. Divergent Validity of the EBPQ
5.3. Internal Reliability
6. Conclusions
7. Limitations and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Country | Specialty (No) | First Language | Second Language | Undergraduate Study Language |
|---|---|---|---|---|
| Egypt | Medicines (2) | Arabic | English | English |
| Nursing (3) | ||||
| Pharmacy (1) | ||||
| Syria | Medicine (1) | Arabic | English | Arabic |
| Pakistan | Medicine (1) | Ordo | English | English |
References
- Lyons, C.; Brown, T.; Tseng, M.H.; Casey, J.; McDonald, R. Evidence-based practice and research utilisation: Perceived research knowledge, attitudes, practices and barriers among Australian paediatric occupational therapists. Aust. Occup. Ther. J. 2011, 58, 178–186. [Google Scholar] [CrossRef]
- Grimshaw, J.; Eccles, M.; Thomas, R.; MacLennan, G.; Ramsay, C.; Fraser, C.; Vale, L. Toward evidence-based quality improvement: Evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966–1998. J. Gen. Intern. Med. 2006, 21, S14–S20. [Google Scholar]
- Shortell, S.M.; Rundall, T.G.; Hsu, J. Improving patient care by linking evidence-based medicine and evidence-based management. JAMA 2007, 298, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Akkawi, F.; Suleiman, S.; Alkaiyat, S.K.A. Nurses’ Competency in Implementing Evidence-Based Practice: A Survey Study from a Governmental Hospital in the United Arab Emirates: Nurses’ Competency in Implementing Evidence-Based Practice. East. J. Healthc. 2023, 3, 32–38. [Google Scholar] [CrossRef]
- Alakhras, M.; Al-Mousa, D.S.; Al Mohammad, B.; Spuur, K.M. Knowledge, attitude, understanding and implementation of evidence-based practice among Jordanian radiographers. Radiography 2023, 29, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Capezio, A.; Decosta, P.L. Evidence-Based Decision-Making and Practice in Organizations; Oxford Research Encyclopedia of Psychology: New York, NY, USA, 2023. [Google Scholar]
- Claridge, J.A.; Fabian, T.C. History and development of evidence-based medicine. World J. Surg. 2005, 29, 547–553. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef]
- Mackey, A.; Bassendowski, S. The history of evidence-based practice in nursing education and practice. J. Prof. Nurs. 2017, 33, 51–55. [Google Scholar] [CrossRef]
- André, B.; Aune, A.G.; Brænd, J.A. Embedding evidence-based practice among nursing undergraduates: Results from a pilot study. Nurse Educ. Pract. 2016, 18, 30–35. [Google Scholar] [CrossRef]
- Tilson, J.K.; Kaplan, S.L.; Harris, J.L.; Hutchinson, A.; Ilic, D.; Niederman, R.; Potomkova, J.; Zwolsman, S.E. Sicily statement on classification and development of evidence-based practice learning assessment tools. BMC Med. Educ. 2011, 11, 78. [Google Scholar] [CrossRef]
- Sin, M.; Bliquez, R. Teaching evidence based practice to undergraduate nursing students. J. Prof. Nurs. 2017, 33, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.A.; McDonald, A.; Dubois, E.; Aljohani, F.G.; Coutts, A.P.; Majeed, A.; Rawaf, S. Assessing the state of health research in the Eastern Mediterranean Region. J. R. Soc. Med. 2013, 106, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Patton, L.J.; Garcia, M.; Young, V.; Bradfield, C.; Gosdin, A.; Chen, P.; Webb, T.; Tidwell, J. Exploring nurse beliefs and perceived readiness for system wide integration of evidence based practice in a large pediatric health care system. J. Pediatr. Nurs. 2022, 63, 46–51. [Google Scholar] [CrossRef]
- Fernández-Domínguez, J.C.; de Pedro-Gómez, J.E.; Morales-Asencio, J.M.; Bennasar-Veny, M.; Sastre-Fullana, P.; Sesé-Abad, A. Health Sciences-Evidence Based Practice questionnaire (HS-EBP) for measuring transprofessional evidence-based practice: Creation, development and psychometric validation. PLoS ONE 2017, 12, e0177172. [Google Scholar] [CrossRef]
- Ruzafa-Martinez, M.; Lopez-Iborra, L.; Moreno-Casbas, T.; Madrigal-Torres, M. Development and validation of the competence in evidence based practice questionnaire (EBP-COQ) among nursing students. BMC Med. Educ. 2013, 13, 19. [Google Scholar] [CrossRef]
- McEvoy, M.P.; Williams, M.T.; Olds, T.S. Development and psychometric testing of a trans-professional evidence-based practice profile questionnaire. Med. Teach. 2010, 32, e373–e380. [Google Scholar] [CrossRef]
- Abuadas, M.H.; Albikawi, Z.F.; Abuadas, F. Development and validation of questionnaire measuring registered nurses’ competencies, beliefs, facilitators, barriers, and implementation of Evidence-Based Practice (EBP-CBFRI). J. Nurs. Meas. 2021. [Google Scholar] [CrossRef]
- Upton, D.; Upton, P. Development of an evidence-based practice questionnaire for nurses. J. Adv. Nurs. 2006, 53, 454–458. [Google Scholar] [CrossRef]
- Diery, A.; Vogel, F.; Knogler, M.; Seidel, T. Evidence-Based Practice in Higher Education: Teacher Educators’ Attitudes, Challenges, and Uses; Frontiers in Education; Frontiers Media SA: Lausanne, Switzerland, 2020; Volume 5, p. 62. [Google Scholar]
- Fajarini, M.; Rahayu, S.; Setiawan, A. Translating, Adapting and Testing the Indonesian Version of Evidence-based Practice Questionnaire (EBPQ). OSF Preprints 2018. [Google Scholar] [CrossRef]
- Rice, K.; Hwang, J.; Abrefa-Gyan, T.; Powell, K. Evidence-based practice questionnaire: A confirmatory factor analysis in a social work sample. Adv. Soc. Work. 2010, 11, 158–173. [Google Scholar] [CrossRef]
- Bolignano, D.; Mattace-Raso, F.; Torino, C.; D’Arrigo, G.; ElHafeez, S.A.; Provenzano, F.; Zoccali, C.; Tripepi, G. The quality of reporting in clinical research: The CONSORT and STROBE initiatives. Aging Clin. Exp. Res. 2013, 25, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Bonett, D.G. Sample size requirements for testing and estimating coefficient alpha. J. Educ. Behav. Stat. 2002, 27, 335–340. [Google Scholar] [CrossRef]
- Dalheim, A.; Harthug, S.; Nilsen, R.M.; Nortvedt, M.W. Factors influencing the development of evidence-based practice among nurses: A self-report survey. BMC Health Serv. Res. 2012, 12, 367. [Google Scholar] [CrossRef]
- Rospendowiski, K.; Alexandre, N.M.C.; Cornélio, M.E. Cultural adaptation to Brazil and psychometric performance of the “Evidence-Based Practice Questionnaire”. Acta Paul. De Enferm. 2014, 27, 405–411. [Google Scholar] [CrossRef]
- Youssef, N.F.; Alshraifeen, A.; Alnuaimi, K.; Upton, P. Egyptian and Jordanian nurse educators’ perception of barriers preventing the implementation of evidence-based practice: A cross-sectional study. Nurse Educ. Today 2018, 64, 33–41. [Google Scholar] [CrossRef]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Springer Nature: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Alblooshi, S.M.; Razzak, H.A.; Hijji, F.H.; Wishah, M.A.M.; Alkarbi, M.; Harbi, A.Z. Knowledge, Attitude and Implementation of Evidence-Based Practice among Nurses; A National Survey. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Reali, S.; Lee, T.; Bishop, J.; Mirkov, S.; Johnson, J.; McCourt, E.; Hughes, J.; Pont, L.; Page, A.T.; Penm, J. Attitudes, barriers and facilitators of hospital pharmacists conducting practice-based research: A systematic review. J. Pharm. Pract. Res. 2021, 51, 192–202. [Google Scholar] [CrossRef]
- Stewart, D.; Al Hail, M.; Abdul Rouf, P.V.; El Kassem, W.; Diack, L.; Thomas, B.; Awaisu, A. Building hospital pharmacy practice research capacity in Qatar: A cross-sectional survey of hospital pharmacists. Int. J. Clin. Pharm. 2015, 37, 511–521. [Google Scholar] [CrossRef]
- Ammouri, A.A.; Raddaha, A.A.; Dsouza, P.; Geethakrishnan, R.; Noronha, J.A.; Obeidat, A.A.; Shakman, L. Evidence-based practice: Knowledge, attitudes, practice and perceived barriers among nurses in Oman. Sultan Qaboos Univ. Med. J. 2014, 14, e537. [Google Scholar]
- Zhou, F.; Hao, Y.; Guo, H.; Liu, H. Attitude, knowledge, and practice on evidence-based nursing among registered nurses in traditional Chinese medicine hospitals: A multiple center cross-sectional survey in China. Evid.-Based Complement. Altern. Med. 2016, 2016, 5478086. [Google Scholar] [CrossRef] [PubMed]


| Variables | N (%) | |
|---|---|---|
| Age | Median (IQR) | 28 (25, 32) * |
| Gender | Female | 721 (47%) |
| Male | 815 (53%) | |
| First language | Arabic | 851 (55%) |
| English | 36 (2.3%) | |
| French | 5 (0.3%) | |
| Other | 644 (42%) | |
| The highest education degree | Doctorate degree | 144 (9.4%) |
| Master degree | 422 (27%) | |
| Bachelor degree in science | 723 (47%) | |
| Still in the internship year | 247 (16%) | |
| Field of practice | Dentistry | 277 (18%) |
| Health and rehabilitation sciences | 183 (12%) | |
| Medicine | 555 (36%) | |
| Nursing | 319 (21%) | |
| Pharmacy | 202 (13%) | |
| Language of the Bachelor of Science | Arabic | 258 (17%) |
| English | 837 (54%) | |
| French | 137 (8.9%) | |
| Other | 304 (20%) | |
| Current work status | Not working (in vacation, retired, volunteers) | 192 (12%) |
| Working full-time | 896 (58%) | |
| Working part-time | 448 (29%) | |
| Number of work experience | 4 (2, 7) * | |
| Type of hospital where you currently train or work | Private and public | 338 (22%) |
| Private hospital | 351 (23%) | |
| Public/teaching hospital/government hospital | 605 (39%) | |
| other | 242 (16%) | |
| Studied an evidence-based practice course in college before graduation | No | 735 (48%) |
| Yes | 801 (52%) | |
| Attended training in evidence-based practice | No | 689 (45%) |
| Yes | 847 (55%) | |
| Number of research carried out in the last three years | Number of research you carried out in the last three years | 1.0 (0.0, 3.0) * |
| Number of research articles you read in the last month | Number of research articles you read in the last month | 2 (0.0, 5.0) * |
| Difficulty to understand English research articles Mean = 3.47 ± (SD) 1.301 Median = 4.0 | Strongly agree | 130 (8.5%) |
| Agree | 268 (17.4%) | |
| Neither agree/disagree | 330 (21.5%) | |
| Disagree | 359 (23.4%) | |
| Strongly disagree | 449 (29.2%) | |
| Items | Raw Alpha | Item-Total Domain Correlation | Mean ± SD | Overall Cronbach’s Alpha with 95% CI for Each Domain | Split-Half Reliability and Spearman–Brown Correction |
|---|---|---|---|---|---|
| 1-Practice (P) | |||||
| P1 | 0.8 | 0.7 | 4.0 ± 1.7 | 0.86 (0.85–0.87) | Split half = 0.8 SB correction = 0.9 |
| P2 | 0.8 | 0.7 | 4.0 ± 1.7 | ||
| P3 | 0.8 | 0.6 | 3.8 ± 1.6 | ||
| P4 | 0.8 | 0.7 | 4.3 ± 1.8 | ||
| P5 | 0.8 | 0.7 | 4.5 ± 1.8 | ||
| 2-Attitude (A) | |||||
| A1 | 0.7 | 0.6 | 4.5 ± 1.8 | 0.74 (0.72–0.76) | Split half = 0.6 SB correction = 0.7 |
| A2 | 0.7 | 0.5 | 4.5 ± 2.1 | ||
| A3 | 0.6 | 0.6 | 4.4 ± 1.8 | ||
| 3-Knowledge (K) | |||||
| K1 | 0.9 | 0.7 | 4.1 ± 1.8 | 0.95 (0.95–0.96) | Split half = 0.9 SB correction = 0.9 |
| K2 | 0.9 | 0.7 | 4.1 ± 1.7 | ||
| K3 | 0.9 | 0.8 | 4.3 ± 1.7 | ||
| K4 | 0.9 | 0.8 | 4.1 ± 1.8 | ||
| K5 | 0.9 | 0.8 | 4.3 ± 1.7 | ||
| K6 | 0.9 | 0.8 | 4.5 ± 1.7 | ||
| K7 | 0.9 | 0.8 | 4.3 ± 1.7 | ||
| K8 | 0.9 | 0.8 | 4.2 ± 1.7 | ||
| K9 | 0.9 | 0.8 | 4.3 ± 1.7 | ||
| K10 | 0.9 | 0.8 | 4.4 ± 1.7 | ||
| K11 | 0.9 | 0.8 | 4.5 ± 1.7 | ||
| K12 | 0.9 | 0.7 | 4.8 ± 1.8 | ||
| K13 | 0.9 | 0.7 | 4.6 ± 1.8 | ||
| Items | Factor 1 (Knowledge) | Factor 2 (Practice) | Factor 3 (Attitude) | Factor 4 (Sharing) | Uniqueness Value |
|---|---|---|---|---|---|
| P1 | 0.3 | 0.7 | 0.2 | 0.1 | 0.4 |
| P2 | 0.3 | 0.7 | 0.2 | 0.1 | 0.4 |
| P3 | 0.3 | 0.6 | 0.1 | 0.1 | 0.5 |
| P4 | 0.2 | 0.7 | 0.2 | 0.2 | 0.4 |
| P5 | 0.3 | 0.5 | 0.2 | 0.3 | 0.5 |
| A1 | 0.2 | 0.3 | 0.6 | 0.2 | 0.5 |
| A2 | 0.1 | 0.2 | 0.6 | 0.1 | 0.5 |
| A3 | 0.2 | 0.3 | 0.6 | 0.1 | 0.5 |
| K1 | 0.7 | 0.2 | 0.2 | 0.1 | 0.4 |
| K2 | 0.6 | 0.2 | 0.2 | 0.1 | 0.5 |
| K3 | 0.7 | 0.3 | 0.2 | 0.2 | 0.4 |
| K4 | 0.8 | 0.3 | 0.2 | 0.1 | 0.3 |
| K5 | 0.7 | 0.2 | 0.2 | 0.2 | 0.3 |
| K6 | 0.7 | 0.3 | 0.2 | 0.3 | 0.3 |
| K7 | 0.8 | 0.3 | 0.2 | 0.2 | 0.3 |
| K8 | 0.8 | 0.3 | 0.1 | 0.2 | 0.3 |
| K9 | 0.7 | 0.3 | 0.1 | 0.3 | 0.3 |
| K10 | 0.7 | 0.3 | 0.2 | 0.3 | 0.3 |
| K11 | 0.6 | 0.3 | 0.2 | 0.4 | 0.3 |
| K12 | 0.4 | 0.2 | 0.3 | 0.7 | 0.3 |
| K13 | 0.5 | 0.2 | 0.2 | 0.6 | 0.3 |
| EBPQ | English Difficulty | No | Mean | SD | t * | Sig. (2-Tailed) | 95% Confidence Interval of the Difference | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Practice | No | 808 | 22.91 | 6.06 | 13.86 | <0.01 | 3.96 | 5.26 |
| Yes | 728 | 18.29 | 6.98 | |||||
| Attitude | No | 808 | 15.10 | 4.30 | 15.62 | <0.01 | 3.00 | 3.87 |
| Yes | 728 | 11.66 | 4.31 | |||||
| Skill | No | 808 | 51.79 | 13.13 | 13.43 | <0.01 | 8.61 | 11.56 |
| Yes | 728 | 41.70 | 16.26 | |||||
| Sharing | No | 808 | 10.43 | 2.84 | 13.53 | <0.01 | 1.83 | 2.45 |
| Yes | 728 | 8.28 | 3.36 | |||||
| EBPQ | Studied the EBP Course in College | No | Mean | SD | t * | Sig. (2-Tailed) | 95% Confidence Interval of the Difference | |
| Lower | Upper | |||||||
| Practice | No | 735 | 19.38 | 7.36 | −7.40 | <0.01 | −3.25 | −1.88 |
| Yes | 801 | 21.95 | 6.21 | |||||
| Attitude | No | 735 | 12.93 | 4.75 | −4.36 | <0.01 | −1.48 | −0.56 |
| Yes | 801 | 13.96 | 4.47 | |||||
| Skill | No | 735 | 43.17 | 16.38 | −9.53 | <0.01 | −8.86 | −5.84 |
| Yes | 801 | 50.53 | 13.82 | |||||
| Sharing | No | 735 | 8.87 | 3.43 | −6.23 | <0.01 | −1.35 | −0.71 |
| Yes | 801 | 9.90 | 3.05 | |||||
| EBPQ—For Domains | r/p-Value * | Age | Experience | Number of Research Carried out | Number of Read Research Articles |
|---|---|---|---|---|---|
| Practice | r | 0.036 | 0.047 | 0.036 | 0.110 |
| p-value | 0.157 | 0.065 | 0.154 | <0.0001 | |
| Attitude | r | 0.137 | 0.107 | 0.018 | 0.040 |
| p-value | 0.000 | 0.000 | 0.470 | 0.115 | |
| Skill | r | 0.010 | 0.055 | 0.048 | 0.114 |
| p-value | 0.706 | 0.031 | 0.062 | <0.0001 | |
| Sharing | r | 0.088 | 0.120 | 0.066 | 0.095 |
| p-value | 0.001 | 0.000 | 0.010 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, N.; Saleeb, M.; Gebreal, A.; Ghazy, R.M. The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region. Healthcare 2023, 11, 2168. https://doi.org/10.3390/healthcare11152168
Youssef N, Saleeb M, Gebreal A, Ghazy RM. The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region. Healthcare. 2023; 11(15):2168. https://doi.org/10.3390/healthcare11152168
Chicago/Turabian StyleYoussef, Naglaa, Marina Saleeb, Assem Gebreal, and Ramy Mohamed Ghazy. 2023. "The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region" Healthcare 11, no. 15: 2168. https://doi.org/10.3390/healthcare11152168
APA StyleYoussef, N., Saleeb, M., Gebreal, A., & Ghazy, R. M. (2023). The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region. Healthcare, 11(15), 2168. https://doi.org/10.3390/healthcare11152168